
Disclaimer #1: While the opinions expressed in this essay are correct, they are mine alone and do not necessarily express the views or opinions of my employer. Probably some of these opinions do also reflect the views of my employer or at least the other people I work with, but I couldn’t specifically say which views or which people, so I’ll just leave it at “these opinions are mine alone.”
Disclaimer #2: I’m not great at writing disclaimers.
When Violence Intersects Medical Misinformation.
As the past weeks have been marked by nationwide protests against excessive force and police brutality in general and the disproportionate killing of unarmed black men and women in particular, I have remained fairly silent on this blog, which has a specific and limited scope, and have expressed my views elsewhere. Last week when George Floyd’s autopsy report was released, I had hoped to write about the medical realities of his death and expose the fallacies of claiming that it was the result of natural causes or elicit substances rather than the lethal and prolonged physical assault we all witnessed with our own eyes. Unfortunately I was utterly unable to create time to do that discussion justice, and thankfully nobody seemed to be buying that nonsense anyway. Dr. Judy Melinek, a Forensic Pathologist, offers a detailed and careful explanation of George Floyd’s death and autopsy findings in an article on MedPage Today. Her evaluation includes the following statements:
“EMS and police are sometimes trained that anyone who says “I can’t breathe” is lying — because if you can speak, you can breathe. This is not true, and there are many reasons why people might say “I can’t breathe” and still be in medical distress. These reasons include increasing fatigue of respiratory muscles; blockage of pulmonary blood flow; incomplete airway obstruction; and acidosis, a buildup of acid in the blood which triggers an increased breathing rate and causes the sensation of shortness of breath.”
In her conclusion, Dr. Melinek also explains why the autopsy performed by the County Medical Examiner actually supports his death being due to his prolonged assault, as opposed to various interpretations that sought to use the term “cardiopulmonary arrest” to argue that his death would have somehow occurred even in the absence of that fatal action.
“Floyd stopped breathing and his heart stopped beating (cardiopulmonary arrest) because of the injury caused by his restraint in the custody of law enforcement officers, to include asphyxia from neck compression. Asphyxia means that there is a lack of oxygen going to the brain. It can happen from obstruction of the airway, restriction of breathing from compression of the neck or chest, or the prevention of blood flow to the brain by collapsing the blood vessels in the neck.”
So during a busy week that offered no time to write, I was glad that this work was already being done by those whose professional credentials and experience in this area greatly surpassed my own. Otherwise, except for calls to protest with proper transmission reduction measures (masks, hand sanitizer, as much physical distancing as possible given the circumstances) since we are still in the middle of a pandemic, I have seen very little intersection between this particular blog and the protests.
However, as I have watched video after video and read account after account of police forces using “non-lethal” weaponry for crowd control purposes, as I have seen people fleeing from rubber bullets, black college students being tased and dragged from their vehicles without even being accused of a crime, and white elderly men being shoved to the ground and bleeding from their ears, I have realized that there is quite a lot happening here that involves medicine; and in fact, medical misinformation. I would argue (and ought to argue, for the sake of justifying this post in the first place) that the very way we conceptualize these methods of force is a form of misinformation in itself.
“Some of my best friends are cops.”
I’d like to start with two important caveats. They may weaken the overall message of this post, but they are true and so they ought to be included. First, I live in a city where I am frequently genuinely thankful for our law enforcement. Our police and Sheriff’s departments are active in combatting human trafficking and working with local non-profits to ensure that survivors receive support services and counseling instead of prosecution and further abuse. I have been told of police brutality and excessive violence in my community from patients who have experienced it directly, and as a white man in a position of perceived authority as their doctor, it is likely I have not been told as much of it as my patients have to tell. I believe these stories, as I believe that tolerance of any racist practices or police brutality implicates an entire department, and have offered to help those patients seek legal services in addition to helping them cope with the physical and psychological consequences of those experiences. Still, if there is widespread police corruption and brutality here in town, I at least have been blissfully unaware of it (and if it does exist, that ignorance is probably my own fault). If our police department is hyper-militarized like so many seem to be, we have at least seen no signs of it at the many recent protests and demonstrations.
Second, there are in fact men and women I care about and respect who are in law enforcement, and some I love as brothers. At least one even works in evaluating and policing the police themselves. It is hard for me to imagine them acting in the ways I have seen officers act in these videos. Yet we cannot be naive to the internal loyalty and in-group mentality that is deliberately cultivated in police departments around the country (a phenomenon that medicine is not immune to, and has to work hard to fight against). When I pray for these friends, I pray not only for their safety but also for the courage to refuse unlawful and immoral orders and to intervene and report if and when fellow officers commit acts of discrimination or excessive force and violence. As I’ve said for years, being against police brutality does not make you anti-police any more than being against child abuse makes you anti-parent. Just as the best doctors are vehemently anti-malpractice, so the best officers are anti-brutality, discrimination, and excessive force.
We only hope it’s non-lethal force.
What follows is a review of the medical facts and literature regarding the “non-lethal” methods and tools we have seen police using around the country. The main point I would like to establish is that any force, any act of assault with any tool of violence, is only “non-lethal” after the fact. We are fearfully and wonderfully made, and I have seen people recovere from shocking injuries; but we are also frail in so many ways. Often these devices only cause injury or pain instead of actual morbidity and mortality because they fail to impact in one of several particularly dangerous locations, or because their intended targets have the benefits of relative youth and relative good health. Other times, it is the heroic efforts of EMS and ER doctors and nurses that keeps the induced injuries from being fatal. The idea of something being non dangerous because the patient was afterward rescued by hospitals and healthcare professionals is obviously a contradiction in itself; if they needed rescuing, it clearly was dangerous. It is outside the scope of this discussion, but this is the same false use of statistics that certain para-health industries use to argue that they are safer than actual medical care, when really they are counting on the medical field to bail them out when things frequently do go wrong. When we look at lethality, we have to remember that many who are saved might have died; and we have to remember too the extensive suffering and lifelong injuries that also do not show up within mortality statistics alone.
The term ‘less lethal’ is far more apt, and even justifiable; but almost every weapon is ‘less lethal’ compared to firearms. The rate of death from intentional stabbing is very small compared to intentional shooting, but we would never call a knife a non-lethal weapon. As we will see, ‘less lethal’ still means potentially lethal, and many of the weapons and techniques being used still possess the potential to kill. They are not crowd control devices or nuisance stimuli, but weapons. The question we need to be asking ourselves is whether the use of weapons, including weapons with potential to maim and kill, has been justified. If police officers in these videos had no justification to discharge a firearm, did they have any justification to discharge a taser or rubber projectiles?
TASER
I want to begin with the TASER, or Thomas A. Swift’s Electric Rifle, because it is both the most commonly used less-lethal weapon employed by police and also our cultural prototype for what a non-lethal weapon is like. The fact that TASER is an acronym, and that the name is an homage to a racist science fiction novel, is something I only learned today and is outside the scope of this essay; but perhaps not irrelevant to the greater discussion of race as a factor in police brutality and use of force, or the recent use of these weapons against protesters.

Tasers are designed to be truly non-lethal. They deliver a high voltage but low current of electricity through clothing or directly into skin, incapacitating a target but causing no lasting harm. Typically this is in a 5 second burst, but the burst can be repeated or prolonged by the controller. When initially reviewing literature on Taser related injuries, most injuries seemed to be from the sudden incapacitation and not the electricity; bruising and lacerations from falling suddenly or striking an obstacle after the shock occurs. However, some of these injuries are very serious, such as concussions, testicular torsion, and even fractures at the base of the skull and around the eyes; they are still weapons, after all, designed to cause real pain. Still, under controlled conditions, at least, they seem very safe compared to traditional weapons, and it is even common for police officers to have the devices tested on themselves when they receive their training. Our shared mental image of someone being tased and their hearts stopping suddenly, based no doubt on a merely superficial relationship to cardiac defibrillators, just wasn’t readily apparent in the literature.
Or at least, that’s how it felt at first, until I came across this line from a Canadian Medical Association Journal editorial entitled Tasers in medicine: an irreverent call for proposals:
“Tasers are perfectly safe and have never, ever killed anyone. We know this because TASER International, manufacturer of the market-leading device, says so, claiming “the TASER ECD (electric control device) cannot stop the heart”. And TASER International is an honourable, and for most of its existence very profitable, company. So honourable, in fact, that they have sponsored research to prove the taser’s safety. Just about all the research, as it turns out.”
This might be that ‘sarcasm’ thing I’ve heard so much about.
The editorial cites the 2007 death of a man in the Vancouver airport following multiple taser bursts, and goes on to cite instances of TASER International actually suing researchers for publishing evidence that their products can be fatal, and even suing medical examiners for listing taser related injury as a cause of death on a death certificate (and here I am hoping this blog never becomes popular enough to catch their attention). To this the author replies, “Obviously, no one is better suited to instruct a qualified physician, coroner or specialist in forensic pathology on how to determine the cause of death than advisors to a corporation with a vested interest in the device being critiqued.” This criticism piqued my interest and led to a renewed literature search, which muddied the waters a bit more on taser safety.

An extensive review by Dr. Douglas Zipes published in the journal of the American Heart Association found multiple cases of cardiac arrest following taser use. Dr. Zipes, professor at the University of Indiana School of Medicine, states “the published body of evidence now makes it perfectly clear that a TASER X26 ECD shock can induce VF (ventricular fibrillation; a pulseless heart rhythm, i.e. cardiac arrest) in humans, transforming the argument from if it can happen to how often it happens.” He reviews both human cases of taser shots fired to the chest resulting in cardiac arrest, many of whom died, and animal models that support the anecdotal evidence offered by these cases. Finally he concludes,
“Educational material should stress avoiding chest shots if possible and should warn against repeated or long trigger pulls. However, it is clear that a single 5-second shock can induce VF. A user should be judicious with ECD deployment and treat it with the same level of respect as a firearm, suspect cardiac arrest in any individual who becomes unresponsive after a shock, quickly call for medical support, and be prepared to resuscitate, including using an automated external defibrillator if needed.”
While Dr. Zipes does conclude that death due to taser discharge is rare, it is not impossible. Treating these weapons as a safe and excellent way to make peaceful persons exercising their 1st amendment rights do as you say is clearly an unacceptable abuse of these devices.
Rubber Bullets
I think we tend to conceptualize rubber bullets and other high-velocity projectile weapons as a painful reminder that you are breaking the law; a non-lethal but extremely uncomfortable option to enforce compliance with police orders and halt a violent criminal in their tracks. Per my understanding, these projectiles are intended to be aimed at the legs (not aimed at the ground, which can cause bullet to ricochet) and at worst would cause soft tissue injury and bruising. Even in this scenario it turns out that more severe injuries are possible; but the bigger problem is that this isn’t the way these weapons are being used.

As we have witnessed in video after video, these weapons are instead being fired into crowds of protesters, often those who are peacefully assembled, without particular regard for where on the body they land. They are indeed ricocheting off of walls and barricades and are striking people in every part of the body. An article published in the British Medical Journal in 2017 found that the greatest risk from these weapons is when they are used at close range and the projectile strikes the face, head, or neck. These weapons have sufficient velocity to cause skull fractures and intracranial hemorrhage, causing permanent brain damage, or tear through the fragile arteries of the neck leading to rapid blood loss. When these projectiles impact the eye they can cause permanent blindness, or can penetrate through the fragile orbit of the eye and cause orbital fractures which can result in extensive brain injury and death. And while intentional targeting of the head and neck at close range is the most dangerous use of these weapons, firing at longer ranges is dangerous as well; while it decreases the velocity it also greatly decreases the accuracy, increasing the chances that even an appropriately aimed lower extremity shot will veer or ricochet and strike someone in a more vulnerable part of the body.
“These articles included injury data on 1984 people, 53 of whom died as a result of their injuries. 300 people suffered permanent disability. Deaths and permanent disability often resulted from strikes to the head and neck (49.1% of deaths and 82.6% of permanent disabilities).”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5736036
Though I have chosen not to include extensive images of these types of injuries on this blog post, they can be found easily enough online. One article from The Internet Journal of Surgery does include images of rubber bullets being retrieved from the neck, where they have lacerated the carotid artery, and from the abdominal cavity; but they aren’t for the faint of heart.
The head and neck are not the only locations that are vulnerable to these types of projectiles. Multiple research articles and case studies report serious injury and death resulting from rubber bullet injuries to the torso. I have quote just a handful below:
“The post-mortem examination revealed that death had been due to gunshot wounds in the chest which had caused heart and lung damage with subsequent massive internal haemorrhaging.”
https://pubmed.ncbi.nlm.nih.gov/18514453
“An autopsy examination of a man who was shot with improved rubber bullets revealed that the bullet caused pulmonary contusion (not the cause of death). The case raised a question as to how severe an injury is necessary to deter a person without causing death.”
https://pubmed.ncbi.nlm.nih.gov/19696582
“Four projectiles penetrated the right chest lodging in the right lung and injuring the right pulmonary artery, causing death. The mechanism of death in this case is rapid massive pulmonary haemorrhage.”
https://pubmed.ncbi.nlm.nih.gov/16167715

The article I quoted at the beginning of this section from the BMJ concludes:
“We find that these projectiles have caused significant morbidity and mortality during the past 27 years, much of it from penetrative injuries and head, neck and torso trauma. Given their inherent inaccuracy, potential for misuse and associated health consequences of severe injury, disability and death, KIPs do not appear to be appropriate weapons for use in crowd-control settings.”
Yet this is exactly the way these projectiles have been used in the past several weeks. And they have not even been reserved for riot response, they are literally being used for crowd control; to move back crowds of peaceful protesters, to assault those engaged in peaceful civil disobedience, and to clear clergy and lay persons working at a scheduled ministry event on private church property so that the president could use their church for a photo op.
Blunt Weapons and Physical Assault

One of the most understated shocking moments during the episode in Washington D.C. when military and police forces forcefully removed peaceful protesters, clergy, and lay persons from the premises of St. John’s church and the surrounding environs, was the one above when an officer in full riot gear rounded the corner and immediately hit a cameraman in the abdomen with the edge of his polycarbonate shield. Compared to the other methods that police can be seen using in videos of the attack, from flash-bang grenades and tear gas to rubber bullets, this may seem mean spirited but fairly minor; but as a physician, I was pretty shocked.
The abdomen is fragile. There are a lot of organs with a lot of blood flow in that area of the body, and unlike the thorax it doesn’t have a cage of hard ribs offering an additional layer of protection; just some skin, muscle, sub-cutaneous and intra-abdominal fat, and various organs. Of these organs, the liver and spleen are particularly concerning in abdominal trauma, and laceration or rupture of either can result in rapid intra-abdominal bleeding that can quickly lead to death without, and even with, proper medical attention. These injuries can sometimes occur even in healthy patients under seemingly innocuous circumstances. In the 4th season of Scrubs, a patient has a splenic rupture after wrestling with his 10 year son; and it isn’t a ridiculous plot line, medically speaking. Shields are shields; they are meant for defense, and we should be very concerned when police officers use them to play “U.S. Agent” (a more violent and aggressive version of Captain America) and assault peaceful civilians and members of the press. Other weapons, such as batons and clubs, are unlike shields actually intended to cause blunt force trauma and internal injuries, and do it well. When used against violent criminals they are far less lethal than firearms; but again, we are seeing them used against peaceful protesters, members of the press, the elderly, and even medics.
But by far the most shocking image of the week came from Buffalo, where two officers shoved 75-year-old Martin Gugino backward and then left him to lay there bleeding from either his ear or the back of his head, either of which is terrifying (this is the same man whom the president later tweeted might have been an “ANTIFA provocateur”). This is the type of injury that can indeed kill or paralyze, and these two officers could probably just have easily picked him up and moved him out of the way instead of shoving him over. As a doctor in a country with an aging population, I shouldn’t have to explain how obscene this is. Any child or grandchild who has received the call that an elderly relative has fallen knows the sinking realization that life is about to change drastically. Often it is a single fall that heralds the onset of a person’s decline. For instance, the risk of dying within the first year after a hip fracture is 21%, and that doesn’t even begin to paint the full picture of loss of independence and alteration in quality of life that often occurs after a major fall. Fall risk screening is a major component of geriatric care because of how devastating any fall can be in that population, but our screening questions are apparently incomplete; we never ask whether our elder patients plan to attend peaceful protests in the proximity of men who have sworn to serve and protect them.
Sensitive images below.


Tear Gas
There are quite a few more “non-lethal weapons” we could review, such as flash bang grenades, water cannons, and long range acoustic devices, which can cause a number of severe short-term and long-term injuries. But in the interest of time I want to focus on one last topic; tear gas.

Tear gas and pepper spray cause irritation of various receptors to produce tearing and crying, coughing, sneezing, intense physical discomfort, temporary (hopefully) blindness or blurred vision, disorientation, and pain in the throat, mouth, eyes, and lungs. Of course we could conceptualize how using this on a large crowd could cause sufficient chaos to result in more serious injuries, but in general the affects of the agents themselves are very short lived and resolve with washing away the chemicals and exposure to fresh air. There seems to be two major situations where these agents would be more dangerous.
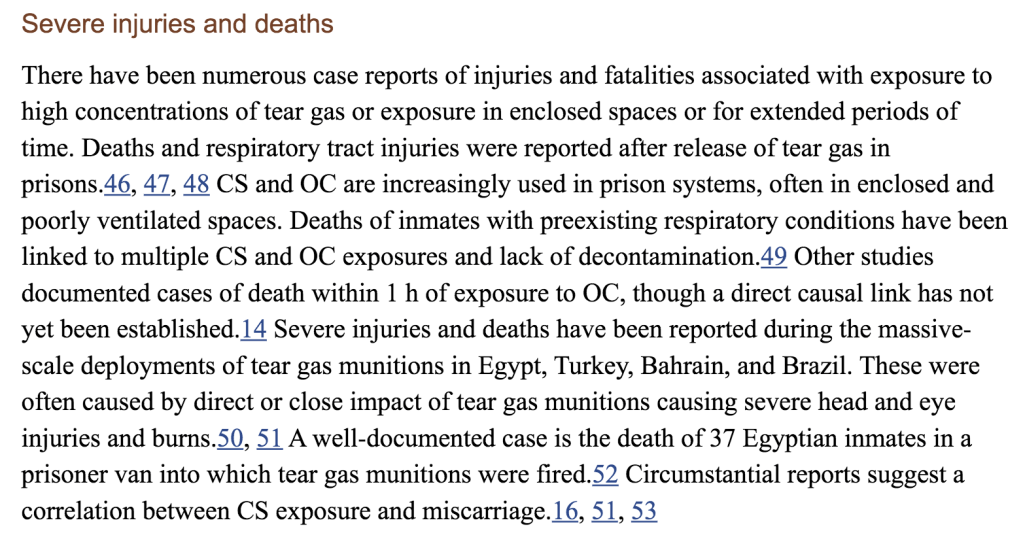
The first is when they are used against individuals with preexisting respiratory conditions such as asthma and COPD, or other medical vulnerabilities, or in situations where proper ventilation and detoxification is not provided. An in-depth 2016 review of the epidemiology of tear gas exposure in the Annals of the New York Academy of Sciences provides the elucidative paragraph below. Of course, when you are firing into a crowd, you are by the nature of that act targeting people indiscriminately, without regard to their personal risk factors or able to offer individual aftercare to those who have suffered more severe injury.
But the second situation where these weapons are extremely dangerous is, as you might have guessed, during a global pandemic caused by a deadly respiratory virus. My most recent blog post discussed the difficulties of gauging the degree of asymptomatic transmission; we know it happens, but we don’t know how often. Part of the difficulty is that the virus is spread primarily through respiratory droplets, so while the viral load is sufficiently high in asymptomatic carriers, the mode of transmission is less well understood. When tear gas and pepper spray are used against peaceful protesters at the height of the COVID-19 pandemic, symptoms that spread respiratory droplets, like coughing and sneezing, are induced and the asymptomatic and presymptomatic among them are themselves weaponized. And the injuries caused by this weaponization, unlike the use of rubber bullets and tasers and police batons that injure or maim or kill only the intended target or bystanders, has the potential to spread to the family members, children, parents, and grandparents of those affected.
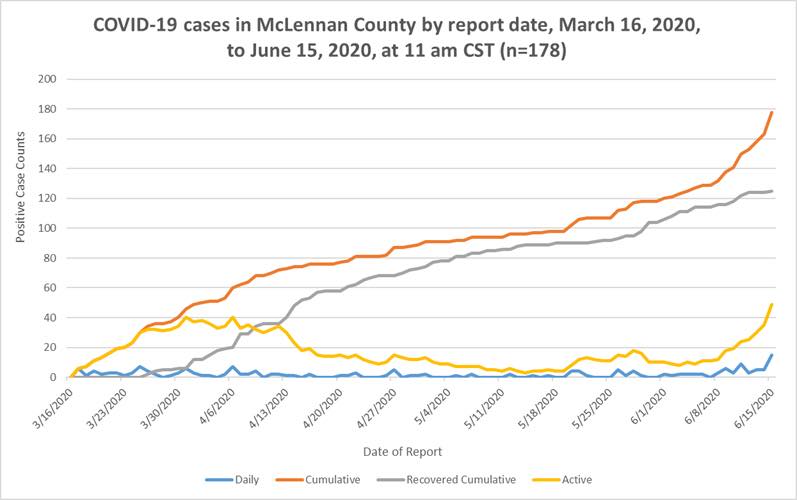
As I write this, our city has had the highest number of new positive COVID-19 cases in one day that we have had at any point in this pandemic. We seem to be entering the first true surge we have experienced here in Texas, and this is mirrored in various cities and states around the country. And while individual protesters and organizations continue to be faced with the very difficult decision of how to balance safety during a medical crisis with their desire to advocate for systemic changes that will lead to long term justice, the police departments in those various cities, with their personal respirators and canisters of tear gas, seem to have decided that using the terror of the pandemic is not outside the scope of measures that they are comfortable with.
But aren’t they at least better than guns?
This is the question I am really wrestling with today. The mortality rate for an assault with a firearm dwarfs all of the above agents and tools, and so it seems very reasonable, on the surface, to be thankful that the law enforcement agencies and officers engaged in these actions were armed with these not-as-lethal-as-guns weapons instead of with guns alone. It is conceivable that instead of hundreds of minor and dozens of major injuries from over a week of police using these various devices against protesting crowds, we might see dozens of deaths and hundreds of major injuries after just a single attack with firearms. One of the core questions we have to ask ourselves is whether the use of these weapons, as part of arming police forces as though for war and sending them en masse to confront groups of non-violent protesters, contributes to a sense of anonymity and freedom from culpability that lowers an officer’s threshold for escalating such encounters. We have seen video after video where police officers dressed in full body armor take sudden and aggressive actions against crowds ranging from the fairly unruly to the utterly non-violent to medics and priests. Perhaps if they had been armed only with firearms, the realization that every life they fired upon would be forfeit, every citizen they attacked a casualty, would be enough to give greater pause before lashing out at non-violent protesters or using their weapons as tools to enforce obedience to the wills of their superiors.
Or perhaps that is a naive and privileged hope, built upon a lifetime of not even being able to imagine a police officer ever shooting me.
Regardless, it is clear from medical research that these weapons are weapons indeed. They cannot be merely dismissed with a wave of the hand as though the damage they caused were transient or their potential to kill negligible. When used in a situation where the only other choice is a deadly weapon, it is likely enough that they represent the most merciful option. But when law enforcement officers use them against those who have committed no crime, have offered no violent resistance, have in fact merely expressed their right to assembly to protest the murder of yet another unarmed black man through excessive and particular police brutality, they represent an unacceptable risk to the public that those officers have sworn to serve and protect, and demonstrate the very calloused disregard for human life that have triggered such protests in the first place.
