
Over the weekend I had several viral medical misinformation videos sent to me, but I chose not to focus an entire essay on any of them for various reasons. One was a nurse speaking at a re-opening rally in Raleigh, North Carolina about empty hospital rooms and postponed surgeries. We’ve talked about healthcare systems being slower in pre-surge areas due to mitigation efforts a good bit in prior blog posts, and since the actual content of her comments were relatively straightforward and could be as easily interpreted as praise for social distancing measures as criticism, I decided it didn’t necessitate and entire post. Another was an interview with Dr. Jeffrey Barke, a concierge medicine doctor in Orange County, California who had recently spoken at a re-opening rally there. While there were a few medical issues he raised that deserved some response (bringing up hydroxychloroquine again, failing to distinguish between the medical realities in pre-surge areas vs. those more heavily effected), his comments were primarily politically rather than medically oriented. Finally, there was an immediately debunked video of Bill Gates briefing the CIA on his plan to release a respiratory virus, and then give a vaccine for it that would actually modify people’s brains to make them hate religion. Which, I mean, come on America. Really?

Instead, what caught my interest is the following letter to President Trump, signed by 600 doctors.

The remaining 8 pages are a collection of signatures from, presumably, over 600 other doctors. The letter itself was written by Dr. Simone Gold, MD, an ER trained Physician in California who now does concierge medicine as well. It is part of her A Doctor A Day campaign and has been featured on Forbes, Fox News, Breitbart, etc. and circulated widely on the internet. Today I would like to focus on the parts of this letter I agree with, for there is much to agree with, and then explain the one great error I believe Dr. Simone is making. But first, we should address a few preliminaries.
Signed by 600 Doctors
When reading a letter like this, the temptation is to get dragged into those last 8 pages and try to address the motivations, credentials, and biases of the doctors signing. Certainly, with 600 signatures this becomes an investigatory nightmare, but I believe it would be a profitless endeavor even with a more manageable list of names. When a doctor shares blatantly erroneous data, like Dr. Erickson and Dr. Massihi, or a scientist promotes false claims and conspiracy theories like Dr. Mikovits, a closer examination of motives is warranted. But unlike those viral videos, there is as far as I can tell no false medical information contained in this letter. This is a position statement, and while some individual co-signers may have their own political or financial motivations, I earnestly believe it is best to take the stated motivation of advocacy for individual patients and our population as a whole at face value.
That said, I believe we can make some general observations, and to do so I will bring you thought my own process when confronted with this list of names.
First, I checked to make sure my own name wasn’t listed. I don’t remember signing anything like this and don’t believe I would have, but arguing against the letter and then finding out my name was on it would be the most embarrassing (and funniest) complication to my opposition that I could think of.
Second, I googled a few of the names. Now nearly 3 months into fighting against medical misinformation in a more formal and deliberate way, I have learned to be surprised by less. I didn’t think anyone would make up 600 doctors to support their letter, but wanted to make sure. I only chose a handful at random, but they were all real life people.
Third, I read about a few of them. The first doctor I looked up had his medical license revoked 20 years ago. Oomph, rough start. But the next practices Family Medicine in California, another is an Ophthalmologist who does LASIK eye surgery, and the one after that is an Emergency Medicine doctor in Connecticut. As I googled a dozen or so names I did not find anybody practicing Emergency or Critical Care medicine in New York, and didn’t really expect to (though maybe there are a handful on this list); but that first doctor who isn’t allowed to practice medicine anymore seems to have been a funny coincidence, and overall it seems that these are, by and large, real practicing Physicians in various specialties around the country. I can in no way vouch for or against their personal experiences with COVID-19, their level of experience or skill as clinicians, or their political views.
Finally, I looked over the list itself and reflected on the numbers. A few Dentists and PhD’s, a few people listed without any credentials, but mainly MD’s and DO’s; Doctors of Medicine. I made a quick scan to make sure there wasn’t anybody I knew, which could get awkward. There are over a million doctors in the United States, as Dr. Gold’s website points out, and here we have 600 names. No doubt there are many, many more who would sign such a letter. If you are trying to google individual names or even just scrolling through, it seems overwhelming; but it’s actually a relatively small group. I am part of one COVID-19 Physician and NP/PA group on Facebook with 150 thousand members, and a Critical Care COVID-19 group with 33 thousand members. The discussions there are focused on treating and preventing the illness, the most recent studies, transmission control strategies, and review of treatment protocols. While many of us are also very concerned about the secondary effects of the virus, such as the complications of isolation and distancing, I have seen no posts and very few comments saying that the whole thing has been overblown. I could not say how many in those groups would or would not sign the letter above, but the idea I am trying to get across is that 600 doctors in a country the size of the US is a fairly small sample. When taken as a whole this letter really does seem to represent a minority opinion, as the website itself alludes to.
A Doctor A Day
Dr. Gold’s personal website, drsimonegold.com (can you believe she used her name as her website url? The arrogance), currently redirects to A Doctor A Day, which almost -but not quite- admits to it’s goal of offering a minority, dissenting opinion of the importance of mitigation strategies in fighting COVID-19. It begins with the following text:
The numbers here send a bit of a mixed message, don’t they? On the one hand, they clearly would like to contrast “ONE opinion” with both the million licensed physicians and the thousands of physicians who have something to tell you. But a straightforward reading is maybe too honest by half; there are nearly a million physicians who seem to be expressing one opinion, that COVID-19 is very dangerous (that’s called a consensus); but thousands of doctors want to give a second opinion, that it isn’t dangerous enough to justify the steps we’ve taken. I’m being quite facetious here, of course, but I do think that they are trying to have their cake and eat it to by implying both that the views of doctors are varied and nuanced, and that the doctors who agree with them are thinking independently while the rest of us are towing the party line and sharing “just one opinion.”
That’s why the second opinion part is what really gets to me, because it so clearly implies that the views expressed by A Doctor A Day are not also being expressed by other physicians who nonetheless support mitigation measures. And that simply isn’t the case. I’ve yet to meet a doctor who isn’t aware of, concerned about, and talking about the potential for secondary harms due to social distancing and quarantine strategies, and the ones I know are working very hard to mitigate those harms. I’ve personally been talking and writing about it since early March. In fact, recognizing how much more vulnerable our patients are in the midst of a pandemic has been a core reason for the mitigation and social distancing measures since day one, because an overwhelmed healthcare system has even less ability to care for patients with chronic illnesses and mental health conditions than a reduced capacity healthcare system.

The A Doctor A Day campaign is promoting a narrative that says the many, many physicians and other healthcare workers encouraging ongoing social distancing and quarantine measures and extreme caution with reopening have simply not thought of, or have refused to acknowledge, the difficulties that those measures create for our patients and our communities. But their second opinion is already contained in the first; it has been weighed carefully, it has been felt deeply, and in the face of a hundred thousand lives lost and who knows how many million in the balance, most of us have found the danger still too great to abandon our fight against the virus. The opposite cannot be said; the doctors vocally forwarding this alternative perspective have been strangely reticent to acknowledge how bad the virus really is, sometimes even leaning on ‘inflated death numbers’ and other misinformation to lessen the reality of what we are facing.
The Videos

Besides the homepage and the letter, the main content is a series of videos featuring interviews with Physicians who talk about the damage and potential damage being done by shelter-in-place orders and social distancing. They run about 5-10 minutes long each and so far there are four, though the link for one seems to be broken. Interestingly, some of the interviews are conducted by Dr. Jeff Barke, who seems to be a partner on the project. There are some problematic moments, mostly in the form of leading questions such as when Dr. Gold asks one Physician how he kept his office open when ‘we have heard from around the country that most patients can’t come see their doctor’, without offering any evidence that this is the case, or when Dr. Barke asks a Cardiologist about caring for Congestive Heart Failure patients when ‘they can’t get Echocardiograms’, which also doesn’t seem to be the case. But these doctors being interviewed sort of hedge on those questions, and mostly they spend their time expressing their concern about the potential negative health effects of mitigation strategies on their patients, like most of us would, and the things their clinics are doing to compensate. I think a video series like this invites comparison. Consider this video from Dr. Mike, who does a handsomer and more successful YouTube version of what I am trying to do on this blog.
The most striking thing to me about these videos is that the doctors from both sides of this discussion seem to be genuinely and primarily concerned about the well-being of their patients. Which shouldn’t be a surprise if you know many physicians. The second thing I notice is that it doesn’t seem hard to get doctors to tell you about their experiences during the COVID-19 pandemic; a contest of who can make the most videos or recruit the most signatures isn’t likely to be helpful, which is why it’s important we look closely at the arguments themselves.
The Letter: What I Agree With
I wrote about treating COVID-19 like a nation-wide mass casualty event back in March, and in many ways I agree with Dr. Gold’s concerns. Faced with such an overwhelming medical reality, one of our first goals has to be to ensure that our vulnerable patients “do not deteriorate a level.” As a primary care physician caring for patients who often have limited access to specialists and treatments at baseline, I and my patients have had to be especially deliberate and strategic about caring for their conditions during COVID-19 while the medical system is even more challenging to navigate. Many of my patients lived pre-COVID-19 in what Dr. Gold describes as ‘triage level red’; poor or no access to cancer screening, unable to afford dental care, not having access to Psychiatry for ongoing and often overwhelming mental health issues. The list could go on; patients with seizures who can’t see a neurologist, those with CHF who can’t get an Echo, not because they aren’t being scheduled right now, but because they cost $2,000. Diabetics whose control has worsened because their insulin prices suddenly skyrocketed in the name of profits. If these doctors are going to advocate for patients who could normally have these services done but might not now because of COVID-19, they should also be advocating for the patients who have never had access to these services and thus live and die in triage level red. Maybe some of them are advocating for those patients; but they all should be, and if they are willing to sign this letter to the president out of that concern then all 600 of their signatures should be on the next petition to improve healthcare access for all.
But COVID-19 is the reality right now, and regardless of the individual examples (it is a hard sell to prove, for instance, that a hip surgery would have reduced someone’s risk of a pulmonary embolism), I have seen many situations similar to the ones they mention in the letter, and some have indeed been made worse by COVID-19; both by fear of the very dangerous virus itself and by the disruptions to ‘normal’ life rhythms and support structures, financial difficulties, and loss of community. I do not have to imagine those stories from the initials and brief vignettes in their letter; I have the names and faces of all of my own.

We all do. Every physician and clinic I know is involved in combatting this, not to mention ministers and priests, social workers, mental health workers, and teachers. I feel like a broken record when over and over again I have to share the changes my own clinic has made to create safe access for patients; seeing patients outside in their vehicles to decrease transmission risk, rapidly building and implementing telephone and video visits without any precedent or prior infrastructure for using those tools, designating COVID-19 testing and treatment sites to keep sick patients and vulnerable patients from putting one another at risk, and all of the individual and corporate work and stress that goes into examining and upending every single protocol and procedure you have used for years. We do all of this because as hard as we worked to ‘flatten the curve’ in March and April, and as loud as are being about preventing a second surge now, we are also worried about that third surge, and are working hard now to flatten that curve, too. The balance of each of those threats has to be weighed in deciding when and how to return to our ‘normal’ routines, if such a thing can even exist again.
Mass Casualty Event
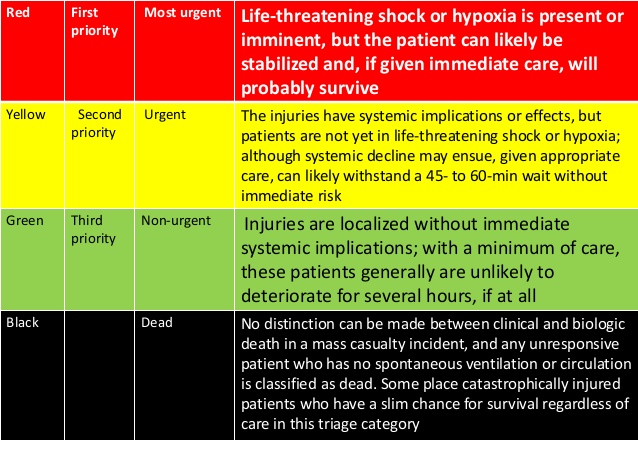
Finally, I want to return to Dr. Gold’s central analogy of COVID-19 as a Mass Casualty Event. A mass casualty event is a situation where so many are injured that the available resources could not possibly care for everyone who needs care. This is the Oklahoma City Bombing, or 9/11. Dr. Gold is right, that in a ‘mass cas’ the most important first step in caring for the injured (besides safety, of course), is an effective triage system. She talks about the color-coding system we use for these types of events, and I think it’s worth studying for a few moments. I’ve provided a couple of different representations, because I want you to understand just how different a mass casualty event is from the normal way we practice medicine.

To the untrained eye, it looks like these diagrams are used to train doctors and other medical professionals to triage patients. But they aren’t. Triaging patients is not a difficult concept, but it does take some time to master. Sorting out those that need immediate attention from those who can safely wait is a skill that is taught early and honed daily. You do this in every context of medicine almost all day long. It is most obvious in the hospital and the ER, when your visit with a sweet older lady recovering from pneumonia is suddenly cut short by sudden shouts from down the hall or a Code Blue over the speaker. But it also happens in clinic, when you hear the crash of a walker in the waiting room or notice that your 2:45 PM “Arthritis recheck” is now listed as having a chief complaint of “Chest Pain,” or your 9:15 didn’t come to clinic even though you know he’s been severely depressed. We triage in our minds constantly, and Mass Casualty is a specialized enough field that our training in it typically comes after we have already been triaging in our minds constantly for years.
These tables are not for training us how to Triage. They are for re-training us how to Triage in a way we are very, very uncomfortable with. They are, in a way, un-training us.
Think about those categories, and what they mean. Green means that person gets none of my time or attention; even with injuries, even having suffered trauma. People I might otherwise spend an hour with talking through their experience and tending their wounds, I deliberately re-route and ignore to get to sicker patients. Yellow is someone who has urgent needs, who probably needs care within the hour. In the ED this would be considered a very ill patient, and someone who is going to get immediate attention; in a mass cas event, they are set to the side because the sicker, red patients need attention now, and the resources are simply too limited. Finally, think about my examples from the hospital, and look back at those tables one more time. Notice black: “Obvious death,” “Non-survivable injury,” “Cardiac Arrest.” Normally if you are running through your continuous mental triage and suddenly find a patient in cardiac arrest, requiring chest compressions, intubation, and defibrillation, that patient becomes your highest priority. Your time and resources are devoted to that individual for as long as it takes, as long as there is a chance. In a Mass Casualty Event, those patients are left for dead.
This is why we do specialized training in mass casualty; this is why we have to study and internalize and accept a triage system that is alien and even repulsive to our oath as physicians and every carefully fine-tuned impulse of our professional judgement. Because the idea of allowing an untimely death that might have been prevented is so terrible to us that it requires a drastic shift, on some level, away from how we’ve trained and even who we are as physicians.
The physicians who wrote this letter are advocating that life return to normal. They are advocating for this from a noble enough sentiment; concern for the well-being of those who they consider to be at Red, Yellow, and Green levels of risk right now. But just as in every mass casualty, their call to shift our standard of care and give our full attention to those groups by abandoning transmission reduction strategies necessitates allowing some to die who might otherwise have lived. This ‘black’ group that should be forsaken, who in the letter’s own words “require too many resources to save”, are the excess dead from COVID-19, who might have been spared by “reopening” with more caution, more national sacrifice, more people-centered policies, and more patience.
Nowhere in their letter do they mention the 100,000 we have already lost, or the thousands more still fighting for their lives. Nowhere in their letter do they mention the suffering of those families, the sacrifices and risk of their caregivers, or the fear of those exposed. Nowhere do they mention the mental health burden inflicted by the virus itself on all those who come in contact with it. All of these should be crucial factors in our decisions about when and how to decrease mitigation efforts. But if you are going to lead a mass casualty response, I guess you have to be willing to walk past some who are dying and force yourself to live with the fact that you had the skills and the tools to save them, but didn’t. The majority of physicians, myself among them, seem to think that we haven’t reached that point yet; that as a society we can continue to protect one another and the vulnerable among us from COVID-19 and still devote time and energy to keeping others from ‘deteriorating a level’ while we fight it, by rethinking the ways we deliver care and support our patients and communities. Maybe that’s typical physician hubris, and maybe the second opinion offered by Dr. Gold and her colleagues is the only real option; to shift our focus to the ‘survivors’ even if it means giving this virus another 100,000 lives, or more. But I don’t believe that’s where we are, and I know it isn’t a decision we can make without counting the unimaginable costs very, very carefully.
