A physician friend recently brought to my attention the First Trust COVID-19 Tracker, a weekly 1-page document released by First Trust, a Wheaton Illinois based blog on *checks notes*… Financial Advising? Ok, that’s fine; COVID-19 has affected everyone in profound ways, and if a financial blog wants to use its resources and time to share important information about COVID more power to them.
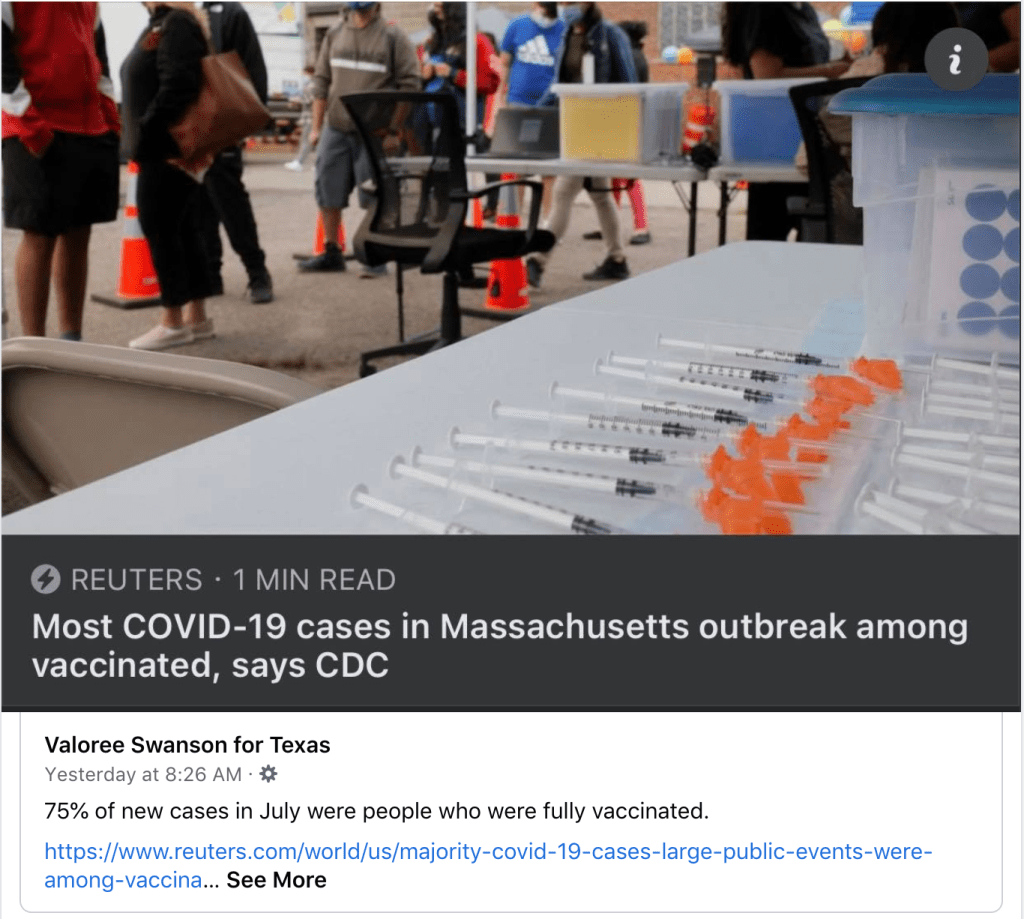
The fact that my friend lives in Texas and is being confronted with this information on a weekly basis does raise concern, however, specifically on the questions of source authority and nitpicking data and sources. Throughout the pandemic we have seen people spread misinformation from non-medical, non-scientific sources far removed from their actual location for the simple reason that they had to look far and wide for data that seemed to support position when the data for their own hometown did not. We saw this on a large scale with the Massachusetts Outbreak in August, which people all over the country pointed towards as proof that the vaccines were ineffective, at the same time that they wouldn’t be able to get an ICU bed in their own city because of the surge of unvaccinated hospitalizations for COVID. There may well be a perfectly legitimate reason that this individual in Waco Texas uses First Trust as their go-to source of COVID-19 information. Many blogs have followers from all over the world (or so I have been told); maybe they have followed the First Trust blog for years and it was already a resource they trusted prior to the pandemic, or maybe they like the attractive layout and graphics. But when someone ignores their local county health department’s COVID-19 dashboard in favor of a weekly COVID tracker from over a thousand miles away (trust me; I drove all 1,000 of those miles a few weeks ago), we do have to stop and ask, “Why? Why look so far away?”
There are some things I definitely likeabout the First Trust COVID-19 Tracker. First, it really is a lovely document; the layout and graphics are eye catching and superb; if I were creating COVID-19 statistics handouts for social media I would want them to look just like this. More substantially, there is nothing overtly partisan about the presentation. We will exam the way that First Trust has selected and chosen to present their data, which is either intentionally or unintentionally misleading at times; but it is data, not conspiracy theories or outrageous lies, and they even include some of the data that weakens their evident position. In that sense it is sort of a breath of fresh air. My overall impression of the First Trust COVID-19 Tracker is ‘bias but honest’, and it’s hard to say how much of the misrepresentation of the information is deliberate vs. accidental; I personally believe it’s mostly the latter.
With the pleasantries now dispensed, let’s take a look at the COVID-19 Tracker segment by segment.
Hostile Behavior over COVID-19 Safety Measures
The inclusion of this data on the hostile behavior experienced by service industry workers over masking and other virus safety measures is the earliest evidence we have of the essentially honest intentions of the writers of the First Trust blog. The fact that hostile and belligerent behavior over masking and other safety measures is so widespread certainly paints a negative picture of those who are opposed to such policies, yet these will by and large be the same people that follow the COVID-19 information put out by the First Trust blog. It meets the criterion of embarrassment and speaks to at least their intention to take a balanced stance.
I realize that there is at least one other possible interpretation, but it’s so cynical- and so transparently flawed- that I wasn’t willing to lead with it. They could be saying, “look at how these masking and social distancing measures have resulted in violence and hostility towards people in the service industry! We need to end these mandates so that people don’t have to experience this hostility any more!“ If you find that argument compelling I’m not really sure what I can tell you. It seems blaringly self-evident that the responsibility for deciding to respond with hostility, intimidation, and violence towards employed individuals simply enforcing the policies of their state, city, or place of business rests solely with the person choosing to respond that way. Placing the blame on the policies themselves and absolving those doing the bullying of any culpability is obtuse in the extreme, and while I am sure some of their readers will take this data that way, I don’t really think it’s what First Trust meant in including this data.
I know people who are against masks and social distancing; I even know and love people who feel persecuted when they are asked to wear a mask (and tell me so, forgetting that I was wearing a surgical mask for hours a day to protect people against pathogens long before the COVID-19 pandemic). Those folks are wrong about masks being dangerous or ineffective, but I don’t for a minute think that they are out there in the world bullying waiters and cashiers over it. But the data shared in the First Trust COVID-19 Tracker shows that somebody is. So if you are one of those folks who are against masks and you happen to be reading this; here’s the take home message from this section of data; get your people. When you see this behavior occurring, don’t cheer it on or be a passive bystander, intervene. As an anti-masker yourself you may have a unique voice to de-escalate a situation where someone who shares your views is acting out towards somebody who is just doing their job.
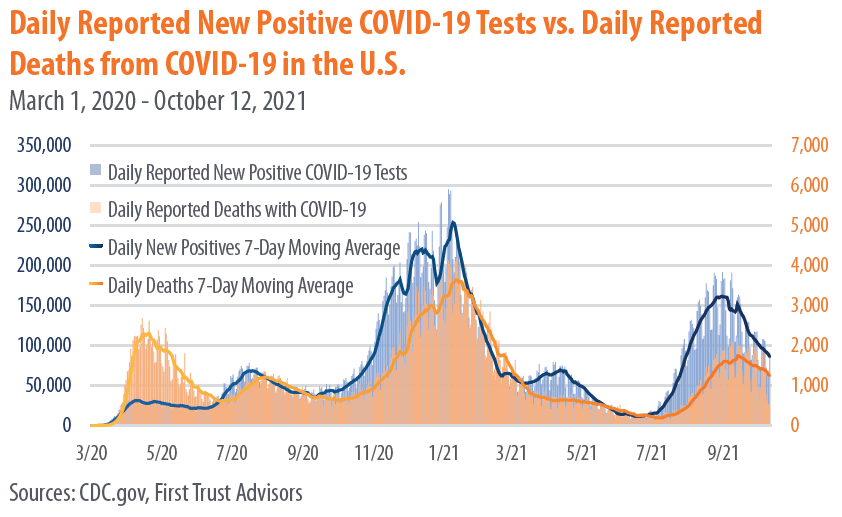
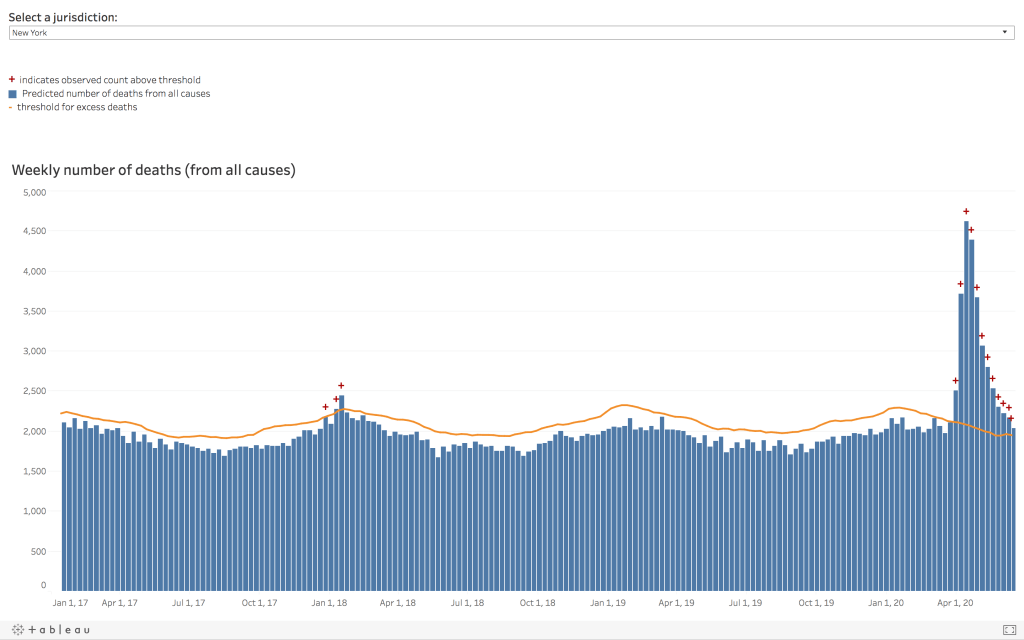
New COVID-19 Cases and Daily Deaths
There’s nothing to criticize here, this data was clearly taken directly from the CDC and demonstrates that we are still very much in the middle of a deadly pandemic. Over 2000 Americans died yesterday from COVID-19, and we have now surpassed 728,000 deaths from the virus less than 2 years.
We are so used to seeing this graph, or something similar, that we have become numb to the enormity of this pandemic, and our tendency is to skip right over it and look for other data that either confirms or contradicts our position. But if there are still people out there claiming that the pandemic is exaggerated and that the virus is basically as deadly as the flu (and there are), then it’s worth pausing to look at this data.
Yesterday 2,011 deaths were recorded from COVID-19. The day before that it was 1,890. Each day in the US an average of 1,805 die of heart disease, and about 1,600 from cancer. The way that deaths are reported means that those 2,011 deaths represent people who died sometime in the preceding couple of weeks, and the people who will die tragically from this virus today will be represented in that data up to a few weeks from now; statistics can’t be reported instantaneously. So it’s most accurate to think of these as averages over time, and based on this we can see that more people are still dying from heart disease and cancer each day, on average, than from COVID-19. But it’s really, really close. And the fact that our healthcare system is stressed to the breaking point by the number of primarily unvaccinated people with severe COVID-19 symptoms means that both heart disease and cancer, and every other illness, are more dangerous now because patients are so much less likely to have access to the are that they need.
Again, we need to recognize that including this data is more evidence of the desire for fairness and balance on the part of First Trust. They didn’t have to include this, and many of the memes, blogs, and videos we have seen spreading misinformation over the past year have deliberately used outdated information and statistics from early in the pandemic, before it had spread significantly in most parts of the country, to ‘prove’ that COVID-19 isn’t dangerous. This data shows how dangerous it really is, and those who use the First Trust COVID-19 Tracker to prove otherwise need to take a closer look at their own resources.
Vaccines Administered by Type
Again, nothing controversial here; this matches the data I have. I’ll just add that the now 409,438,987 doses of COVID-19 vaccines given as of today represents 57.5% of the US population, which is encouraging. We should see that number skyrocket soon, once the vaccines are approved for children ages 5-11. My two oldest will be first in line, and my 3rd, who turns 5 this winter, will be right behind them.
Mask Usage vs. Daily Positive Tests
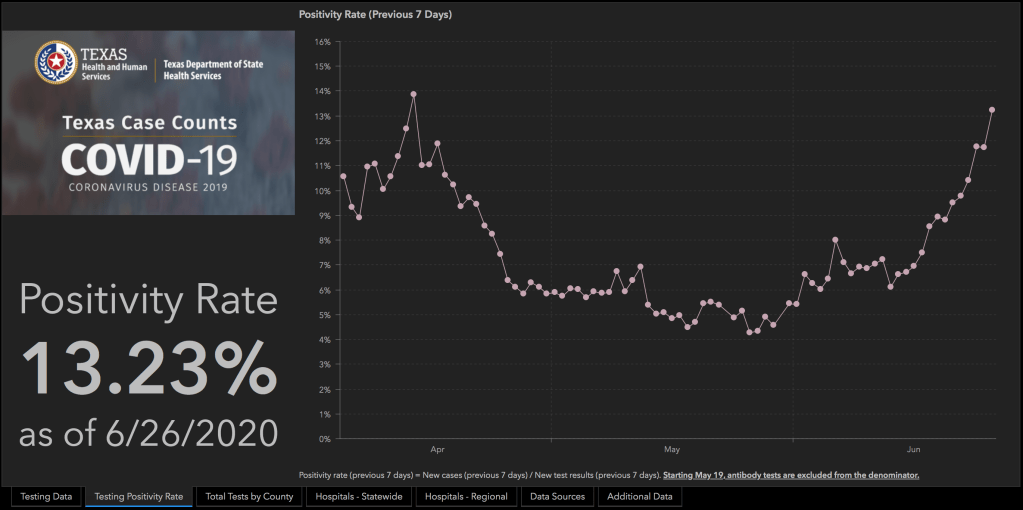
All good things must come to an end, and this is the point where the data presented in the First Trust COVID-19 Tracker begins to drift towards the highly suspect. Take a moment and look at this graph, and ask yourself whether the numbers you are seeing seem right to you.
Statistics are not always intuitive. The fact that meticulously collected and cautiously interpreted data transcends the limited observations we have to draw from in our own realms of experience is the reason they are so powerful. Sometimes our own circles or spheres of influences are outliers, and data from a wider selection of the population upends our expectations. Nevertheless, when a piece of data is so contrary to our experience that it actually seems impossible, we need to at least pause and consider the source, how it was collected, and what it means- good habits to get into with all data, to be perfectly honest.
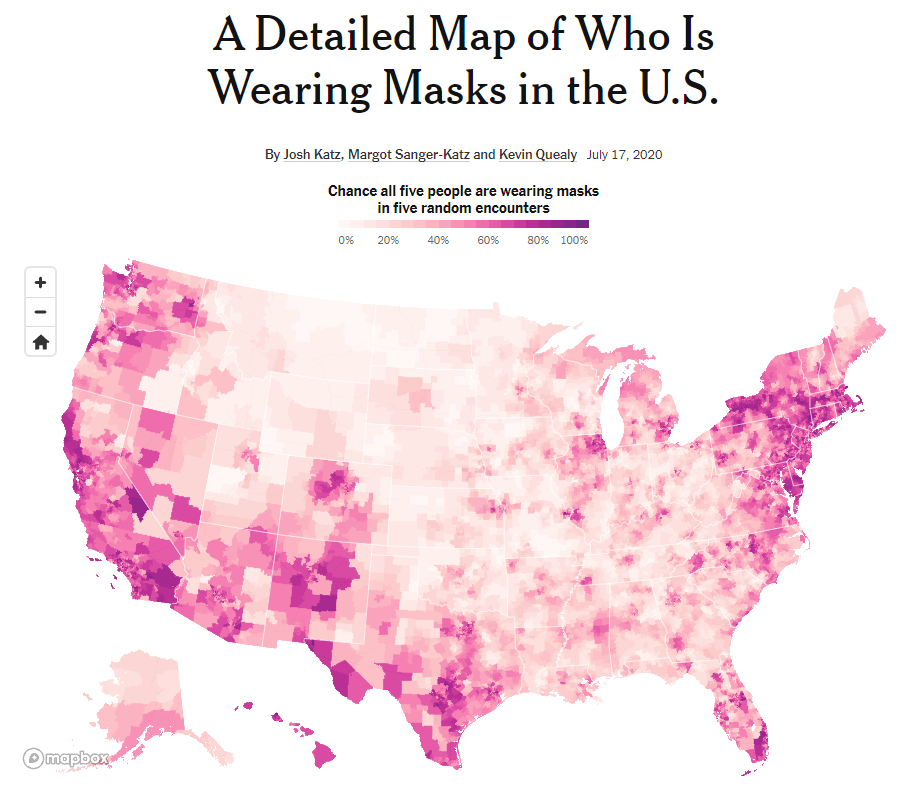
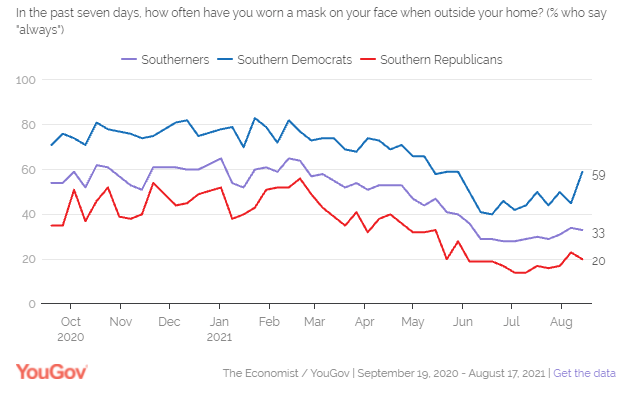
If you live in Texas (as I did until very recently), what might jump out at you from this data is the idea that up until May 70-80% of people were wearing masks indoors consistently when they left their homes.I’m not sure if you’ve been to the grocery store in Texas recently, but that number seems… High. Without a statewide mask mandate, I have frequently been inside of a place of business where I was the only person wearing a mask, and at best the numbers seem split about 50/50. Again, my personal experience might not be normative; we have to look at the data, which in this case comes from YouGov.com online poll data.
You may live in another part of the country (like, say, the suburbs of Chicago) and are saying to yourself, ‘no, that looks about right to me.’ And the reason is pretty simple; the USA is not anywhere close to a homogenous society, and health behaviors around COVID-19 are subject to dramatic regional differences, both due to and apart from varying State and local regulations.
Why does it matter? It would be easy for someone to look at the data from the Mask Usage vs. Daily Positive Tests graph from the First Trust COVID-19 Tracker and come to the conclusion that mask wearing is generally high in the US (close to 80% throughout the Winter) and that it makes very little difference in the ebb and flow of the pandemic. As you look towards the Summer of 2021 this illusion breaks down a bit; there is a definite drop in mask wearing prior to the Delta Variant surge beginning in mid-July. But because this data ignores the regional differences in mask wearing, it is telling a very one-dimensional version of the story; we also need to ask where the cases have been high, and where mask wearing has been prevalent. YouGov.com has some data that helps with this, even though the graph shown in the First Trust COVID-19 Tracker isn’t one of them. For instance, at the end of August, during the peak of the Delta Varint surge, only 33% of Southerners stated they consistently wore a mask. Yes, that feels much more like the Texas I know and love.
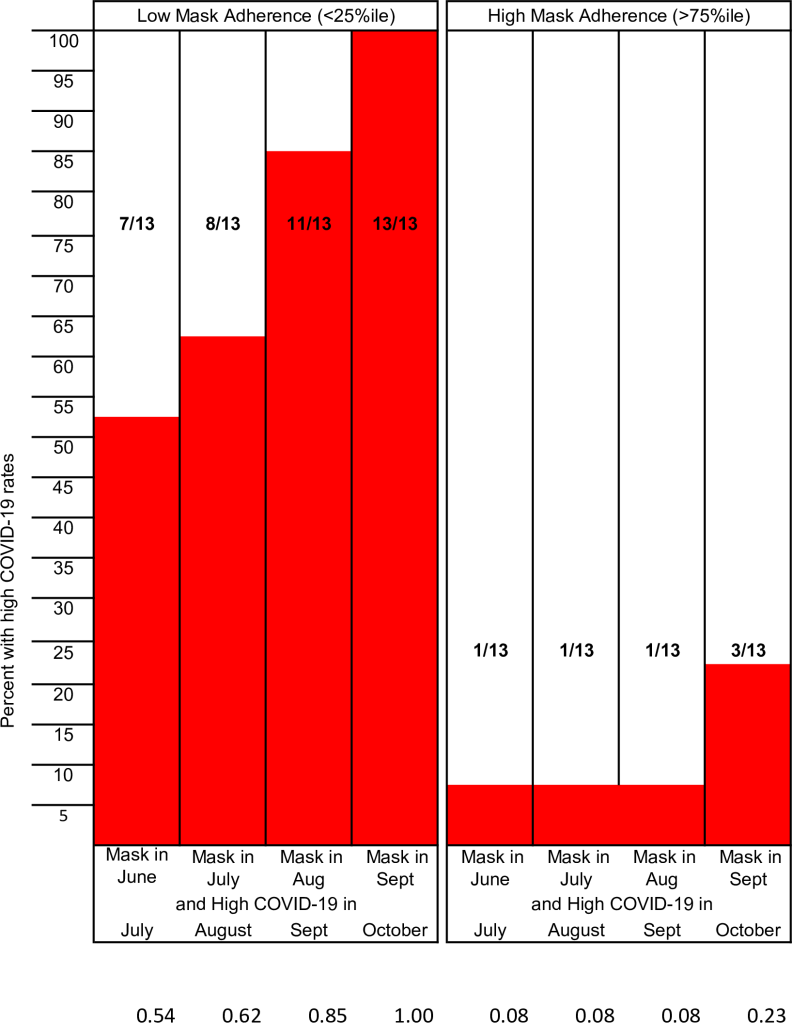
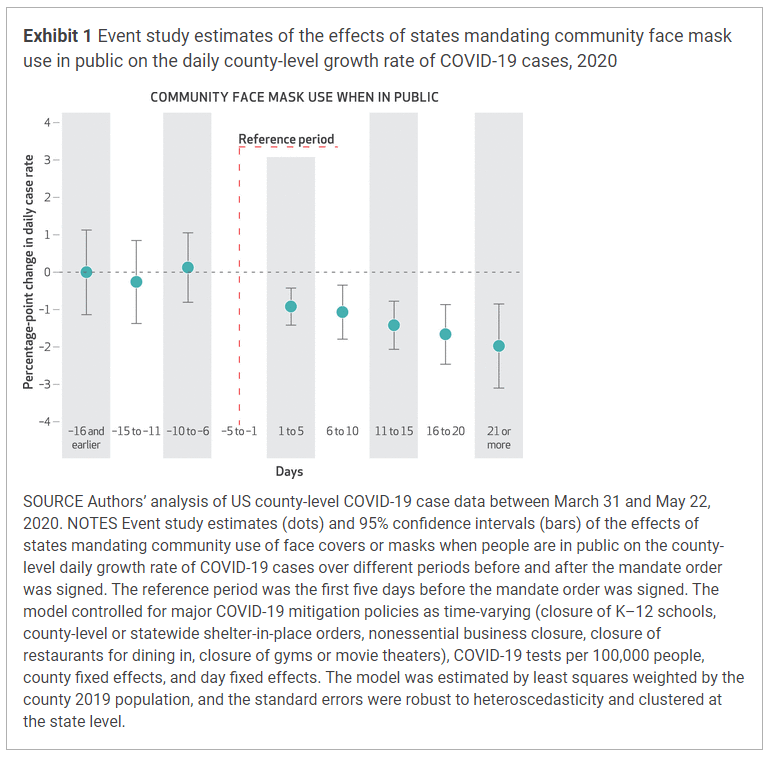
It’s a challenging question to study because demographics and climates vary, and surges are affected by not just state residents but also visitors and tourists and the people living in surrounding states. But there are studies that have done the work of comparing the rate of COVID-19 cases to adherence to masking at the state and local levels. The methodologies have been different, but each has shown what we already knew from comparisons between nations with varying mask policies early in the pandemic; in regions where mask adherence is high, COVID-19 cases are lower. And in regions that adopt mask mandates or similar policies, COVID-19 cases begin to fall.
It’s impossible to fully tease out the effects of different behaviors that commonly occur together. People who are more likely to wear a mask at the grocery store are also more likely to eat outside whenever they can, to stay home from work when they feel ill, and to generally treat the pandemic with more caution in order to protect themselves and those around them. And though human beings are complex and nuanced in their actions and behavior, it’s still fair to say that in general those who do not believe in masking are also less likely to observe other mitigation measures as well. The question of percentage wearing a mask helps vs. what percentage coughing into your elbow or eating outside helps will probably never be answered with a high degree of precision; but they don’t really need to be. The point is that these efforts do prevent infection and death from COVID-19, especially when done together, and especially when used in conjunction with widespread vaccination.
Flu Vaccine Effectiveness
I’ll be honest, I have no idea why this graph is here. It is approaching flu season, so maybe First Trust wants you to see the importance of getting your flu shot? Or maybe they don’t want you to get your flu shot because it is never 100% effective? I don’t really know. If you want to read more about the differences between COVID-19 and Influenza, and why Influenza has been so unpredictable since the pandemic began, I have an article on that here: What Happened to the Flu? (Hint: It’s not because doctors are ‘changing flu cases to COVID’).
Duration of Immunity from COVID-19 Vaccines
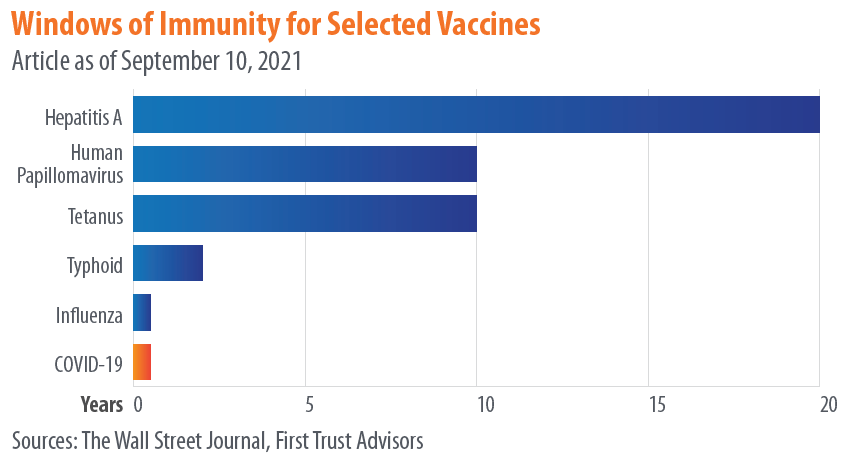
We saw earlier how the comparison between mask wearing and COVID-19 cases juxtaposed data in a way that obscured rather than elucidated the relationship between masking and prevention of COVID. It told a false narrative, sure, but using real and related data, just data that was too generic to actually draw conclusions from. This is the first example of what I would really call misinformation, and it falls under the category of comparing apples to oranges.
While I applaud First Trust for listing their sources, the problem is that their manner of referencing doesn’t actually allow to get back to primary data. They list their source for this data as “The Wall Street Journal,” without listing a specific article. When you find the article on the Wall Street Journal, they just have the same exact chart up but instead list their source as “The CDC,” again without linking to any specific publication, announcement, article, or study. Why not just list “The Internet” for your source and call it a day guys?
What this graph seems to be showing is not how long you are immune against various infections following vaccination, but how long you have detectable antibodies after vaccination. Calling these “windows of immunity” is highly problematic and misleading (whether it’s being done by the Wall Street Journal or the CDC), because- and I cannot stress this enough- presence or absence of antibodies is not the same thing as immunity.
So much has been written explaining this; here is an article, and another, and another, and another. Antibodies are one of the main, active end-products of your immune response to both infection and to vaccination, but they are proteins, and they do not live forever. Most antibodies will die between 3-6 months after they are created, and then they have to be replaced by newly produced antibodies. If you have been exposed to a virus, either through vaccination or infection, and are then exposed to it later, your ability to mount a robust, effective immune response does not depend on the present of antibodies, but on your ability to make antibodies.
This is determined by a variety of immune cells that your body makes in response to the presence of a pathogen, including plasma cells. An essential strategy that your body uses to fight illness is that it can remember what infections you have already fought off in the past; it doesn’t have to keep circulating antibodies to every disease, but it does keep long-lived cells that can produce a rapid and robust immune response- including the rapid production of massive amounts of antibodies- if you are exposed again in the future. Showing a chart of how long antibodies last has absolutely no bearing on whether or not the vaccines that produced those antibodies will protect you for years to come. Thankfully, the studies that have been done so far give us compelling reasons to believe they will.
Let’s leave aside for the moment the question, which this chart seems to beg, of why someone in Texas is confronting my friend with a publication from Chicago comparing COVID-19 statistics between The UK and Seattle. There may be a very rational explanation, I just have no idea what it is. Why did they choose these locations? And why is it more compelling to this person than data from their own state?
I think there are two impressions that someone might walk away from this chart with (though I would like to add a third).
First, one might compare these side-by-side graphs where the death rate seems to be about 100 times high in the UK, and determine that for whatever reason our risk of death from COVID-19 in America (or at least Seattle) is far lower than in other countries (or at least the UK). The problem with this is pretty clear, and I’m surprised it wasn’t caught before First Trust published this infographic: the graph from the UK shows total death rate per 100,000 people for a selected time period (the UK is currently experiencing a sustained surge of the virus), while the Seattle graph shows the death rate per 100,000 people per day. And that daily rate is an average of 9 months, including months where cases were very low and months where the Delta Variant was causing a significant surge. If you want to get the total death rate for the Seattle graph for that entire time period, you would need to multiply the daily rate by 261, the number of days from January 27th to September 29th.
This would give you numbers like a death rate of 80.91 out of every 100,000 for unvaccinated people ages 50-64, and 467.19 out of every 100,00 for unvaccinated people aged 65+. This is still comparing apples to oranges with the UK numbers (9 months with and without surge vs. 1 month of sustained surge), but it seems like maybe the point is to just make the numbers look small, regardless of what they actually mean. “Hey,” you might think, “it’s less than 0.5 for people my age! That’s not bad!” Except that 0.5/100,000 risk of dying from COVID-19 is every single day and includes the days where there very few COVID cases. It’s important to know what this data means before you use it to inform your decisions about the pandemic.
The 2nd impression you might walk away with is that the virus is very dangerous for people in their 50’s, 60’s, or older, somewhat dangerous for people in their 30’s and 40’s, and not as dangerous for children, teenagers, and young adults. This is absolutely true; age is a huge risk factor. But one of the effects of choosing a daily death rate is that you can get the numbers on the graph as close to zero as possible, to leave someone with the impression that practically nobody has died from COVID-19 which isn’t the case.
When one child dies we call it a tragedy, and it affects the course of their family’s life forever. As a father of four, I can’t imagine what it would be like to lose one of my children. The COVID-19 pandemic has killed 513 children in the US. When a young person dies we call it a tragedy, and their parents, loved ones, and friends are left devastated. The COVID-19 pandemic has killed 3,888 young people. Those 712,930 people who we have lost to the virus all represented lives cut short; live full of purpose, filled with people who loved them. Yes, a disproportionate number of those who have died were elderly, and a disproportionate number of the younger people died had chronic illnesses or disabilities. If you’re here to make the argument that their lives were somehow less valuable, that they were less deserving of a society’s efforts to protect them from the virus, or that it was somehow less of a tragedy that they died from it, you can exit my blog right now and go read something else.
Finally, the third impression you could take from this data (and again, props to First Trust for not trying to alter this data in any way), is just how effectivethe COVID-19 vaccines really are. Whether you are looking at the Seattle data or the UK data, there is a hug difference in the height of those orange ‘not fully vaccinated’ bars and those blue ‘vaccinated’ bars. I’m still not sure why they chose King County Washington, but here’s some additional data from the same county COVID dashboard that produced these graphs.
If you can take one salient, actionable piece of wisdom from the First Trust COVID-19 Tracker, it would be this: the COVID-19 vaccines work. You should go get vaccinated.
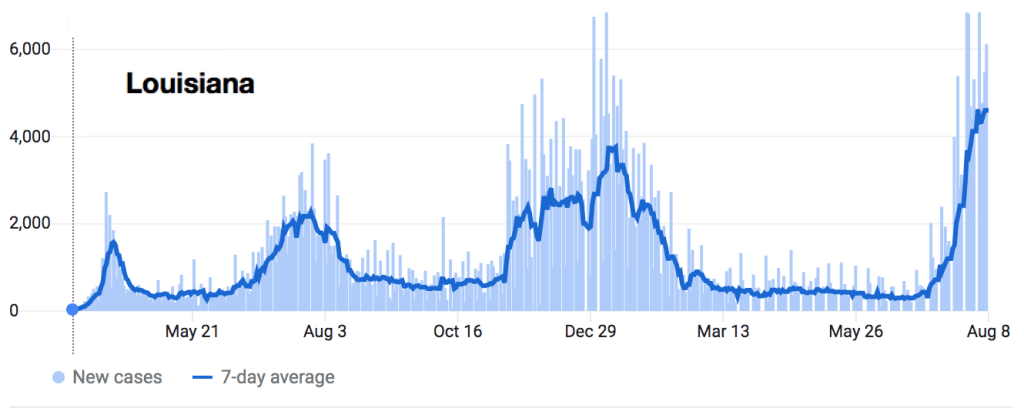
It’s rare for me to be able to muster the time to write two misinformation blog posts in the same month, let alone in two days. Between moving across the country, fighting a global pandemic (still), and the unbelievable amount of take-home work created by practicing Family Medicine five days a week, it’s unfortunately a lower priority than I’d like for it to be. But when friends all over the country send me the same video and a friend in Louisiana, which is utterly overwhelmed by COVID-19 right now, posts it as proof that vaccines are ineffective and dangerous, watching and dissecting the video becomes a higher priority.
For those of you who would prefer a quick 8 minute video in response to this quick 6 minute video, I’ll refer you over to ZDoggMD. We cover some of the same ground and he is much, much more fun to listen to compared to reading however many thousand words I can manage to write this evening.
A few preliminaries. Dr. Dan Stock practices Family Medicine (the same specialty I practice) in Hancock County, Indiana, just east of Indianapolis. Unlike many early medical misinformation sources, he appears to be fully licensed. His website is currently down (no doubt flooded with new patients in the wake of this viral video) so there is no way to know if his practice is evidence based in its approach to science and medicine. His speech here is to the Mt. Vernon school board… Sorry, “Community Education Corporation.” It’s essentially a rapid-fire review of misinformation we have seen shared throughout the pandemic, up to and including the recent misinformation regarding the Massachusetts “Outbreak.”
Many people still see the removal or censorship of any misinformation, no matter how dangerous or how full of lies and half-truths, as proof of it’s absolute validity. I have mixed feelings on taking down these misinformation videos, but since my (self-appointed, unpaid) job is to debunk the videos and my preferred method of doing so is going through them minute-by-minute, I tend to include a direct link to them on my blog posts. It’s the method I personally find most convincing, and that I believe best arms others with the information and insight they need to engage in conversations about viral misinformation like this with their friends and relatives.
The Video: Dr. Dan Stock at the Mt. Vernon Community School Corporation
0:25 “We’re getting our information from the Indiana State Board of Health and the CDC, who don’t read any science.” In my opinion Dr. Stock has severely harmed his credibility here within the first 30 seconds. By stating that the Center for Disease Control, a federal agency comprised of researchers, epidemiologists, laboratory based scientists, virologists, statisticians, experts in every field of biomedical science and physicians of every specialty, and his own state-level department of the same composition “don’t bother to read science,” he is making a statement that is obviously ridiculous. I would submit to you that Dr. Dan Stock does not believe this. He knows that both the CDC and the ISDH read scientific literature, closely follow and analyze epidemiological studies, conduct extensive studies of their own, and in fact maintain rigorous standards of evidence on which they base their recommendations. He knows it, and he could have chosen here to say, as ZDoggMD says about his ambivalence about children wearing masks (an ambivalence I do not share; my kids are definitely wearing masks if we have to take them anywhere right now), that he earnestly disagrees with some of the CDC’s recommendations or conclusions. That is a credible and understandable stance, and many doctors I know have taken issue with some one or another of the CDC recommendations for various reasons. But Dr. Stock chose instead to make a statement he can’t possibly believe because he knew it would be appealing to certain people; the people in the room speaking out against vaccination, for instance, and whether he knew it or not many people across the country who would like to believe that any scientific finding or recommendation they disagree with is simply fake. Saying the CDC “does not bother to read science” is a signal of what team you are on, and nothing more; and it’s an unfortunate harbinger of what is to come in the rest of his speech.
0:39 “Everything being recommend by the CDC and the State Board of Health is actually contrary to all the rules of science.” Again, these blanket statements should begin to make your misinformation Spider-Sense tingle pretty early on. Everything the CDC has recommended throughout the pandemic has contradicted the “rules of science”? Social distancing and staying home when sick don’t decrease transmission? Quarantining when exposed to a deadly and contagious pathogen doesn’t save lives? Dr. Stock would be on a much stronger footing if he said that he opposed specific recommendations- for instance masking and vaccinations- and then told us why he opposes them on scientific grounds. This “CDC is BAD” signaling is sure to get applause and video shares, but it’s hardly a good start for reasonable, precise debate.
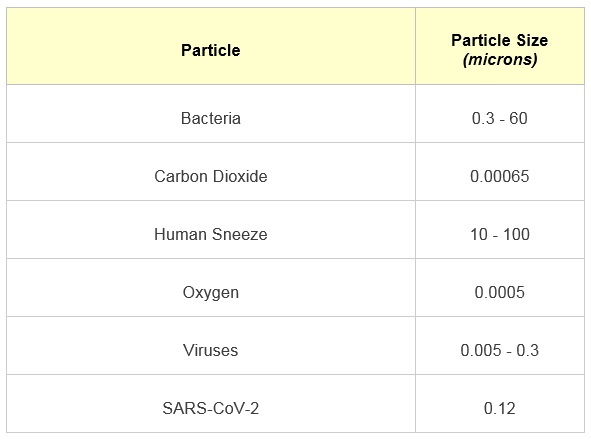
0:43 “Things you should know about Coronavirus and every other respiratory virus…” I would be incredibly suspicious of anyone lumping SARS-CoV-2 in with “all other respiratory viruses”… or lumping ‘all respiratory viruses’ together at all, for that matter. The virus that causes COVID-19 has behaved unpredictably throughout the course of this pandemic in more ways than we could count. It is a strange and unpredictable virus, which is why we had an even harder time treating it effectively in the hospital early on and why our transmission control measures, which have worked astoundingly well for Flu, have only ever managed to take the edge off of it’s transmission.
Dr. Stock would like to lull you into thinking that there is a set of regularities that viruses called “upper respiratory viruses” all follow, and that COVID-19 follows all of these as well. He may be lulled into believing it himself; he says later that he has seen only 15 COVID-19 patients. Last March many of us, myself included, believed that the ‘new coronavirus’ in China and parts of Europe was just media medical sensationalism. “Coronaviruses aren’t that dangerous,” we said (forgetting all about SARS since many of us had never actually seen a case of it), “they cause the common cold; there’s nothing to be worried about.”
Then we started treating it. I still remember the night I sat in bed watching videos from ICU’s in Italy, completely overwhelmed and without the medical equipment, supplies, rooms, or staff to care for all of the patients dying in respiratory distress, and I realized for the first time, “this is real.”
When Dr. Stock tells you throughout this video, “we shouldn’t do x, y, or z for COVID-19 because we’ve never done it for respiratory syncytial virus (RSV),” you need to remember that we have never seen RSV kill 600,000 Americans of all ages in 18 months. It’s the grossest kind of false-equivalence.
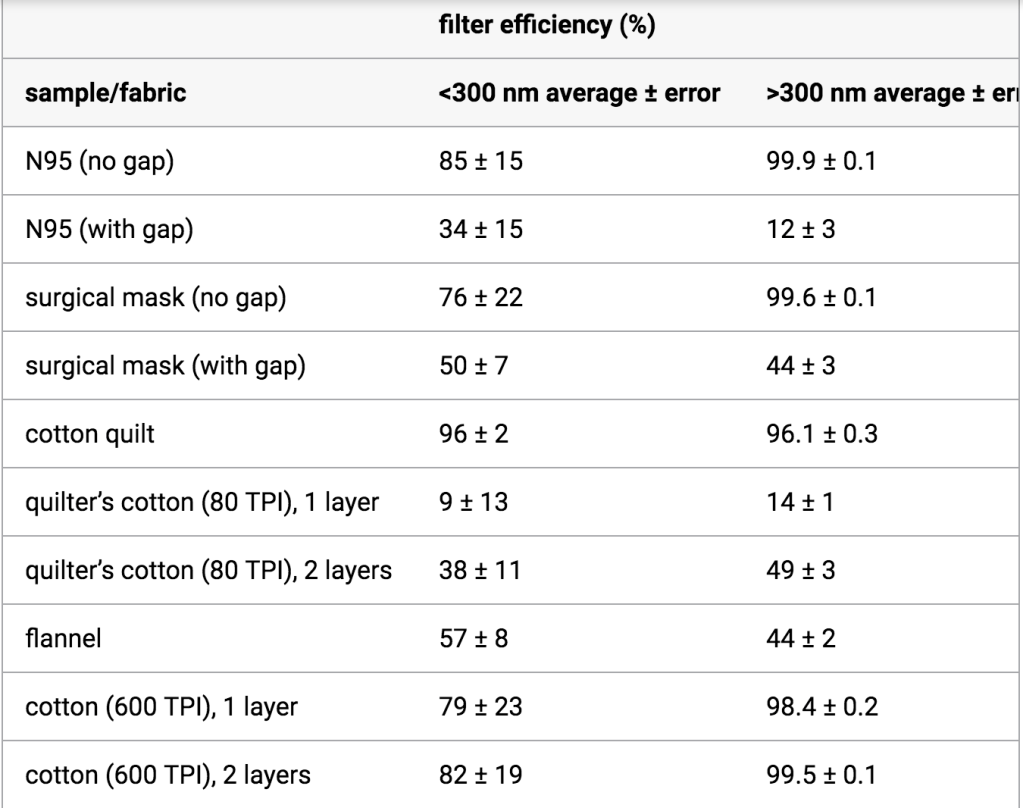
0:45 “Coronaviruses are spread by aerosol particles that are small enough to go through every mask.” It’s been 18 months and it’s really hard to believe we are still talking about whether or not masks work, considering the abundance of data from epidemiology, physics, microbiology, and virology. I wrote about this extensively in June of 2020, and the evidence was already robust then. Yes, while masks like N95’s do a reasonably good job of stopping even small aerosolized particles that contain live viruses, surgical masks, simple cloth masks, and other options have a much lower filter efficacy at the 50-140 nanometer range, the size of the Sars-CoV-2 virions. A surgical mask will not stop every viral particle; but the mask that you are wearing will filter out a percentage of them depending on the type of mask; more for an N95, less for a surgical mask, and even less for a bandana or scarf. And the mask the infected person is wearing both block respiratory droplets from normal talking and will greatly decrease the velocity and spread of respiratory droplets, including the smaller aerosolized particles, and ensure that they hang around in the air for a shorter period of time.
I have never heard a scientist or physician claim that if 100% of people wore masks it would completely halt COVID-19 transmission; I’ve certainly never made that claim. But it does help, a lot, and the evidence for it is supported by far more than the three studies referenced by Dr. Stock (to be fair, he mentions these are the 3 that were funded by the CDC; he surely has more). This article on masks and COVID-19 transmission from Sri Lanka from last June cites 139 articles on upper respiratory viral transmission, particle size and dynamics, and prevention; a pretty good benchmark for that sort of paper. Saying “the masks don’t work” at this point in the pandemic is a call-back to the COVID-19 anti-mask skepticism of last Summer.
1:03 “Even though the CDC and the NIH have decided to ignore the very science they paid to have done.” The CDC and the NIH fund literally tens of thousands of research studies each year; many of them are looking at the exact same or very closely related issues, and many times different studies that they fund produce differing conclusions; data that requires analysis, synthesis, and careful parsing. We would be extremely worried if they didn‘t. The fact that the CDC and NIH sponsor many studies and then carefully analyze the results, as well as the results of studies they didn’t pay for, before giving recommendations is a very good thing. If the CDC were to either ‘not read the science’, or cherry-pick the information they believe based on what agrees with their presuppositions- as Dr. Stock is doing with these studies he references- they would not be a reliable source of medical and epidemiological guidance. Thankfully, they don’t do that.
1:15 “The history of all respiratory viruses is that they circulate all year long waiting for the immune system to get sick through the Winter or become deranged as has happened recently with these vaccines.” Dr. Stock practices something called “functional medicine”; basically the idea of addressing the root causes of disease and using the body’s own systems, as much as possible, to fight illness. It isn’t different than the practice of medicine in general, but it is a neat field that certainly has a more intentional focus on underlying causes. Because the emphasis so often lies on the patient’s own immune system fighting any infectious illnesses, the functional medicine doctors I know are very pro-vaccine; vaccination is as much in-line with the concept of letting the immune system do what it was designed to do as any medical practice. Unfortunately, functional medicine also attracts some doctors who are embracing certain anti-medicine or anti-science narratives, either because they have come to believe them themselves or because they see what a lucrative market there is for someone willing to offer all the benefits of modern medicine from an anti-modern medicine perspective and without the restrictions of having to follow the scientific evidence when it’s inconvenient. Good functional medicine doctors don’t do that, and I have heard recently from those practicing functional medicine who feel that doctors like Ben Edwards and now Dan Stock who spread misinformation give their discipline a bad name.
Because Dr. Stock has embraced a perspective that emphasizes the immune system above all else (yet somehow he doesn’t embrace the vaccines that give the immune system the data it needs to fight COVID?), his perspective on the seasonal pattern of respiratory viruses here is extremely incomplete. I thought about skipping this section, but it’s such subtle misinformation that it might get past people and lay the groundwork for more direct misinformation he shares in a few minutes.
Dr. Stock claims that respiratory viruses are worse in the Winter because the immune system is weaker, or because we get seasonal vaccines (like the flu shot or COVID-19 vaccines) that ‘derange’ the immune system. The latter part is nonsense; we’ll talk about it more later but it’s like saying that a construction crew becomes deranged when given a set of blueprints, or a sniper becomes deranged when given a photograph of her target. There is some truth to the first part; the immune system does work better during the Summer for a number of reasons, including sunlight exposure and increased exercise. But of the three major reasons for respiratory illnesses being worse during the Winter (or during the rainy season in temperate climates), it is probably the least influential in the seasonal pattern of these types of viruses.
First, viruses spread more during the Winter because of our behavior. How often have you heard the cultural myth that someone became ill with flu or pneumonia because they went out in the cold or got wet out of doors? It’s the opposite; they got ill with an infectious illness when they came back in to warm-up or dry-off, and were around someone with the virus. We spread respiratory viruses person to person through contact, sneezing, coughing, and touching surfaces while contagious. That transmission happens more easily indoors because of the close proximity and decreased air-flow compared to outside, and we spend most of our time indoors during the Winter. Think of your last Summer event; say spending the day at the lake. Yes, there were many people there, but you could spread out, the wind was blowing, and your conversations tended to happen with some space between you. Now think of your last Winter event- say a Christmas party. The same number of people, but this time inside, talking less than a couple of feet away, sharing the same air. Both events are wonderful (and I missed the latter this past year more than I can tell you), but there is no denying that one is a better opportunity for respiratory viruses to be transmitted than the other.
But the second reason is because of the behavior of the viruses themselves. Viruses are living organisms and like all living organisms they respond to their environment. Viruses like RSV and influenza are more stable in colder temperatures, meaning they can survive longer outside of the body when it is cold; both on surfaces and in the air. They also are more effective as aerosolized droplets when the humidity is low, because the droplets tend to be smaller. There are also effects of sunlight exposure on the viruses themselves, with the UV radiation damaging the genetic information of the viruses (just like it does ours; please wear sunscreen!), inactivating them to a certain degree. If anyone remembers last April, we all hoped that COVID-19 would disappear during the Summer because of these environmental factors. SARS-CoV-2 is an incredibly contagious, previously unknown virus; we hoped that it would display strong seasonal patterns like the flu and we would have a reprieve during the Summer. And maybe we did; but it wasn’t enough of a reprieve to prevent outbreaks, including here in Texas. In a little while Dr. Stock will tell you that the COVID-19 vaccines are the cause for the virus causing outbreaks this Summer. This is a myth, plain and simple. These outbreaks happened last year too, before anyone outside of clinical trials had access to the vaccine. The outbreaks this Summer are simply due to the fact that, unfortunately, COVID-19 does not display as strong seasonality as many of the other respiratory viruses we liken it to, and even more importantly, because the Delta variant is probably the most contagious dangerous respiratory in human history.
1:25 “The CDC has managed to convince everybody that we can handle this like we did smallpox.” The CDC and public health experts, and those of us fighting COVID-19 every day, have not felt a sense of extreme urgency to promote effective vaccinations against COVID-19 in order to eradicate it, but to prevent people from dying from it. Vaccination was invented by Dr. Edward Jenner, and was taken directly from the practice of inoculation- deliberately exposing the person to a small amount of the disease or a similar disease and hoping they would survive if they were exposed later. The practice of inoculation- or variolation when we are referring specifically to smallpox- was dangerous; since it was a live, active infection, it was possible to become sick with the disease when inoculated, and possibly to die from it. Nevertheless it was effective, and when American doctors were first given the idea to use inoculation to combat smallpox by an enslaved African man in 1721, his knowledge of traditional African healing practices saved hundreds of people during a smallpox epidemic in Boston.
Vaccination was different; it exposed the person to enough of the virus to trigger an immune response without the risk of the person contracting the virus. Traditionally this has been done by weakening or killing the virus, or by giving very closely related viruses that cannot cause disease (cowpox, in the case of smallpox vaccination). We now have the technology to teach cells to build specific, non-dangerous viral proteins so the immune system can learn to recognize them and build antibodies against them without exposing the body to any virus at all. This is a natural progression of the principal of inoculation that humans have used for thousands of years; live virus to weakened virus, weakened virus to dead virus, and now dead virus to no virus at all. The mRNA vaccine technology feels unknown or unnatural to many people, because it came about in their lifetime (I was 6 years old the first time scientists successfully used mRNA technology to teach cells to express viral proteins); but it is really the logical next step along the path set for us by traditional African, Indian, and Asian healing practices; the path of using the body’s own immune system to fight disease.
Dr. Edward Jenner’s personal goal, oft stated, was to eradicated Smallpox. But that was not the only or even the primary goal. The goal of inoculation, variolation, and vaccination has always been to prime a person’s immune system to fight an illness so that they have a less severe course of illness and a lower risk of dying from it. That was the goal of variolation in Western African and later in Boston, it is the goal of the childhood vaccinations we give against measles, whooping cough, and tetanus, it is the goal of the annual flu shot, which has saved millions of lives, and it is the goal of the COVID-19 vaccines; a goal they have seen incredible success at achieving, for those who have received them. We may not be able to eradicate COVID-19; but we can very effectively protect people from it.
2:04: “I would hope this board would start asking itself, before it considers taking the advice of the CDC, the NIH, and the State board of health, why we are doing things about this that we don’t do for the common cold, influenza, or respiratory syncytial virus?”
Seriously Dr. Stock? That’syour question?
2:16 “Why is a vaccine that is supposedly so effective having a breakout in the middle of the Summer when viral respiratory syndromes don’t do that? It’s a little tricky to understand what he is talking about right here. First of all, the vaccine isn’t having an outbreak. That would actually be awesome, if just suddenly there was this uncontrollable surge of people getting vaccinated. What he means is, ‘the virus is having an outbreak because of the vaccines.’ He is subtly shifting responsibility for the outbreaks away from the virus itself, the incredibly contagious delta variant, the general lack of caution and transmission control measures being exercised, abysmally low vaccination rates, and widespread conspiracy theories and disinformation, and onto the vaccines, which is a tactic from the “it’s so crazy it just might work” school of misinformation. He is asking you to shorten your memory and ignore the fact that we already knew pre-vaccine that this is how COVID-19 behaves, since this is what it did last Summer. He wants you to think something like this; “COVID-19 is really bad this Summer. Dr. Stock says that shouldn’t happen during the Summer. A lot of people I know have been getting those vaccines… I bet that’s why.” It’s a logically bankrupt argument with no foundation in reality… But it just might convince some people.
In a moment Dr. Stock is going to offer a seemingly plausible explanation for his false narrative in the form of “antibody-mediated viral enhancement.” Dr. Simone Gold shared this same misinformation a few months ago, so below I will copy my discussion of the phenomenon from that time.But the best cure I have for Dr. Stock planting this sort of deliberate misunderstanding is just data. The vaccines are working well, and anywhere that you see high vaccination rates you see fewer and less severe cases, not higher numbers and more severe cases. All of the evidence says the vaccines are working against COVID-19. If we had higher vaccination rates in Texas and Louisiana, we would have smaller and less severe outbreaks this Summer, plain and simple.
2:28 “You need to know the condition called “antibody-mediated viral enhancement. That is a condition done when vaccines work wrong…” There’s a lot of misinformation here. For instance, he implies that COVID-19 has low pathogenicity- a low rate of causing illness- which is totally disconnected from reality. He also implies that the current COVID-19 vaccines caused antibody mediated enhancement in previous studies, which they absolutely did not. In fact, even though Dr. Stock presents this as though he were blowing the lid off of this hitherto-unheard-of fatal flaw in COVID-19 vaccines, avoiding the risk of this phenomenon was foremost in researchers minds when designing these vaccines; he would have you believe that the scientists designing the vaccines had never heard of it before, simply because you might not have heard about it before.
Immune enhancement is a very real concerned, and one that has been hotly debated within research circles since the beginning of the pandemic, especially in regards to severe COVID-19 cases and the potential role of vaccines. Here’s an article from way back in May 2020 (what is that, like 8 years ago now?) about this exact issue. The specific proteins chosen for the mRNA vaccines were chosen carefully and specifically to avoid this problem, and moreover, this is exactly why we do animal studies and clinical trials.
The Moderna and Pfizer trials were simply huge, with ten times the number of people participating than is typical in a vaccine trial; and no evidence of Antibody-Dependent Enhancement was found. The Nerdy Girls over at Dear Pandemic have a short but great social media update on it from just a few months ago:
Moreover, we have now given 352 million COVID-19 vaccine doses in the US alone and over 4 billion doses worldwide, and there is still no evidence that the COVID-19 vaccines cause antibody-dependent or antibody-mediated enhancement. The entire course of the pandemic shows exactly the opposite; those who have the vaccine get less sick, less often, and have drastically lower rates of severe illness, hospital and ICU admission, or death from COVID-19.
3:10 “75% of people who had COVID-19 positive symptomatic cases in the Barnstable Massachusetts outbreak were fully vaccinated.” And 4 of them were hospitalized, and none of them died. I wrote about this just yesterday so I won’t rehash it; it’s a very short post and the link is just below. The long and short of it is, the Barnstable “outbreak” is proof of how well the vaccines work, not of the contrary. What we saw in Barnstable is the opposite of antibody-dependent enhancement; it’s a clear demonstration of the effective protection against severe illness and death for those with the vaccine, and an example of what might have been if we had such high vaccination rates in Texas, Louisiana, and Florida before the Delta variant hit.
3:23 “Therefore there is no reason for treating any person fully vaccinated any differently than any person unvaccinated.” In a sense, he’s correct; morally we absolutely should be aiming to treat all people the same regardless of their personal health choices. I am reminded of the quote by C.S. Lewis:
“There are no ordinary people. You have never talked to a mere mortal. Nations, cultures, arts, civilizations – these are mortal, and their life is to ours as the life of a gnat. But it is immortals whom we joke with, work with, marry, snub and exploit – immortal horrors or everlasting splendors.”
― C.S. Lewis, The Weight of Glory
Your unvaccinated neighbor, your vaccinated friend… They are equal in dignity and honor; they are equal bearers of the Imago Dei. Yet our very respect for that Image of God in each person does require us to weigh many factors in the balance as we consider our approach to this complex pandemic. I believe that profound respect for the dignity of all people requires us to “treat” vaccinated and unvaccinated people differently in two ways.
First, we need to recognize that, regardless of Dr. Stock’s subsequent comments, the COVID-19 vaccines do prevent transmission of the virus. The jury is still out on how well they do this; most of our data just establishes how good they are at preventing symptomatic infection and especially severe infection and death, and there are studies happening right now to see to what degree vaccinated folks can still pass the virus along when symptomatic and when exposed but asymptomatic. The Barnstable MA outbreak is warning enough for all of us who are vaccinated to continue to take precautions like wearing masks and staying home and getting tested when we are ill, if anyone had any doubts. But it was also a contained, small outbreak and we don’t actually know how much of it was transmitted by vaccinated residents of Barnstable county vs. out-of-state visitors; and there’s no way to go back and find out. Nationwide we are seeing Delta surging, and surging most in the states with the lowest vaccination rates. All of the physiology of how our immune systems fight viruses when primed with vaccines suggests that vaccinated people will transmit the virus at a lower rate, and for a shorter duration, than those who are unvaccinated. Vaccines don’t teach your immune system how to ignore the virus, while it multiplies and gets passed along to others; it teaches your body how to kill it. And this, married to the epidemiology evidence of how the surge is progressing in highly vaccinated vs. poorly vaccinated areas constitutes strong evidence that the vaccines do confer protection not only against getting sick from the virus, but against passing it along to others as well.
This is not how your antibodies and the COVID-19 virus interact.
Does this mean that I treat my unvaccinated friends and family like second-class-citizens, barring them from my home and preventing them from ever spending time with my children? While I understand and sympathize with those who feel forced to do so, my answer is a definite “no.” But it does mean that the complex balance of goods and risks that determine in what way I and my family interact with others- which always existed even prior to COVID- has one more important factor. My children are unvaccinated (though I am trying to enroll them in clinical trials so they can get a COVID-19 vaccine as soon as possible), and there is already anecdotal evidence that the Delta variant effects children more than the original strain. I have a basic moral responsibility to protect my children, and the reality is that factors like community transmission rates and the personal health choices of others do have to be factored into our decisions. For us it’s not a question of, “who do we cut out of our lives because they won’t get vaccinated?”, but a question of, “how can we best build and maintain relationships while limiting risk?” That answer is going to vary to some degree with the current prevalence of COVID-19, with the level of caution those in our lives are themselves following, and with their vaccination status.
But I think the second way we treat unvaccinated people differently is arguably much more important. The reality is that, whether they believe it or not, they are more vulnerableto the virus. As a physician, the rapidly branching mental decision tree I follow when helping a patient decide what level of caution to exercise, what treatments to pursue, what symptoms to watch out for, how aggressive to be in seeking further care, and how closely to follow-up is determined by many factors. For COVID-19 care, vaccination status is a big one. My vaccinated patient’s chances of dying from COVID-19 are far, far lower than my unvaccinated patient’s chances, all other things being equal. As a society, our decisions about protecting people from the virus need to be centered on those who can’t be vaccinated, like children or those with true vaccine allergies, on those like the immunocompromised for whom the vaccines might not be as effective, and on those who decide not to be vaccinated. They are still at risk, and nowhere in my medical training can I recall an ethical precedent that says we don’t take excellent care of people if their personal health choices led to their illness (though I do realize that, far too often in modern medicine, we treat patients poorly if they are perceived as contributing to their own health problems or ‘not caring enough’. It’s a huge problem, and trying to address it is one of the reasons I’ve taken a new job teaching at a medical school).
In general I don’t agree with measures that say, “if you are vaccinated you can do this, if not you have to do this.” I understand that from an epidemiology standpoint some of these distinctions are logistically impossible to get around; but the tenets of my faith call for humility and self-sacrifice on behalf of others. If their decision to not get vaccinated means that I have to endure some ongoing inconveniences- like wearing a mask while buying groceries or sitting outside and socially distanced at my favorite coffee shop in the middle of August, when it would be more pleasant inside- I’m here for it. If I knew for a fact that everyone at that store or everyone inside the coffee shop were vaccinated, I might loosen those measures, as I do in small gatherings where I do know that everyone is vaccinated (just ask my Dungeons and Dragons group; we had this exact conversation last week!). I wouldn’t advocate for stricter transmission control measures imposed only on the unvaccinated, but I would advocate for us all following those strict measures, and then dropping some of them that are no longer needed when we know the unvaccinated aren’t going to be potentially hurt by doing so. If that still means I’m “treating them differently,” I guess guilty as charged; I’m treating them like their lives are in danger, because they are, and well, that’s something I really do care about.
3:27 “No vaccine ever stops infection.” By “infection” Dr. Stock does not mean the virus multiplying significantly in your body for any specific period of time, or the onset of any specific symptoms; only the state of having the virus enter your body and begin to reproduce itself. This is what I’ve been trying to help patients understand for the past 9 months as we have talked about the COVID-19 vaccines: vaccines don’t place a forcefield around you that prevents the virus from entering your system; they prime your immune system to defeat it.
But saying that infection still occurs whenever you are exposed to the virus is not the same as saying that transmission occurs, or occurs at anywhere near the same rate, if you are vaccinated. We’ve just talked about how the evidence on this is still evolving for COVID-19, but that it’s very clear that those areas with higher vaccination rates have lower transmission rates. Yes, some people who are vaccinated still get COVID-19, but tend to have shorter illness, lower viral loads, and less severe symptoms. It’s unclear exactly how well they spread the virus, just as it’s still unclear whether the vaccinated are sometimes asymptomatic carriers. But we do know that both of those types of transmissions occur, and occur at extremely high rates, in the unvaccinated who become infected with COVID-19. The current surge of the Delta variant is being driven by transmission from and to unvaccinated individuals.
I won’t keep rehashing the same points, but I will add this; Dr. Stock iswrong about vaccination ‘never stopping infection’ (the virus getting into your system in the first place); it stops infection for the next person, by decreasing the chances that you’ll get sick and pass it along. Please catch the contradiction he has created for himself; Dr. Stock is painting a picture of viral infections moving from person to person uninhibited by their immune systems, with those who get the vaccine (or at least, the vaccines he agrees with) not getting sick but still invisibly passing it around as much as anybody as it lives rent-free in our systems forever.
But a couple of minutes ago he admitted that vaccines eradicated smallpox.
I’ve never been vaccinated against smallpox. Hardly anyone in the US has since 1972. So where is it? High vaccination rates literally stopped it from infecting anyone. If it only suppressed disease and not infection and transmission, we should have seen a smallpox resurgence decades ago, once we stopped vaccinated for it; thankfully, there is still no evidence of smallpox transmission anywhere in the world. No, I don’t think we’ll eradicate COVID-19 the same way, even with high vaccination rates; it’s a very different sort of virus, and the best we can probably hope for is to remove its teeth. But since he brought up smallpox in the first place, I think it’s fair to point out how the history of smallpox vaccination and eradication blows his picture of how vaccines work right out of the water.
3:38 Mumps Outbreak in the National Hockey League. In 2014 there was an outbreak of mumps in the NHL that affected 24 players. The mumps vaccine is not 100% effective, but it is very, very effective as Dr. Stock admits. Prior to the mumps vaccine, almost all children got mumps at some point during childhood. After vaccination against mumps became common, the rate of mumps infection dropped by 99 percent. Yes, it is still possible to get or spread a virus if you are vaccinated, no one has ever said otherwise; but it is far less likely. Why is Dr. Dan Stock currently citing contract tracing for a so-called outbreak that affected 24 people, when just 50 years ago most people got mumps during childhood? Because vaccination against mumps is so effective.
How effective? Well, two doses of the mumps vaccine is about 88% effective at preventing this previously ubiquitous illness. 88% is also how effective the mRNA vaccines seem to be against the Delta variant of COVID-19. Ask yourself, when was the last time you worried about mumps? Wouldn’t it be great to get to that point with COVID-19 too?
4:12 “You get infected, you shed pathogen; you just don’t get symptomatic from it.” We’ve talked this false idea that vaccinated people spread the virus just as well as unvaccinated people to death in the last few paragraphs, so I’ll just add this; when “getting symptomatic” from COVID-19 has resulted in 617,000 deaths in the US in just 18 months, doesn’t “not getting symptomatic” sound like a really, really good thing?
4:14 “You cannot stop spread, you cannot make these numbers that you’ve planned on get better by doing any of the things you’re doing, because that is the nature of viral respiratory pathogens.” All of the epidemiological evidence, from all over the country, says he’s wrong. The vaccines are slowing the spread and making the numbers better. He’s also wrong that the nature of viral respiratory pathogens means that you can’t slow them with basic transmission control efforts like wearing masks and strict sick policies in schools; those very efforts helped us kick influenza’s butt last year. COVID-19 is trickier to beat since it is so much more contagious and has so much asymptomatic transmission, but there’s no doubt that when these measures are followed, they do help. There’s ample evidence of that all over the world, both pre- and post-vaccine.
I’ve said it before and I’ll say it again; there is something deeply disingenuous about people who refuse to wear masks or follow transmission control measures, and have refused to do so since the beginning of the pandemic, pointing to increasing case counts and saying, “see! these masks (I won’t wear) and transmission control measures (I won’t follow) don’t work!”
4:26 “You will be chasing this the rest of your life until you recognize that the Center for Disease Control and the Indiana State Board of Health are giving you very bad scientific guidance.” And what does Dr. Stock place in opposition to this scientific guidance? Other expert organizations with teams of researchers and epidemiologists devoted to finding the very best ways to slow the pandemic and combat COVID-19? A specific, innovative plan of attack that none of the experts have thought of yet (hey, it could definitely happen!)? No; his e-mail, and the other people in the room who have presumably come to the board meeting to protest mask mandates or vaccines or whatever specific measure was originally on the table for discussion that night.
4:47 “That’s why you’re still fighting this with this vaccine that was supposedly going to make all of this go away...“ “The vaccine I won’t get and am telling all of my patients not to get. Why hasn’t it worked yet?”
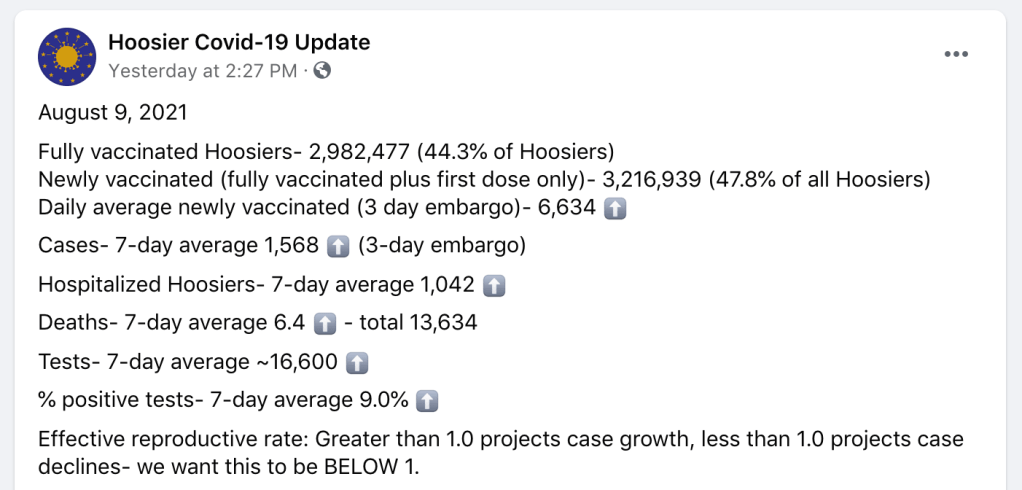
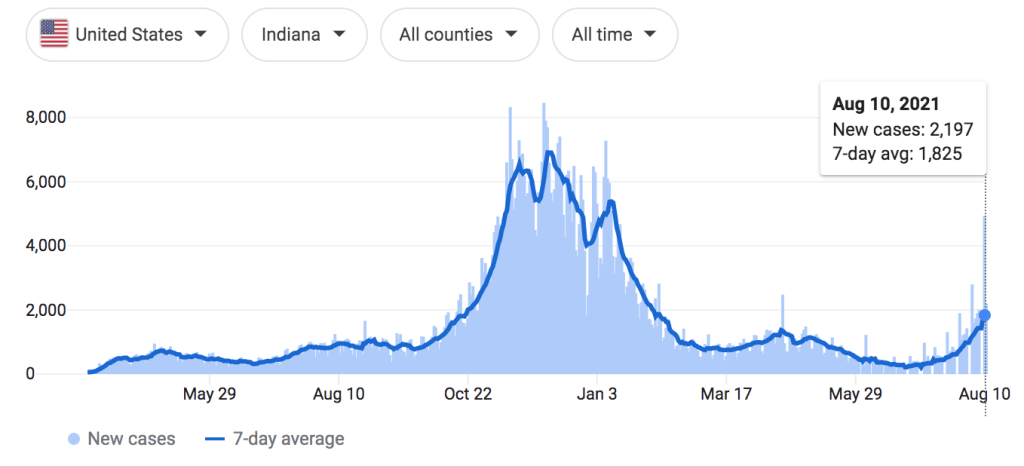
Indiana has only a 44.3% vaccination rate. They are in the middle of a COVID-19 outbreak; not as bad Texas or Louisiana, but still on the rise.
Again Dr. Stock blames the vaccines, instead of the virus and our low vaccination rates, for the outbreak, reinforcing his false narrative that vaccines have caused the outbreak through antibody mediated viral enhancement instead of reduced or prevented outbreaks wherever vaccination rates are high. If his “outbreak in the middle of the Summer” reference is to his own state of Indiana, I would paraphrase G.K. Chesterton; ‘the vaccines have not been tried and found wanting; they have been found shrouded in disinformation, and left untried.’
On the other hand, if he is again referencing the contained “outbreak” in Barnstable Massachusetts, one would ask why he feels compelled to rely on epidemiology data about the pandemic from a county a thousand miles away, when the evidence from his home state shows how effective the vaccines are? I submit that it is because theoutbreak in Massachusetts is the data that best seems to support his claims (again, we’ve seen already that it doesn’t), and he would go to the ends of the earth to find it. When you are committed to misinformation, the experiences of people affected by the virus all around you simply aren’t important unless they fit into your narrative.
5:05 “I can tell you having treated over fifteen COVID-19 patients…” Listen, I know no misinformation video would be complete without touting the latest en-vogue, unproven therapies. But 15 patients? Fifteen?!
I’ve treated hundreds. Nobody wishes that we had a safe and effective prophylactic or early symptomatic treatment regimen more than I do. I spend so much time kneeling on pavement next to cars in the Texas heat, counseling my patients on what to look out for with COVID, helping them establish a posture of vigilance and discernment but without fear or anxiety, helping them navigate the different options for considering monoclonal antibody therapy, and helping them make decisions about work, school, and how to prevent transmission to loved ones. This narrative that we are refusing to give effective treatment to our patients is deeply frustrating and not at all based in truth; I have never withheld a medicine I believed my patient needed, not once in my life; and I spent a lot of my time trying to help them figure out how to get those medicines regardless of expense or other barriers. We are giving them the best that we have to offer; we have been since the beginning of the pandemic and long before.
This “clinical experience” that these doctors like Simone Gold or Ivette Lozano who have treated a small handful of COVID-19 patients (or in their own words, people who thoughttheymight have COVID-19; many times these doctors don’t even bother to test because they don’t believe the tests work) share about how they’ve found a universally effective treatment against COVID aren’t even anecdotal evidence; they are just sampling bias. They see a couple of patients, some of them have COVID and some of them don’t. They put them all on a cocktail of drugs, none of which have been shown to be effective in clinical trials. Those patients recover, as most patients with COVID-19 do without these unproven treatments; but then these doctors tell themselves “without my treatment, that patient would have died.” Except there is no evidence they would have; for some of these docs, there isn’t any evidence those patients who “would have died without my treatment” even had COVID-19 to begin with. They were doing this same nonsense last March and April in areas that hadn’t even seen their first surge of COVID-19 yet, drawing customers (they aren’t your patients when you are just selling them something) from all over the state and saying things like, “yeah, you probably have it, take all of these medicines”, then adding that person’s “survival” to their “evidence.”
I don’t know if this is what Dr. Stock is doing or not. Maybe his patients all had laboratory confirmed COVID-19, or a convincing combination of symptoms and exposure history. Maybe they had really significant risk factors for severe illness, and their recovery turned him from a skeptic to a believer; I don’t know. He certainly seems sincere in his beliefs. but the fact of the matter is, 15 patients with COVID-19 is not enough to base your case on. That’s one of the principals of evidence-based medicine, having the humility to give our own personal experiences only the weight they are due, and respecting our colleagues, our patients, and people from around the country and world enough to recognize when our experiences are atypical or, as in this case, just way, way too small to actually draw conclusions from. I’ve had many days in clinic when I took care of more than 15 patients with COVID-19. Sometimes I’ve been surprised by how sick a young, previously healthy person got with the virus, and sometimes I’ve been surprised by how light a course of illness someone with many risk factors experienced. I can’t draw conclusions from those experiences any more than Dr. Stock can; even my vastly more extensive experience with COVID-19 pales in comparison to our collective experiences as a medical field, compiled as evidence and then analyzed carefully.
And look, I get it. If I were seeing less than 1 patient a month for COVID-19, I might be tempted to abandon evidence and just throw whatever the current theoretical treatment was at them too. These medicines like hydroxychloroquine, zinc, Azithromycin (remember when that was a thing?), and Ivermectin are generally safe, and I’ve prescribed them all for different illnesses in the past. If I gave out one prescription a month because I though there was a chance they would help, I wouldn’t be doing something morally wrong. But it’s not evidence based medicine, and it only feels excusable to practice on gut instinct or social media hearsay like that when you are talking about incredibly small numbers of patients. But because there is no evidence that they do work against COVID-19, prescribing them routinely, prescribing them for thousands of patients with COVID-19, COVID-19 exposure, or COVID-19 like symptoms like I would have to do as someone who fights this virus every single day, would be no different than throwing antibiotics at viral infections because it’s quicker than explaining the difference being a viral and a bacterial infection, doing unnecessary surgeries because it “might help the pain,” or adding more and more medications because you are too busy or too lazy to help your patient find a diagnosis and understand their illness. It isn’t the practice of medicine.
If I’m going to prescribe a medication to a thousand patients, I have to have evidence that it works. And if I’m going to hold a certain high standard of care for a thousand patients, my one patient deserves that same standard of care; they don’t deserve to be the guinea pig for the ‘Ivermectin study I’m doing in my head.’ Right now there is no evidence Ivermectin prevents severe COVID-19. I hope that changes. It didn’t change for azithromycin or hydroxychloroquine, but I hope it does for ivermectin so I can start prescribing just tons of it. And if it doesn’t, I hope the next hot-button medicine really does work, so that I’ll finally have the silver bullet many patients are looking for when I give them the anxiety provoking news that they have COVID-19, instead of ‘just’ careful counseling, reassurance, guidance, and symptomatic treatment.
You know what is safe and does work extremely well at preventing severe COVID-19? Vaccination. As a functional medicine doctor, Dr. Stock’s entire ethos should revolve around identifying root causes, relying on our own body to produce a state of health (a privilege not everyone has), and prevention rather than treatment whenever possible. In stating that we should abandon training our immune systems to fight COVID-19 with the vaccines for all of the erroneous reasons he has offered because unproven treatment is available, he has abandoned functional medicine altogether.
5:45 “People who have recovered from COVID-19 infection get no benefit from vaccination.” Dr. Stock’s very last point is that people who have already had COVID-19 get no benefit from vaccination. This is a question I am asked frequently, and the epidemiology data about who is getting COVID-19 and who is not, and who is getting the most sick from it, does show that those who have already recovered from COVID benefit from the vaccine. The truth is that, if you have already had COVID-19 (just as I did back in December) and then are subsequently vaccinated (just as I was, also back in December, about 2 weeks later), you probably have the best immunity out of just about anybody. Seriously, I wouldn’t encourage anyone to go out and get COVID, but if you’ve already had it and decide to vaccinate, you are getting protection against COVID-19 that money can’t buy. Studies of antibody titers have shown that the immune response elicited by vaccination is equal or greater than that from natural immunity from previous infection. These vaccines are very, very good at what they do, and they work incredibly similarly to how our body’s learn how to defeat viruses from natural infection, only without the risk of illness since the vaccines contain no actual SARS-CoV-2 virus.
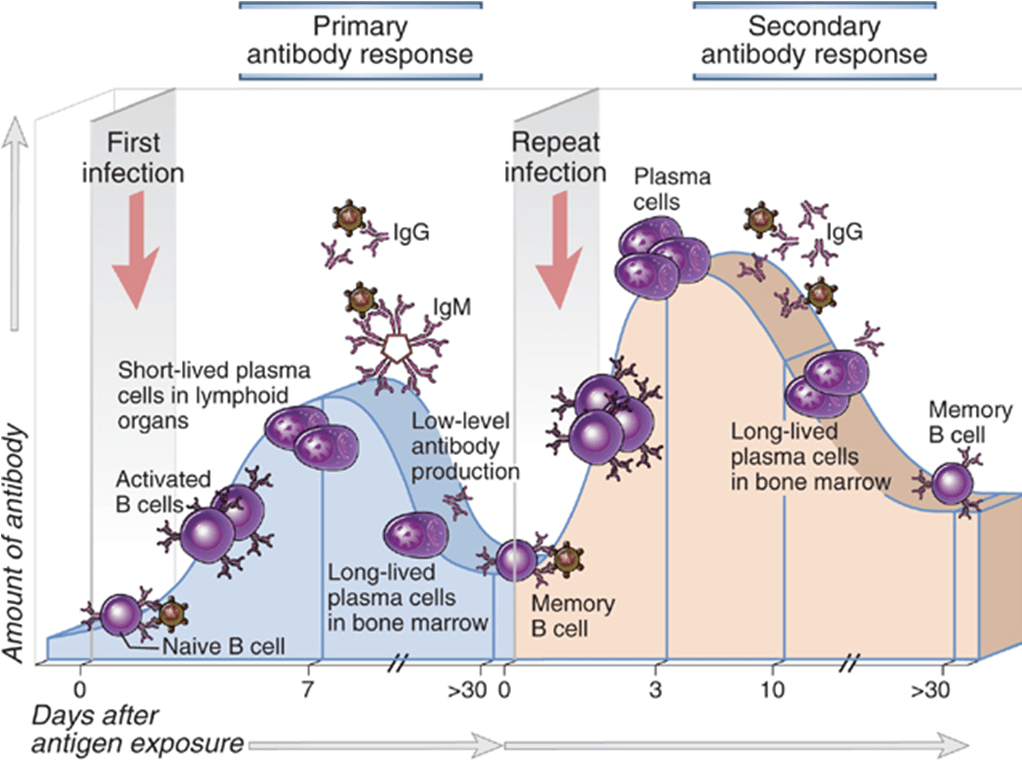
When you have an infection, your body responds with a host of inflammatory and immune cells. It’s a very good system, and if we are lucky enough to have a healthy immune system, it prevents us from becoming seriously ill from the various pathogens in our environment most of the time. But just like Sherlock Holmes, it needs a lot of information before it can produce its most incredible work.
To be perfectly honest, I prefer the BBC version of your immune system.
During that initial infection, the body is building antibodies, memory B and T cells, and other other specific immune cells targeted at that virus specifically. The next time you are exposed to that virus, the secondary immune response leaves the first one standing. With repeated exposures, the body learns that a threat is real and something you need to be prepared for; cells created after the first exposure, whether it’s from an infection or a vaccine, respond to the immune cells reacting to the 2nd exposure to create and even more robust response; cells that produce massive amounts of antibodies, cells that are incredibly active against the virus, and cells that move to the bone marrow and live for decades; maybe even your entire life.
If you’ve been lucky enough to avoid COVID-19 so far, the vaccines give you the opportunity to teach your body how to effectively produce this robust immune response without having to actually suffer through or take on the risk of getting the virus that has killed over 617,000 Americans in the past 18 months. If you’ve been unlucky enough to have COVID-19, but have recovered from it, the vaccines give you the opportunity to take that immune response you have already started building and ensure that you don’t just have some immunity, but that you actually have robust, probably very-long-lasting immunity. Your body doesn’t check Facebook or watch the news; the vaccines are your best and safest way of telling your body, “Remember COVID-19? Yeah, so that’s still a thing… Might want to be really prepared for it.”
The Barnstable County outbreak in July is a great example of how effective the COVID-19 vaccines are. They show us what an outbreak of the Delta variant of COVID-19 looks like in a highly vaccinated population.
Barnstable is a county of 213,000 people in the 2nd most densely populated state in the country. It is a popular tourist location, especially during the Summer. It just suffered an outbreak triggered by a super-spreader event. This resulted in only about 500 cases of COVID-19 (in residents; we don’t have data, including vaccination data, on the other half who were from out-of-state), 5 hospitalizations, and 0 deaths. About 79% of the population is fully vaccinated, with many more partially vaccinated. The various disinformation purveyors cite the fact that 74% of those who got COVID-19 during this outbreak were vaccinated as a shocking counterpoint to literally all of the data pouring in from all over the country, as though it proves that the vaccines don’t work… When really, it is exactly what we should expect even if they do work. It’s a bit like saying “the people who lived there are the ones who got it while living there”; unvaccinated Texas and Floridians couldn’t have gotten COVID-19 from the outbreak in Barnstable County Massachusetts; they weren’t there. We know many people who were just visiting did get COVID-19 during the outbreak, we just don’t have information on their vaccination rates because they went back home and added to their county’s COVID-19 statistics after the event; they aren’t included in Barnstable’s.
This is what COVID-19 hospitalizations look like all over the country in areas with low vaccination rates.
The misinformation would have you believe that 5 hospitalizations in Cape Cod are more statistically meaningful than 1,003 hospitalizations in Baton Rouge.
All of the evidence we have from the other 3,005 counties (and 64 Parishes) in the US strongly suggests that if Barnstable had had this outbreak with, say, a 36% vaccination rate like we have here, this would not be a mere 500 person outbreak with just 5 hospitalizations and 𝐳𝐞𝐫𝐨 deaths. Less densely populated counties without super-spreader events are seeing worse numbers than these every day, and their hospitals and ICU’s are filling up rapidly as patients continue to die. To put it another way, when I worked as a full-time hospitalist in a small town I considered it a “light day” when I personally had 8 or 9 patients to care for by myself; I felt busy once that number was above 14 or 15 (and some hospitalists routinely see 18 or more). The entire Barnstable outbreak resulted in a burden on their hospital system that required 1/3 of the time and effort of 1 doctor each day. And they all lived.
By the way, Barnstable is doing fine now; they really did have a contained, limited surge and now cases are falling again. Barnstable County, Massachusetts is not on fire.
My home state of Louisiana is. Texas will be soon (parts of it already are). We both have vaccinations rates that are about half of Barnstable County. That’s the difference in our case trends.
This is what might have been. This is what Texas could be experiencing right now if we had a higher vaccination rate: a minor surge, entirely within our capacity to handle, and quickly contained and improving. Instead hospitals all over the state are cancelling elective surgeries and operating beyond surge capacity, and the ER, hospital, and ICU doctors and nurses are so overwhelmed with COVID-19 that other patients can’t get access even when they are very ill or injured.
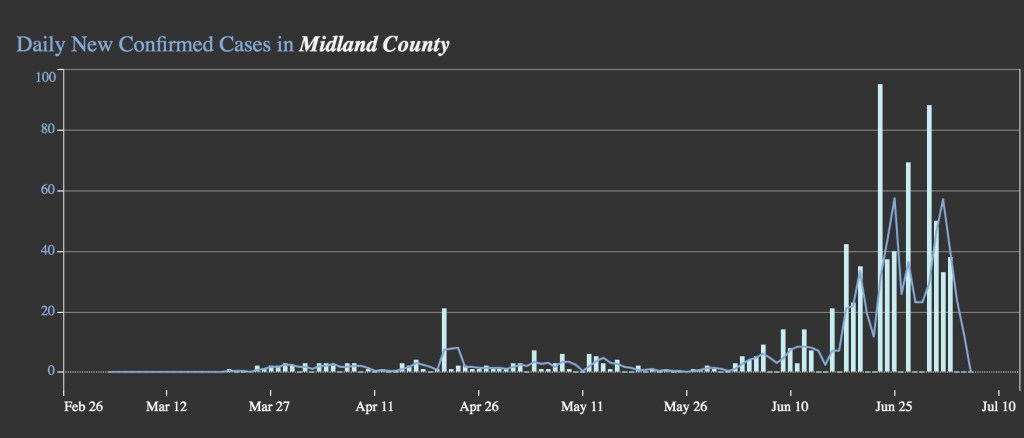
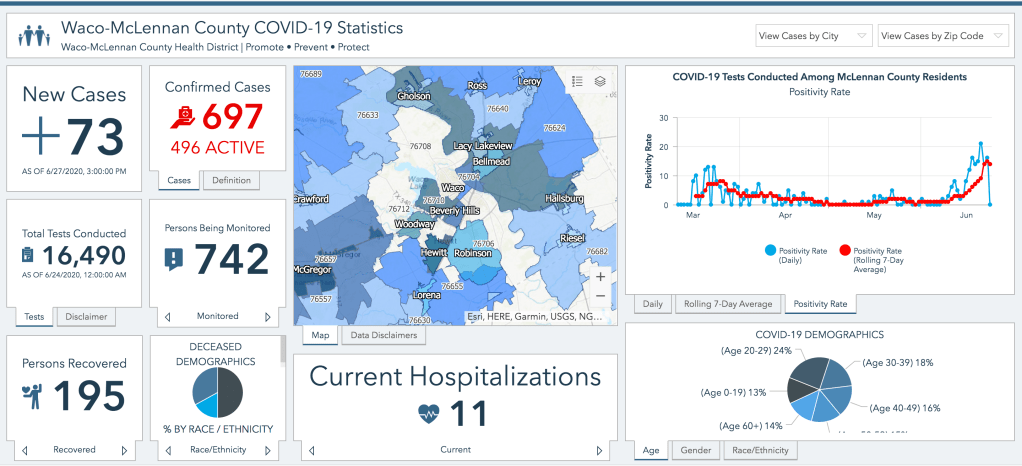
I live in a similarly sized county to Barnstable with half the population density, excellent local leadership, and no recent super-spreader events; yet we have 866 active cases, 173 new cases from just Friday (I diagnosed some of those personally), and over 100 hospitalizations. Most of those cases- and almost all of those hospitalizations- are unvaccinated patients. Our numbers just leave Barnstable county standing- because we have such a low vaccination rate. And we aren’t even calling it an outbreak; this is just what the COVID-19 Delta variant looks like anywhere without adequate vaccination rates to prevent widespread transmission.
McLennan County, Texas(This Week)
Population: 256,623
Population Density: 227 People/Sq. Mile
Current Active Cases: 866
Current COVID-19 Hospitalizations: 106
Barnstable County, Massachusetts (July Outbreak)
Population: 212,990
Population Density: 562 People/Sq. Mile
Total Cases in July: 560
Total Covid-19 Hospitalizations in July: 5
Vaccines don’t put a forcefield around us that keep us from coming in contact with the virus; they prime our immune system to fight the virus effectively when we do come into contact with it by teaching us how to build antibodies and a targeted immune response. No vaccine can keep every person from becoming symptomatic when they are exposed to COVID-19. But they do substantially reduce infections and thus transmission, and most importantly they greatly reduce the risk of severe illness and death; that has been their purpose since they were invented in the late 1700’s, and that was the purpose of vaccination’s predecessor, inoculation, which we inherited (one could argue, stole) from African, Indian, and Asian traditional healing practices.
Right now, hospitals all over the country are drowning in almost entirely unvaccinated COVID-19 cases that are absolutely overwhelming our medical infrastructure, and many of those patients are dying tragically- as are those who don’t have COVID-19 but can’t get medical access because the healthcare system is stretched so thin. They didn’t have to die. The Barnstable outbreak is indeed a warning about just how contagious the Delta variant really is- and how even vaccinated people need to continue exercising caution and wearing masks. But it also shows us how much better off we would be right now as a nation if all of our counties- and parishes- had vaccinated at the rate of Massachusetts.
The vaccines are incredibly safe and super effective; please go out and get one.
My web designer, who also designed and sells this shirt over at his site justacovelldesign.com, assures me that the vaccine can’t be “super effective” because “technically that describes a move and how effective it is against a certain type Pokémon rather than an item.” So the “It’s Super Effective” sticker I added “doesn’t make any sense.”
It’s been a difficult pandemic. And while our COVID-19 cases and the severity of illness we faced as a community was undoubtedly worse over the Winter, the hardest time period for me professionally has been the past 3 or 4 months, as we have dealt with the emotional, psychological, spiritual, and physical fallout of the pandemic’s worst season, trying to help people rebuild while still managing chronic medical problems and, of course, trying to keep everyone safe from the possible threat of another surge.
Healing is hard. Anyone who has done Primary Care Medicine, and especially those who have served a community that faces a great deal of healthcare injustice, knows that those 10 or 15 minutes the doctor gets with the patient in the exam room are not nearly enough to address their mental and physical health needs. The extra time has to come from somewhere, and since there’s another patient already waiting in the next room, for me it tends to come out of evenings, weekends, and early mornings. The number of hours your Family Doctor (or PA, or NP) works on your behalf behind the scenes is hard to calculate. Just check out Dr. Glaucomflecken’s take on Family Medicine:
Or maybe ZDoggMD puts it best when he simply says, “We love our patients, hate the system.”
I last published on medical misinformation back in February. Since that time I have had to choose between writing and carving out some amount of time with my family, and even with such an important topic as COVID-19 and vaccine misinformation, it was a pretty easy choice. So consider this my apology to anyone who has sent me conspiracy theory videos and disinformation memes that I haven’t had time to write about over the past few months; I hope you found the answers you needed.
But when a doctor in your clinic texts you at 7 AM, and it’s a video of a former Chief Resident from your own residency program sharing outrageous disinformation about the COVID-19 vaccines in front of the Texas state senate, it’s probably time to pick up the pen (or keyboard) again and do your part to debunk it.
Can we all just agree to collectively ignore how cringey it is that I went with this GIF?
Dr. Ben Edwards Testifies in front of the Texas Senate Committee on State Affairs
I first saw this video this morning; it’s from earlier in the week and was sent to me by a Physician that actually trained with Dr. Edwards. It’s short, barely over 8 minutes long, and in keeping with my longstanding policy I have shared it below. If it does get taken down by YouTube, which seems unlikely since it was a testimony before a government body and part of the public record, I will make efforts to find another active link to it. Even though it is short there is a lot of misinformation to unpack here, so I’ll be following a time-stamp format below as we dive in.
0:09 “The Chair calls Dr. Ben Edwards” For context, this was part of a Texas Senate Committee on State Affairs hearing to consider a proposal by State Senator Bob Hall regarding what measures or policies public and private entities can and cannot implement based on COVID-19 vaccination status. It is part of a broader misinformation campaign trying to portray those who choose not to get the COVID-19 vaccine as experiencing widespread prejudice and portray basic epidemiology measures based on vaccination status as a form of discrimination.
Of course there’s a balance here; while the evidence that the vaccines are very safe is overwhelming, I don’t know any doctor that would be comfortable with people being vaccinated against their will (something that has never been on the table despite the alarmist misinformation to the contrary) or becoming second-class citizens based on a personal health choice. There’s a discussion to be had about which measures are reasonable for government and private entities to take based on vaccination status and which are not; absolutely there is. But as I’ve been saying since the beginning of the pandemic, any such balance has to be struck on the basis of truth; that is, on firm evidence and an honest understanding of how dangerous the COVID-19 virus really is. State Senator Bob Hall, a consistent promoter of myths and misinformation throughout the pandemic, is not a man I would trust to strike such a balance. The balance we need to find is not a middle-ground between truth and lies.
Evidence Based Medicine
0:29 “Ben Edwards, trained as a Family Physician” Family Medicine is a noble and challenging field of medicine. We take care of patients of all ages, we are trained in obstetrics and pediatrics, we perform many outpatient surgical procedures, and have experience in every field of medicine. Working in underserved care, we help carry some small fragment of our patients’ burdens and fight for healthcare justice on their behalf on a daily basis. It’s a struggle sometimes, but I am incredibly proud to be a Family Medicine Physician.
From what I can tell, Dr. Ben Edwards no longer practices Family Medicine. Or least, he doesn’t just practice Family Medicine. While the point of this post is to address Dr. Edward’s arguments in the video and not his philosophy of medicine, it is important to understand that despite the credentials and training background he shares at the beginning of his testimony, he now practices fringe, non-evidence-based medicine.
Take a look at the price sheet from his clinic’s website. Yes, there are some evidence-based services here; I am very thankful that his clinic is providing cervical cancer screening, and I certainly do cryotherapy for appropriate skin lesions in my own clinic. But they also provide a variety of unproven services like ozone infusions and ultraviolet blood irradiation.
As Dr. Edwards essentially states in the video, he does not believe in limiting his practice to only what is supported by scientific evidence. Maybe you believe in some of these treatments and maybe you don’t. Maybe you are curious about UV blood irradiation therapy or you believe that in vitro studies on the effects of ozone against cancer cells means it will really cure cancer (fire also kills cancer cells in a petri dish, but you wouldn’t inject it into your body). Maybe you are like me and believe this is essentially modern day snake oil. At the very least, I hope we can all give Dr. Edwards the benefit of the doubt and assume that he, at least, believes in his own medicine. Honestly it doesn’t really matter, because the main point is this; when a doctor tells you that he doesn’t believe in scientific evidence, why would you give credence to his testimony about scientific evidence?
0:30 “Did my undergrad at Baylor” I love Baylor University, despite its flaws. I have great friends that work there, men and women I greatly respect and admire who are working tirelessly to help it become the best university it can be. I’ll even be teaching a class there in the Fall. Still, I never studied there and am only a Baylor Bear by proxy, so this doesn’t hit too close to home.
0:31 “UT Houston Medical School” Great, fine. I went to UC Denver.
0:33 “And then Waco for Family Practice Residency where I was Chief Resident.” Uh-Oh.
The reunion is going to be awkward.
Now, Dr. Edwards and I trained more than a decade apart and we’ve never actually met; but I know doctors who trained with him, and I feel like a doctor who trained in my clinic, who probably even saw some of the same patients I’ve cared for, sharing false information before the state legislature definitely puts me in a position of “come get your people.”
0:57 “I’d like to begin with a reminder to everyone on the definition of Evidence Based Medicine“ When I first watched this video I did not know about Dr. Edwards’ alternative practices, so I was expecting something pretty standard and uncontroversial here. Most of the doctors I’ve argued with on this blog (I should say “argued against“, not with, since none of them know I exist) have portrayed themselves in the position of sharing scientific evidence, even when such evidence was anecdotal or when their analyses were utterly incorrect. None that I know of have actually come right out and said that evidence doesn’t matter to them, which is why I was so surprised by what came next.
1:09 “The elements of Evidence Based Practice are the integration of best research evidence with clinical expertise and patient values.”
Here’s the full quote if you want it. The landmark article was published in 1996; I’m assuming he found a later quote of the same article, which is where the 2002 in his citation comes from. So far, we are all on the same page.
“Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research.”
-David L. Sackett, OC FRSC, et al. Evidence Based Medicine: What it is and what it isn’t. British Medical Journal, 1996
Whoa, whoa, whoa. Hold up a second. Is that what Dr. Sackett meant? Is that what “integrating” means in the original quote, that one always trumpsthe other? Of course not. Yes, patient values always overrule anything else we do in medicine; but that’s the ethics principle of patient autonomy, not the best practice for harmonious, evidence-based patient care, where the physician and the patient work together to find an evidence-based treatment that corresponds to the patient’s goals and values. In order to understand Dr. Edwards’ subsequent comments better, let’s look at what that quote actually means, and how his interpretation of it completely turns it on its head.
Example 1: Insulin for Diabetes. Integrating patient values, evidence, and clinical expertise. I will use this illustration becomes it’s a conversation I have multiple times a month. Let’s say you have a diabetic patient whose blood sugar is still not well controlled despite taking multiple oral diabetes medications. The best evidenceon helping that patient prevent the terrible long-term effects of uncontrolled diabetes says it is time to talk about starting insulin. And for most patients, that’s what ends up happening. But the principle of integrating evidence with clinical expertise and patient values means that decision is a discussion, not something you can arrive at with a flow-chart or a “Idiocracy” style medical computer interface.
That discussion is focused on your patient’s values. How do they feel about insulin? What is their personal or family history with insulin? For many people who have a family history of diabetes, insulin carries an emotional weight; it represents the point where their loved one’s diabetes began to take a more severe toll on them. Of course there’s good reason for that, we give it for more serious cases of diabetes; but I’ve often spoken with patients who genuinely believed that insulin would make you lose your leg or your eyesight based on associations they have had since childhood. Even when we carefully discussed that this was actually due to the uncontrolled blood sugar levels the insulin was prescribed to treat (and my patients typically see that distinction right away once I really explain it), the emotional impact of starting insulin remains. For others, the inconvenience of daily or multiple-times-per-day injections or the barriers involved in administering the medication may represent an insurmountable barrier.
And this is where clinical expertise comes in, to help bridge the gap. The doctor, who has (hopefully) earned the patient’s trust and proven themselves a reliable source of health information and wise counsel, now has to figure out how this evidence relates to this specific patient. The person is a person and people always fit imperfectly into diagrams and algorithms. Maybe the evidence says insulin is indicated at this point, but you also know this patient was recently on a long taper of steroids for resistant poison ivy; steroids that drove up the blood sugar and gave the impression of worsening diabetic control. Maybe your patient has such a negative association with insulin that this discussion itself was the wake-up call they needed to take greater ownership of their health, and you truly believe they are going to be able to get their blood sugar down through dietary changes, exercise, and better adherence to their other medications even without the insulin. Or maybe you are seeing not just the high blood sugar numbers, but also the early signs that the diabetes is taking a toll on their body; the early signs of neuropathy in the feet, the subtly worsening renal function, the minor scrapes and wounds that just aren’t healing like they used to. In that case, integration of evidence, expertise, and patient values may mean helping your patient find a way to be ok with starting insulin, and walking alongside them knowing it’s a really difficult decision for them; or helping them fully grasp the medical realities they are facing so they can make the most informed choice possible, even if it’s not the one you were hoping for. Your medical expertise doesn’t mean practicing against the evidence or ignoring the evidence any more than it means trying to overrule your patient; it means combining your understanding of the evidence with your relationship with the patient to help the patient thrive. It’s why we have doctors in the first place.
Contrast this to Dr. Edwards’ misrepresentation of these concepts.
“Patient values trump clinical expertise, and clinical expertise trumps the scientific evidence.”
Dr. Ben Edwards, Just Now
Example 2: Antibiotics for Viruses. Patient values trump clinical expertise; clinical expertise trumps evidence. There are a million examples we could use to illustrate the model Dr. Edwards seems to espouse, but this one is prototypical. Let’s say you have a patient come in for upper respiratory symptoms; cough, runny nose, slight fever, etc. (for the sake of argument let’s say it isn’t in the middle of a global respiratory viral pandemic). You have diagnosed the patient with an upper respiratory virus, and they tell you they would like a prescription for antibiotics. Since they have no indication for needing an antibiotic, prescribing one would be a medical error; probably not a dangerous error, but it’s possible; antibiotics are notbenign medications. Normally, this would be an opportunity to educate your patient. This is one of the most important roles physicians have; we have the privilege of years of high level medical training that almost none of our patients had access to; it is a true joy to see your patients more empowered and more knowledgeable because of their relationship with you. Under Dr. Sackett’s model, this would be part of integrating patient values and medical evidence.
Or you could take a different approach. If you believe that “patient values trump clinical expertise, and clinical expertise trumps scientific evidence,” you could do some pretty modest mental gymnastics to convince yourself that your patient wanting an antibiotic is part of their “values,” and therefore the right medical decision despite there being no evidence that it will actually help them, and plenty of possibility that it will harm them. By treating preference or assumption as though they were values and autonomy, you have moved from evidence based, patient-centered care to retail medicine; just give the people what they want. A doctor who has fully embraced this philosophy of medicine won’t help you reach a diagnosis, won’t help you get treatment supported by the full weight of thousands of years of learning about the human body that humans have acquired, and won’t help you face harsh realities about your health and learn to cope with them. Such physicians, whoever they may be, have apparently decided that their hard-won medical degrees and board certifications were really just a means to gain the power to prescribe treatments; not to take on the responsibility to use that knowledge and experience in the best interest of their patients.
Thanks Uncle Ben, we needed to hear that.
But the second part of Dr. Edwards’ quote is even more disturbing, if only because it is seemingly so much more common. “Clinical Expertise trumps Scientific Evidence.” In the best light, this mindset seeks to portray the Physician as the Lone Ranger, a maverick that plays by their own rules and uses common sense instead of all that med school learning. They don’t need fancy books and studies to tell them how to care for their patients, they just know. The went to the Med School of Hard Knocks, etc. And the scary part is that we are all really at risk to fall into that mindset and paint ourselves in this light.
But every single time, it’s because we as Physicians have fallen into one of three professional sins; hubris, avarice, or laziness. The former abandons evidence, holding their own clinical experiences higher than the accumulated experiences and careful analysis of their peers around the world, because they think that they alone are capable of intuitively navigating the minefield of confirmation bias and tunnel vision that constantly threatens those who seek to heal. The second abandons evidence because it simply isn’t profitable; a lot of evidence based treatment involves sitting with the patient in the midst of pain and difficulty, helping them find internal resilience and make healthy choices, or prescribing simple, affordable (with the right advocacy) medications that you will never see a dime from (your doctor doesn’t get a cut of your prescription medications!). Instead choosing to push designer, unproven and unregulated treatments can be incredibly lucrative; all doctors know that our medical degrees could be incredibly profitable if we abandoned medical ethics; it’s a temptation we all see coming a mile away, but some still fall into it. The third; well, it’s the easiest of all to understand. I would love to tell myself that my clinical expertise trumps scientific evidence because it’s comforting; it means it’s ok if I can’t keep up. Medicine is hard, and there’s a lot of it; human health and disease is a vast and complex field. If arrogance and greed aren’t my bugbears, this one definitely is; I know I have the tendency, like Dick Van Dyke’s character in Scrubs, to rest on my laurels and lean on my own understanding because I just don’t have the energy. I have to fight that temptation every day.
Saying my clinical expertise trumps the evidence is really just a self-assuring way of me saying that my clinical expertise trumps everyone else’s.
Vaccine Safety
1:29 “I am also concerned that the forced and coerced COVID-19 vaccinations would be a violation of the Nuremberg Code, etc.” I completely agree, and as a Physician I would never support any forced or coerced medical treatment of any kind; patient autonomy is sacred.
I also don’t know what he’s talking about; I’ve heard exactly zero evidence that anyone is being forced or coerced into being vaccinated against COVID-19. When patients come to see me and we discuss the vaccines, we look at the evidence together and I help them integrate their values with the best available evidence. We don’t shoot needles in their arms as they walk in; we don’t deny them services if they don’t want the vaccine. Right now, I don’t know of any businesses that deny service if you aren’t vaccinated, and I certainly don’t know of any government services vital to health and human thriving that do so either. I’ve heard of some sporting events- huge gatherings that are entirely voluntary to attend and have the potential to become super-spreader events- having separate entrances or seating sections for unvaccinated and vaccinated attendees. Surely we do not consider this to be tantamount to forcing or coercing vaccines? I always want to look at the strongest argument from the other side; if you know of a situation that comes closer to truly forcing COVID-19 vaccinations on people, please send it my way.
2:00 “According to the CDC’s vaccine adverse event reporting system (VAERS), 4,178 deaths are now being reported.“ I think this is the most important point in the entire video, and it’s worth spending some time on. This is a similar claim to one that’s been circulating on social media, and even repeated earlier this month by Tucker Carlson. And the thing is, it’s a fascinating bit of misinformation. Let’s dive into it.
Dr. Edwards shares a number that is incredibly easy to find; the number of deaths reported in VAERS for all people who have received a dose of the COVID-19 vaccine. You can find the numbers for yourself; start by going to https://vaers.hhs.gov/data.html and clicking through until you find an option to search the VAERS data, then select the COVID-19 vaccines and run a report on ‘deaths’. It took me less than 5 minutes to figure out how to run the report, and I’ve never used the system before. Nobody is trying to hide this data. I will note, however, that you have to indicate that you agree that you have read and understood a disclaimer that you can’t use this data the way Dr. Ben Edwards is using it in this video because that’s not what it means at all. At the very least, Dr. Edwards is guilty of breaking the website’s end-user agreement.
Running the report right this second gives me a figure of 3,919 deaths of persons who have received at least one dose of the COVID-19 vaccine; close enough to Dr. Edward’s 4,178 that we won’t split hairs about it. So we agree on the numbers, which are publicly available. The more important question is what the numbers mean.
Remember last year when we repeatedly saw the claim that deaths from COVID-19 were being inflated to make the pandemic look more dangerous, and that all deaths at any point following COVID-19 infection were being called “COVID Deaths,” even if someone got shot or hit by a car or died of cancer. I debunked this one over and over again, but the key to understanding that misinformation hinged on understanding death certificates. Those numbers of COVID-19 deaths were not raw data of ‘everyone who had died’ around the time they had COVID-19; there were based on the detailed reports of physicians, coroners, and other medical experts who had to analyze the cause of death and file a report, with their name attached, in a specialized system that not everyone has access to. If a death is reported as being from COVID-19, it is because a medical expert believed that COVID-19 contributed to or caused the death.
But the VAERS system is the exact opposite. As the disclaimer on the VAERS website says outright, this is raw data without any analysis attached. It can be submitted anonymously and by absolutely anyone. And it absolutely includespeople who happened to die from car accidents and gun shot wounds at some point after receiving the COVID-19 vaccines.
And I find this really fascinating because it really seems like after a year of saying the CDC and WHO and your Family doctor down the street were just attributing every death to COVID-19 to inflate the apparent danger, which wasn’t true at all, the medical misinformation spreaders decided that was actually a great idea and decided to do that exact thing with the COVID-19 vaccines! “If you can’t beat ’em, join ’em!”
So now that we understand a little better why the VAERS data can’t be used the way Dr. Edwards is trying to use it, to say that those 4,178 deaths are due to the COVID-19 vaccine, let’s look at what that data does mean.
The first question we have to ask ourselves is, is this more deaths than we would expect in this population even if people didn’t get the vaccine? This is a concept called attributable mortality, and it’s been one of the major proofs of the real danger of the COVID-19 virus against all of the misinformation claims over the past year. We can’t get perfect data from the VAERS system (because, again, that’s not what it’s for), but what we basically need to ask ourselves is whether the death rate in those who received the COVID-19 vaccine is any higher than the rate we would have expected from all causes anyway. Let’s do that math.
To date, 158.4 million Americans have received at least one dose of the COVID-19 vaccine, which became available to the public just over 5 months ago on December 14th, 2020. That’s just below half of the US population. Half the US population with at least one vaccine dose; 4,178 deaths reported on VAERS since we started vaccinating. In that same time period, there have been over 1.4 million deaths in the US. Or to put it another way, in a population of 158.4 million people we would expect about 517,924 deaths in the amount of time since we started vaccinating people. And that’s based on pre-COVID mortality rates.
So among the people who receiveda dose of the COVID-19 vaccine, VAERS reports far fewer deaths than would be expected in the normal population in that time period. Does that mean that the doctors and nurses are lying about vaccine safety? Does it mean that the CDC is changing the numbers? Does it mean the COVID-19 vaccines are protecting people against more than just COVID? Does it mean they are bestowing some degree of immortality or vitality on people, protecting them from heart disease and diabetes and gunshot wounds?
No. It just means you can’t use the data that way because it doesn’t represent what Dr. Edwards is telling the senate it represents. That’s it.
2:00: “Over the past 20 years, all vaccinations combined there were a reported 4,182 deaths.”
The second question we have to ask is why the deaths reported on VAERS (I won’t say ‘the deaths associated with the COVID-19 vaccine’ the way he does, since we just saw why that is not accurate) in the past 4 months rival the deaths reported from all vaccines in the past 20 years. Surely that, regardless of the small number of deaths compared to the general population, indicates that these vaccines are far more dangerous than ‘traditional’ vaccines we’ve been using for years, right?
No. Again, it entirely depends on what those numbers mean, and the fact that we are reporting adverse events differently for the COVID-19 vaccines than we have for vaccines in the past. This is not clandestine or hidden information; it’s right there on the VAERS website under the reporting instructions. Look at the instructions for medical professionals for reporting adverse events following vaccines, from the VAERS reporting FAQ:
For most vaccines, we report adverse events that have a credible link to the vaccine itself, such as an allergic reaction, and any serious events that occurred within a specific, limited time period following the vaccine. Here’s a preview of the table they mention and link to above:
So for the DTaP vaccine, for instance, I would obviously report a severe reaction like anaphylactic shock, if it occurred within 7 days of the vaccine. Anaphylactic shock doesn’t occur a week after a vaccine, and yes this would mean that I would still report it if the patient got a vaccine on Monday and had an anaphylactic reaction to a bee sting on Sunday… But that’s really unlikely, and they have to set a reasonable, liberal time-period. If the patient dies from that anaphylaxis or complications of the reaction, that gets reported too. If the patient is shot, or they develop sepsis from a pneumonia, or their heart failure claims their life, those events don’t get reported because there is no theoretical link between those events and the vaccine; that data is being filtered through clinical reasoning. Which makes sense, because in the past 20 years about 60 million Americans have died; some of those folks happened to receive a vaccine of some sort around the time of their death, but with no plausible causal link there would be no reason to report those deaths on VAERS; it would be entirely unreasonable and misleading to do so.
Now look at the instructions for COVID-19 vaccine adverse event reporting, from the same FAQ:
If a patient dies at some point after receiving the COVID-19 vaccine, healthcare professionals are required to report it. Even if there is no theoretical link; even if there is no possible causal link, such as the reports in VAERS involving traffic accidents and end-stage cancers. If a patient dies and the clinician knows they have been vaccinated against COVID-19, they are required to report it in VAERS, full stop. That’s not the case with other vaccines, so it makes sense that many, many more of the deaths that occur every day as a part of normal human life will be reported on VAERS than ever before. And that’s a good thing; it’s better to have that data than not have that data. But using that data in a way it was never intended, to scare people away from safe and life-saving vaccines, is either ignorant, unethical, or both; you are told before you even pull of the data what it represents, and my hope for Dr. Edwards is that he simply didn’t understand this when he testified in front of the state senate; to knowingly misrepresent this data is simply lying.
The other thing you’ll notice from the above instructions is that, unlike with the TDaP or MMR vaccines, there is no time limit on COVID-19 vaccine adverse event reporting. That means that, while deaths within a week or two of the vaccines are more likely to be reported because the professional treating the patient is more likely to be aware of their recent vaccine, it is still technically required to report deaths on VAERS even 4 or 5 months after vaccination. The same goes for all adverse events. And lest you think it’s far fetched that any of the data on VAERS is coming from that long after people got vaccinated, just remember that if you signed up for V-SAFE to report adverse events to the CDC on your smartphone, you were still getting these texts months later:
I was vaccinated in December
So to summarize, those 4,178 deaths that Dr. Edwards mentions are an incredibly small percentage of the people who have actually died in the US in the past 5 months, those deaths reported on VAERS are explicitly stated by the reporting system itself to not represent a causal link with the vaccines, and out of 1.6 million people who have been vaccinated it is a statically insignificant figure. And the rules for reporting adverse events to VAERS are different for the COVID-19 vaccines than for other vaccines, both in the types of events reported and in the length of time since vaccination that a report is required; comparing the “deaths associated with the COVID-19 vaccines” on VAERS to the “deaths from all vaccine over the past 20 years” isn’t just comparing apples to oranges; it’s a total misrepresentation of the data. It’s a scare tactic, plain and simple.
2:29 “This includes a 15 year old boy in Colorado, two 16 year old girls in Wisconsin, a 17 year old girl in Wisconsin, and a 17 year old boy, all healthy, in New Hampshire.” If these 5 teenagers have died it is absolutely a tragedy. At this point we do not know anything about them; their names, their medical conditions, their history, or what led to their deaths. We don’t have that information because it isn’t in VAERS, and because there are no independent, verified reports of these deaths available. You can search for local news stories or articles about these individuals and so far there don’t seem to be any details of these situations; no information other than that they died at a tragically young age, and that they had receive the COVID-19 vaccine at some point; and all of that only from VAERS itself. Remember that the VAERS reporting system is anonymous, open to anyone, and that none of the reports are verified. In fact, though we know that the COVID-19 vaccines have never been given to children younger than age 2, even in clinical trials, when you run the numbers on VAERS there are well over 200 reports of adverse events to the vaccines in that age group. This is raw, unverified data from the public and it has to be understood as such.
The CDC really does investigate these cases; far from the conspiracy theories about the CDC trying to cover up vaccine injuries, the whole goal of V-Safe and VAERS is to help us make sure the vaccines are safe, and a lot of resources are devoted to following-up on these reports. When there are reports of deaths in teenagers who have received the COVID-19 vaccine, that deserves attention and an assumption of authenticity; but there is no reason to believe that the COVID-19 vaccine they received contributed to the death; VAERS can’t tell us that. What we actually have is basically, “someone went online and reported a death in a teenager who had been vaccinated against COVID-19. We need to look into this.” By transforming this into “the COVID-19 vaccine killed this teenager,” Dr. Edwards is not advocating for the teenager and their family. He is not bringing light to their situation. He is simply using the report of that death in VAERS to create fear, with no understanding of the circumstances around that death and no knowledge of the people affected by that tragedy. We cannot use other people’s tragedies, which we know nothing about, to promote our own political agendas.
2:42 “The evidence is pretty clear that VAERS grossly underestimates the adverse events that are reported... Only 1% of adverse events are ever reported to VAERS.” This is absolutely true, but before you let Dr. Edwards guide you into inaccurate assumptions, you need to realize the subtle switch he’s just made.
Up until now Dr. Edwards has been talking about deaths reported in VAERS. He’s given numbers, he’s given tragic examples. He’s been trying to convince you that the number of deaths “from” the COVID-19 vaccines has been astronomical. Without any clarification or verbal signal, he has now switched from deaths to adverse events.All adverse events, including mild reactions. So when he tells you that ‘4,178 people have died from the COVID-19 vaccines’ (which isn’t true), and then immediately tells that “less than 1% of adverse events are reported to VAERS,” he wants you to do some quick head math and say to yourself, “Wait, that means that over 400,000 people have died from the vaccines!” If that number sounds crazy to you, it’s because it is. We passed 400,000 deaths from COVID-19 in January of this year (we are now pushing 600,000). It took 11 months from the first American COVID-19 death in February 2020 to get to that point, and at various times in the pandemic our hospital systems were utterly overwhelmed. If we were now seeing 400,000 deaths from the COVID-19 vaccines in 5 months, you wouldn’t have to watch Dr. Ben Edward’s testimony on Facebook or YouTube to hear about it; you would be seeing it in your hometown, you’d be hearing about it from your friends and family who were affected by it personally. Your local hospitals would be on divert and over-capacity like they were because of COVID-19 back in December. No, the COVID-19 vaccines are not causing massive numbers of deaths. In fact, they are very, very safe.
So where does that 1% statistic come from? Well let me ask you; when you had a sore arm from the Flu shot last year, or your child spiked a mild fever due to their MMR shot and you had to give them tylenol, did you report it on VAERS? No; I didn’t either. We could have, it would have been totally reasonable to do so; but since those were expected, mild, self-limited reactions to the vaccines it never occurred to us to report them. The more serious reactions are reported at much higher rates, which is exactly the way VAERS is designed. There’s a great discussion of this phenomenon on Vaxopedia, and since they’ve done the literature review already I’m going to steal some of the studies they cite.
Serious reactions, and especially deaths that clinicians believe might be linked to a vaccine, are going to be reported at high rates, while mild, expected reactions will be reported far less than 1% of the time. Dr. Edwards uses “deaths” and “adverse events” almost as synonyms in this section by not clarifying what that 1% statistic really means. At the end of the day, the Vaccine Adverse Event Reporting System is doing exactly what it is supposed to do; providing huge amounts of raw data that we can search for unexpected patterns and then form hypothesis. Unfortunately, any time raw data is publicly available, there is the risk that people, including physician scientists who trained in Waco, will latch onto the data and use it to weave false narratives, stoking unfounded fear and panic.
3:44 “Personally I have received numerous reports from family members of my patients, close friends of my patients, that within hours to days of receiving the vaccine they have suffered from stroke, heart attack, pulmonary embolism, blood clots, and death.”
I also see patients every day, and many of my patients have received their COVID-19 vaccines. I couldn’t give you an estimate of how many. My patients are typically excited to show me their vaccine card and we celebrate together that they now have better protection against the virus. I always ask if they had any side effects, and I often hear about body aches, chills, nausea, fevers, malaise, and fatigue; “All the things you told me to expect, Dr. Webb.” I also talk to plenty of patients who had a sore arm, or no side effects at all. I have had no patients tell me about a dangerous side effect or death they believed was related to the COVID-19 vaccine.
How do we reconcile this? One of two ways. Either one of us, me or Dr. Edwards, is lying; or at least exaggerating. Or else, we are receiving the types of narratives from our patients that they expect we will resonate with and appreciate. My patients know I am a vaccine advocate and I want to see them protected against COVID-19. Some of them know I write about COVID-19 misinformation. Many decided to get vaccinated after we talked about the vaccines and I answered their questions. It’s entirely possible that my patients are more apt to tell me about their minor symptoms. But isn’t the opposite at least as true for Dr. Edwards? My population of patients are from all walks of life, all backgrounds; his are self selected; they have specifically chosen his clinic because they are strong believers in homeopathic and alternative medicine and want those services. Their doctor is against vaccines and they likely know it just as much as my patients know I am for them. Wouldn’t his patients be apt, even anxious to share vaccine horror stories they had heard with him? And of course, referencing these stories later while trying to make a point, how much verbal precision can we expected someone to exercise in distinguishing between “my patients have told me they’ve heard stories about serious adverse events from the vaccines” and “my patients’ friends and family members have experienced serious adverse events from the vaccines.” It’s the most important distinction in the world; it’s also exactly the kind of distinction most of us wouldn’t scruple to make if we really believed our point was valid and wanted to emphasize it as strongly as possible. Adverse events, like jokes, are best when told in the 1st person.
Vaccine Immunity vs. Acquired Immunity
4:19 “Studies have shown a 2-3 fold increase risk of adverse reactions to this vaccine if you’ve already had COVID.” I am not familiar with the studies he is referencing here, but I don’t doubt this for a moment. We already expected this because of the more robust set of side effects we’ve seen with the second shot in the Moderna and Pfizer vaccine series; in fact, I’ve been counseling my patients to expect more robust side effects if they’ve already had COVID-19 for months. It certainly matches my experience; I had COVID-19 in December and got the vaccine a few weeks later; I had body aches, chills, and nausea after both doses, not just the 2nd, and I’m sure it was because I had already had COVID-19.
Remember, he is not saying there is a 2-3 fold increase in injury or death from the COVID-19 vaccines if you’ve already had the virus; just in adverse reactions. Most of the adverse reactions we experience are related to our body’s immune response to the vaccines; they are part and parcel of that robust immunity we are hoping for. We get fevers after vaccines because of Interleukin-1, which the macrophages that pick up the viral proteins release to stimulate B and T cells. We get body aches and headaches because of the Interleukin-6 those cells produce to turn the B cells into antibody producing plasma cells. We feel tired because… Well, nobody really knows; but all of that immune response does take up a lot of energy. Yes, you are more likely to have adverse events after the COVID-19 vaccine if you’ve already had COVID-19, because your immune response is more robust; those “adverse events” are the symptoms of your immune system working.
4:26 “Natural immunity confers a more robust immunity than vaccine immunity could.” Dr. Edwards repeats this idea multiple times in the next minute, and there was a time I would have agreed with him; intuitively it seems like that would always be the case. But it isn’t true. This is an area where I was skeptical at first, but the data has forced me to change my mind; the COVID-19 vaccines really do create a stronger immune response than our own natural response to COVID-19 once we’ve recovered from it. My friend and medical misinformation hero Dr. Emily Smith has written bout this before, and she’s better at explaining things than I am:
So Dr. Edwards is simply incorrect on this point. But it’s not a competition between your body’s response to COVID-19 and your body’s response to the vaccine, because his assertion that it is dangerous or unwise to vaccinate someone who has already survived COVID-19 is inaccurate; it’s actually the best immunity you can get, if you were unfortunate enough to already get sick from COVID-19 like I was.
This kid gets it; disease acquired immunity and vaccine acquired immunity together is the best protection you could hope for.
5:03 “God gave us an amazing, robust immune system, and I don’t think you can improve on God.” Absolutely! I complete agree. I was writing about how awesome our immune system is, and how we ought to treat it, back at the beginning of the pandemic. I’m a big, big fan of my immune system.
You know who else was a fan of the immune system? The folks who invented vaccines. Vaccination came to the United States from, among other sources, an enslaved African man in Boston whose knowledge of the African traditional medicine practice of inoculation helped save hundreds, maybe thousands from Smallpox in the 1720’s. We don’t know his true name, but his slave name was Onesimus, and it’s only in recent years that his insight and knowledge is bringing him the credit that was previously received only by the man he shared these with, the Boston doctor who owned him.
Onesimus, like the traditional healers before him and the vaccine pioneers since, understood that the immune system is an incredibly powerful defense against disease, but that it works best when it knows what it is fighting. By giving the immune system a template- previously by injecting a small amount of live pathogen into the body through inoculation, but now by presenting it with just a few key proteins (that cannot cause disease) through vaccination- we unlock the immune system’s full, robust, God-given disease-fighting potential. Vaccines are not an improvement on God’s design; that’s just anti-vax propaganda. They are the best way we have to arm the immune system with the information it needs without having to actually get sick in the process.
Imagine you want to assassinate someone (for the sake of argument), and you hire the world’s best assassin. You pay her exorbitant asking price, all up front and in unmarked bills, and receive her guarantee that the job will be done. Finally, you try to tell her the name of the target, maybe even hand her a picture and dossier; she plugs her ears and won’t look at the picture. “I’m the world’s greatest assassin,” she says, “I don’t need to know who the target is.”
That’s what it sounds like, saying we shouldn’t try to “improve on God’s design” of the immune system with vaccines.
Before I started blogging about medical misinformation, my last blog (which lasted for exactly one post) was called “Mad Virtues.” It was based on this quote from G.K. Chesterton:
“When a religious scheme is shattered it is not merely the vices that are let loose. The vices are, indeed, let loose, and they wander and do damage. But the virtues are let loose also; and the virtues wander more wildly, and the virtues do more terrible damage. The modern world is full of the old Christian virtues gone mad. The virtues have gone mad because they have been isolated from each other and are wandering alone.”
G.K. Chesterton
While my intention was never to deny the existence either of real nefarious intentions in the world or of original sin, my thesis was that most disagreements, and especially the most deeply felt and violent disagreements, were actually due to a clash of deeply but disproportionately held virtues; virtues that had gone mad, and caused terrible damage, because they had been isolated from the other virtues and truths meant to keep them in check.
In general, I believe this is true today, and I believe it applies to the content of this blog. I think that people like Dr. Richard Bartlett or Dr. Ivette Lozano really believe they are doing the right thing by treating all of their patients with budesonide or hydroxychloroquine, and encouraging people around the country to seek out these unproven therapies for mild COVID-19 cases. I think Dr. Dan Erickson and Dr. Artin Massihi really convinced themselves that their erroneous statistics were valid, which allowed them to view the harm that the shutdown was causing to their own business and the economy around them as a greater threat than the virus. I even believe that Dr. Judy Mikovits, with 20 years of fighting the medical field and presumably becoming increasingly entrenched in narratives of far-reaching conspiracies among doctors and scientists, earnestly believes that her Plandemic interview was an opportunity to expose the “truth” about the virus.
In each of my responses to each of these viral misinformation videos, I have tried to assume the best; that the intentions of those making the videos, like those sharing them, were sadly misguided, misinformed, and erroneous, but ultimately sincere. I hope that if I ever fall into unintentional but very public professional error and embarrassment, the same grace would be shown to me. But today I’d like to try something a little different; instead of assuming the best, I’d like to assume the worst; I want to ask what the game plan would be if a doctor were in fact knowingly lying about the virus; what they would stand to gain from such an immoral act.
Are most doctors lying, or just a few?
As soon as we abandon the idea that deeply held differing opinions dramatically shape our perception of events and even our understanding of statistics (in other words, that most of the doctors who are deceiving others are only doing so because they have already deceived themselves first), we are left with only one alternative conclusion; someone is deliberately lying. So who is it? According to a recent tweet that was retweeted by the president, it’s most doctors.
If we follow this theory, we are going to arrive at some uncomfortable but fairly inevitable conclusions. First, it means that I am lying, because on this blog and in my conversations with patients, family, and friends, I’ve consistently been repeating the ‘party line’ that COVID-19 is very dangerous and encouraging people to exercise caution and take it seriously. It means that when I told you in my last blog post that I was worried about a lot of my patients who have pre-existing heart and lung disease, I actually just wrote that because it made me sound like a compassionate doctor. It means when I said at the end of June that I was seeing a steep rise in the number of positive tests at my clinic, I was making that up and just banking on none of the nurses or lab techs I work with reading that and calling me out on it (I don’t have to worry about the other doctors; they are all in on it too). It means that the long nights and early mornings and sacrificed Saturday afternoons it has taken to write this blog on the side of my full-time clinic job has been motivated not by the stated desire to provide clear (if a bit long-winded) refutations and explanations to dangerous medical misinformation, but by a desire to run a convoluted and ineffective interference to people like Love Connection up there tweeting the truth about the virus. And all I can say is, hey, I’m just as shocked as you are. My wife is going to be very upset when she reads Mr. Woolery’s tweet and realizes that the reason I’ve failed to build her that Ana White potting bench for the past month is because I was busy deceiving some very, very small segment of the American public.
It also means my friends from medical school and residency have been lying, not just to the public but also to each other. Since late March I’ve reconnected more frequently and with a wider range of former classmates and co-residents than I have in years as we’ve checked in on one another and provided updates and insights from our own experiences with the virus. I’ve talked with friends working in the ED in New York during their worst weeks of crisis, and with friends working in rural hospitals that have seen hardly any COVID-19 at all. You could fill libraries with the texts, e-mails, and facebook messages that have taken place between doctors in the past 4 months, and not a one of those has been to clarify the latest lies the WHO, CDC, Bill Gates, and Dr. Fauci want us to push this week (not exactly true; that has been said a lot and is actually a pretty tired joke by now. At least, all of my friends are tired of me making it). If those texts and e-mails are ever subpoenaed, the American public is going to learn a lot; but not about any conspiracy.
Crimes against punctuation and grammar, yes. Against humanity though?
And by the way, not all of those conversations are private, although more are now because of social distancing. Even though we aren’t sitting at coffee shops having these discussions, many take place on very public Facebook comment threads instead of private messaging, and a pediatrician friend and I have had more than one of our Google Hangout Dungeons & Dragons sessions derailed by comparing notes about the virus while the rest of our party waited patiently for us to get back to the quest at hand. If you believe that most doctors are lying about the virus, you have to believe that these types of conversations are actually planned and carried out to deceive friends and loved ones who are not doctors. There’s a joke about ‘rolling a deception check’ in there somewhere, but I don’t have the emotional energy to think of it. Every time you see two or more doctors talking about the virus, how dangerous it is, or what they’re doing to fight or prevent it, that’s a staged performance for the benefit of the public.
Nailed it.
So why all of this lying? We have consistently been given two explanations; because we want to hurt the economy (in order to hurt Donald Trump’s chances of re-election), and because we want to make money. You might notice right away that these two motivations almost but not exactly completely contradict each other. I’m sure it is possible to both want to hurt the economy overall and stand to make money yourself (and here I’ll be called naive by friends who believe that this is essentially the go-to strategy of the ultra rich), but for someone earning a wage like a physician it must be somewhat rare; we would really have to spend some time with a fresh cup of coffee and some excel spreadsheets to make sure that the ‘extra money’ we were making would be enough to offset the hit to our 401k’s and Roth IRA’s, not to mention the doctors who actually own stocks. Honestly, I’m surprised the White Coat Investor hasn’t done an article on “5 financial reasons you should trick people into believing in COVID-19 (and 5 reasons you should blow the whistle on this global conspiracy of doctors and scientists now!).”
If we look at them separately, the first one feels like the type of thing that makes sense only if you forget that you actually know some doctors, and makes even less sense the more doctors you know. For me it’s easy to intuitively disbelieve that doctors as a group are out to get Donald Trump because for the past 13 years I’ve had to endure an almost endless stream of Fox News in every doctor’s lounge I’ve been in from here to Denver. But if you only know one doctor and they happen to vote the same way you do, you might think your doctor is ‘one of the few telling the truth.’ If they do think the virus is a pretty big deal, you might think they have nuanced and complex views on the pandemic, which is probably true, or that they are essentially honest but have been ‘tricked’ by the CDC or other doctors or whomever. But if you knew hundreds of doctors, like I do, you would have to face the reality that while there are many you like and trust and a few you don’t, and while they fall all over the political spectrum, you would be hard pressed to pick even a handful that would be willing to participate in anything like a conspiracy, and that as a group they would be even less likely to be duped by a medical conspiracy if there was one.
This guy’s definitely in on it, but I can’t think of anybody else.
Doctors are not a monolith, and we don’t vote as one. In fact, some of the medical specialties that have been most negatively impacted by the pandemic financially, like Surgery and Otolaryngology, and some that have been most intimately involved in COVID-19 treatment, like Pulmonology, Anesthesiology, and Emergency Medicine, are the exact fields that vote Republican at higher than average rates. There’s only so far you can take this information, and it’s probably true that Donald Trump has lost some physicians from his constituency since this data was collected just before the 2016 election; but at the very least it shows that that if COVID-19 were really a conspiracy to hurt the president, there would be thousands of Republican critical care physicians coming forward to reveal this, instead of a handful of urgent care and concierge medicine doctors. I personally know several doctors who are fighting the virus on the frontlines and still plan to vote for Donald Trump in 2020 despite being frustrated with his administration’s response to the pandemic; for them, a virus is not a political issue, even if it is being used as one.
But the second one is actually even more ridiculous. I’ll start with myself again. Of course it doesn’t matter since we’ve already established that I’m lying about everything, but I can tell you that I’ve made exactly zero extra dollars from COVID-19. I am thankful to work in a clinic system where my personal income isn’t determined by the number of patients I see or what type of insurance they have (our work volume is instead driven by the extensive primary care needs of the population we serve), and unless somebody votes to give frontline doctors hazard pay or student loan forgiveness, this pandemic seems extremely unlikely to be some sort of lucrative opportunity for me (I’ve got a pretty good life insurance policy, though, and my med school loans are non-transferrable, so it could end up being fairly profitable for Katie by the end)(grab a screenshot now, because she’s going to make me delete that one as soon as she reads it). I have put in dozens of hours of overtime, mostly back in March and April helping our clinic get ready for whenever the virus finally surged in our area, but this was all gladly done and entirely unpaid, and I certainly wasn’t alone in this. Since then I’ve spent many hours writing this blog, but it would be hard to argue that this is financially motivated either since so far the net earnings of tjwebbmd.com is negative whatever the cost of WordPress Premium is.
But not every doctor has the same type of employment contract that I have, and when we look at other types of business models we discover that my not especially profitable is the very best case scenario for most doctors during COVID-19. Remember that social distancing measures meant thousands of primary clinics cancelled any appointments they felt their patients could safely postpone as soon as COVID-19 cases began to rise in the US; despite the fact that many of them could ill afford to do so. Some of these clinics closed for good, and this unfortunate side effect of the virus, which is going to affect the health of many people for years to come, was actually put forward by COVID-19 conspiracy theorists alongside the idea that most doctors were lying about the pandemic, without any apparent irony. I know doctors that work for larger healthcare systems who were laid-off during the pre-surge months of the pandemic here in central Texas, not to mention surgeons cancelling elective cases and many hospitalists and ER docs working fewer shifts because hospitals volumes were so low (this is outside the scope of the discussion, but we talked about this phenomenon most recently in my response to Dr. Simone Gold and her A Doctor a Day campaign). For most doctors, COVID-19 has been either financially neutral or a financial hardship.
But what about that big $39,000 paycheck hospitals are presumably getting for putting a patient on a ventilator? We’ve dealt with this conspiracy theory before, and you can read all about it on Snopes.com, or you can wait until this weekend when we try to tackle this meme and a whole bunch of others on the blog. But even if you believed this crazy theory that doctors are intubating people who didn’t need it in order to get their hospital a big pay check (instead of, say, actively working to push the limits of non-invasive ventilation for every possible patient, which is what they are actually doing), consider what else you would have to believe to think this somehow explains “most doctors” lying about the virus: 1. The doctors are getting the money instead of the hospital (yeah, right), 2. the other doctors and nurses and healthcare professionals that know the patient’s case are complicit and staying silent in massive numbers, 3. ER docs are admitting patients who don’t need to be in the hospital just so that their critical care counterparts can get put them on ventilators and get those payments (“set ’em up, knock ’em down”), 4. other doctors who are not involved in the hospital care at all and cannot possibly get a cut of that money are lying about the pandemic and letting their practices get closed so that another doctor in town can make money intubating patients unnecessarily, and 5. they aredoing all of this despite their Oaths to do no harm, years of devotion to caring for people, a very real chance of getting caught, and, for about half, the fact that the whole conspiracy is designed to hurt a president they voted for in the first place.
That’s a lot. I’m not saying it’s impossible, but $39,000 seems like a pretty low-ball figure to betray all of the ideals we hold most dear and participate in some grand plot at the expense of the American people. Maybe come back when you can afford to pay us whatever the insurance companies pay their doctors to deny prior-authorizations all day.
You want a cure?
But what if it’s the other doctors who are lying? What if it’s not doctor after doctor I see on Facebook and Twitter saying ‘stay safe, please wear a mask, please do physical and social distancing in order to keep you and your families safe from the virus’ that are trying to deceive you with this advice because it somehow makes them money (Step 3: ???… Step 4: Profit!), but the handful of doctors writing things like this:
The social media post is about 2 weeks old by now, which I realize is ancient in internet misinformation time. One of the struggles of doing this as a hobby on the side of a full-time job. Regular readers will notice I’ve done something unusual for this blog: I’ve omitted the name of the author I am responding to. This is a fellow Texas physician a few hours north of here (whom I’ve never met), and his name isn’t hard to find; I’ve even mentioned him when referencing this post in prior essays and his post has been viral on social media. But I’ve omitted his name here because, unlike in those other essays, I plan to treat this post as cynically as possible. I’d like to work through this post and ask what we can conclude about this doctor’s practice style, COVID-19 testing and treatment policies, and overall goals in writing this post, and while I believe my worst-case-scenario conclusions are a valid interpretation, I sincerely hope that the real, living and breathing, created in the Image of God person who wrote this is better than he will get credit for in those post. He probably is, and so I’ve erased his name from his post and plan instead to treat the author as a fictitious person.
Dr. Lozano is the doctor who spoke about Hydroxychloroquine at the Set Texas Free Rally way back in mid-May. I wrote a response to her speech at the time and tried to address her use of Hydroxychloroquine in the outpatient setting for minimally symptomatic and even asymptomatic patients. Since the doctor in this post is using it much the same way, I won’t spend as much time on this and will to some degree take it as a given that we agree this is an improper use of the medicine, or at least that you have heard my side of the argument already.
I think this is a really fascinating set of claims, for a couple of reasons. First, as I said in the post responding to Dr. Lozano, numbers matter. This doctor claims at the end of June to have been treating people in the ‘outpatient trenches’ for 2 months, but like the rest of Texas, McKinney began to hit a surge in cases just about a week prior to his post; by the time of the post there had been less than 500 in the entire city, and fully half of those were in June; at the end of May the total confirmed cases in McKinney was 251. He goes on to say that he has treated ‘over 50’, (which, since we are being cynical today, means 51 or 52) patients relatively early in their disease course, trying to catch them 3-6 weeks before they would need the hospital; but with so few cases in April and May, how many of those 50 could possibly have made it to his 6 weeks post treatment yet to ensure they were out of the woods? The time course he lays out for concluding his treatment works and the time course he would have had to observe his patients’ response to his treatment just don’t line up.
But the saving grace for this post’s author on that point is that he could still get credit for most of the patients he treated this way up until about mid June, because the time course from first symptom onset to the rapid deterioration from Acute Respiratory Distress Syndrome in severe cases of COVID-19 is typically between 8 to 12 days. His time course of “starting treatment 3-6 weeks earlier” doesn’t make any sense, because the incubation period of the virus is 2-14 days and the time from symptom onset to clinical deterioration is typically 8-12 days or less; at the very most, a patient with a severe course of COVID-19 may have about 3.5 weeks from the time of their exposure to the point of requiring hospitalization, and that would be an extremely rare occurrence; most commonly it would be about 10 days to 2 weeks.
His citing a time frame of treating people 3-6 weeks before they would need hospitalization suggests one of two things. First, he could be comparing the start of symptoms to the time of death in patients that spent a number of weeks on the ventilator, claiming that hydroxychloroquine might have saved these individuals if they had been started on it 3-6 weeks sooner because he isn’tactuallyfamiliar with the hospital-based treatment protocols or clinical trials that used hydroxychloroquine, which certainly did not start the medication in the final days prior to the patient’s death, after they had already spent a couple of weeks in the ICU. Or second, he could be building a narrative that says COVID-19 really presents much earlier and can be detected by someone with special expertise or insight into the virus, which he happens to possess. The problem with this later one is that the incubation period means he reaches a firm time cap, the date of first exposure to the virus, long before he gets to his 3-6 weeks early; by claiming he is treating people 3-6 weeks before they would have been sick enough to need the hospital, he is essentially saying that he’s treating some people before they’ve even been exposed to the virus. If you just now thought, “wait, isn’t ‘treating people before they’ve even been exposed’ the same thing as treating people who are healthy and might not ever be exposed?”… Yes, yes it is.
“Fine, he has his time course a bit off; but his overall point is still valid, that maybe the medicine would work if it was started before the patient needed the hospital.” I think this is a common and very understandable stance, and there are so many different ways to approach it it’s hard to know where to start. We could point to the fact that notall hospital patients with COVID-19 who were treated with hydroxychloroquine had the same disease severity when they started the medication; if it were most useful early in the disease course, wouldn’t we have seen the less severe patients and those who were hospitalized earlier in their disease course derive greater benefit from it in all of the studies and the widespread clinical use it had a couple of months ago? Yet no such trends emerged to point us towards even earlier use of the medication. We could point out that it was doctors who started using hydroxychloroquine broadly in thefirst place based on some early anecdotal evidence and only stopped once more and better data was collected which unfortunately showed it wasn’t beneficial, which is exactly how science is supposed to work, and that both the idea of the president coming up with the treatment from his own research and the medical field abandoning it as soon as he endorsed it just to spite him are complete political fabrications. Here’s me and my friends texting again, this time on the same day President Trump mentioned hydroxychloroquine for the very first time.
Not pictured: My text a couple of hours later saying “whoops, Donald Trump mentioned this in his press conference today, so let’s abandon the drug even if it would have helped our patients. Too bad.”
We could also point to studies that have been done in exactly the clinical scenario in which this doctor is using his treatment plan- self-reported exposure to the virus- using hydroxychloroquine as post-exposure prophylaxis to prevent symptoms, which ultimately showed no benefit: as many patients became symptomatic and were hospitalized in the group taking the medication as in the group taking placebo. But as Dr. Myron S. Cohen, M.D. points out in an editorial about this study, medical research is not entirely free from popular opinion, and there are a great many ongoing trials still being conducted with hydroxychloroquine right now, many of which are focused on treatment very early in the disease course. (Edit: One was published in Annals of Internal Medicine the same day I published this article. It found that “Hydroxychloroquine did not substantially reduce symptom severity in outpatients with early, mild COVID-19“).If there is a use for it against COVID-19 at any point in the course of illness, we will hopefully know about it soon. But the doctor who wrote this post had no reliable data to suggest that his treatment would be effective; after looking at his own numbers, it’s pretty clear we still have no reliable data.
We talked about this last week when another Texas doctor claimed that inhaled Budesonide was a “silver bullet” against COVID-19 based on only a dozen patients. Right now we think the fatality rate of the virus is somewhere between 0.5% and 1.3%; still 5 to 13 times higher than a very deadly virus called Influenza, but not anywhere near the civilization ending numbers we had to work with before more widespread testing was available (I talk about these numbers more in this post). This means that if you took a random sample of 50 patients with confirmed COVID-19 and actually did absolutely nothing for them (which is not the same as offering anticipatory guidance, providing symptomatic support, carefully discussing emergency room precautions and red flag signs and symptoms, and talking through and arranging follow-up care) and 50 of them were alive a few weeks later, you would be thankful but you certainly wouldn’t be shocked. If you had 100 patients with the virus and they all lived and none ended up intubated in the ICU, you might call that God’s grace or good luck (or both, depending on your theological leanings), and you’d probably look at the demographics and risk factors of the patients, but you wouldn’t assume that the doctor had done anything extraordinary. Looking at this doctor’s sample of 50 or so patients, the one thing we can definitively say is that these statistics are not amazing. Any number of doctors around the country treating COVID-19 appropriately without unproven medications dosed with a heavy mix of conspiracy theories could give you a similar case series and claim that their particular brand of talking with patients had a “100% success rate.”
It is a little interesting, though hardly amazing, that none of his patients required hospital level care at all, and is enough to want to know more about his subset of patients. But it is exactly here that this doctor first tips his hand a little bit, by giving the details of just one of his patients. He states that he treated a patient who had been discharged from the hospital after 4 days of treatment but still ‘felt terrible’ (as people tend to do when they are ill, and also when they’ve just spent 4 days in the hospital. Heck, I feel awful after 4 days in the hospital as a doctor, much less as a patient). He treated this patient with his unproven drug regimen as well, and includes them as an example of just how effective it is. But please bear in mind that this patient had not been refused admission or callously sent home to die; they had already been treated in the hospital during the worst period of their illness, and deemed healthy enough to continue to recover at home by their hospital doctors. To include this patient not just in your data set but as an example of how effective your therapy is at preventing the illness from worsening is proof in itself that your understanding of how this virus operates is not based on reality and the experiences and insights of your peers who have more experience with it, but on narratives that you have built for yourself because you happen to find them useful. We already suspected this doctor was treating patients before they were exposed to the virus; now we know he is treating them after they were already far along in their recovery as well.
The doctor doesn’t stop there, but he goes on to give a list of other measures he doesn’t agree with, and we need to spend some time here, because this is where we really come to understand his treatment philosophy.
He states that he doesn’t believe in contact tracing, calling it ‘communism’ and stating that he ‘cannot even get the Public Health Dept. on the phone’. This is a bit like saying ‘you can’t fire me, I quite!’ and then asking about your severance package; if he really believes contact tracing is communism, one would wonder why he was calling the Public Health Dept. about contact tracing in the first place. I also don’t understand how contact tracing could possibly be communism, but clearly this is a secondary issue at best.
He also doesn’t believe in quarantine, which while undoubtedly difficult on a broad-scale (other countries have found ways to help their effected citizens deal with quarantine and isolation with adequate social and emotional support measures) is also common sense epidemiology, and in wearing masks, which have plenty of solid evidence (which has only increased since I wrote that blog post). He doesn’t believe in social distancing (I don’t understand what he’s talking about in the parenthesis, but I think it’s about the economy), and he even says he doesn’t believe in testing, citing an insanely inaccurate false negative rate that is only possible, even for the veryworst tests, once COVID-19 is at 55%-65% prevalence in the population you are testing; a number we have not seen anywhere in the world at any point during this pandemic. For reference, the highest his county has reached at any point has been a test positivity rate of 16.89%, just 2 days ago. This would give the two tests I use a false negative rateof 4% and 1.3% respectively.
This is really a whole separate set of claims. He is claiming that the methods used by every single country that has seen success in protecting their citizens from the virus don’t work, while an unproven and incredibly politicized medication regimen used by him and one other doctor in a nearby city is the miracle cure. One might advise a more humble approach, claiming that while these strategies might work (as the evidence clearly demonstrates they do), they would be rendered unnecessary by his treatment strategy; but he boldly claims both, even to the point of saying that other doctors not using his treatment regimen has lead to 100,000 deaths. If he is wrong about the latter and is widely believed, the virus will spread more quickly; if he is wrong about the former, those who are exposed as a result will be without the miracle cure they were promised.
What if he were lying?
Here’s the cynical part, and the part I find hardest; what if this misinformation, rather than the honest misunderstanding of a doctor with very limited experience with the virus, were a deliberate and calculated deception in order to make money, as so many other doctors have been accused of? Would this, unlike advising social distancing at the expensive of your own clinic’s bottom line or cancelling lucrative elective surgical cases, be an effective financial strategy?
Let’s review. In this post, this doctor:
Advises against wearing masks, social distancing, and quarantine. If he’s lying, this would increase the number of COVID-19 cases during a time of otherwise decreased medical visits, thus creating more sickness and more patient visits in general.
States he doesn’t believe in testing. This eliminates a natural barrier to receiving ‘targeted’ treatment, because it places the diagnostic decision making entirely in the subjective realm, all based on phony statistics about the COVID-19 tests. This means that a number of his patients will receive treatment without even having the virus in the first place, which will inflate his “amazing” treatment statistics. This is great, because he also states that he…
Claims he is treating 3-6 weeks earlier than other doctors. This means he is relying on some unique way of diagnosing the illness that is entirely original to him, that would lead to a diagnosis weeks before a patient would end up in the hospital; in other words, it won’t even matter if you have recognized symptoms of or exposures to COVID-19, he is able to diagnose you well ahead of any normal doctor. Combined with a promise that he won’t rely on test results for the virus, this is tantamount to a promise of specific medications for treatment ahead of time, which is an advertising tactic, not conscientious evidence-based medical practice. It would be like promising antibiotics for your child’s ear infection whether they need it or not, and then claiming that your child would have had an ear infection and that most doctors don’t treat as early as he does because they just don’t know the very early signs, like being fussy, tugging at their ears, and wanting to watch Moana over and over again (hey wait! My toddler does have all of those symptoms!).
Promises “completely safe and incredibly effective” treatment without any credible scientific evidence of its effectiveness. This reinforces his criticism of masks, social distancing, and quarantine for his patients specifically (who wouldn’t need them anyway, since they are now ‘healed’), which increases subsequent cases in their families and friends; the very people his patients are likely to refer to him by word of mouth.
Shares his post on social media. This spreads the word, especially once it goes viral, and not only increases cases as people believe it and use it to justify forgoing mitigation and transmission control measures, but also drives people to his clinic from all over the state and region because he…
Shares his name and says to contact him. Having now promised treatment for a virus that his post is likely to cause more cases of, he now ensures that he will have a higher percentage of the market share of both these new COVID-19 cases and people who don’t have COVID-19 but are seeking pharmaceutical treatment out of fear due to the increasing surge; a surge his post is at the very least contributing to.
In summation, this post is saying don’t do any of the these inconvenient things doctors around the world say will help keep you and your family safe from the virus; just come see me in my clinic and I will diagnose you with COVID-19 whether you have classic symptoms or not, whether you test positive for it or not, and without fail prescribe you these medications that you can’t get from most other doctors.
You don’t need five years of medical school to understand why this should make you cautious.
I have to admit, that felt really dirty. I’ll say it one last time; I actually think this doctor, like so many of those I’ve argued with from a distance on this blog, really believes his post. He has gotten his stats wrong, relied on old and incomplete data on masks, misunderstood what other countries have done to fight the virus, confused contact tracing with communism (ok that one is new), leaned on anecdotal evidence, and I believe in general approached the subject with enough bias and preconceived ideas and little enough actual exposure to the virus that he never had a chance of reaching a different conclusion. In fact, his very limited clinical experiences with ‘treating’ the virus are almost perfectly calculated to provide him the confirmation bias he needs to firmly cement the truth of all of his claims in his mind, and that will only get worse as more patients come to him “early” in their disease course and experience a full recovery, whether they ever had the virus in the first place or not.
I do think this doctor can be wrong, and yes, do damage, without it being nefarious. But it’s clear from social media that there are some people, perhaps many people, who are not comfortable with the majority of physicians drawing one conclusion while a small minority draw the opposite conclusion unless one of those groups is lying. If that’s you, please consider which doctors have the greater financial motivation to build a false narrative- and stand to actually gain from the narrative they are building- and which are willing to tell the truth to keep you safe even if it potentially hurts them financially. That’s already one of the most obvious ethical principals we nevertheless have reinforced for us repeatedly throughout medical school and residency and a decision that a great many of us got used to making years ago anyway, and the idea of a doctor telling his patients “please stay home and stay safe” as he wonders how he’s going to pay the rent on his clinic building is far easier for me to imagine than any of the critical care doctors I’ve met in the last 13 years intubating a patient that they thought didn’t really need to be on a ventilator, much less because it was going to make them some extra money.
Last week I saw about 80 patients who had screened positive for either exposure to COVID-19 or possible respiratory viral symptoms; this week more of my time is devoted to working in outdoor COVID-19 testing clinics, so it will probably be well over 100. Some of those patients had been ‘caught’ by our screening questions but really had no COVID-19 exposure or symptoms; the lady with a chronic cough who was really just coming for her high blood pressure, the gentleman with a fever that was caused by an abscess under his axilla (we call it ‘axilla’ because ‘armpit’ sounds so un-doctory). I treated them too, of course. But for the most part people were seen in our COVID-19 focused clinic specifically for COVID-19 related concerns. I don’t have exact numbers in front of me, but of the 70 or so I tested for the virus, about 20 came back positive (Epidemiology note: this is too small of a sample to calculate anything like a test positivity rate or prevalence from), and there were at least a couple that, due to certain combinations of exposures and symptoms, I’m convinced had the virus despite a negative test (way, way too small of a sample to make any calculations from; please don’t go and quote me as saying that based on my sample of 2 out of 50 negative tests I think there is a false negative rate of 4% or something crazy like that)(although now that I look at prevalence estimates and test sensitivity, 4% is actually about right. Hmm…).
I called each patient who tested positive personally to give them the news and answer their questions. Amid the many questions I was asked (‘Should I go to the hospital’?; not now, but let’s talk again about red flag symptoms and emergency precautions. ‘Should I isolate from my children?’; that’s really complicated, and it depends on the age of your children, your support structure, and their specific developmental, physical, and emotional needs), one question that came up over and over again is one I sincerely wish I had a better answer to; ‘what medicine can I take to make sure this gets better?’
This is a big and important question. Doctors kind of like medicine; kind of a lot. After all, prescribing them is a big part of our job, and even though adding a medication is not always the right answer (more on this later), it is incredibly satisfying to prescribe the right medication or therapy for the right diagnosis and then see your patient get better. It can also be fairly stressful at times, because no medication (except prenatal vitamins) is perfectly safe; giving someone a medicine, especially one that wasn’t actually necessary, and then seeing them suffer because of drug interactions or unexpected side effects is devastating to a physician. We have taken an oath to ‘first do no harm,’ and we take it seriously. This is why I’ll spend 10 minutes carefully explaining to a parent about how viruses and bacteria infect the body differently and how antibiotics work rather than spend 2 minutes prescribing their child an unnecessary antibiotic for a viral illness, which would surely feel more satisfying for both of us. It is also why, as certain as I am that some of the patients I have shared the news of a positive COVID-19 test result with will end up getting sicker, and as nervous as that makes me on their behalf, I have not been prescribing unproven, untested medications out of desperation, but have instead focused on teaching those patients how to keep themselves and others safe and how to recognize the early signs of a severe infection.
It’s also why I check for new or updated studies or professional recommendations, and review information being shared between doctors and other clinicians on COVID-19 social media groups every every single. The moment that there is a proven, safe early therapy to prevent COVID-19 infections from becoming severe, I will be the first to start using it.
Dr. Richard Bartlett discovers silver bullet for COVID-19.
Last night I came across a viral video, which has since been sent to me multiple times, which seemed to promise exactly this. A doctor here in Texas went on a morning news show to discuss the 100% effective, perfectly safe COVID-19 treatment he is using to prevent severe illness in his patients. If you have any degree of medical training or even personal experience with medical issues, you are probably just as skeptical as I am about both the ‘perfectly safe’ and the ‘100% effective’ claims; few medicines are ever either. We will go through Dr. Bartlett’s interview in detail below and try to evaluate the quality of data he is relying to make these claims, and answer two questions; should you call and ask your doctor for this ‘new’ treatment, and should I call back all of my patients and tell them, much to my satisfaction, that we do have a medication I can put them on after all?
One quick note: the video is about 30 minutes long and trails off a lot into conspiracy territory concerning mandating vaccines, instituting lockdowns to destroy the economy in order to hurt President Trump’s reelection chances, and quite a few other areas. We’ve covered a lot of that before, and frankly a lot of it falls outside the realm of medical misinformation. We will try to cover the most important parts of Dr. Bartlett’s interview regarding his new COVID-19 therapy, but I won’t try to write the 10,000 words it would take for a rebuttal to all of these ideas.
Here is the video:
00:16: Midland Texas is located in Midland County, about 6 hours West of Waco (golly, Texas really is huge). With a population of 138,000, it is almost exactly the size of Waco. Just like for us and the rest of Texas, they began to see a significant increase in COVID-19 infections about 3 weeks ago. Before this, they had seen very few cases total, like most pre-surge areas. You can review their data here.
00:33: The article is here; it provides some additional details and we will reference it later.
At 02:04 Dr. Bartlett begins his discussion on COVID-19 treatment in earnest by discussing the context for the pandemic in America, namely a comparison to both nations that have fought the pandemic successfully and those who have struggled more with a higher number of infections and deaths. He begins with Taiwan.
02:07 “In the country of Taiwan there’s over 25 million people, they’re stacked on top of each other, if they did social distancing they’d be out in the ocean floating around.”
He goes on to say that there isn’t enough room to social distance, and yet the country has seen only 7 COVID-19 deaths, “as many people as you could stack in a minivan.”
The problem here, besides Dr. Bartlett’s strange obsession with stacking people, is that Taiwan has done social distancing. Dr. Bartlett goes on in the video to assert that Taiwan has foregone both social distancing measures and widespread face mask use (which he associates with Communist China). Do any reading on Taiwan’s response to COVID-19 and you will find widespread wearing of face masks and aggressive physical/social distancing measures since the earliest days of the pandemic, in addition to other mitigation strategies such as providing social support for quarantined patients to help them maintain a high level of isolation, and using mobile phone technology to perform extremely precise contact tracing. This is all in the context of a strongly collectivist culture willing to engage in such measures for the good of their neighbors regardless of official mandates, with a history of understanding the stakes in such a pandemic because of their experience with SARS in 2003.
So as Dr. Bartlett moves forward talking about Taiwan later in this video, you need to understand that, perhaps entirely unintentionally, almost everything he has said about their success in fighting COVID-19 so far is the opposite of what they have actually done.
02:41 At this point Dr. Bartlett also mentions Iceland, Singapore, and Japan, who all engaged in some combination of extensive masking and social distancing except Iceland, who used aggressive contact tracing and quarantine measures. Dr. Bartlett’s assertion that they have been successful because they have used similar treatment plans to what he uses for his patients seems entirely unfounded.
02:59 “That’s not possible according to what we’re being told in the mainstream media.”
Literally nobody is hiding this data. If you google “Taiwan COVID” you get this:
“You can even look it up in the Johns Hopkins COVID website and you’ll see those numbers. They’re hidden in there, but I’m pointing them out.”
“Hidden” in the sense that geography is hard.
I’m concerned that what Dr. Bartlett is doing here is contributing to a false narrative that the powers that be, especially the CDC, the WHO, and the medical establishment (i.e. he and I), doesn’t want people to have access to good reliable data. Maybe this is where Dr. Bartlett’s search for reliable information to back up his COVID-19 treatment has led him; not trusting the available information because he wasn’t able to find the scientific verification he is sure must be out there for his new therapy. Maybe this is strongly ingrained in his political position (he recently ran for office) and he is interpreting the ready availability of this kind of data through a lens of suspicion, or knows that his audience on this show will affirm the idea that this information is being hidden from them and that it is harmless to reinforce that belief. But I am always a little suspicious of physicians who want to weave these tells of conspiracy theories and hidden truths about the pandemic while promoting their own unverified findings, and part of me wonders if they are certain they will face pushback from their fellow doctors and scientists, and want to head it off at the pass by encouraging the idea that those doctors and scientists don’t want you to know ‘the truth.’ I certainly hope this isn’t the case with Dr. Bartlett, but part of me thinks it must be an easy trap to fall into without realizing it.
It isn’t Hydroxychloroquine
03:32 “(In these other countries) they’re doing what I’m doing, which is not hydroxychloroquine, although that works….
Before he reveals his miracle drug, he gives a brief shout-out to Hydroxychloroquine, stating it does work but not providing further explanation as to how he knows it does or why he doesn’t use it as well. I almost wrote today about a viral post by a doctor in McKinney Texas again promoting outpatient, widespread hydroxychloroquine use in patients regardless of test results and risk factors. We covered this pretty extensively over a month ago following his colleague Dr. Lozano’s speech at the Set Texas Free Rally in Dallas. He also claims that masking, social distancing, and even testing are ineffective. I’ve chosen to write about Dr. Bartlett’s video instead, but in terms of relying on anecdotal evidence and not understanding representative sample sizes, there are a lot of similarities. If things are quiet this week I will try to write about Dr. Procter’s social media post as well and try to tackle hydrochloroquine one last time.
I want to talk hydroxychloroquine. I want to talk about these scripts that you’re writing; Put down the pen, stop prescribing. I want to talk about what I have learned, About the research you have spurned…
The Silver Bullet: Inhaled Budesonide
03:36 “So what they’re doing is an inhaled steroid. So my silver bullet is inhaled budesonide.”
Dr. Bartlett finally reveals his miracle drug, inhaled budesonide; a commonly used inhaled corticosteroid that is commonly used for patients with Asthma or COPD.
This is the first good place to stop and look at this idea in more detail. The first two questions we need to ask when someone proposes a novel use of a medication or therapy are 1. Is there a proposed mechanism by which this would work? 2. Why did nobody else think of this (has this been tried/studied before)?
Dr. Bartlett’s rationale is that since this is an inhaled respiratory anti-inflammatory, it should work for COVID-19 which is a ‘respiratory inflammatory condition.’ Part of the problem here is that this is gross oversimplification of the virus’s pathophysiology, which is still not completely understood (see below). It is supposed to make you go “wow, that’s just common sense! It causes inflammation in the lungs, so an anti-inflammatory breathed into the lungs will cure it!” But if you reflect on whatever extent of experience you have with medicine, you will realize that things are never quite that simple. If you came to me for your severe, debilitating back pain you’ve been struggling with for years and I said, “oh I’ve got it, back pain is caused by inflammation of the muscles and joints, so I’ll give you a medicine to decrease inflammation; here’s some ibuprofen,” you’d probably lose a great deal of respect for me. You’d be right to. NSAID’s (non-steroidal anti-inflammatory drugs, like ibuprofen) may well be part of your treatment plan, but your back pain is complicated and is going to require more thorough evaluation and treatment. In medicine, you are right to beware of easy answers.
Sentences like these are why I went into clinicalmedicine.
Budesonide is a common medication, as he points out repeatedly beginning in a few minutes, and I think this is actually the strongest argument against his proposed use of it in COVID-19. You read that right; I’ll explain. The usual dosing of budesonide is twice a day as a maintenance medication; by decreasing inflammation and swelling in the airways, it can eventually (it may take weeks to months) lead to less frequent asthma and COPD symptoms like cough and chest tightness, and fewer exacerbations. However, Asthma and COPD patients still have acute exacerbations despite using inhaled corticosteroids. We still see patients on budesonide in the clinic and in the hospital for acute worsening of their symptoms due to respiratory infections. Sometimes these are bacterial infections, but more often they are viral; including coronavirus species. Sometimes these patients go into respiratory distress, and sometimes die, even when the virus they have isn’t nearly as deadly as COVID-19. If budesonide was able to completely prevent viral respiratory illnesses from causing inflammatory respiratory symptoms like cough, shortness of breath, wheezing, and chest tightness, we would never see these patients getting sick from respiratory viruses; but we do, because the medication doesn’t really work that way. If Dr. Bartlett consulted his complex understanding and professional history of treating respiratory infections he would realize that his proposed mechanism really doesn’t make sense, especially as the 100% effective silver bullet he is promoting it to be.
Later in the video (around the 06:36 mark) Dr. Bartlett does talk about the “cytokine storm” in COVID-19 and prevention of the body’s own inflammatory response to the virus. Is it possible that the medication he is using, while not preventing all respiratory viral infections, at least treats this one? Without getting into the weeds too much here (the idea of a cytokine storm being the underlying cause of ARDS in COVID-19 is still controversial), we need to understand that you don’t just have this one thing called ‘your immune system’ causing this process called ‘inflammation’, so that if ‘inflammation’ (or in this case, ‘cytokine storm’) is the problem we can just suppress the immune system and call it a day. The immune system is incredibly complex, and any given immunomodulating medication is going to work on parts of the immune system (and not always in the ways we hope or expect) while not significantly affecting others. As an example, the primary cytokine implicated in the COVID-19 cytokine storm seems to be interleukin 6, a pro-inflammatory cytokine that budesonide, in previous studies unrelated to COVID-19, doesn’t seem to affect appreciably. Studies focused on medications that do appreciably decrease IL-6 activity are currently underway.
I’m having bad flashbacks to 2nd year of med school right now.
The second question, if the mechanism did make perfect sense, would be to ask whether anyone has tried this before. Dr. Bartlett indicates that it has been tried elsewhere; he states that this is what they are doing already in Taiwan and Singapore. I was unable to substantiate this; I cannot find any evidence that these nations have used anything like widespread protocols with inhaled steroids to treat COVID-19 early in the disease course. There are some ongoing trials with use of inhaled corticosteroids (not budesonide, at least that I could find), as Dr. Bartlett mentions, but there is not any data available from them yet; if they prove safe and beneficial for COVID-19 patients, we would start using them in all the clinical contexts where they were shown to be effective.
There are two other data sources we could look at. First, the most successful trial we have right now with use of steroids in COVID-19 is the RECOVERY Trial out of Oxford, which I wrote about recently. In this study patients were put on systemic steroids (dexamethasone) once they were already hospitalized. You might argue that this isn’t what Dr. Bartlett is talking about at all, that he wants to use budesonide before they are sick enough to go to the hospital. I understand that; but the study showed a reduction in mortality in both the groups needing oxygen and those requiring mechanical ventilation, but not in those who didn’t require oxygen. You can only extrapolate so much from this, but if Dr. Bartlett’s theory of the earlier the steroids the better panned out, you would expect the non-oxygen group to see at least as much improvement in outcomes as the patients who were already very, very sick; but that wasn’t the case. We need to remember that even though our first successful randomized drug trial for COVID-19 is indeed a steroid, the role it plays is complex and the benefits limited to certain clinical scenarios; the data still shows that immunocompromised patients, including those on medications that modulate the immune system, are at a higher risk for COVID-19 than those who aren’t.
We can also look at the two closest viruses to COVID-19 that we have experienced, SARS in 2003 and MERS in 2012. These are both Coronaviruses that seemed to involve a ‘cytokine storm’ causing acute respiratory distress syndrome. During these outbreaks inhaled corticosteroids were used more widely, but results were mixed; there was no strong evidence of benefit, and some evidence of worsening of the disease, including increased risks of secondary bacterial pneumonia and prolonging the time it took for the body to clear the virus.
Edit: When discussing this issue, a colleague also pointed that this idea of ‘what about decreasing inflammation in the lungs’ is not novel, and studies have tested inhaled corticosteroids on practically every lung infection (infection is a very pro-inflammatory state) over the past 30 years, not just SARS and MERS. Results have been extremely unimpressive, but there has been consistent evidence of increased risk of certain types of lung infections, including tuberculosis, non-tuberculosis mycobacterium infections, and severe drug-resistant bacterial pneumonia.
So I’ll conclude this section where many people with much more expertise in this area than myself have, by saying that the balance of risks and benefits still doesn’t justify use of an inhaled steroid in people without asthma or COPD who are already taking one or would benefit from one anyway. There is no reason to believe that they will appreciably decrease the chances of developing the severe acute respiratory distress syndrome that makes the virus so dangerous for some people, and for the vast majority of people who will do fine with their own innate immune system fighting the virus, steroids would potentially increase both the risk of worsening infection and delayed clearance of the virus, and the risk for associated bacterial infections (in addition to a host of other potential side effects). If we were to begin using this in patients who don’t have COVID-19 as prophylaxis, we could conceivably increase their likelihood of getting the virus. The mechanism of causing these types of harm is at least as strong as the proposed mechanism of preventing worsening of the disease.
03:46 “It’s super cheap, it costs about $200 for the total treatment if you pay cash.”
I understand that he is probably intending this as a comparison to a hospitalization for COVID-19, which is disastrously expensive, as he truly believes the budesonide will prevent hospitalization. Still, all I can say is that Dr. Bartlett and I have different ideas about what constitutes super cheap medication; most of my patients could not afford a $200 medicine.
“But what does all of that matter? He said it is working for his patients.”
There are some more problematic statements in this video, including the idea that our numbers in Texas are only going up because of increased testing (17:05), revisionist statements that totally invert the sequence of events and thus cause and effect of social distancing and masking measures in the most affected countries (21:50), a troubling statement about Japanese people ‘crawling all over each other in Sushi bars’ (22:55), and strangest of all, repeated statements about how waiting to treat someone until they have symptoms is un-American, whereas early treatment is the American way (both preventative and acute care are part of every healthcare system in the world; there is nothing particularly American about throwing medications at people before you know whether or not they need them).
I hope to update this post with some rapid-fire answers to these issues later, but I want to focus here, for now, because I sincerely believe this is the part of Dr. Bartlett’s interview that people find most convincing.
“One hundred percent of my patients are alive. I’ve been treating this since March.”
I’ve written before about the dangers of anecdotal evidence. I think as physicians we are prone to fall into this trap for a couple of reasons. One is because we want so badly to help our patients, and if we hit on a medication that really feels like it is working, it’s hard to let go of that feeling. Another is because we spend so much time thinking about our patients and working for their well-being that their stories loom very large in our minds, and it’s easy for the relative importance, as data, of our personal small numbers of cases to become overinflated. With that in mind, I think it’s worth looking at Dr. Bartlett’s evidence from the outside and asking whether it really has the value he credits to it.
According to the local news article featuring Dr. Bartlett back on May 21st where he first publicly called budesonide his ‘silver bullet’ against COVID-19, at that time he had treated 12 people. Twelve. This is an incredibly small sample size, but we could hardly expect larger; Dr. Bartlett is not the only doctor in Midland, and throughout March, April, and May the entire county only had 1 or 2 new cases of COVID-19 most days; there just weren’t that many COVID-19 patients to go around. Dr. Lozano had previously gotten around this issue by saying that she wasn’t even testing, but was treating empirically based on symptoms or possible exposure, which doesn’t really make sense in a pre-surge area with incredibly low prevalence. Dr. Bartlett has stated that he believes in testing, and although his comments are mixed on whether he is treating only confirmed COVID-19 cases with budesonide, I think we could credit him with such qualms. Twelve cases over 3 months is an extremely small sample size, and it is important that we understand that this is not coming from someone who has been inundated with COVID-19 cases like our peers in New York; at the time that Dr. Bartlett decided that budesonide was a miracle drug he had practically no experience with the virus. It is certain that his numbers have come up by now, with cases rising all across Texas; but with lag time between exposure and the onset of symptoms, and a second lag between the beginning of symptoms and severe respiratory complications, it is not possible to say that all of Dr. Bartlett’s recent COVID-19 patients are out of the woods yet.
So Dr. Bartlett’s first error is over valuing the data from his sample size, but his second error is in thinking this disease is more dangerous than it actually is. I know that seems like a strange thing to type; the disease is plenty dangerous, and I have encouraged the utmost caution on this blog more times than I can count. We have looked over and over at the hundreds of thousands to millions of lives that might be lost if we do not discover effective drug therapies and if the virus continues to spread unabated because of poor adherence to mitigation strategies like face masks and physical distancing. But the virus has never been estimated as having a 20% fatality rate as Dr. Bartlett says in the video. Dr. Bartlett has no doubt been worried about COVID-19 since March, just like me. Just like me, he probably has friends and classmates working in ER’s and hospitals in New York and New Orleans and other areas that have already been hit hard, and has heard the horror stories about what this can do to both individual patients and entire healthcare systems. Like me, as soon as he started thinking about this respiratory virus he probably immediately thought of the names and faces of two dozen patients that he was particularly worried about. Due to this anxiety, surviving the virus has become, in his mind, the exception rather than the rule. We see this in his account of the woman battling cancer; he says “she should die according to what you hear from the CDC and the WHO,” even though we know that COVID-19 is not universally fatal for any group. By increasing the danger of the virus in his mind, or at least increasing the probability that any given patient will go to the hospital or die, it makes it seemingly unlikely for people to get better without some specific intervention, even though we know that is what happens most of the time; thus the interventions he has chosen (budesonide, zinc, antibiotics) receive the credit for his patients’ recovery.
Put these two biases or statistical errors together and it may be easy for a physician to believe, based on the slightest of clinical experience with this virus, that he has discovered a cure. Each patient you treat this way will confirm it for you, as long as they get better, even if they would have gotten better anyway, and particularly if they tell you they feel better right away, which is such a wonderful feeling even if it doesn’t always correlate to their eventual outcome. If you are willing to loosen your treatment criteria to include people who have had no test or negative tests, or who are fully asymptomatic as Dr. Lozano seems to have done with hydroxychloroquine, you can inflate your treatment numbers even higher. And if you top-out at something manageable for a small-town physician, say in the low 100’s, you might never see a fatality from COVID-19. Imagine that we were back in May when Dr. Bartlett had only treated 12 COVID-19 patients. He states boldly that 100% of his patients were alive, yet we think the death rate is around 1.3%. If just one of his 12 patients had died we might still find this convincing because we are so easily swayed by anecdotal evidence, but that would have been a fatality rate of 8.3% in his budesonide patients. We would have fallen into the same trap as Dr. Bartlett, of picturing those 12 patients heading toward certain demise and all but one rescued by his treatment plan, without which they would have died, when in reality there is no evidence to suggest that they would have been any worse off without the treatment. Dr. Bartlett’s experiences with the virus so far are exactly what we would expect without budesonide and antibiotics.
“Look, he says it is helping his patients and you don’t have to use it for yours, so why does it matter to you?”
Great question, hypothetical person who keeps arguing with me on the internet. Any time we begin talking about someone’s personal experiences, the temptation is to treat their narrative as incontestable; I wasn’t there, I didn’t see his patients, so I don’t have the ability to second-guess his clinical judgement. In a way this is actually sort of fair; Dr. Bartlett had just as many years of medical school and residency as I did, and has many years more clinical experience, and to some degree each physician has earned a degree of professional trust to practice in a way we see fit with accountability only to ourselves and our patients, at least in many circumstances. But we know that this professional leeway has been abused in the past, and even in the absence of abuse of that privilege, lone-wolf medicine is a real problem because by it’s very nature it is disconnected from one of the best tools we have to improve our clinical abilities and correct our errors; the honest feedback and accountability of our fellow doctors. If a physician feels that a patient’s clinical situation calls for a unique approach that is not supported by evidence, this can often still be tried as long it is accompanied by an honest and careful explanation to the patient of the reasoning behind this approach, the unproven nature of the treatment, and the risks involved. If we begin to make a habit of such practices, and particularly if we do so ignoring the voices of our peers around the world saying we’ve tried this before and it didn’t show reliable results on a larger scale, or the voice of researchers and scientists saying that doesn’t actually work the way you think it does, then we are doing so at our own, and more importantly at our patients’, peril.
In many ways I think Dr. Bartlett is actually going about this fairly well. He seems to imply that he is using the medication, which does have a theoretical mechanism of action after all, only on those who really do have COVID-19. He does not seem to be doing television interviews or talking with newspapers in order to make a name for himself and attract clientele from all over the state to help his business, as seems to be the case with some other doctors prescribing unproven treatments, but in order to ‘get the word out there’ to other doctors (as one of those other doctors, I deeply appreciate this impulse), although I am not sure why he has not utilized any of the many avenues on social media that many of use are using to get physician specific feedback and share ideas; maybe he is and we just aren’t part of the same COVID-19 doctor groups. Most importantly, he states that he has written and is submitting a paper for publication, which will provide both more details about his patients, their demographics, commodities, and clinical presentations, and allow for peer review and a higher degree of detail and scrutiny than we could possibly get through a TV interview.
But there are at least three ways (besides the tacit endorsement of several conspiracy theories) that I find Dr. Bartlett’s approach truly troubling. First, he is not presenting his treatment plan as an entirely unsubstantiated experimental approach driven by hope and a hunch, which is what it absolutely is, but as a “Silver Bullet” that is perfectly safe and cannot fail, which is certainly is not. One would hope that this is bravado or enthusiasm for the TV audience and not hubris; in other words, we have to hope that whatever confidence in his treatment regimen he shows in this interview, he is still very carefully explaining to his patients the limitations of his evidence and the potential risks they are taking on if they use it, and the red flags to look for in case it doesn’t work.
Second, he is not just promoting his unproven treatment but also discouraging mitigation measures, such as physical (social) distancing and wearing masks, that actually have been proven to save lives. It is unclear whether he believes the misinformation around these strategies not working or is just so confident in his treatment approach that he no longer thinks they are necessary, but the effect will be the same; as Dr. Bartlett’s video goes viral there will be increased pushback against wearing masks and observing distancing measures by those who find him convincing, which will ultimately lead to more cases, more hospitalizations, and more deaths. His evidence is too weak and his scientific rationale too shaky to convince a conscientious doctor to start using his treatment approach; but he speaks with enough confidence and sincerity to convince some people on the fence not to wear masks. The net effect of his interview, like any viral misinformation, is to make the pandemic more dangerous for everyone.
And third, by presenting his treatment plan as something that it isn’t and ascribing to it all of the confidence and reliability of a truly proven treatment, he is spreading misinformation that blocks out the transmission of reliable information for the public and pollutes the relationship between his listeners and their own doctors and healthcare systems. When I explain to patients that I do not have a proven medication I can in good conscience prescribe them to prevent their COVID-19 from progressing, their exposure to voices like Dr. Bartlett’s, Dr. Lozano’s, and Dr. Procter’s have already sewn the seeds of mistrust in the information I am providing, and they are less likely to believe the other recommendations I am carefully trying to give, such as isolating within their home and monitoring for red flag symptoms, and the reassurance I am trying to provide to alleviate their fear and anxiety as we discuss their individual chances of having a severe course of the virus. It may lead anxious patients to seek additional visits elsewhere and shop for a doctor that will prescribe them what Dr. Bartlett says they need, further increasing their chances of exposing others and potentially increasing the costs associated with their medical care, both to them personally and to an already strained system. It may even lead some patients, convinced by these doctors and desperate for medicines they now believe are their only hope of beating the virus, to misrepresent their symptoms in ways they think might push their doctor into prescribing them.
When lone wolf doctors promote unproven therapies and set themselves up as experts with miracle cures, without having actually done the clinical research to validate their claims, it erodes the fragile trust that we work so hard to build with our patients when we are unwilling to engage in that same type of speculative treatment. This unearned mistrust has the potential to breakdown the patient-physician relationship and affect our patients’ health for years to come. Millions of doctors, nurses, and other medical professionals around the world are working as hard as we can to both care for our patients in the midst of this pandemic and stay up to date with the latest diagnostic and treatment options. Viral voices drowning out the excellent work that is being done researching potential treatments, and calling out any doctor not willing to follow their lead, should humbly re-evaluate their limited clinical experiences in the face of this global pandemic and bring forward their innovations, not with less hope or enthusiasm, but with much more care and a realistic appraisal of the strength, or lack thereof, of their evidence.
I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now in 8-bit Color!
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Question #3: Isn’t a surge a good thing since it will give us herd immunity?
The concept of herd immunity, susceptible persons being protected from infectious diseases by a sufficiently highnumber of people in their community already being immune, was controversial even before the COVID-19 pandemic. I don’t mean it was a controversial area of epidemiology; the science behind it is very well established and pretty straightforward (and if you are going to read about the eradication of smallpox from that link, you should also read about a man called Onesimus, a slave in Boston whose knowledge of West African inoculation saved hundreds or thousands of lives and paved the way for Edward Jenner’s eventual invention of vaccination techniques). I mean it was something that we’ve had to argue about constantly in recent years because the anti-vaccine movement uses herd immunity as one of its many arguments against vaccination, while at the same time undercutting its effectiveness by seeking to decrease the number of people who are immune through being vaccinated. The idea is great in principal; just weather the storm now and then we will all be safe from the virus forever. The problem (one of the problems, for there are numerous) is that we don’t yet know exactly what percentage of the population needs to be immune to confer protection to everyone else. Most estimates have put this number somewhere between 60-70%, but a recent model published in Science estimates it at a much more attainable 43%. These numbers are based on several parameters that tell us both how easy the virus is to spread and whether certain activities, situations, or even individuals are more likely to spread it than others (you can read about the median reproduction value and dispersion factor if you want to dive a bit more into the math of it all). Because these numbers are incredibly hard to definitively determine in the midst of a pandemic, any percentage we arrive at is going to be a best guess; an estimate derived from multiple assumptions that will only be proved wrong if many more people get very sick even after we’ve achieved the required numbers for herd immunity. Herd immunity is a gamble because Virology, during a pandemic, is an applied science; the virus will correct all of our miscalculations and false assumptions for us. (other questions, such as whether immunity to SARS-CoV-2 is indeed long-lasting and whether the virus will mutate in such a way that it causes future outbreaks despite our acquired immunity are also important, but outside the immediate scope of the discussion).
*This is from early in the pandemic, but a great visualization tool
But even more important than the difficulty in calculating the necessary percentage of people being immune to confer protection to everyone else is the question of how dangerous it is to get there in the first place. Let’s talk about measles for one moment. We know that the herd immunity required for measles is somewhere around 93%, which is part of the reason we have seen outbreaks of the disease recently in areas that have a substantial anti-vaccine sub-culture; it isn’t hard to fall below that number. Let’s say there wasn’t a Measles vaccine; that means 93% of people would need to develop immunity by living through the disease. With modern medical advances the case fatality rate for measles is a lot lower than it used to be, but it is still around 2.2%. This means that in a country of 330 million people that had no immunity to measles, 306 million would need to contract the disease to confer herd immunity to everyone else; of those, 6.75 million would die, not to mention the longstanding residual neurological deficits and other health complications in tens of millions more. Without effective vaccination, herd immunity would simply never have been an option for Measles; the cost in human life and suffering would just be too high. But what about COVID-19? We know that SARS-CoV-2 is thankfully less contagious, and we believe less deadly (see the last post for a discussion on this) than measles, but is it enough to make herd immunity a viable option? Let’s apply those same calculations based on the current estimates we have for infection fatality rate. If we accepted a 1% death rate estimate, then to achieve the widely accepted 60% mark for herd immunity we would see 198 million cases and 2 million deaths, while if we accepted the recently released 43% estimate and assumed an even more conservative 0.5% death rate, that would be 709,500 deaths; and neither accounts for the longstanding health deficits or the cost in human suffering of those who survive, or the other deaths and suffering that come with an overwhelmed mid-surge healthcare system. Now, could we devise some clever epidemiology strategy that uses emerging data about the already-immune, super-spreaders, natural resistance, new drug therapies, contact tracing, and protection of the most vulnerable? Of course; assuming that we could get a high degree of buy-in (we can’t even get people to wear masks), that’s exactly what we are all hoping for. But that’s not ‘herd immunity’, and it’s clear that the cost in lives and suffering from a “just get it and get it over with” ‘strategy’ would be astronomical even with our most optimistic estimates. Trust me, I’m tired too; I completely understand the pull towards a roll the dice approach that just gets this over with and lets the chips fall where they may; that approach completely appeals to my intellectual and emotional fatigue. But the longer we can work together to flatten the curve, the more time we create to discover those new therapies, improve our understanding of the virus, and collect high quality data about transmission and vulnerability that can help us develop novel, strategic mitigation approaches (which would probably incorporate something like herd immunity); and we are already seeing the benefits of the work of this kind that we have done so far as a society.
Question #4: What is the RECOVERY Trial?
(Confession: nobody asked about this, but I’m going to write about it anyway)
The RECOVERY Trial is a randomized(poor British researchers spelled it wrong) clinical trial out of Oxford that has shown benefits from using low-dose dexamethasone (a cheap and readily available steroid) for hospitalized COVID-19 patients on oxygen or on a ventilator; you can read a more detailed analysis of the trial from First10EM. This is still in the peer review process but results have been incredibly promising; the study showed a relative decrease in mortality of 20% in hospitalized patients requiring oxygen, and up to a 35% decrease in patients requiring ventilator support. Unlike many of the drug therapies that have been touted up until now, this is based on a randomized trial and not on anecdotal evidence, so it is much more likely that these results will be reproducible when used broadly. Already this has become the standard of care in the hospitals in your city, and if we see these results persist with widespread use it has the potential to save tens or hundreds of thousands of lives. I wanted to write about it for two reasons. First, I want to call on us all now to not let this become the next hydroxychloroquine. The study has established the benefits of this drug therapy only in a specific group of people; hospitalized patients requiring oxygen or ventilator support. They also studied hospitalized patients who were not sick enough to need oxygen, and it showed no benefits whatsoever. There is no reason to infer that this medication is protective in those without severe symptoms or in asymptomatic individuals, and so there is no reason for individuals to ask their doctor for an outpatient prescription or for pharmacies or clinicians to stockpile the medication as we saw done with hydroxychloroquine. We can be thankful that we have at least one helpful medication for our sickest patients without that immediately translating into figuring out a way to get it for ourselves whether it would actually help us or not. And if peer review and follow-up studies and the increased clinical experience that comes with widespread use of dexamethasone ultimately shows that it actually isn’t helpful for COVID-19, that will be tragic; but we should all understand now that that is just how science works, and won’t be part of some big government conspiracy to prevent people from getting the medication, just as it wasn’t with hydroxychloroquine.
But even more importantly, I wanted to talk about the RECOVERY Trial because it illustrates exactly what it looks like to fight this virus by engaging in mitigation and flattening the curve. Since April people have been saying (and we have all been feeling, to some degree or another) that if a certain amount of death and suffering from the virus is inevitable, we might as well just get it over with. We have also heard the slightly more sophisticated position that as long as our hospitals aren’t overwhelmed and we aren’t running out of ventilators and other equipment and resources for sick patients, then we have reduced the danger as much as is helpful and anything more is unnecessary. The RECOVERY Trial is a powerful illustration of why flattening the curve is beneficial even beyond these important goals. If you had a severe case of COVID-19 one month ago and had to be on a ventilator, you would have been treated with hydroxychloroquine and not with dexamethasone; today, you would be treated with dex and not with hydroxychloroquine, and your chance of dying would be 35% less; and that doesn’t even take into account the less quantifiable benefits from all that your doctors have learned about this virus in the meantime. A month from now, with more high quality trials and more clinical experience, who knows what the new standard of care will be and how much better a very sick person’s odds of surviving the virus will be because of it. The reason I wear my PPE with every patient and am a stickler about fomites and transmission, the reason I wear my mask when I’m in public, and the reason I am writing from home instead of a coffee shop today and attended church online this morning, isn’t because I’m afraid of the virus; it’s because when and if (and for me it has always felt more like an ‘if’ than a ‘when’) I get COVID-19, I would rather be treated by doctors and nurses and respiratory therapists who have had ample time to learn how to fight it, who have perfected their approach to ventilator settings and other supportive techniques for this virus specifically, and who have access to medications that have been carefully studied and have been proven to be effective; and because Iwould like to have that knowledge base and those techniques and medications available if and when I have to treat you.
I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now in 8-bit Color!
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Question #2: Do antibody testing and asymptomatic cases prove the virus isn’t as dangerous as we thought?
Asymptomatic Cases
The short answer here is, yes. And also in a very real sense… No. When antibody testing first began to confirm that a certain percentage of people contracted the virus but never developed symptoms, or had symptoms that were so mild they failed to associate them with the virus (‘weird how my allergies just acted for a couple of days’), it was great news for everyone. What it was not (and I’ve been on this soapbox for a while now) was proof that the ‘experts were wrong’ about how dangerous the virus is. I’ve been reading every model and study and expert opinion about COVID-19 I could keep up with for the past 3 months, and I cannot tell you the number of times that physicians and epidemiologists and researchers have either implied or explicitly stated that the mortality rates we were seeing from the virus didn’t account for asymptomatic and minimally symptomatic cases. I’m no expert, but I’ve typed it more times than I can count myself.
Actually I counted; it’s been 6 times. That’s still a lot.
Those scientists anticipated that a certain percentage of the population would contract the virus but never develop significant symptoms, but had to work from the best numbers they had until such testing was actually available. And it’s a very good thing that those assumptions were correct, since the original case fatality rates we were seeing were in the civilization ending range of 8-15% in certain countries. If antibody testing had been developed and found only a negligible amount of asymptomatic and minimally symptomatic cases, it would be devastating news for everyone; not least for the doctors, nurses, epidemiologists, and others who have turned their lives upside down to fight the pandemic. Accounting for asymptomatic and minimally symptomatic cases would clearly yield a much lower death rate, but still firmly in the very, very dangerous range. For instance, large scale antibody testing in New York in April found antibodies in 13.9% of the population (WBUR has an excellent article picking through the wildly varied estimates of asymptomatic cases) , which reduced their overall estimated fatality rate from 6% to 0.5%. Many current estimates place the overall fatality rate between 0.5% and 1.3%. For a virus this contagious, these are still scary numbers. Even here at the end of June, many people are still wanting to compare this to the flu to dismiss the danger, even though these much lower death rate estimates are still 5 to 13 times higher than seasonal influenza’s commonly accepted 0.1% fatality rate, and even though the flu itself regularly threatens to overwhelm our healthcare systems. Please keep in mind that this is at best an apples and oranges comparison. We don’t routinely measure influenza antibodies to determine the percentage of asymptomatic cases, focusing instead on those who are symptomatic, and our death rates for flu are based on a totally separate set of calculations (I talked about this in more detail in my response to the Bakersfield Urgent Care doctors). If you want to compare oranges to oranges we can look at excess mortality for both viruses. Consider the graph below from New York State: the first cluster of red crosses is the peak of the 2017-2018 flu season, the worst flu season I have experienced since starting medical school; the second is COVID-19 during New York’s surge in April.
Not the Flu.
Before we move on from asymptomatic cases, we need to mention two more things. First, while knowing the overall infection fatality rate including data from those who never had significant symptoms is great from an epidemiology standpoint, it doesn’t mean that the case fatality rate for people with symptoms is a ‘fake number’ or falsely elevated. If you develop symptoms and test positive for the virus, and especially if you end up in the hospital, it would be small comfort to know that some people didn’t get sick from it at all. We still need to know what the specific risk is for people with symptoms, and for people with severe symptoms, in order to properly counsel those patients and to inform our medical response. Second, asymptomatic cases are a double edged sword; yes, it means that some people will become immune without actually getting sick themselves, but it also means that some people can spread the virus without ever knowing they’ve had it. We all need to exercise caution even if we don’t have a cough and fever.
I realize this is the same joke from earlier. I just really like it.
Antibody Testing
One of the problems in determining a final overall death rate (besides the fact that we are still in the middle of the pandemic) is the accuracy of antibody testing, since we have to rely on this to tell us how many people had the virus and were either asymptomatic or didn’t get tested for it at the time. And this in turn relies on something called the positive predictive value, how likely it is your ‘positive’ test result has really detected the antibodies, which depends both on how well the antibody tests are designed (and their not being fake, which is apparently a problem now as well), but also on the prevalence, or in this case cumulative incidence, of the virus. The higher the percentage of people who have actually had the virus, the more likely it is that a positive test really represents a true positive and not a laboratory error. It’s a relatively simple concept, but honestly it’s just unintuitive enough that I’ve struggled with it myself for years. Basically, every lab test has some degree of error; sometimes these tests will tell you that you have the antibodies when you don’t, and sometimes it will tell you that you don’t have them when you really do. The more rare the virus has been in your area, the more likely that your ‘positive’ test was the result of such an error instead of actually having the antibodies. Carry this to the logical conclusion; if you brought an antibody testing system back in time to last Summer when nobody had SARS-CoV-2 antibodies, or for that matter back to Medieval England, you would still have some tests turn positive; but they would clearly all be from laboratory error because the prevalence of the disease then would have been 0%. When doing these tests, we cannot ignore the importance of how common or rare the virus has been in the region where we are testing.
Still less useful than bringing Sony Walkman
Calculating positive predictive value based on prevalence can be done with just a few numbers (test sensitivity, test specificity, and prevalence) and the simple equation PPV = (sensitivity x prevalence) / [ (sensitivity x prevalence) + ((1 – specificity) x (1 – prevalence)) ] (Um, there’s also an online calculator if you’d rather follow along that way), and it’s always shocking to me how quickly the lab error for even very good tests becomes relevant when the prevalence of a disease is low. Most manufacturers rate their antibody tests in the extremely accurate range of 95-100% for both sensitivity and specificity (because of course they do); some have performed well in independent testing, but others not so much. Let’s use the online calculator (or the equation above, if you just really like that sort of thing) and plug in a few of these numbers.
Scenario 1: Post-Surge New York City, excellent quality antibody test.
Let’s say you never definitively got diagnosed with COVID-19 during the surge in New York, and wanted to get an antibody test to see if you have already had it and are immune.
This means if you get a positive results from this very accurate test done after your city has survived a severe surge, there’s still about a 17% chance you don’t actually have the antibodies after all.
I hope you guys are having as much fun with this as I am.
Same scenario as the last, but the quality of the test isn’t quite as good as the manufacturer funded studies seemed to promise.
Sensitivity: 88.6% (.886)
Specificity: 90.2% (.902)
“Prevalence”: 4.6% (0.046)
Results:Positive Predictive Value = 30.4%
At this point you are probably better off just switching the ‘positive’ and ‘negative’ labels on the readout…
Now, savvy statisticians will note three things in looking at the above numbers and playing around with the data. The first is that I’ve used the very antibody testing methods I’m questioning to fill in the prevalence, which is itself part of my calculations. Figuring out the real prevalence is a complex problem epidemiologists are still trying to solve; this is a simplification for illustrative purposes. But more importantly, you will notice that as the prevalence goes down so does the likelihood that a positive test was really positive; in fact, it drops quite precipitously, especially as you get below 5%. However, as the specificity– the likelihood that the test correctly calls a negative result negative– approaches 100%, the number of false positives actually drops to 0. If we want to make sure we never tell someone they are immune when they aren’t, we need a very high specificity; but because no test is truly perfect, this will mean some sacrifices in actually being able to detect the antibodies when they are there, which hurts our ability to accurately estimate the number of asymptomatic cases. To get a perfect specificity, you will lose some sensitivity, and vice versa; the right balance depends on what you intend to use the test for.
So all of that to say, when that antibody test you got comes back positive and the manufacturer says their test is “95% accurate,” you may be tricked into thinking it means there’s a 95% chance you really have already had the virus and now have antibodies against it. But they are only telling you half the story, and you either need access to some more data to make your calculations and determine the real positive predictive value, or at the very least you need to take it with a grain of salt and still exercise caution; especially if your area hasn’t actually had anything like a true surge yet. After all, only a great fool would accept what he was given, and you are not a great fool.
I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now in 8-bit Color!
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Question #1: Isn’t the rise in cases just a reflection of more widespread testing?
This is a question that has been on everyone’s minds since the very earliest days of our testing woes, back in March when we had barely any testing available. It has ranged from a very fair question to a rhetorical device for spreading misinformation, with at least one prominent political figure even seeming to say that it would be better if we didn’t test so much so that our numbers looked better. I honestly believe most people really are curious about the relationship between our testing numbers and our numbers of cases and are not asking to try to minimize the appearance of the surge we are facing in Texas right now. In one sense, we will always find more cases of a disease when we test for it than when we don’t; that’s a truism. But if we want to determine whether cases are really going up we can look at a few other parameters than the absolute number of positive tests that will inform our understanding of the ’75 new cases’ or ‘5,747 new cases’ we are seeing in the news and on social media each day (To go through these numbers I highly recommend you spend some time navigating the Texas DSHS COVID-19 Dashboard; both their case data and testing and hospital data sections).
The first number is the percentage of positive tests.Ever since testing became more widely available in April and we were able to shift away from testing only those with a high likelihood of having the disease and/or of developing complications, we have been testing essentially the same types of cases; people with some combination of cough, shortness of breath, fever, loss of taste and smell, etc. and/or known or suspected exposure to the virus. There are many causes of these types of symptoms, from allergies to other respiratory viruses to chronic conditions like asthma and COPD, and in our pre-surge days these explained the symptoms in the vast majority of people we tested. If you look at the Texas testing data from April you will see two things; an overall low number of tests (a very modest 5-10k per day) and a fairly high percentage of tests that are positive, between 10-14%. This reflects our very strict testing criteria at that time; we were only testing the people we already really thought had it. In late April and all through May we see an ever increasing number of daily tests and a falling rate of positive tests, a reflection of liberalizing testing criteria and strong evidence of overall low prevalence in our State. Throughout June, and especially over the last 2 weeks, we continue to see an increasing number of tests each day; but we are now also seeing our percentage of positive cases rising again. This isn’t because we’ve tightened up or restricted our testing criteria again; it’s because more people actually do have the virus.
Percentage of positive tests
This exactly matches my own clinical experiences; back in May I was testing for COVID-19 based on essentially the same criteria and clinical judgement I am using right now, but it was rare to get a positive case; I would know, because being told you have COVID-19 can be a very stressful experience, so I still personally call every patient I’ve tested who has a positive result in order to answer their questions and help them process that information. This past week I have had to make multiple of those phone calls daily and have been feeling the strain on my time that it has created. As a physician I was on the front lines in May just like I am now, and I can tell you that we are definitely feeling this surge in a way we didn’t then; it isn’t a statistical artifact.
The second kind of data that should inform our understanding of that increase in cases is the number of people who are hospitalized with COVID-19; and the number of people who are dying from it. A raw increase in cases without a change in the test positivity rate could certainly be explained by more widespread testing; but it could not explain why more people had severe enough symptoms to be hospitalized, and there is no question that we have seen an increase in hospitalized cases.
Hospitalizations
Many people will quickly point out that we don’t know what percentage of those people were hospitalized for COVID-19 related symptoms and what percentage just happened to have a positive test when they came to the hospital for other reasons. This is a seemingly fair argument on the surface, but it is guilty of two fallacies. First is the idea of COVID-19 infection being a coincidence that doesn’t effect the trajectory of someone’s chronic illnesses. For months now I have heard the argument that the people whom we know have the absolute highest risk of COVID-19 complications, elderly people with chronic heart and lung disease, have not died from COVID-19, just with COVID-19. Yes, they happened to have the virus but actually died, in large numbers, from their chronic illnesses all getting worse at the same time, during a surge in COVID-19 cases in their area. This is the tired conspiracy theory that doctors are misattributing the cause of death to inflate COVID-19 death numbers, and it’s one I’ve had to debunk over and over again on this blog; it willfully ignores the pathophysiology of the virus, the normal course of those illnesses, and the way that doctors understand and report contributing causes of death. The idea that we are suddenly seeing a huge uptick in COVID-19 hospitalizations as an artifact of testing patients when they come in and unrelatedto the virus itself is just another version of that same conspiracy theory. It’s also a very hypocritical argument, considering the types of sources it is coming from. One of the criticisms about mitigation efforts from the beginning was that people who needed care might not come in to the clinic or hospital because of fear of the virus; it’s a very real concern and a problem I’ve fought against daily as a physician, and have been writing about since my earliest social media and blog posts during the pandemic.
Their argument has been that telling people that the virus is dangerous and taking mitigation measures would discourage them from seeking care for conditions that were really dangerous, like congestive heart failure or blood clots in the lungs, because they were more afraid of catching COVID-19 at the hospital. Our argument has been that the virus is dangerous, and that it also makes congestive heart failure more dangerous and actually causes blood clots in the lungs, so we have an obligation to keep people safe from the virus and help them navigate when and how to seek care for other health concerns; it’s work we are doing constantly in our clinics and hospitals. Now these same sources are arguing that in the midst of a dramatic increase in cases and our first real surge in Texas, thousands of people with conditions that put them at risk for complications from COVID-19 suddenly aren’t worried about the virus after all and are all seeking hospital care at the same time, and just happen to test positive for the virus while they are there. There may well be some situations where this actually is the case, and people who were overlooked by our healthcare systems really are now getting very sick from their diabetes or coronary artery disease at the same time as our surge (you can only ignore a worsening chronic illness for so long before hitting a crisis point), but the idea that this would happen on a broad scale, all at the same time, and that enough of those patients would be positive for COVID-19 that it would cause a state-wide spike in hospitalized virus cases is a very, very, frustratingly silly argument.
The final number we need to consider is the number of deaths, and here at least there is some good news; we are not seeing a substantial increase in the people in Texas dying from COVID-19, at least not yet. There are two ways to understand this. The optimistic way is to think that something has changed; either the virus has somehow become less deadly than before, or our increased understanding of COVID-19 has led to a better ability to fight the virus; improved disease-specific ventilation strategies, effective drug therapies, and more efficacious supportive care measures. In fact, there is a great deal of evidence that the latter really is true, as we will discuss in another post. But the pessimistic view (and the truth is probably a combination of both) is to realize that most people do not just get admitted to the hospital with severe COVID-19 infection and pass away the same day. There is a significant lag time as those patients are treated and fight against the virus, and our surge in hospitalized cases is only a little more than a week old.
Many of those hospitalized patients are fighting for their lives in the ICU right now, as the hospitals are starting to fill up around them and their nurses and doctors are becoming fatigued. Many of those people will recover, but many will not; and it will take a couple of weeks, and often times much longer, to see how many, and who. As we’ve seen elsewhere, the ratio of those who don’t recover will only increase if resources and the margin for careful attention and heroic efforts on their behalf begin to run short. Yes, our improved understanding of the virus and more effective therapies gives us a better chance to fight the virus than Italy had in March or New York had in April; but doubling down on the difficult work of mitigation now to prevent our healthcare systems from being overwhelmed in a couple of weeks when more and more patients reach their crisis point is every bit as important.
What will next month’s data look like? It’s still partly up to us.
I had intended to write this weekend on a variety of topics, including herd immunity, the recent RECOVERY trial using low-dose dexamethasone in critically ill COVID-19 patients, antibody testing, and the question of whether the increase in cases is really just due to increased testing (answer: unfortunately, no). But when I woke up this morning the world seemed suddenly, vehemently, and inexplicably divided on just one subject: wearing masks.
Part of this can be accounted for, at least locally; yesterday the City of Waco issued an order requiring businesses to create and post mask policies for employees and customers. As with anything that has been unnecessarily politicized and sensationalized, I recommend you read for yourself what the order actually does and does not require. This morning I had half a dozen messages asking for my thoughts on whether or not masks are an effective strategy, and several people shared pieces of misinformation they wanted to bring to my attention.
So while I would still like to write about all of the above issues, I think this one will have to take priority today.
Are masks safe and effective?
G.K. Chesterton said that he was most convinced by evidence that is ‘miscellaneous and even scrappy.’
“A man may well be less convinced of a philosophy from four books, than from one book, one battle, one landscape, and one old friend. The very fact that the things are of different kinds increases the importance of the fact that they all point to one conclusion.”
G.K. Chesterton, Orthodoxy
So while we will look at scientific studies, journal articles, and other medical evidence, I want to include data from various kinds of research, including both laboratory conditions and real-world epidemiology, and from both prior to and during the COVID-19 pandemic. I also want us to apply some common sense and a good bit of our own past experiences. This can be dangerous in a field like medicine, where realities are often counter-intuitive, but if undertaken cautiously this common sense approach can serve as an anchor for the more academic information.
With that in mind, I think we can start by thinking about the advice we give to children when they are sick or have seasonal allergies (if your children are like mine, these efforts are ultimately futile, but struggling against that futility is a time honored parenting tradition). We tell children to place their hands over their mouths when they sneeze or cough. If we are particularly savvy (and can get past the occult theme; looking at you anti-Harry Potter friends), we teach them the Vampire Sneeze/Cough, where we cough into the antecubital fossa (the bend of the elbow) instead of our hands.
It does work much better if you wear a cloak at all times.
Why? Because respiratory viruses are spread through respiratory droplets; mucous and saliva from the respiratory track that contains the virus. In this article we will look at the filtering ability of various types of masks and whether they are actually able to catch the microscopic particles that cause illness, but you don’t need a microscope to measure the number of microns between a toddler’s fingers when she almost but not quite entirely fails to cover her mouth for a cough; it’s a lot.
Now it’s true that these etiquette maneuvers do not actually stop or absorb all of the particles; they catch some and merely redirect others into the surrounding environment. But you knew that. If you live with a sick child, the odds of yourself or another family member getting sick is high regardless of how good they are at vampire coughing. The goal isn’t to stop 100% of the droplets, but to modify the spatial distribution; to make it less likely that you will get sick from someone coughing or sneezing a few feet away or across the room. Even in science some things are intuitive; if you can feel the spray of respiratory droplets on your face when someone coughs near you, you know your chances of getting sick are higher.
This is the same principal we are talking about when it comes to masks. Nobody is saying that if someone has COVID-19 they can just wear a mask, N95 or otherwise, and cough and sneeze without getting anyone sick; studies have show that the particles still escape. But if someone coughs across the room from you, their mask or their elbow, or even better both, interrupts the momentum of the droplets (50 mph for a cough, 100 for a sneeze according to a study in the Journal of Fluid Mechanics) and decreases the chances of the droplets reaching you, giving you time to move away or at least cover your own face, blocking a few more particles. These are components of an overall risk mitigation strategy that involves things like social and physical distancing, frequent hand washing, sitting outside instead of inside, contact tracing of COVID-19 patients, and staying home if you are sick.
Masks aren’t perfect, but nobody is claiming they are.
It’s also important to note that the studies that have shown only very modest benefits of masks, such as the study that produced the graph above, have focused on the spread of droplets through coughing and sneezing; high pressure, high velocity events that force droplets through and around barriers such as masks and sleeves. However, the City of Waco is not asking 100,000 people to wear a mask in case one of those people happens to cough in HEB. We now know that both asymptomatic and presymptomatic COVID-19 transmission do indeed occur, and the mechanism of transmission still seems to be from saliva and respiratory mucous, including respiratory droplets and aerosols, even in the absence of coughing and sneezing. Talking, forcefully exhaling, singing, yawning, spit talking; all of these are lower pressure events where a mask may actually block, rather than redirect, a higher percentage of these small, lower velocity particles. Again, you already believe this intuitively, because you cover your mouth when your breath stinks.
Or you should.
I also think that revisiting our actual real life experience and common sense is particularly important when dealing with medical misinformation, which is often found to be self-contradictory and manifestly illogical within only a few moments consideration and comparison to facts we already know. It rarely takes being a physician or another scientist to figure out that these wild claims on social media aren’t accurate, though I’m sure it helps.
Unmasking Mask Misinformation (sorry)
A friend sent this to me this morning; it was posted on a public forum (“public forum” sounds so much more legitimate than “Facebook comments”) as a response to our city’s new masking policy. I’ve also been sent a longer paragraph format piece that starts “I am OSHA 10&30 certified.” Since they overlap quite a bit, I won’t re-post that one in its entirety, but it’s just full of contradictions (‘surgical masks only filter on the exhale’ yet ‘become useless’ for protecting you if your breath clogs them), false claims (‘N95 masks can’t filter COVID-19’, ‘asymptomatic spread doesn’t occur’), and nonsensical statements (if you wear a mask and get exposed to COVID-19 you become a walking virus dispenser, cloth masks are worse than no barrier at all). It does make one really excellent point though; if you are relying on wearing a mask to fully protect you from getting or spreading COVID-19, that is indeed a false sense of security. We can’t say that often enough; but it just doesn’t follow that masks are worthless or make the problem worse, which is what they repeatedly claim. I’d like to go through the claims above in order, before concluding with some final arguments for masking.
Claims #1 and #2: Masks decrease oxygen intake and increase carbon dioxide retention.
This is something that has been studied extensively, and there is no evidence that simple surgical or cloth face masks will cause hypoxia or any significant decline in oxygen levels. Oxygen molecules are very small and diffuse easily both around and through these types of masks; they are nowhere near the size of viruses, or the much larger respiratory droplets that carry most of the virus that is exhaled. The same is true about Carbon Dioxide, which is only slightly larger.
But you can also consult your own experience here. Many types of people already wear masks for many hours of the day, from surgeons to certain industrial workers, and women in many cultures wear face coverings as a part of their public clothing. Yet we do not consider these persons to be at high risk for either hypoxic (low oxygen) or hypercapnic (high CO2) injury. A big part of the problem is that we have sensationalized the wearing of masks during COVID-19 and have started to treat it like it isn’t a normal part of our experience already, which it absolutely is. Whether it is the above examples, or Halloween or Comic-Con, or my 5 year old spending three weeks straight in his Spider-Man costume and refusing to wear anything else, the wearing of masks is something we all have some degree of experience with and have never really been concerned about until now, when we are suddenly being told they are extremely dangerous, generally by the same people who have been spreading various types of COVID-19 misinformation since mid-March.
But more to the point, you can study this on your own. A battery powered pulse oximeter is very accurate and costs about $12, and you can use one to do a simple experiment that will reassure you, at the very least, that your face mask is not causing your oxygen levels to drop. Check your oxygen level with your mask off, and then wear it for however long you expect to need it when you are out running errands or whatever scenario you are worried about. Then check it again. In general in a healthy adult, readings above 95% are normal and below 90% are concerning. As an example, I’ve been wearing my properly fitting N95 for the last half-hour and my O2 saturation has fallen exactly one percentage point.
I’ll admit, I freaked out for a minute before I realized the labels are upside down.
There is one group of people we should mention here, and that’s people with chronic lung disease such as COPD or Asthma. For people with these conditions, the increased heat and moisture of the air within the mask, and the decreased air flow directly to the nose and mouth, really can create both real and perceived difficulty breathing (and in these conditions, these trigger each other so easily that drawing a distinction between the physiologic respiratory distress and the anxiety-provoked sensation of respiratory distress is almost a false dichotomy; not being able to breath is scary). These are also conditions that predict a higher likelihood of severe illness in COVID-19, which complicates matters. For these individuals who should already be taking every precaution possible for their own safety in the midst of this pandemic, the decision of whether and what kind of mask they should wear when they do have to go out should be a discussion between them and their doctor. For the rest of us, especially those of us who personally care about someone with Asthma or COPD, it’s important that we take every precaution we can; it should go without saying that our “what about someone with a chronic respiratory illness” should only ever be a legitimate question on their behalf, not a rhetorical ‘gotcha’ to turn off our intellectual honesty on this issue and dismiss the benefits of everyone else wearing a mask.
Claims #3 and #4: Masks shut down the immune system and reactive your own viruses.
The third claim, that masks shut down your immune system, is just a reiteration of the above two, and there is absolutely no evidence for it. As we’ve already said, doctors, nurses, and other medical professionals, and especially those involved in surgery, wear masks all the time without any fear of their immune systems being shut down or weakened. And while these types of people are often fearless when confronting deadly situations or illnesses in order to care for their patients, as we have seen throughout this pandemic, they tend to otherwise be fairly health conscious. I still remember being shocked during a group discussion in medical school when we were asked what it was we valued most highly. I was trying to honestly wrestle with whether I valued my faith, my wife, or my daughter most, and how it was even possible to separate those things from one another, when my friend answered “my health,” and several others nodded in agreement. I have no judgement for that person, but the whole idea was very alien to me (and maybe that shows something of my privilege in having lived overall a very healthy life, often despite my personal choices). Maybe this friend would risk the thing he valued highest on behalf of a patient (in fact I think he would); but if there was any evidence that his health was imperiled by wearing a mask, he would be leading the charge against masking (just checked facebook; he isn’t), and probably would have been doing so since medical school.
The fourth claim is one that I first came across in the Plandemic “documentary” last month, and based on the wording it seems to be taken directly from there (or they are both taken from a 3rd, unknown source, which I’ll call “Q”)(I’m now being told that “Q” is already taken). The actual claim is that wearing a mask will activate dormant retroviruses that live in your body. Retroviruses are a family of viruses that replicate by inserting viral DNA into host cells and hijacking cellular machinery, and only a few known species causes disease in humans, including HIV and Human T-Lymphotropic Virus, which can cause certain cancers. This claim is very specific and very conspiracy-theory oriented, but I suspect that this distinction between retroviruses and common viral illnesses like cold and flu is not being made by the people spreading this meme.
The long and short of it is that this just isn’t the way the immune system works. You don’t have a host of dormant viruses sitting in your lungs that, if breathed into a cloth or small space and then breathed in again, will suddenly become active and cause an infection. Do you get sick when you sit in a car? What about when you hold your breath? What if you sleep with your face too close to a pillow? Is there evidence that we see more respiratory infections in people that wear masks regularly? Of course not. In someone who has a functioning immune system, once your immune system has seen and defeated a virus, you cannot give that virus to you; you already have an effective immune response to it. There are a small number of exceptions, like getting shingles through varicella zoster reactivation, but coronaviruses aren’t one of them and there is no evidence that wearing a mask or breathing out and then breathing in the ‘same air’ has anything to do with viral reactivation; there isn’t even a physiologic mechanism that would make this possible.
Claim #5: The virus is too small to be trapped by the masks!
This is where both the misinformation and the answer get a bit more technical, and if you want all of the scientific details, the blog First10em has an amazing article on masking, viral transmission, the 6 feet apart rule (which they call the “2 meter” rule, whatever that means), and the transmission patterns and particle sizes of both droplets and aerosols. The question of whether various types of face masks besides N95’s actually do filter the COVID-19 virus itself is still an unanswered question, but the answer seems to be, to some degree, yes. Studies have shown different types of masks to have varying filtering efficacy even down to to very, very small particles in the range of 300 nanometers or less, in fact right in the range of the virus itself (the SARS-CoV-2 virus is roughly 120 nanometers; an earlier version of this article incorrectly reported the size of the measured particles in this study as 40 times smaller than the virus, which was just due to me getting my conversions wrong. Sorry; pay attention in 8th grade algebra, kids), but other studies have shown that the virus is still able to transmit through (or around) masks, at least to a few inches away and if propelled by a cough. Taken together these studies seem to reiterate what we have been saying all along; masks aren’t perfect, but they do decrease the risk, especially in short-term contact with non-cough, non-sneeze related transmissions like we would see in asymptomatic and presymptomatic cases. Indeed, this is confirmed by a Hong Kong study in 2011 that found that the protection offered against respiratory pathogens by all types of face masks decreased with higher velocities and prolonged exposure.
Again, Oxygen molecules are < 0.5 nm
Regarding this piece of misinformation though, we can summarize the two main errors pretty succinctly; the virus isn’t floating through the air by itself, it’s suspended in respiratory droplets and aerosols; and the masks aren’t supposed to block 100% of the particles on the microscopic level (though that would great), just trap most of them and slow the others down. The mosquito through a chain link fence analogy is silly because mosquitos can fly around barriers volitionally, and because it uses the size of the virus instead of the size of the respiratory particles, which are much larger (1-100 microns, mostly, instead of 0.12 microns). But if you want to use the analogy, it’s more like hitting golf balls through a chain link fence; yes, the gaps are bigger than the golfballs, and some will go through if they are hit really hard; but many will be blocked outright and many others will be slowed down and redirected.
Claim #6: There is no evidence to support masks.
We have already looked at some of the various types of evidence that I believe we all find somewhat convincing. We believe as a culture that masks are least helpful in preventing infections in some situations, such as surgery, and believe they are safe when we wear them for cultural or religious reasons, as part of our jobs, or as part of costumes. We engage in barrier maneuvers (some better than others) to block large respiratory droplets when we cough and sneeze. We know the masks redirect and lessen such droplets even in these high-velocity conditions, and we’ve seen the evidence from physics and fluid dynamics studies that they can filter the smaller aerosols under low-velocity conditions. For me, the last remaining piece of the puzzle is, “does it actually work, really?”
I want to look at two more types of evidence; epidemiology evidence from before the COVID-19 pandemic, and emerging epidemiological data from right now. An Australian study in 2009, well before the COVID-19 Pandemic (but you knew that), found that the wearing of face masks did diminish the transmission of upper respiratory illnesses even among household contacts, but that there were fairly low rates of compliance with masking. If masks were worn more, they could help significantly.
“Adherence to mask use was associated with a significantly reduced risk of ILI-associated (Influenza Like Illness) infection. We concluded that household use of masks is associated with low adherence and is ineffective in controlling seasonal ILI. If adherence were greater, mask use might reduce transmission during a severe influenza pandemic.”
This study and others like it, 10 years prior to the COVID-19 pandemic, should at least put to rest any ideas that wearing masks is a novel recommendation or a government ploy to control yet another aspect of our lives. Masks have been recommended, and shown to work, for preventing respiratory virus transmission for decades; any suspicion of them now likely comes more from the current hyper-politicized, conspiracy saturated climate than from anything else. But the COVID-19 virus is new and acts very differently from other respiratory viruses in so many ways, so what’s to say that masks will be effective for COVID-19?
It is too early in this pandemic to have robust and definite conclusions about which measures helped most and which showed modest or negligible benefits. We know that social distancing helps from evidence in places like Sweden and Norway, and we now seem to be living the results of relaxing our own social distancing measures without other robust mitigation strategies in place. When it comes to masks, we could compare the United States, which is (apparently) very resistant to masks becoming a social norm to places like South Korea where wearing a mask has been the norm since early in the pandemic; but this comparison is complicated by vastly different healthcare systems and populations and by a strong difference in adherence to other mitigation efforts as well, which we Americans have also been consistently defiant of.
Population: 328 Million
Population: 52 Million
I do agree in principal with the approach by one writer to the CDC’s journal, Emerging Infectious Diseases, in comparing Taiwan to Singapore; but again this is not a perfect comparison by any means.
Update: It has been pointed out to me that there are now several recently published studies, conducted during the COVID-19 pandemic itself, that have looked at the issue of mask wearing to determine if the benefit is significant. You can find two of them here and here (with thanks to Baylor Epidemiologist Dr. Emily Smith, PhD, who has written an excellent summary of the current evidence for masks). I’m sure many more studies are ongoing. Of course none of these are going to be able to perfectly measure the effectiveness of masking under real life pandemic conditions; if you can imagine a scientific experiment that could, it would probably be unethical and immoral (and logistically impossible), such as taking members of a population and randomizing them to wearing or not wearing masks and then measuring how many become sick from each group. Those types of study designs are entirely off the table, so we analyze epidemiological data; looking at what happened in countries, regions, and cities where masks were adopted early, and what happened in other places after they were adopted later on. It isn’t possible to know how well the mask policies were followed from such data, or to perfectly tease out confounding factors like social distancing measures, the success of contact tracing, and the robustness of testing programs; it wouldn’t be possible to say masks are the most important thing if they are always or nearly always used in conjunction with other mitigation strategies, which is exactly how they should be used. But these studies do conclude that implementing mask policies (and following them!) makes a significant difference in the trajectory of this pandemic, and taken as just one important kind of the multiple kinds of evidence we have looked at, I do think they contribute to a convincing case for wearing masks.
Ultimately, once this turns the corner, we will never be able to say with certainty what the real answer was; whether it was wearing masks that helped the most or the heightened caution in other areas when cases began to climb, whether reopening resulted in a surge here in Texas or if it was our bucking of social distancing all along, whether each of our mitigation measures individually made a difference or not. What we can say for certain is that the American method so far has not been working. By denying the disease’s existence and danger, producing conspiracy theory after conspiracy theory, claiming we beat it prematurely, and fighting tooth and nail against every reasonable recommendation and rule meant to protect ourselves and our neighbors, we have taken a global pandemic and made it largely into an American pandemic, with the highest number of cases and deaths in the world.
There is plenty of evidence that masks are safe, and that they stand a fair chance of helping, especially against asymptomatic and presymptomatic spread. If you are sick, get tested, stay home, and isolate; make sure you get the medical care you need. If you are well and can physically distance yourself from others, then distance yourself from others while finding ways to still care for your community and your own mental and physical health. If you cannot distance because of strong religious or moral convictions or the realities of your job, or due to strong personal preferences, then please wear a mask and wash your hands frequently.
This is just one of the ways we can do better during the rest of this pandemic; myself included.