Before I started blogging about medical misinformation, my last blog (which lasted for exactly one post) was called “Mad Virtues.” It was based on this quote from G.K. Chesterton:
“When a religious scheme is shattered it is not merely the vices that are let loose. The vices are, indeed, let loose, and they wander and do damage. But the virtues are let loose also; and the virtues wander more wildly, and the virtues do more terrible damage. The modern world is full of the old Christian virtues gone mad. The virtues have gone mad because they have been isolated from each other and are wandering alone.”
G.K. Chesterton
While my intention was never to deny the existence either of real nefarious intentions in the world or of original sin, my thesis was that most disagreements, and especially the most deeply felt and violent disagreements, were actually due to a clash of deeply but disproportionately held virtues; virtues that had gone mad, and caused terrible damage, because they had been isolated from the other virtues and truths meant to keep them in check.
In general, I believe this is true today, and I believe it applies to the content of this blog. I think that people like Dr. Richard Bartlett or Dr. Ivette Lozano really believe they are doing the right thing by treating all of their patients with budesonide or hydroxychloroquine, and encouraging people around the country to seek out these unproven therapies for mild COVID-19 cases. I think Dr. Dan Erickson and Dr. Artin Massihi really convinced themselves that their erroneous statistics were valid, which allowed them to view the harm that the shutdown was causing to their own business and the economy around them as a greater threat than the virus. I even believe that Dr. Judy Mikovits, with 20 years of fighting the medical field and presumably becoming increasingly entrenched in narratives of far-reaching conspiracies among doctors and scientists, earnestly believes that her Plandemic interview was an opportunity to expose the “truth” about the virus.
In each of my responses to each of these viral misinformation videos, I have tried to assume the best; that the intentions of those making the videos, like those sharing them, were sadly misguided, misinformed, and erroneous, but ultimately sincere. I hope that if I ever fall into unintentional but very public professional error and embarrassment, the same grace would be shown to me. But today I’d like to try something a little different; instead of assuming the best, I’d like to assume the worst; I want to ask what the game plan would be if a doctor were in fact knowingly lying about the virus; what they would stand to gain from such an immoral act.
Are most doctors lying, or just a few?
As soon as we abandon the idea that deeply held differing opinions dramatically shape our perception of events and even our understanding of statistics (in other words, that most of the doctors who are deceiving others are only doing so because they have already deceived themselves first), we are left with only one alternative conclusion; someone is deliberately lying. So who is it? According to a recent tweet that was retweeted by the president, it’s most doctors.
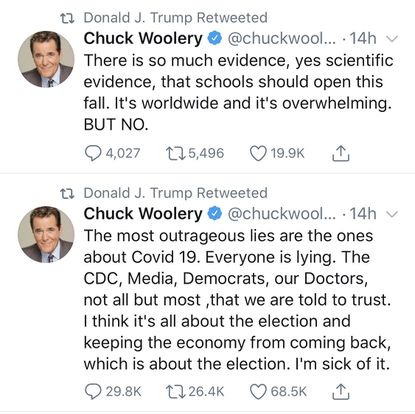
If we follow this theory, we are going to arrive at some uncomfortable but fairly inevitable conclusions. First, it means that I am lying, because on this blog and in my conversations with patients, family, and friends, I’ve consistently been repeating the ‘party line’ that COVID-19 is very dangerous and encouraging people to exercise caution and take it seriously. It means that when I told you in my last blog post that I was worried about a lot of my patients who have pre-existing heart and lung disease, I actually just wrote that because it made me sound like a compassionate doctor. It means when I said at the end of June that I was seeing a steep rise in the number of positive tests at my clinic, I was making that up and just banking on none of the nurses or lab techs I work with reading that and calling me out on it (I don’t have to worry about the other doctors; they are all in on it too). It means that the long nights and early mornings and sacrificed Saturday afternoons it has taken to write this blog on the side of my full-time clinic job has been motivated not by the stated desire to provide clear (if a bit long-winded) refutations and explanations to dangerous medical misinformation, but by a desire to run a convoluted and ineffective interference to people like Love Connection up there tweeting the truth about the virus. And all I can say is, hey, I’m just as shocked as you are. My wife is going to be very upset when she reads Mr. Woolery’s tweet and realizes that the reason I’ve failed to build her that Ana White potting bench for the past month is because I was busy deceiving some very, very small segment of the American public.
It also means my friends from medical school and residency have been lying, not just to the public but also to each other. Since late March I’ve reconnected more frequently and with a wider range of former classmates and co-residents than I have in years as we’ve checked in on one another and provided updates and insights from our own experiences with the virus. I’ve talked with friends working in the ED in New York during their worst weeks of crisis, and with friends working in rural hospitals that have seen hardly any COVID-19 at all. You could fill libraries with the texts, e-mails, and facebook messages that have taken place between doctors in the past 4 months, and not a one of those has been to clarify the latest lies the WHO, CDC, Bill Gates, and Dr. Fauci want us to push this week (not exactly true; that has been said a lot and is actually a pretty tired joke by now. At least, all of my friends are tired of me making it). If those texts and e-mails are ever subpoenaed, the American public is going to learn a lot; but not about any conspiracy.

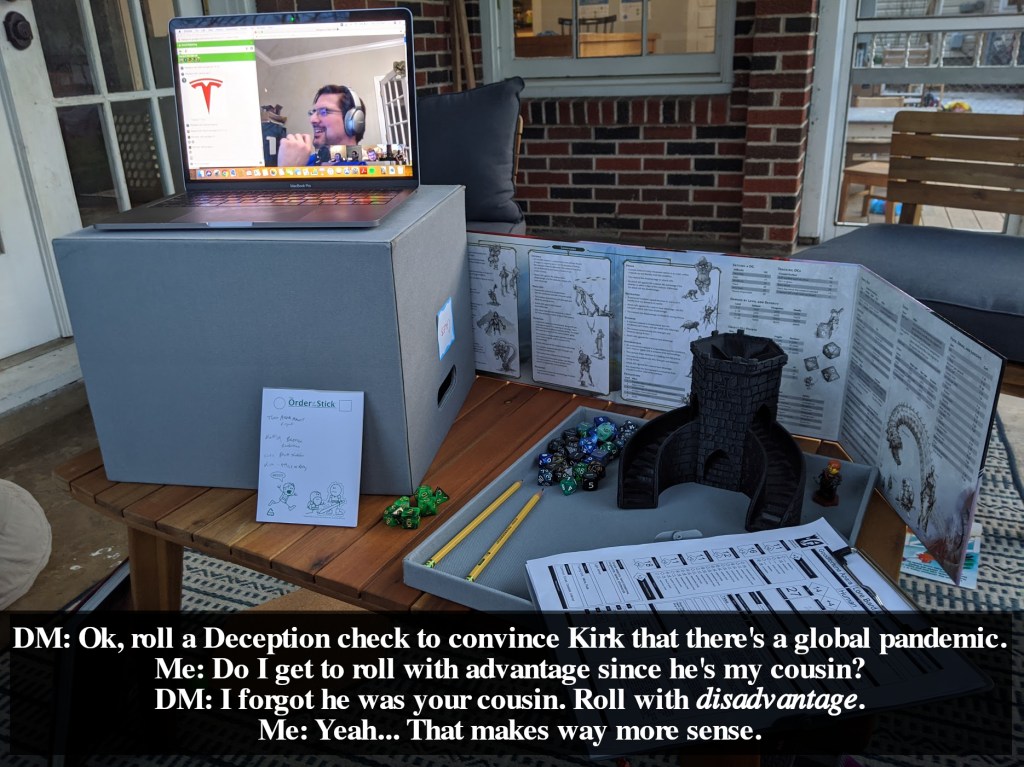
And by the way, not all of those conversations are private, although more are now because of social distancing. Even though we aren’t sitting at coffee shops having these discussions, many take place on very public Facebook comment threads instead of private messaging, and a pediatrician friend and I have had more than one of our Google Hangout Dungeons & Dragons sessions derailed by comparing notes about the virus while the rest of our party waited patiently for us to get back to the quest at hand. If you believe that most doctors are lying about the virus, you have to believe that these types of conversations are actually planned and carried out to deceive friends and loved ones who are not doctors. There’s a joke about ‘rolling a deception check’ in there somewhere, but I don’t have the emotional energy to think of it. Every time you see two or more doctors talking about the virus, how dangerous it is, or what they’re doing to fight or prevent it, that’s a staged performance for the benefit of the public.
So why all of this lying? We have consistently been given two explanations; because we want to hurt the economy (in order to hurt Donald Trump’s chances of re-election), and because we want to make money. You might notice right away that these two motivations almost but not exactly completely contradict each other. I’m sure it is possible to both want to hurt the economy overall and stand to make money yourself (and here I’ll be called naive by friends who believe that this is essentially the go-to strategy of the ultra rich), but for someone earning a wage like a physician it must be somewhat rare; we would really have to spend some time with a fresh cup of coffee and some excel spreadsheets to make sure that the ‘extra money’ we were making would be enough to offset the hit to our 401k’s and Roth IRA’s, not to mention the doctors who actually own stocks. Honestly, I’m surprised the White Coat Investor hasn’t done an article on “5 financial reasons you should trick people into believing in COVID-19 (and 5 reasons you should blow the whistle on this global conspiracy of doctors and scientists now!).”
If we look at them separately, the first one feels like the type of thing that makes sense only if you forget that you actually know some doctors, and makes even less sense the more doctors you know. For me it’s easy to intuitively disbelieve that doctors as a group are out to get Donald Trump because for the past 13 years I’ve had to endure an almost endless stream of Fox News in every doctor’s lounge I’ve been in from here to Denver. But if you only know one doctor and they happen to vote the same way you do, you might think your doctor is ‘one of the few telling the truth.’ If they do think the virus is a pretty big deal, you might think they have nuanced and complex views on the pandemic, which is probably true, or that they are essentially honest but have been ‘tricked’ by the CDC or other doctors or whomever. But if you knew hundreds of doctors, like I do, you would have to face the reality that while there are many you like and trust and a few you don’t, and while they fall all over the political spectrum, you would be hard pressed to pick even a handful that would be willing to participate in anything like a conspiracy, and that as a group they would be even less likely to be duped by a medical conspiracy if there was one.

Doctors are not a monolith, and we don’t vote as one. In fact, some of the medical specialties that have been most negatively impacted by the pandemic financially, like Surgery and Otolaryngology, and some that have been most intimately involved in COVID-19 treatment, like Pulmonology, Anesthesiology, and Emergency Medicine, are the exact fields that vote Republican at higher than average rates. There’s only so far you can take this information, and it’s probably true that Donald Trump has lost some physicians from his constituency since this data was collected just before the 2016 election; but at the very least it shows that that if COVID-19 were really a conspiracy to hurt the president, there would be thousands of Republican critical care physicians coming forward to reveal this, instead of a handful of urgent care and concierge medicine doctors. I personally know several doctors who are fighting the virus on the frontlines and still plan to vote for Donald Trump in 2020 despite being frustrated with his administration’s response to the pandemic; for them, a virus is not a political issue, even if it is being used as one.
But the second one is actually even more ridiculous. I’ll start with myself again. Of course it doesn’t matter since we’ve already established that I’m lying about everything, but I can tell you that I’ve made exactly zero extra dollars from COVID-19. I am thankful to work in a clinic system where my personal income isn’t determined by the number of patients I see or what type of insurance they have (our work volume is instead driven by the extensive primary care needs of the population we serve), and unless somebody votes to give frontline doctors hazard pay or student loan forgiveness, this pandemic seems extremely unlikely to be some sort of lucrative opportunity for me (I’ve got a pretty good life insurance policy, though, and my med school loans are non-transferrable, so it could end up being fairly profitable for Katie by the end)(grab a screenshot now, because she’s going to make me delete that one as soon as she reads it). I have put in dozens of hours of overtime, mostly back in March and April helping our clinic get ready for whenever the virus finally surged in our area, but this was all gladly done and entirely unpaid, and I certainly wasn’t alone in this. Since then I’ve spent many hours writing this blog, but it would be hard to argue that this is financially motivated either since so far the net earnings of tjwebbmd.com is negative whatever the cost of WordPress Premium is.
But not every doctor has the same type of employment contract that I have, and when we look at other types of business models we discover that my not especially profitable is the very best case scenario for most doctors during COVID-19. Remember that social distancing measures meant thousands of primary clinics cancelled any appointments they felt their patients could safely postpone as soon as COVID-19 cases began to rise in the US; despite the fact that many of them could ill afford to do so. Some of these clinics closed for good, and this unfortunate side effect of the virus, which is going to affect the health of many people for years to come, was actually put forward by COVID-19 conspiracy theorists alongside the idea that most doctors were lying about the pandemic, without any apparent irony. I know doctors that work for larger healthcare systems who were laid-off during the pre-surge months of the pandemic here in central Texas, not to mention surgeons cancelling elective cases and many hospitalists and ER docs working fewer shifts because hospitals volumes were so low (this is outside the scope of the discussion, but we talked about this phenomenon most recently in my response to Dr. Simone Gold and her A Doctor a Day campaign). For most doctors, COVID-19 has been either financially neutral or a financial hardship.
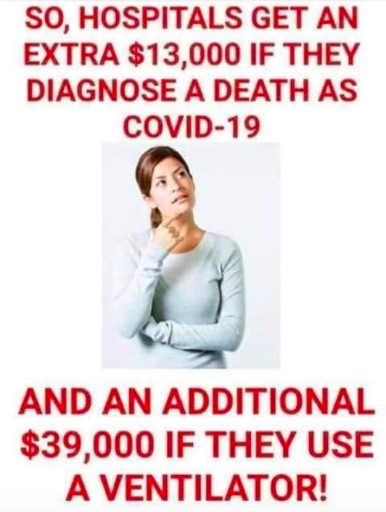
But what about that big $39,000 paycheck hospitals are presumably getting for putting a patient on a ventilator? We’ve dealt with this conspiracy theory before, and you can read all about it on Snopes.com, or you can wait until this weekend when we try to tackle this meme and a whole bunch of others on the blog. But even if you believed this crazy theory that doctors are intubating people who didn’t need it in order to get their hospital a big pay check (instead of, say, actively working to push the limits of non-invasive ventilation for every possible patient, which is what they are actually doing), consider what else you would have to believe to think this somehow explains “most doctors” lying about the virus: 1. The doctors are getting the money instead of the hospital (yeah, right), 2. the other doctors and nurses and healthcare professionals that know the patient’s case are complicit and staying silent in massive numbers, 3. ER docs are admitting patients who don’t need to be in the hospital just so that their critical care counterparts can get put them on ventilators and get those payments (“set ’em up, knock ’em down”), 4. other doctors who are not involved in the hospital care at all and cannot possibly get a cut of that money are lying about the pandemic and letting their practices get closed so that another doctor in town can make money intubating patients unnecessarily, and 5. they are doing all of this despite their Oaths to do no harm, years of devotion to caring for people, a very real chance of getting caught, and, for about half, the fact that the whole conspiracy is designed to hurt a president they voted for in the first place.
That’s a lot. I’m not saying it’s impossible, but $39,000 seems like a pretty low-ball figure to betray all of the ideals we hold most dear and participate in some grand plot at the expense of the American people. Maybe come back when you can afford to pay us whatever the insurance companies pay their doctors to deny prior-authorizations all day.
You want a cure?
But what if it’s the other doctors who are lying? What if it’s not doctor after doctor I see on Facebook and Twitter saying ‘stay safe, please wear a mask, please do physical and social distancing in order to keep you and your families safe from the virus’ that are trying to deceive you with this advice because it somehow makes them money (Step 3: ???… Step 4: Profit!), but the handful of doctors writing things like this:

The social media post is about 2 weeks old by now, which I realize is ancient in internet misinformation time. One of the struggles of doing this as a hobby on the side of a full-time job. Regular readers will notice I’ve done something unusual for this blog: I’ve omitted the name of the author I am responding to. This is a fellow Texas physician a few hours north of here (whom I’ve never met), and his name isn’t hard to find; I’ve even mentioned him when referencing this post in prior essays and his post has been viral on social media. But I’ve omitted his name here because, unlike in those other essays, I plan to treat this post as cynically as possible. I’d like to work through this post and ask what we can conclude about this doctor’s practice style, COVID-19 testing and treatment policies, and overall goals in writing this post, and while I believe my worst-case-scenario conclusions are a valid interpretation, I sincerely hope that the real, living and breathing, created in the Image of God person who wrote this is better than he will get credit for in those post. He probably is, and so I’ve erased his name from his post and plan instead to treat the author as a fictitious person.

Dr. Lozano is the doctor who spoke about Hydroxychloroquine at the Set Texas Free Rally way back in mid-May. I wrote a response to her speech at the time and tried to address her use of Hydroxychloroquine in the outpatient setting for minimally symptomatic and even asymptomatic patients. Since the doctor in this post is using it much the same way, I won’t spend as much time on this and will to some degree take it as a given that we agree this is an improper use of the medicine, or at least that you have heard my side of the argument already.

I think this is a really fascinating set of claims, for a couple of reasons. First, as I said in the post responding to Dr. Lozano, numbers matter. This doctor claims at the end of June to have been treating people in the ‘outpatient trenches’ for 2 months, but like the rest of Texas, McKinney began to hit a surge in cases just about a week prior to his post; by the time of the post there had been less than 500 in the entire city, and fully half of those were in June; at the end of May the total confirmed cases in McKinney was 251. He goes on to say that he has treated ‘over 50’, (which, since we are being cynical today, means 51 or 52) patients relatively early in their disease course, trying to catch them 3-6 weeks before they would need the hospital; but with so few cases in April and May, how many of those 50 could possibly have made it to his 6 weeks post treatment yet to ensure they were out of the woods? The time course he lays out for concluding his treatment works and the time course he would have had to observe his patients’ response to his treatment just don’t line up.
But the saving grace for this post’s author on that point is that he could still get credit for most of the patients he treated this way up until about mid June, because the time course from first symptom onset to the rapid deterioration from Acute Respiratory Distress Syndrome in severe cases of COVID-19 is typically between 8 to 12 days. His time course of “starting treatment 3-6 weeks earlier” doesn’t make any sense, because the incubation period of the virus is 2-14 days and the time from symptom onset to clinical deterioration is typically 8-12 days or less; at the very most, a patient with a severe course of COVID-19 may have about 3.5 weeks from the time of their exposure to the point of requiring hospitalization, and that would be an extremely rare occurrence; most commonly it would be about 10 days to 2 weeks.
His citing a time frame of treating people 3-6 weeks before they would need hospitalization suggests one of two things. First, he could be comparing the start of symptoms to the time of death in patients that spent a number of weeks on the ventilator, claiming that hydroxychloroquine might have saved these individuals if they had been started on it 3-6 weeks sooner because he isn’t actually familiar with the hospital-based treatment protocols or clinical trials that used hydroxychloroquine, which certainly did not start the medication in the final days prior to the patient’s death, after they had already spent a couple of weeks in the ICU. Or second, he could be building a narrative that says COVID-19 really presents much earlier and can be detected by someone with special expertise or insight into the virus, which he happens to possess. The problem with this later one is that the incubation period means he reaches a firm time cap, the date of first exposure to the virus, long before he gets to his 3-6 weeks early; by claiming he is treating people 3-6 weeks before they would have been sick enough to need the hospital, he is essentially saying that he’s treating some people before they’ve even been exposed to the virus. If you just now thought, “wait, isn’t ‘treating people before they’ve even been exposed’ the same thing as treating people who are healthy and might not ever be exposed?”… Yes, yes it is.
“Fine, he has his time course a bit off; but his overall point is still valid, that maybe the medicine would work if it was started before the patient needed the hospital.” I think this is a common and very understandable stance, and there are so many different ways to approach it it’s hard to know where to start. We could point to the fact that not all hospital patients with COVID-19 who were treated with hydroxychloroquine had the same disease severity when they started the medication; if it were most useful early in the disease course, wouldn’t we have seen the less severe patients and those who were hospitalized earlier in their disease course derive greater benefit from it in all of the studies and the widespread clinical use it had a couple of months ago? Yet no such trends emerged to point us towards even earlier use of the medication. We could point out that it was doctors who started using hydroxychloroquine broadly in the first place based on some early anecdotal evidence and only stopped once more and better data was collected which unfortunately showed it wasn’t beneficial, which is exactly how science is supposed to work, and that both the idea of the president coming up with the treatment from his own research and the medical field abandoning it as soon as he endorsed it just to spite him are complete political fabrications. Here’s me and my friends texting again, this time on the same day President Trump mentioned hydroxychloroquine for the very first time.
We could also point to studies that have been done in exactly the clinical scenario in which this doctor is using his treatment plan- self-reported exposure to the virus- using hydroxychloroquine as post-exposure prophylaxis to prevent symptoms, which ultimately showed no benefit: as many patients became symptomatic and were hospitalized in the group taking the medication as in the group taking placebo. But as Dr. Myron S. Cohen, M.D. points out in an editorial about this study, medical research is not entirely free from popular opinion, and there are a great many ongoing trials still being conducted with hydroxychloroquine right now, many of which are focused on treatment very early in the disease course. (Edit: One was published in Annals of Internal Medicine the same day I published this article. It found that “Hydroxychloroquine did not substantially reduce symptom severity in outpatients with early, mild COVID-19“). If there is a use for it against COVID-19 at any point in the course of illness, we will hopefully know about it soon. But the doctor who wrote this post had no reliable data to suggest that his treatment would be effective; after looking at his own numbers, it’s pretty clear we still have no reliable data.

We talked about this last week when another Texas doctor claimed that inhaled Budesonide was a “silver bullet” against COVID-19 based on only a dozen patients. Right now we think the fatality rate of the virus is somewhere between 0.5% and 1.3%; still 5 to 13 times higher than a very deadly virus called Influenza, but not anywhere near the civilization ending numbers we had to work with before more widespread testing was available (I talk about these numbers more in this post). This means that if you took a random sample of 50 patients with confirmed COVID-19 and actually did absolutely nothing for them (which is not the same as offering anticipatory guidance, providing symptomatic support, carefully discussing emergency room precautions and red flag signs and symptoms, and talking through and arranging follow-up care) and 50 of them were alive a few weeks later, you would be thankful but you certainly wouldn’t be shocked. If you had 100 patients with the virus and they all lived and none ended up intubated in the ICU, you might call that God’s grace or good luck (or both, depending on your theological leanings), and you’d probably look at the demographics and risk factors of the patients, but you wouldn’t assume that the doctor had done anything extraordinary. Looking at this doctor’s sample of 50 or so patients, the one thing we can definitively say is that these statistics are not amazing. Any number of doctors around the country treating COVID-19 appropriately without unproven medications dosed with a heavy mix of conspiracy theories could give you a similar case series and claim that their particular brand of talking with patients had a “100% success rate.”
It is a little interesting, though hardly amazing, that none of his patients required hospital level care at all, and is enough to want to know more about his subset of patients. But it is exactly here that this doctor first tips his hand a little bit, by giving the details of just one of his patients. He states that he treated a patient who had been discharged from the hospital after 4 days of treatment but still ‘felt terrible’ (as people tend to do when they are ill, and also when they’ve just spent 4 days in the hospital. Heck, I feel awful after 4 days in the hospital as a doctor, much less as a patient). He treated this patient with his unproven drug regimen as well, and includes them as an example of just how effective it is. But please bear in mind that this patient had not been refused admission or callously sent home to die; they had already been treated in the hospital during the worst period of their illness, and deemed healthy enough to continue to recover at home by their hospital doctors. To include this patient not just in your data set but as an example of how effective your therapy is at preventing the illness from worsening is proof in itself that your understanding of how this virus operates is not based on reality and the experiences and insights of your peers who have more experience with it, but on narratives that you have built for yourself because you happen to find them useful. We already suspected this doctor was treating patients before they were exposed to the virus; now we know he is treating them after they were already far along in their recovery as well.

The doctor doesn’t stop there, but he goes on to give a list of other measures he doesn’t agree with, and we need to spend some time here, because this is where we really come to understand his treatment philosophy.
He states that he doesn’t believe in contact tracing, calling it ‘communism’ and stating that he ‘cannot even get the Public Health Dept. on the phone’. This is a bit like saying ‘you can’t fire me, I quite!’ and then asking about your severance package; if he really believes contact tracing is communism, one would wonder why he was calling the Public Health Dept. about contact tracing in the first place. I also don’t understand how contact tracing could possibly be communism, but clearly this is a secondary issue at best.
He also doesn’t believe in quarantine, which while undoubtedly difficult on a broad-scale (other countries have found ways to help their effected citizens deal with quarantine and isolation with adequate social and emotional support measures) is also common sense epidemiology, and in wearing masks, which have plenty of solid evidence (which has only increased since I wrote that blog post). He doesn’t believe in social distancing (I don’t understand what he’s talking about in the parenthesis, but I think it’s about the economy), and he even says he doesn’t believe in testing, citing an insanely inaccurate false negative rate that is only possible, even for the very worst tests, once COVID-19 is at 55%-65% prevalence in the population you are testing; a number we have not seen anywhere in the world at any point during this pandemic. For reference, the highest his county has reached at any point has been a test positivity rate of 16.89%, just 2 days ago. This would give the two tests I use a false negative rate of 4% and 1.3% respectively.
This is really a whole separate set of claims. He is claiming that the methods used by every single country that has seen success in protecting their citizens from the virus don’t work, while an unproven and incredibly politicized medication regimen used by him and one other doctor in a nearby city is the miracle cure. One might advise a more humble approach, claiming that while these strategies might work (as the evidence clearly demonstrates they do), they would be rendered unnecessary by his treatment strategy; but he boldly claims both, even to the point of saying that other doctors not using his treatment regimen has lead to 100,000 deaths. If he is wrong about the latter and is widely believed, the virus will spread more quickly; if he is wrong about the former, those who are exposed as a result will be without the miracle cure they were promised.
What if he were lying?
Here’s the cynical part, and the part I find hardest; what if this misinformation, rather than the honest misunderstanding of a doctor with very limited experience with the virus, were a deliberate and calculated deception in order to make money, as so many other doctors have been accused of? Would this, unlike advising social distancing at the expensive of your own clinic’s bottom line or cancelling lucrative elective surgical cases, be an effective financial strategy?
Let’s review. In this post, this doctor:
Advises against wearing masks, social distancing, and quarantine. If he’s lying, this would increase the number of COVID-19 cases during a time of otherwise decreased medical visits, thus creating more sickness and more patient visits in general.
States he doesn’t believe in testing. This eliminates a natural barrier to receiving ‘targeted’ treatment, because it places the diagnostic decision making entirely in the subjective realm, all based on phony statistics about the COVID-19 tests. This means that a number of his patients will receive treatment without even having the virus in the first place, which will inflate his “amazing” treatment statistics. This is great, because he also states that he…
Claims he is treating 3-6 weeks earlier than other doctors. This means he is relying on some unique way of diagnosing the illness that is entirely original to him, that would lead to a diagnosis weeks before a patient would end up in the hospital; in other words, it won’t even matter if you have recognized symptoms of or exposures to COVID-19, he is able to diagnose you well ahead of any normal doctor. Combined with a promise that he won’t rely on test results for the virus, this is tantamount to a promise of specific medications for treatment ahead of time, which is an advertising tactic, not conscientious evidence-based medical practice. It would be like promising antibiotics for your child’s ear infection whether they need it or not, and then claiming that your child would have had an ear infection and that most doctors don’t treat as early as he does because they just don’t know the very early signs, like being fussy, tugging at their ears, and wanting to watch Moana over and over again (hey wait! My toddler does have all of those symptoms!).
Promises “completely safe and incredibly effective” treatment without any credible scientific evidence of its effectiveness. This reinforces his criticism of masks, social distancing, and quarantine for his patients specifically (who wouldn’t need them anyway, since they are now ‘healed’), which increases subsequent cases in their families and friends; the very people his patients are likely to refer to him by word of mouth.
Shares his post on social media. This spreads the word, especially once it goes viral, and not only increases cases as people believe it and use it to justify forgoing mitigation and transmission control measures, but also drives people to his clinic from all over the state and region because he…
Shares his name and says to contact him. Having now promised treatment for a virus that his post is likely to cause more cases of, he now ensures that he will have a higher percentage of the market share of both these new COVID-19 cases and people who don’t have COVID-19 but are seeking pharmaceutical treatment out of fear due to the increasing surge; a surge his post is at the very least contributing to.
In summation, this post is saying don’t do any of the these inconvenient things doctors around the world say will help keep you and your family safe from the virus; just come see me in my clinic and I will diagnose you with COVID-19 whether you have classic symptoms or not, whether you test positive for it or not, and without fail prescribe you these medications that you can’t get from most other doctors.
You don’t need five years of medical school to understand why this should make you cautious.
I have to admit, that felt really dirty. I’ll say it one last time; I actually think this doctor, like so many of those I’ve argued with from a distance on this blog, really believes his post. He has gotten his stats wrong, relied on old and incomplete data on masks, misunderstood what other countries have done to fight the virus, confused contact tracing with communism (ok that one is new), leaned on anecdotal evidence, and I believe in general approached the subject with enough bias and preconceived ideas and little enough actual exposure to the virus that he never had a chance of reaching a different conclusion. In fact, his very limited clinical experiences with ‘treating’ the virus are almost perfectly calculated to provide him the confirmation bias he needs to firmly cement the truth of all of his claims in his mind, and that will only get worse as more patients come to him “early” in their disease course and experience a full recovery, whether they ever had the virus in the first place or not.
I do think this doctor can be wrong, and yes, do damage, without it being nefarious. But it’s clear from social media that there are some people, perhaps many people, who are not comfortable with the majority of physicians drawing one conclusion while a small minority draw the opposite conclusion unless one of those groups is lying. If that’s you, please consider which doctors have the greater financial motivation to build a false narrative- and stand to actually gain from the narrative they are building- and which are willing to tell the truth to keep you safe even if it potentially hurts them financially. That’s already one of the most obvious ethical principals we nevertheless have reinforced for us repeatedly throughout medical school and residency and a decision that a great many of us got used to making years ago anyway, and the idea of a doctor telling his patients “please stay home and stay safe” as he wonders how he’s going to pay the rent on his clinic building is far easier for me to imagine than any of the critical care doctors I’ve met in the last 13 years intubating a patient that they thought didn’t really need to be on a ventilator, much less because it was going to make them some extra money.