As the pandemic has escalated over the past several months and almost all of us who had been previously unaffected have now had friends, family members, or other people we care deeply about either pass away or at least become very, very ill from the virus, I’ve noticed a trend in the misinformation that we accept, share, and believe. The nature of a global pandemic is that it robs us of our delusions, and we are now many months out from being able to believe what was commonly said in March and April, that the pandemic is not coming, and that even if it does come it is not deadly. The landscape has shifted, and until more conspiracy theories crop up about vaccines or possible outpatient treatments in the coming weeks and months, the misinformation has settled back into the realm where it is most resilient; into the question of motives. It doesn’t matter what actually happens with medications, vaccines, case numbers, and death rates; believing that the people trying to help you are actually trying to control you is always fair game.
In about a week we are going to see the merger of COVID-19 misinformation and the ever-popular “War on Christmas” conspiracy which annually reminds us that dark forces are at work in the world to destroy my favorite holiday and everything it stands for. But until then, Thanksgiving is the target apparent of the powers that be.
Full disclosure, I’ve waged a small private war against Thanksgiving for years, and it has nothing to do with how many people are gathered. My concern is with the way we celebrate and especially teach children about the history of Thanksgiving and the way we sterilize the history of Native America-European settler relations. I also have some concerns, as the doctor to many patients with diabetes and CHF, about the lack of nuance in our culture’s understanding of feasting, and typically resolve this by telling my patients not to check their fasting blood sugar on Black Friday (unless they take correction dose sliding-scale insulin, of course). For me, it’s the most hypocritical holiday of all, because while I caution moderation to my patients I know I will probably fail to practice it myself. Because you see, despite all of my concerns about Thanksgiving as a holiday, I also love turkey and dressing, pumpkin pie, and most importantly (as any true Southerner will tell you) green bean casserole, macaroni and cheese, mashed potatoes and brown gravy (I’ll lose readers over that), and a sweet potato and marshmallow dessert we have hilariously convinced ourselves is a side dish instead of a hedonistic excess and probable harbinger of the end times.
(I also like seeing my family and stuff.)
So the togetherness and joy of the thanksgiving holiday is something I’m loath to give up for any reason, and I would be lying if I told you that I knew all along that we would opt for a small family Thanksgiving day in our own home, or that I immediately made that decision after reviewing the trends in COVID-19 numbers or even after reading Dr. Emily Smith’s excellent, excellent review of the relevant epidemiology facts. We earnestly struggled with it. And as we weighed the medical risks of our extended family members against my daily interaction to COVID-19 positive patients and my wife’s recent exposure to the virus, I could taste the potato casserole fading from my future as we made the difficult call and informed very disappointed (but understanding and supportive) family.

And I’ve been counseling my patients to do likewise, just like many physicians, epidemiologists, and other health scientists around the country. And despite the suspicion and mistrust that a doctoral degree elicits these days, it has nothing to do with wanting to control my patients lives, training them for future subservience to the government, my crusade against the idea that our relationship with Native Americans was ever truly mutually respectful and supportive, or even the principle that misery loves company and if I don’t get to eat my grandma’s turkey dressing recipe on Thursday they shouldn’t either.
Instead, it’s because we are living today in the most dangerous window of the pandemic so far, and because there are characteristics of Holidays in general, and Thanksgiving in particular, that makes this week an incredibly dangerous one for our country.
3 Reasons that Thanksgiving is Dangerous.
1. Certain holidays are more dangerous than others.
Even allowing for difference of culture and family tradition, the innate characteristics of certain holidays make them more or less dangerous in terms of transmission of a respiratory virus. January 2nd, World Introvert Day, will probably be just fine; but the indoor concert you are planning for National Kazoo Day three weeks later on January 28th should be cancelled because that is a lot of aerosolized spittle in an enclosed space (it should be cancelled anyway regardless of COVID-19, but that’s not my point).
If we are going to discuss the characteristics of Thanksgiving, it would help to compare it to another widely celebrated holiday we’ve experienced during COVID-19, the 4th of July. As a reminder, here is a look at the numbers.

California 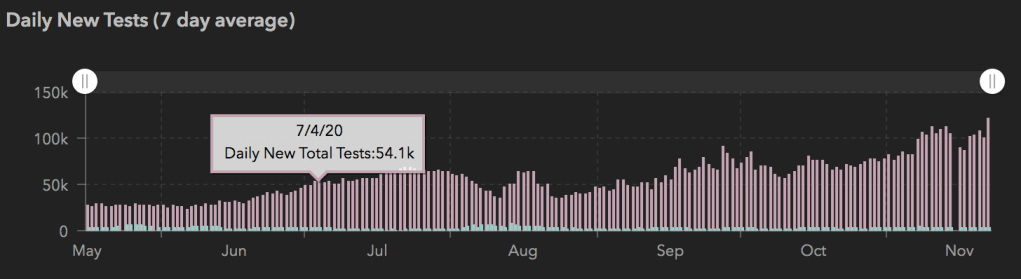
Texas 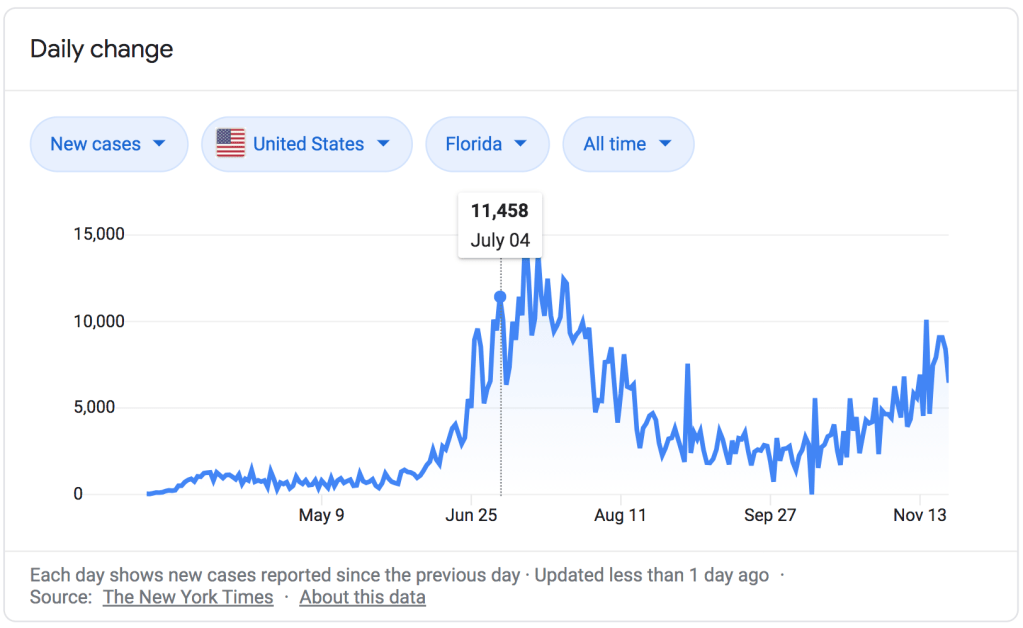
Florida 
USA
The two weeks after the 4th of July saw the largest spike in cases of COVID-19 we’ve experienced during the entire pandemic (except for the one we are in now). There’s a strong enough case to be made that the trajectory of that wave was already increasing prior to the holiday; but the public gatherings, parties, and beach trips dramatically contributed to the rise in cases, heightened the severity of that late-July peak, and appreciably altered the curve for the worse in places like Florida and California. In a moment we’ll compare some of the characteristics of these holidays, but that’s really splitting hairs; the biggest reason that Thanksgiving is dangerous is because COVID-19 transmission follows the principles of exponential growth; the more cases you start with going into a time of decreased caution like a holiday, the greater the impact it will have on the curve. We are already close to or above capacity in many hospitals around the country; even another 4th of July, with the numbers we have right now, would absolutely drown us. And there’s plenty of reasons innate to the holiday that make Thanksgiving much, much worse.
It’s true that the 4th of July has some characteristics that could make it more likely to result in spread of COVID-19 than Thanksgiving; mainly that it involved very large events that brought together people from very different spheres of contact. A few cases of COVID-19 could spread easily to multiple social circles and families from one big 4th of July party. But Thanksgiving has some characteristics that make it more dangerous too. First, unlike the 4th of July, most people celebrate Thanksgiving indoors; transmission is more likely indoors than outdoors, all things being equal. Second, contact tends to be prolonged; you aren’t just passing various people for a moment on the way to the beach or grabbing a beer, you are sitting face-to-face for hours while eating and visiting and (unless you are a good-for-nothing-in-the-kitchen family freeloader like me) cooking. If a contact at a 4th of July party has COVID-19, you may or may not have been exposed. If someone at Thanksgiving Dinner has COVID-19, everyone there is definitely an exposed close contact.

Third, that issue of bringing people together from different spheres of contact is true for Thanksgiving just as much as for the 4th of July. Traveling for the holiday is one of the major things that public health experts are warning against, and even if you aren’t flying or driving across state lines, not everyone’s social circles really overlap much with their cousins’ or grandparents’. One family member who has had an exposure or hasn’t taken precautions in the weeks leading up to Thanksgiving runs the risk of infecting their entire family, and those family members bring their exposure back to the other members of their community. Finally, Thanksgiving brings people together who are not likely to socially distance from one another. It’s all well and good to say ‘we will eat outside and stay 6 feet apart’, but how many times has that actually happened when getting together with family you have been longing to see? There will be hugs, there will be boardgames, there will be long heartfelt conversations- or yelling matches about politics. Not to mention the decision of whether or not to finish off somebody else’s half eaten piece of pumpkin pie if nobody is looking, which is a difficult enough choice even under normal circumstances.
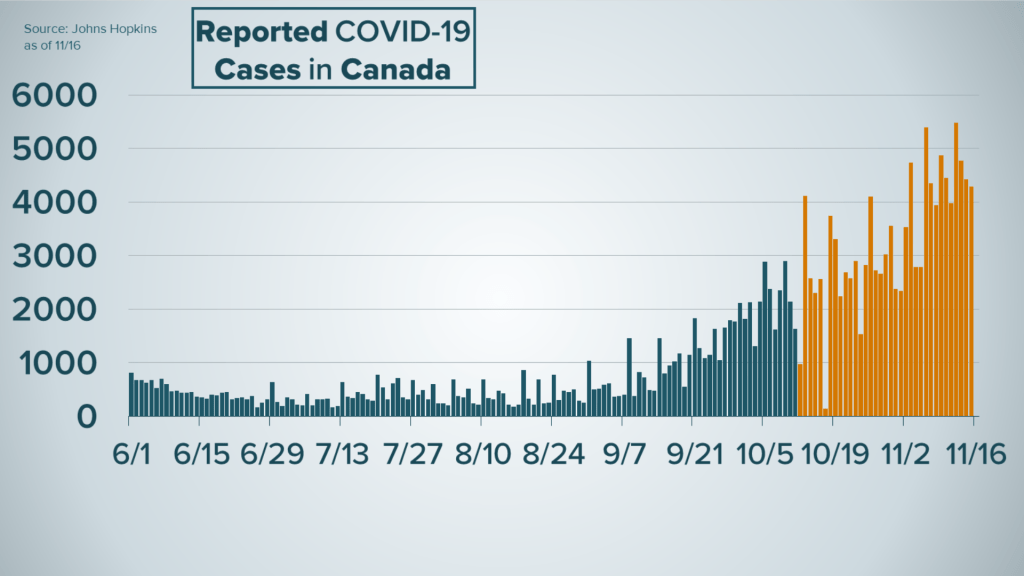
But we don’t have to just take my word for it or guess whether Thanksgiving will be as bad (or worse) as the 4th of July, because Canada has a Thanksgiving too, which they hold (ridiculously) on October 8th.
The Canadian numbers show a miniature warning of exactly what we would expect after a national holiday during a national uptick in cases; a steepening of the curve and a much larger number of new cases over the next month. The difference is that Canada has nowhere near the number of active cases or the amount of community transmission that we have; our increase is going to be much, much more dramatic.
2. Holidays bring together those who are at greatest risk with those who spread the virus best.
We talked about the total lack of social distancing between relatives when they finally get together, and nobody is better at not socially distancing than children. If you think about the emotional value we all place on the holidays, probably one of the first images that comes to mind is the sight of your children running to their grandparents and covering them in hugs and kisses. It’s honestly one of my favorite moments each and every time it happens. It’s also a very, very dangerous situation if there’s any possibility those children have COVID-19. Children spread COVID-19 very easily; some studies have shown that children spread it even longer and more efficiently than even the sickest ICU patients. They spread it even when asymptomatic, and are asymptomatic at a higher rate than adults. They are also in school, and schools are full of other small gross people that spread COVID-19 efficiently, and those schools will not be closed for the holidays for any significant period of time prior to Thanksgiving.
And who are they hugging on? Almost certainly the people in your family who are at the highest risk if they do get exposed. We have been discussing the risk factors for severe COVID-19 infection, COVID-19 pneumonia and respiratory distress syndrome, and death on this blog since April and a lot of those factors haven’t changed; age, chronic lung disease, diabetes, heart disease, other chronic medical problems. But age is the first one, and the risk of someone dying from COVID-19 increases dramatically after age 50.

By bringing together the people in your family most likely to have been exposed to COVID-19 over the past few weeks (because of school) and most likely to spread it even when asymptomatic, and the people most likely to get seriously ill if they are indeed exposed to COVID-19, holiday gatherings with extended family really do present a dangerous situation for the most vulnerable members of our families.
I’ve had patients ask my advice on what to do about visiting grandparents and great-grandparents for Thanksgiving over the past few weeks. I hear their anguish, their indecision, their desire to celebrate with family fighting against their fear of spreading the virus to someone they love, and the deeper fear and guilt that they are making the wrong decision by choosing to miss out on those beautiful moments together. My recommendation? If you think that, barring some tragedy, the person you love has some good years of holiday celebrations left, it seems wise to sacrifice this one in order to safeguard all of the others. This pandemic won’t last forever.


3. It isn’t just COVID.
I’ve been reflecting on my very first efforts at writing about COVID-19 back in March, before I even started this blog. At that time the US had 23,604 deaths from COVID-19 and healthcare workers and public health experts were urging caution, which people were generally willing to follow… for a little while. Today it is 260,000 and instead of seeing this as validation of the concern we have had since March about how bad this virus can be, many people have long since thrown caution to the wind for really no other reason than that we are all incredibly, unbelievably fatigued. I’ll write about that sometime soon; but what I’ve really been thinking about from those first posts is these two short paragraphs, which are just as true today as they were then.


Guess what? We are there.

As I’ve said before, most people don’t understand what an overwhelmed healthcare system looks like because we’ve never experienced it. It means not having access to doctors and nurses when you are in DKA or have a skull fracture. It means your kid can’t get treatment for his seizures or his infected spider bite. It means that every single medical condition is more dangerous (many are more dangerous during the holidays anyway) because medical professionals don’t have the time, the mental energy, the tools and equipment, or even the staffing to deal with them properly. It means not being able to get an ambulance to get you to the hospital or a bed when you get there. At a time when tent hospitals are being put up around the country, we need to decrease COVID-19 transmission right now to prevent permanent injury and death from everything from high-risk pregnancy to Congestive Heart Failure to snow-skiing accidents.
And of course, as we saw in New York, an overwhelmed healthcare system makes the virus itself incredibly more dangerous as well. “I can always go to the hospital if I have a bad case” has never been a good argument against exercising caution; but it is simply not true if you can’t go to the hospital or if they can’t take care of you well once you get there. The death rate has held more or less steady since it started to decline because of our increased understanding of how to fight the virus with targeted, COVID-19 specific ventilator techniques and successful use of medicines like dexamethasone for hospitalized patients. But the biggest factor that will cause it to go up again is doctors who are too tired to think and nurses who are too busy and fatigued to catch their mistakes.
But how can I celebrate Thanksgiving with family safely?
I never want to be accused of being an alarmist, and if we are talking about reliable epidemiology principles and the solid medical realities of how the virus is transmitted, I would say of course there are safe ways to do Thanksgiving together. In theory. We could talk about things like only meeting outside, everyone distancing from people not in their immediate family, no sick people at all being allowed, and everyone strictly quarantining for a full 14 days prior to the Holiday. The problem is, those are things that are hard for anyone to do, let-alone a large group of people, and the chances that every member of your family can or will strictly adhere to those guidelines is very low; and it gets lower with every person you add. If people are working anywhere other than home, or they are traveling at all prior to the holiday, or if you’ve got just one family member that believes the pandemic is a government sponsored hoax meant to force you to wear a mask and will therefore gleefully shirk every precaution the family has agreed upon when the time comes, your gathering has gone from perfectly safe to not perfectly safe; and not perfectly safe is, in aggregate, really really dangerous right now.

Or let me put it another way. I’ve seen more patients with COVID-19 than any doctor in my clinic system; maybe more than any doctor in town, though there are those whose exposure risk I would rate as being higher than mine (our pulmonologists and ICU docs, for example, or the young medical residents who are seeing patients with COVID-19 in both the outpatient and inpatient setting and the ICU… and of course our nurses, who typically have more time face-to-face with our patients in the hospital, and in clinic perform procedures like nasopharyngeal swabs that are higher risk for aerosolizing respiratory droplets). I’ve been tested for COVID-19 12 times; half because of symptoms and half because of our internal exposure protocols. I’ve been negative 12 times; my 13th test is tomorrow (and if it’s positive I’m coming back to delete this paragraph). I would never disparage the degree of caution that has been taken by my medical brothers and sisters who have contracted COVID-19 in the line of duty, or imply that I’ve done anything they haven’t; but I’ve been seeing COVID-19 positive patients almost daily since April and have utterly failed to contract the virus. My PPE game is strong. I’m really, really good at being cognizant of fomites and at personal transmission control. I’m confident that if I can design and implement clinic protocols that protect patients and staff 40 hours a week, I could do the same for a 3 hour meal… But I’m staying home for Thanksgiving.
Why? Because it isn’t worth the risk. Because the virus is very, very real and I really care about my relatives and neighbors. I’m not afraid of COVID-19, and I’m not letting it control my life. I’ve heard all of that hyperbolic nonsense and rejected it; prudent action on behalf of those you love is not “living in fear,” and giving up one meal with extended family for one year is not letting it “control your life.” I’ve also heard the rejoinder, “but where do we draw the line?” Somewhere else, obviously. And even though I’ll probably be back here in three weeks encouraging you to have a small family Christmas this year, if you want the best possible chance at a safe Christmas with extended family (after strictly quarantining for 2 weeks and carefully laying out ground rules for everyone attending, and not flying to get there…), the best thing we can do is take wise, collective action to stem the tide now. Turkey and dressing will taste just as good in May or June.