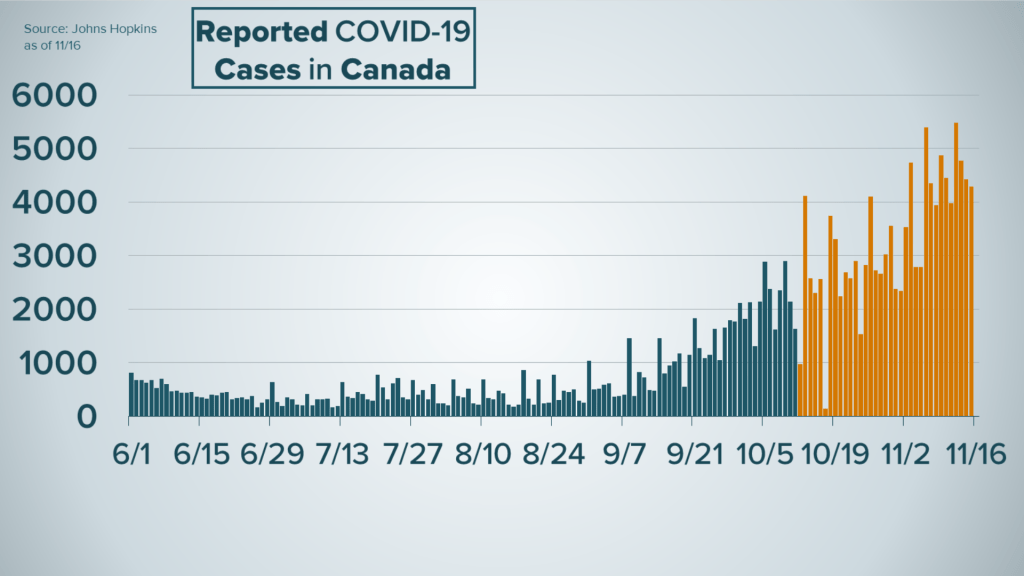
The Barnstable County outbreak in July is a great example of how effective the COVID-19 vaccines are. They show us what an outbreak of the Delta variant of COVID-19 looks like in a highly vaccinated population.
Barnstable is a county of 213,000 people in the 2nd most densely populated state in the country. It is a popular tourist location, especially during the Summer. It just suffered an outbreak triggered by a super-spreader event. This resulted in only about 500 cases of COVID-19 (in residents; we don’t have data, including vaccination data, on the other half who were from out-of-state), 5 hospitalizations, and 0 deaths. About 79% of the population is fully vaccinated, with many more partially vaccinated. The various disinformation purveyors cite the fact that 74% of those who got COVID-19 during this outbreak were vaccinated as a shocking counterpoint to literally all of the data pouring in from all over the country, as though it proves that the vaccines don’t work… When really, it is exactly what we should expect even if they do work. It’s a bit like saying “the people who lived there are the ones who got it while living there”; unvaccinated Texas and Floridians couldn’t have gotten COVID-19 from the outbreak in Barnstable County Massachusetts; they weren’t there. We know many people who were just visiting did get COVID-19 during the outbreak, we just don’t have information on their vaccination rates because they went back home and added to their county’s COVID-19 statistics after the event; they aren’t included in Barnstable’s.
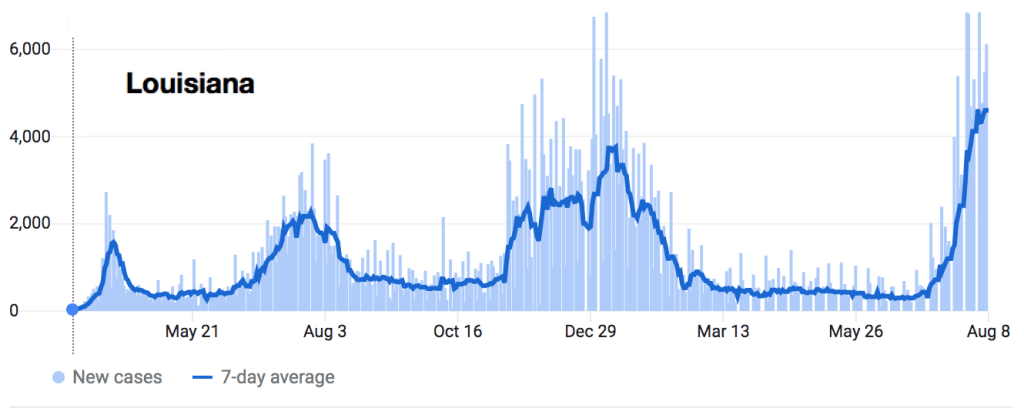
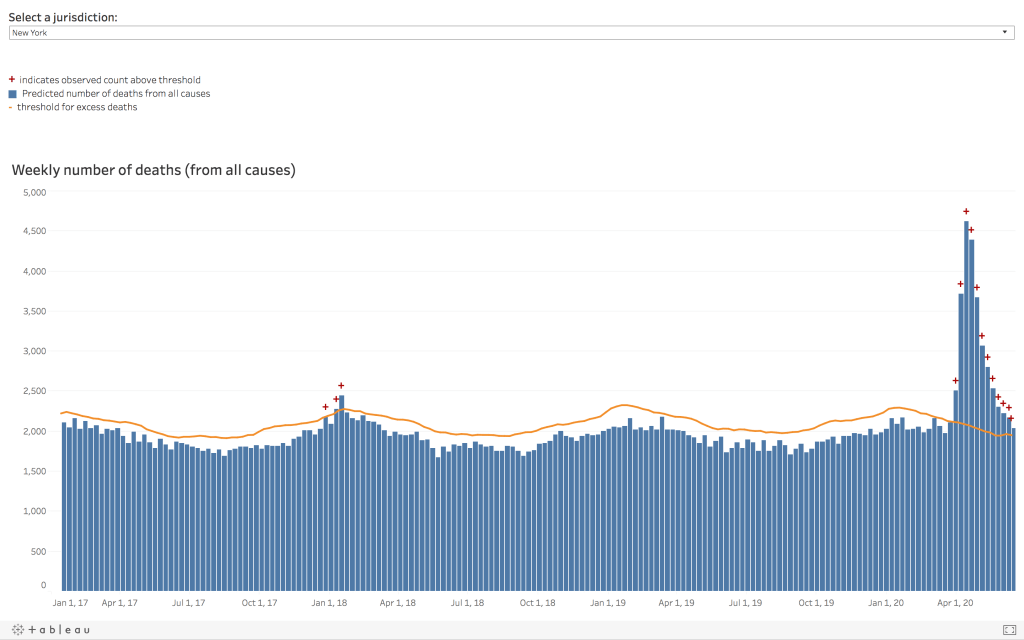
This is what COVID-19 hospitalizations look like all over the country in areas with low vaccination rates.
The misinformation would have you believe that 5 hospitalizations in Cape Cod are more statistically meaningful than 1,003 hospitalizations in Baton Rouge.
All of the evidence we have from the other 3,005 counties (and 64 Parishes) in the US strongly suggests that if Barnstable had had this outbreak with, say, a 36% vaccination rate like we have here, this would not be a mere 500 person outbreak with just 5 hospitalizations and 𝐳𝐞𝐫𝐨 deaths. Less densely populated counties without super-spreader events are seeing worse numbers than these every day, and their hospitals and ICU’s are filling up rapidly as patients continue to die. To put it another way, when I worked as a full-time hospitalist in a small town I considered it a “light day” when I personally had 8 or 9 patients to care for by myself; I felt busy once that number was above 14 or 15 (and some hospitalists routinely see 18 or more). The entire Barnstable outbreak resulted in a burden on their hospital system that required 1/3 of the time and effort of 1 doctor each day. And they all lived.
By the way, Barnstable is doing fine now; they really did have a contained, limited surge and now cases are falling again. Barnstable County, Massachusetts is not on fire.
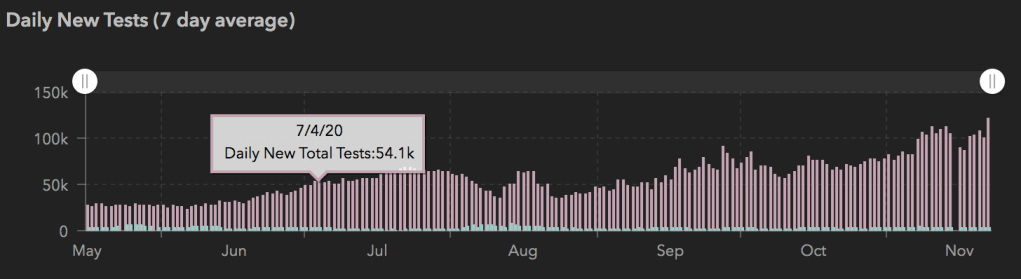
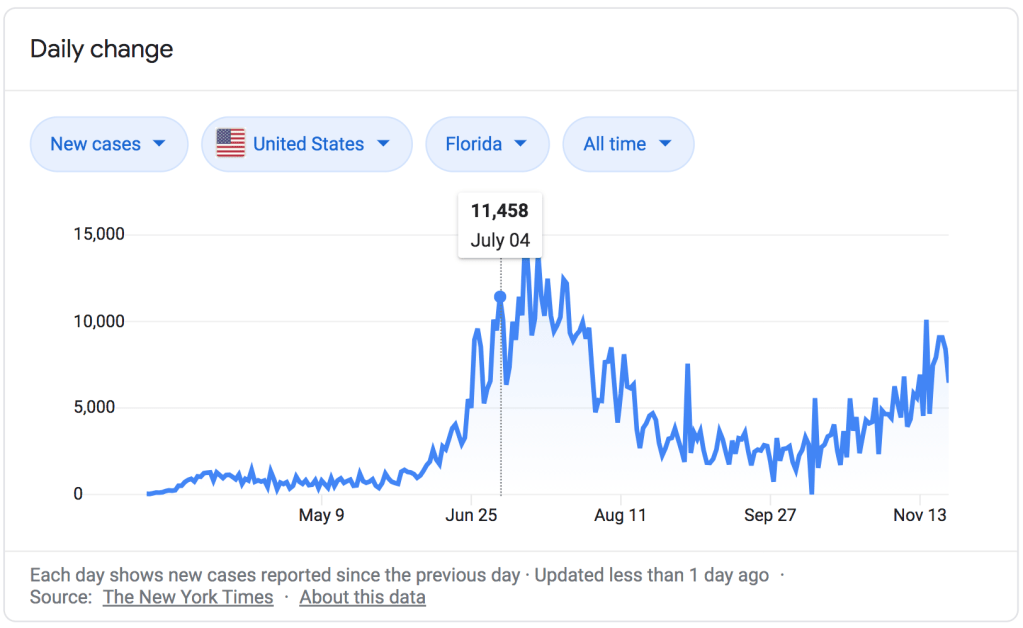
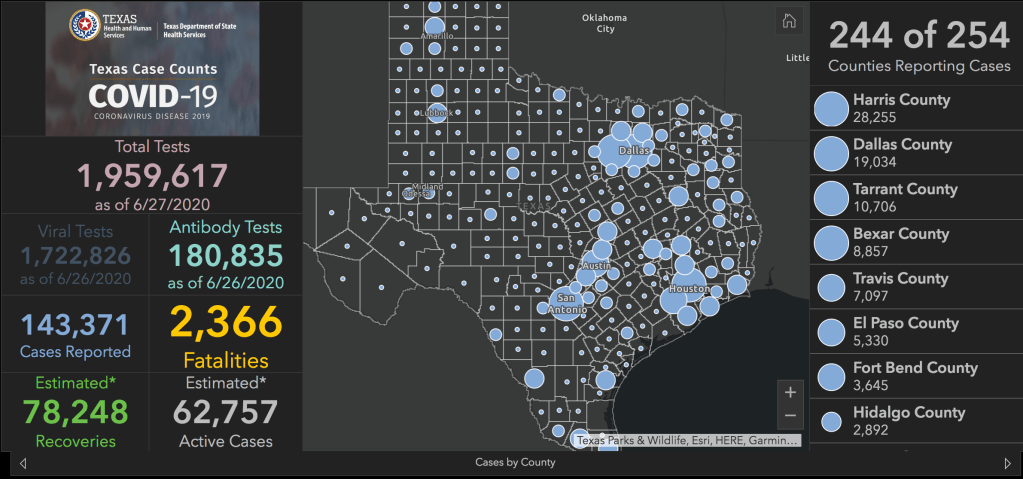
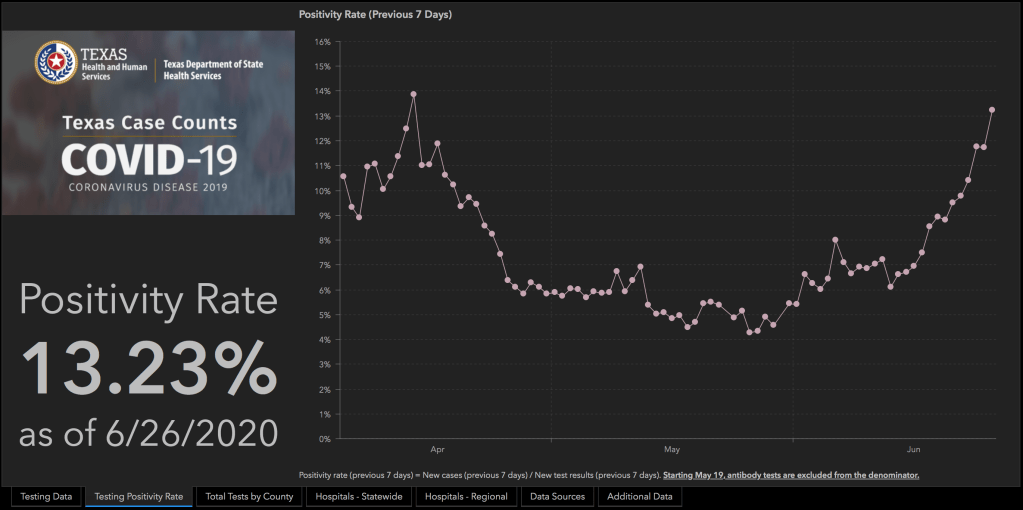
My home state of Louisiana is. Texas will be soon (parts of it already are). We both have vaccinations rates that are about half of Barnstable County. That’s the difference in our case trends.
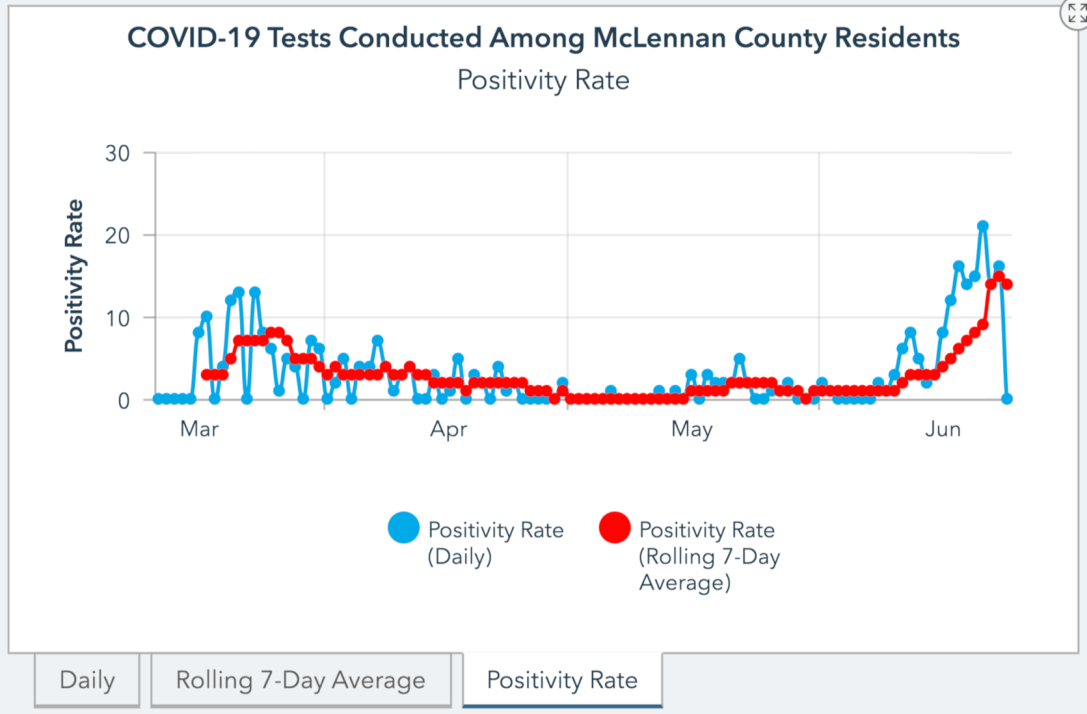
This is what might have been. This is what Texas could be experiencing right now if we had a higher vaccination rate: a minor surge, entirely within our capacity to handle, and quickly contained and improving. Instead hospitals all over the state are cancelling elective surgeries and operating beyond surge capacity, and the ER, hospital, and ICU doctors and nurses are so overwhelmed with COVID-19 that other patients can’t get access even when they are very ill or injured.
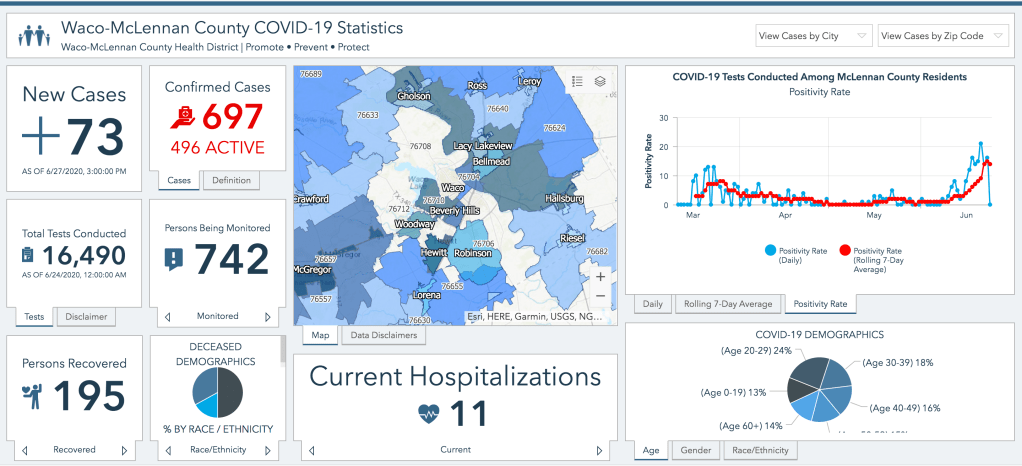
I live in a similarly sized county to Barnstable with half the population density, excellent local leadership, and no recent super-spreader events; yet we have 866 active cases, 173 new cases from just Friday (I diagnosed some of those personally), and over 100 hospitalizations. Most of those cases- and almost all of those hospitalizations- are unvaccinated patients. Our numbers just leave Barnstable county standing- because we have such a low vaccination rate. And we aren’t even calling it an outbreak; this is just what the COVID-19 Delta variant looks like anywhere without adequate vaccination rates to prevent widespread transmission.
McLennan County, Texas(This Week)
Population: 256,623
Population Density: 227 People/Sq. Mile
Current Active Cases: 866
Current COVID-19 Hospitalizations: 106
Barnstable County, Massachusetts (July Outbreak)
Population: 212,990
Population Density: 562 People/Sq. Mile
Total Cases in July: 560
Total Covid-19 Hospitalizations in July: 5
Vaccines don’t put a forcefield around us that keep us from coming in contact with the virus; they prime our immune system to fight the virus effectively when we do come into contact with it by teaching us how to build antibodies and a targeted immune response. No vaccine can keep every person from becoming symptomatic when they are exposed to COVID-19. But they do substantially reduce infections and thus transmission, and most importantly they greatly reduce the risk of severe illness and death; that has been their purpose since they were invented in the late 1700’s, and that was the purpose of vaccination’s predecessor, inoculation, which we inherited (one could argue, stole) from African, Indian, and Asian traditional healing practices.
Right now, hospitals all over the country are drowning in almost entirely unvaccinated COVID-19 cases that are absolutely overwhelming our medical infrastructure, and many of those patients are dying tragically- as are those who don’t have COVID-19 but can’t get medical access because the healthcare system is stretched so thin. They didn’t have to die. The Barnstable outbreak is indeed a warning about just how contagious the Delta variant really is- and how even vaccinated people need to continue exercising caution and wearing masks. But it also shows us how much better off we would be right now as a nation if all of our counties- and parishes- had vaccinated at the rate of Massachusetts.
The vaccines are incredibly safe and super effective; please go out and get one.
My web designer, who also designed and sells this shirt over at his site justacovelldesign.com, assures me that the vaccine can’t be “super effective” because “technically that describes a move and how effective it is against a certain type Pokémon rather than an item.” So the “It’s Super Effective” sticker I added “doesn’t make any sense.”
Intro: Talking about vaccines as a Family Medicine doctor
As a Family Medicine Physician, helping patients navigate uncertainty and doubt around vaccines has been a part of my day-to-day job since long before the COVID-19 pandemic. I have always tried to approach those conversations with patience and understanding (not that I’ve succeeded each and every time), knowing that behind their questions and even suspicion there is, without exception, a deep desire to do what is best and safest for themselves and their families. I get it; vaccines can feel scary. They are pretty mysterious for most people, and there is so much controversy over them that our intuition tells us surely some of it must be true (even though the people who creating it are often intentionally deceitful). I am a father of 4 myself and understand how strange and frightening it can feel to have your child undergo any medical procedure; but unlike an infusion of antibiotics or a dose of tylenol, or the sedated lumbar spine MRI my daughter needed for tethered cord syndrome when she was 1 year old, vaccines are given to children who are healthy to prevent future illness; it makes the decision harder, because the reason for the treatment isn’t readily apparent or at the forefront of our minds.
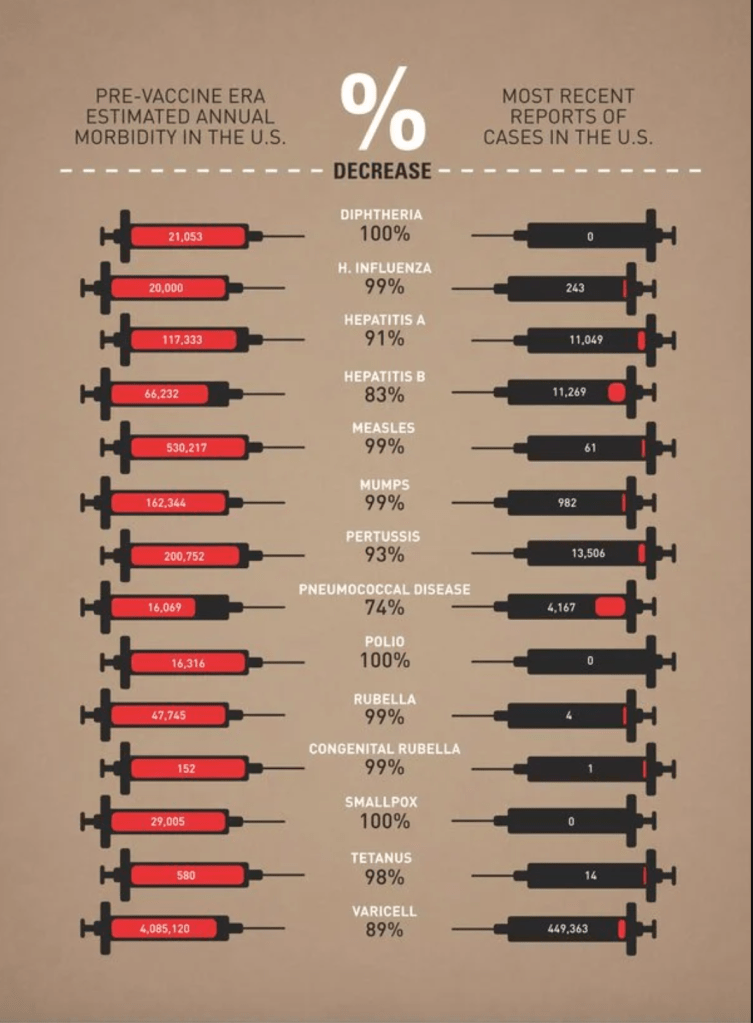
Vaccines are also one of the single most important innovations of modern medicine, and have saved millions of adults and children from dying of some of the worst and most painful infectious diseases that afflict humanity.
That’s why it’s incredibly important to me that my patients have the time to ask their questions and why I believe they deserve careful, sincere, and thorough explanations. So when I think about all of the medical misinformation that is out there right now around the COVID-19 vaccines and how we can possibly alleviate those fears, I start by imagining a patient sitting across from me in my clinic exam room with doubts, uncertainty, or even trepidation about these new and rapidly developed vaccines, and try to write out how I would try to answer their questions.
𝐇𝐨𝐰 𝐝𝐨 𝐭𝐡𝐞𝐬𝐞 𝐯𝐚𝐜𝐜𝐢𝐧𝐞𝐬 𝐰𝐨𝐫𝐤?
Updated 12/24/2020
When discussing vaccines with my patients, I always, always start with a brief discussion of how they work. It’s not uncommon to hear someone say “I think it’s better to rely on my own immune system” when discussing vaccine preventable illnesses. We’ll talk about this in more detail later on, but my first response is usually to help my patients understand that that is exactly how vaccines work; by relying on your own immune system.
Our immune system is designed with two strategies for fighting infections. The first is non-specific but immediate; in addition to our innate protective barriers like skin, hair, and mucous, we have cells like macrophages, mast cells, and natural killer cells that are able to detect and attack any foreign invader that the body recognizes as not being part of itself. This is a good system and prevents you from getting sick all the time; without it, we would be constantly fighting illness and infection from normal everyday exposures, just as many do who have compromised immune systems.
But even more powerful is our adaptive immunity, which is directed specifically against infections our body recognizes and has dealt with before. This is an incredibly robust system of B and T lymphocytes and antibodies that recognize the invading pathogens and kill them with a higher degree of efficiency and precision. The only problem with it is that it takes time to kick into gear the first time your body is exposed to a new infection; and then it’s a race to see whether it can become active enough, fast enough to prevent an illness from becoming severe. On subsequent exposures, that response is much, much more rapid; so much so that you usually don’t even know you’ve been re-infected with that bacteria or virus because you don’t get sick.
The principle behind vaccines is simple; what if we could safely teach the adaptive (specific) immune system to recognize the deadliest infectious diseases, so when someone is exposed the first time they can mount that powerful, targeted immune response right away and not even get sick?
And that’s exactly what these COVID-19 vaccines are designed to do, just like all of the vaccines before them; they give the body the information it needs to mount a robust immune response with the adaptive immune system as well as the innate immune system, without any possibility of causing an infection in the process. So when someone asks, “wouldn’t it be better to rely on our own immune system?” my answer is, “Yes, absolutely! And vaccines allow us to rely on our entire immune system, not just the weaker half, without even getting sick.”
We will talk about the differences between how traditional vaccines and the mRNA vaccines accomplish this later (and whether or not they re-write your DNA). For now I’ll just say that the new vaccines are even closer to naturally acquired immunity than traditional vaccines, because they trigger our immune system almost exactly like the viruses themselves do.
Will the vaccines have any lasting effect on my body?
Updated 12/26/2020
Hopefully! That’s sort of the idea. While the messenger RNA only survives for a few minutes before degrading, the antibodies that are produced will circulate for months, and some of the other cells of the adaptive immune system, specifically the antibody-producing plasma cells, will hopefully migrate to the bone marrow and lie dormant for decades, which is how vaccines given in childhood continue to provide protection many years later. This is true of the annual flu vaccine too, by the way; the issue isn’t that those vaccines don’t provide lasting immunity, but that influenza is a rapidly mutating virus and different strains are more common every flu season. So your flu shot from 1997 or 2008 is still providing you with protection… But only against the flu strains that were chosen for the vaccine in 1997 and 2008. They’ve even done studies that showed people who survived the Spanish Flu Pandemic of 1918 could still produce an antibody response 100 years later! Coronaviruses mutate much more slowly than the flu, but it is too early to know whether SARS-CoV-2 will mutate enough or in the right way to require additional, regular vaccinations. If we can judge by the SARS and MERS epidemics of 2002 and 2012, it seems unlikely.
As far as other changes to our bodies, thankfully there is no plausible mechanism by which the COVID-19 vaccines could cause other chronic changes than the desired immune response. The mRNA only codes for a few specific proteins and cannot produce an active virus, and the fats, sugar and salts in the vaccines do little else than package the mRNA and help it get into the cell.
What about Infertility?
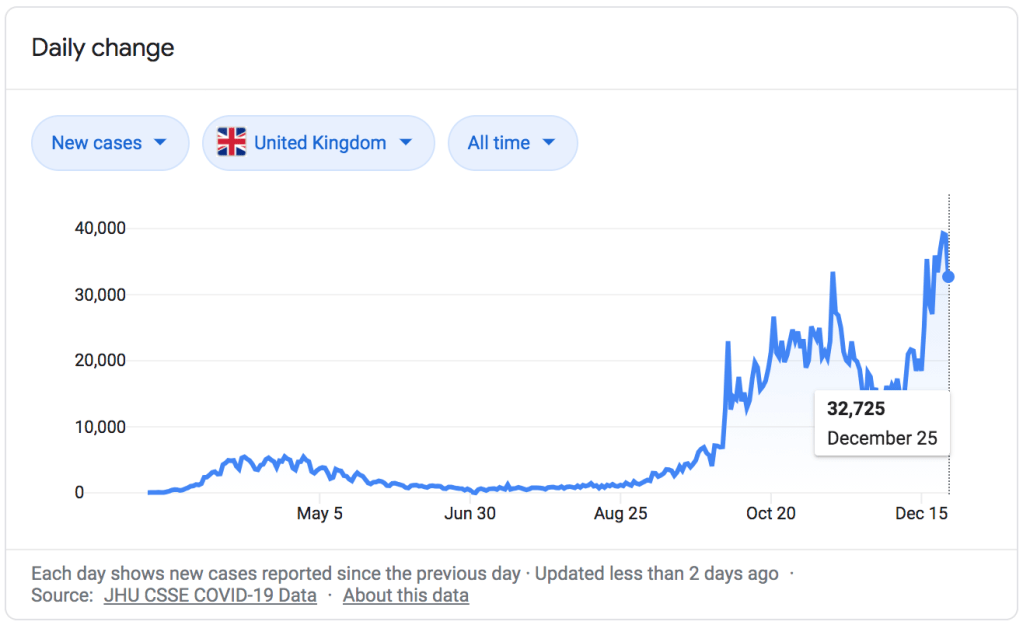
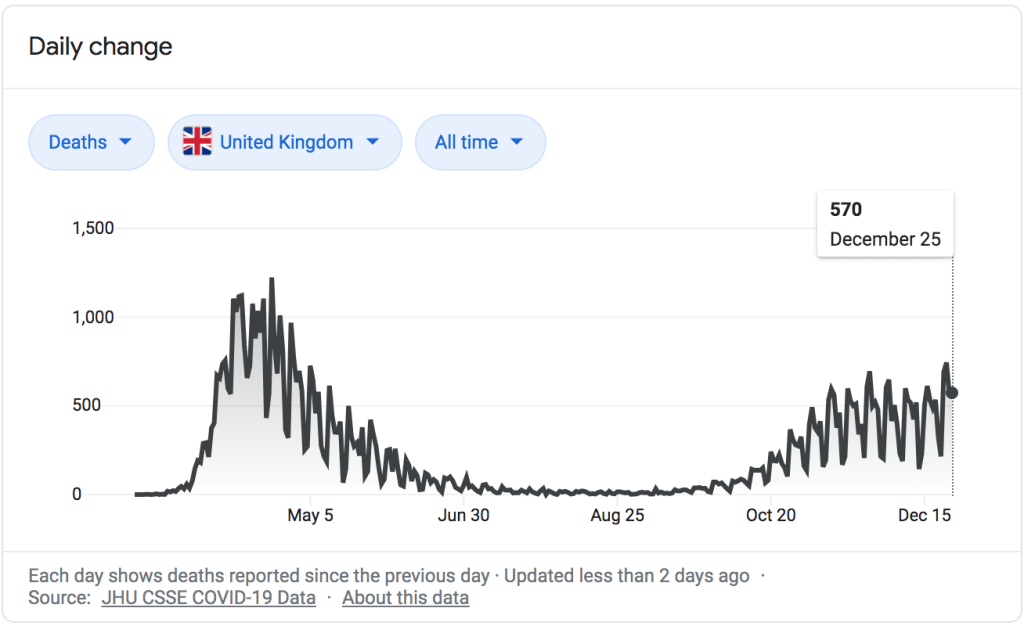
There has been misinformation circulating online about the vaccines causing female infertility, but these are baseless. The original claim can be traced back to Michael Yeadon, a former Pfizer researcher and COVID-19 denier who has also posted videos claiming that the pandemic really ended in late Spring, at least in the UK, because most of the population was already immune due to having antibodies to other coronaviruses, which cause the common cold (as of today there have been over 70,000 deaths in the UK from COVID-19). This is an extremely ironic idea in light of his claims about the vaccine causing infertility, as we shall see shortly. He has not worked for Pfizer since 2011, and calling him the “Head of Pfizer Research” is just as deceptive as the rest of the headline and article.
The vaccine does not contain a spike protein called Syncytin-1, at all; the article above is simply lying at that point. The actual theory claims that the COVID-19 spike protein the vaccines code for shares similar amino acid sequences with a human protein, Syncytin-1, which is important in placental development. They reason that antibodies trained to attack COVID-19 would also attack Syncytin-1, causing infertility. This is illogical and scientifically invalid for a few reasons.
First, we have already had 80 million cases of COVID-19 worldwide and there has been no evidence of infertility as a side effect; yet the body of any infected person is going to produce antibodies against multiple COVID-19 proteins, including the spike protein in question. If the antibodies we develop against the spike protein from having the virus don’t attack Syncytin-1, there is no logical reason to believe vaccine-induced antibodies would either.
Second, we have evidence from the COVID-19 vaccine trials themselves that pregnancy occurs at similar rates between those vaccinated and those not vaccinated. The vaccine trials did not include pregnant women or women who intended to become pregnant, and all women of child-bearing age that participated had a negative pregnancy test before their first dose and committed to using a method of birth control throughout the study. Thirty-nine women became pregnant anyway; twenty-three in the Pfizer trial and sixteen in the Moderna trial, and the rate of unintended pregnancy in those who received the vaccine was about the same as in the placebo group. Those numbers are too small to draw serious conclusions, but the point is that we already have examples of women who became pregnant after receiving the vaccine, even though they were actively preventing pregnancy; in the coming months as more and more people receive the vaccines, we will have many more examples, and because this misinformation has been popular there are already studies planned to track the pregnancy rate following vaccination.
Third, the number of amino acids in the shared sequence is actually tiny; a segment of 5 amino acids, with only the first two and the last two being shared. Syncytin-1 has a full sequence of 538 amino acids, and the COVID-19 spike protein itself is 1,273 amino acids long. We have an analogy in human disease; one explanation for rheumatic heart disease following streptococcal infection is that certain proteins in the Group A strep bacteria share similar amino acid sequences with myosin, a protein found in heart muscle, allowing antibodies against the bacteria to cross-react with heart tissue. However, in that case there are not only much longer sequences of shared amino acids, but multiple sequences that repeat multiple times each. The section of shared amino acids in the case of Syncytin-1 and COVID-19 antibodies just isn’t significant, and you will find many viruses and bacteria in nature that share such similarities with a great many proteins in humans.
Finally, SARS-CoV-2 is not the only coronavirus in existence; not by a long shot. Coronaviruses are one of the main groups of viruses that cause the common cold, and you and I have both had many coronavirus infections throughout our lives. You still have antibodies to those coronaviruses, as Dr. Yeadon points out in his other videos. Every single coronavirus has spike proteins (that is what gives them their name; they form a halo, or corona, around the virus when you look at it through an electron microscope), and all of those spike proteins share as much or more similarity to Syncytin-1 as the COVID-19 spike protein, because they play similar roles in viral replication to what Syncytin-1 does in placental development (they are fusion proteins). So you have already developed antibodies against coronavirus spike proteins all throughout your life, maybe even every single year, just like everyone around you; and yet this has never been identified as a contributing factor in human infertility.
So yes, the vaccine will have a lasting impact on your body, assuming you respond well like 95% of clinical trial participants. The lasting effects will be the same as the lasting effects of surviving the virus: immunity to COVID-19, and hopefully long-lasting immunity. The difference is that the vaccine doesn’t carry a risk of serious illness or death to you or transmission to those around you. And thankfully, neither immunity from getting the vaccine nor immunity from getting the virus itself will cause infertility.
Aren’t the vaccine ingredients toxic?
Updated 12/29/2020
Those whom I interact with regularly who are undecided or hesitant about vaccines are typically patients and parents with sincere, legitimate questions, who deserve the time it takes to hear their concerns, answer their questions completely, and offer reassurance. But unfortunately, therearealso people out there who are promoting anti-vaccine propaganda and deliberately creating false narratives. One common strategy to increase unease or paranoia about vaccinating our children is to simply list the scientific sounding ingredients and then ask, “do you really want to put that into their bodies?” Usually this approach will ignore benign sounding ingredients like “sucrose” or “gelatin”, and focus in on lengthy or scientific-sounding ingredients like “nicotinamide adenine dinucleotide” or “cetyltrimethylammonium bromide,” which register emotionally as more intimidating, less safe, and less natural. Of course we know that logically a chemical with a long name would not necessarily be any more or less dangerous than one with a short name; “ricin” has a short name, and it’s the 5th most dangerous chemical in the world (that is just an example; there is NO ricin in your vaccines. I do not want to see a bunch of memes next week claiming they put ricin in vaccines). But fear mongering is not always logical.
DANG IT
They might also home in on a naturally occurring and well known chemical that most people think about in conjunction with another of its uses, counting on that association alone to create fear. A good example is formaldehyde, which most of us think of in the context of embalming, but is also used in applications from color photography to deodorants; and of course, as an anti-bacterial and anti-fungal in certain vaccines. Some vaccines contain about .005 to .01 mg per dose; a 2 month old baby produces up to 200 times more than that every single day as a part of their normal metabolism (for adults, it’s more like 3,000 times more). Yet because our culture so strongly associates formaldehyde with death, merely invoking it’s name is enough to create unease.
Most of the ingredients in vaccines are there to keep the attenuated or killed virus pieces from decaying long before they are injected. Others are there to prevent the growth of bacteria or fungi in the vaccine vials themselves. Still others are used to stimulate the body’s immune cells around the injection site to make them more likely to produce an adequate response that leads to long-term immunity. All chemicals we encounter in our lives are toxic under certain circumstances; none of the ingredients in vaccines are toxic at the doses or in the manner given. I think people often forget that the scientists who design the vaccines, and the doctors and nurses that counsel patients about them and inject them, are human beings who also vaccinate ourselves and our children; we want vaccines to be safe for selfish reasons, too, not just altruistic ones.
That all applies to traditional vaccines; the new mRNA vaccines are made differently, and so they don’t need a lot of the same additional chemicals to ensure they work. In fact, what’s shocking about them is just how few ingredients they actually have. In addition to the messenger RNA molecules themselves, the Pfizer vaccine has just 4 synthetic fats (lipid nanoparticles) meant to deliver the mRNA into the cells that will build the COVID-19 spike protein, 4 salts to make sure the vaccine is at the same acidity and osmolality as the tissue it is being injected into so it can get absorbed (and hurt less), and 1 sugar, sucrose, to protect the vaccine during cold storage.
Salt, fat, sugar. And that’s it.
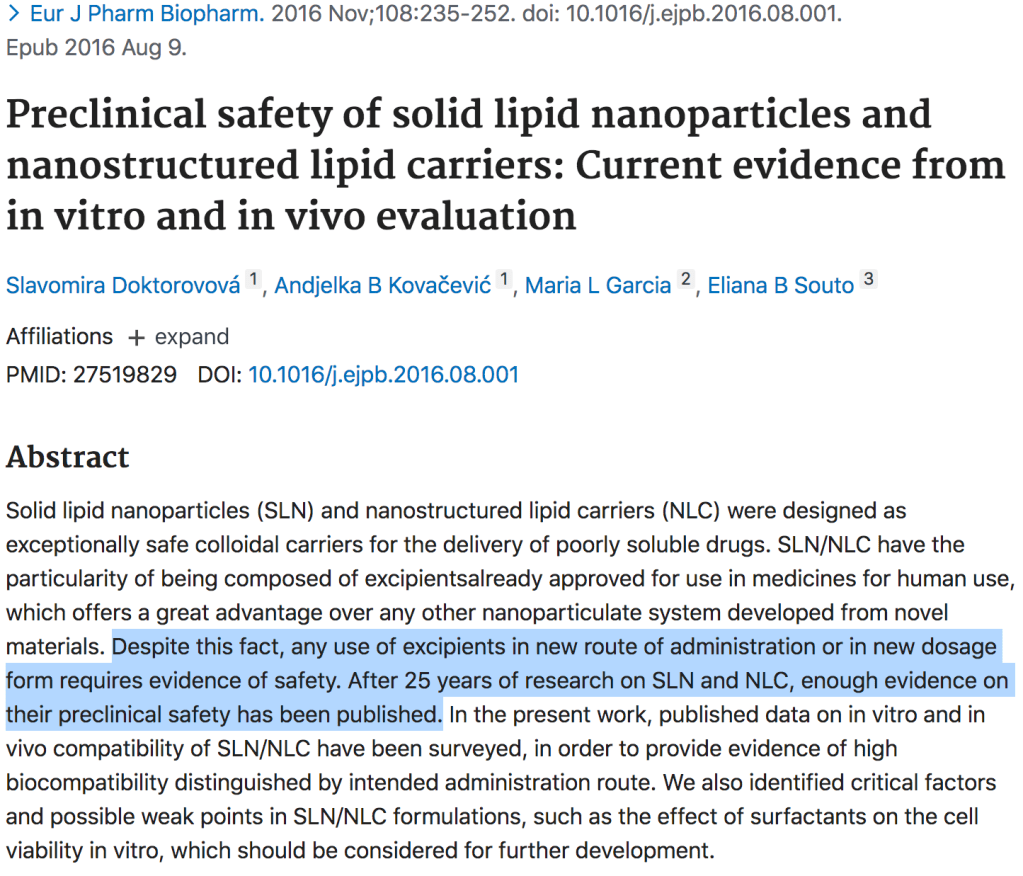
Some of the substances can still cause a reaction; the leading theory right now is that the few anaphylactic reactions to the Pfizer vaccine were likely due to polyethylene glycol, a common chemical we give in huge doses for constipation, but which can cause an extremely rare, but serious, allergic reaction. This chemical is used to create the lipid nanoparticles through some Tony Stark level methods I can’t hope to understand. The lipid nanoparticles (very small fat molecules that can protect the mRNA) themselves are indeed new technology; which in science terms means about 30 years old. Over that time period their safety has been studied extensively and found to be safe, non-toxic, and biocompatible/biodegradable. And because the world is crazy,no, they are not tiny robots(but how cool would that be?!).
By contrast, “Nana Lipid Particles” are just the cookies she keeps sneaking your kids when you aren’t looking.
An article in 2016: “After 25 years of research…” The math checks out.
I can’t claim to be familiar with every anti-vaccine meme and article out there, but I haven’t seen as much about ‘toxic ingredients’ with the COVID-19 vaccine, and I think that’s because even compared to the safe ingredients of traditional vaccines, the ingredients of the COVID-19 mRNA vaccines just sound very unimpressive, and thus feel less intimidating.
If I get the vaccine, can I still transmit/spread the virus?
This is a question I’ve heard frequently, especially from those who themselves work in healthcare or have vulnerable friends and loved ones. It is a question driven by compassion. In this blog we have been trying to address the fears and concerns that arise not only from conspiracy theories and misinformation, but also from the very small but real risk associated with the vaccines; yet I know that many people would brave whatever degree of risk to themselves (again, It’s very small) if it meant protecting their family and community. If they could be guaranteed that their choice to get vaccinated meant they could safely visit an unwell grandparent or have coffee face to face with a friend without any risk of spreading the virus, it would be a no brainer even if there was a considerable risk it might cause significant side effects like Bell’s Palsy (there isn’t).
And I wish I could give that reassurance today, but while I can say that the chances are very good this vaccine will not only protect you but also protect those around you, we still need much more data to be able to quantify the degree of that protection.
The point of the vaccines is to provide your systemic adaptive immune system, the part that acts powerfully and rapidly against specific disease, with the information it needs to produce the antibodies you need to keep you from getting very sick. A common misconception is that after you get say the flu shot, you can’t get the flu. It’s not true. The flu shot doesn’t give you a magical forcefield around your body that blocks flu virus, it just helps you fight it much, much more quickly and efficiently when you do get it; often to the point that you never even know you are infected, or at least only have very minor symptoms. Vaccines drastically reduce the chances of you becoming extremely ill from deadly disease like influenza, measles, or COVID-19; that’s their job.
This is not how you get a cold. He’s the best he is at what he does; but what he does is not immunology and pathophysiology.
This main function of vaccines is what underpins the epidemiology strategy of giving the COVID-19 vaccine to healthcare workers and the most vulnerable first. The medically vulnerable, because they are the most likely to require high levels of care, to suffer long-term problems from infection, or to die from COVID-19; and healthcare workers because as the pandemic worsens it becomes more and more important to preserve our medical workforce, and vaccinated folks are less likely to need sick time (much less become seriously ill and require hospitalization themselves) for COVID-19. The other reasons for vaccinating healthcare workers go back to courage, trust, and solidarity with our patients in the face of any new treatment. We are prioritizing vaccinating the vulnerable instead of say pathologic extroverts because the effectiveness of the vaccines at preventing significant illness is known (90-95%), but their effectiveness at preventing transmission is still unknown.
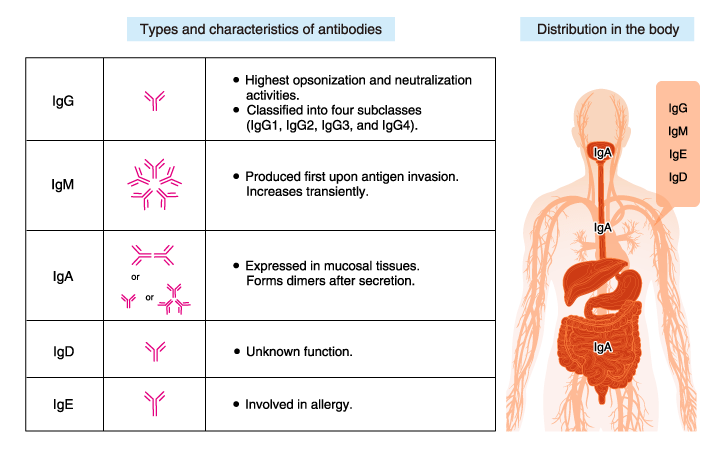
So how do we find out so that Dustin can get his vaccine? Well, the big question mark is IgA antibodies. Most of the research on antibody production from COVID-19 vaccination focuses on IgM and IgG because they predominate in the blood and represent, respectively, our short-term and long-term antibody protection against systemic (whole body) illness. But IgA is the main antibody in the mucous membranes; your mouth and throat, nasal passages, lung surfaces, and digestive track (it’s also the antibody responsible for passive immunity transmitted through breastmilk), and we know that the IgA response to infection is a big, big part of what neutralizes the virus and decreases transmission in those first 10 days of symptoms. If the vaccines “only” cause a significant IgG and IgM response during that post-vaccine exposure to the COVID-19 virus, it will prevent severe infection; and may still prevent enough viral replication to slow transmission. But if it produces a strong IgA response too (or a strong enough mucosal IgG response), it will almost definitely neutralize any live virus in the upper airway as well, making transmission as unlikely as severe illness. In other words, the degree of IgA response is a strong predictor of whether the vaccine protects those around you as well as it protects you.
Because of this, researchers are already studying the degree of production of mucosal IgA against COVID-19 in vaccine recipients, with some promising results, and at least one intranasal vaccine (which produce a very strong IgA response) is under development. And while the best information we could get would be to see exactly how well someone develops IgA and neutralizes the virus by studying them when they are exposed to COVID-19 after vaccination, it’s sort of hard to catch people in that window. In the end we will probably have to settle for epidemiology data instead; carefully watching to see if clusters of infection occur around exposed, asymptomatic vaccinated people at the same rate that they do around unvaccinated people. That will take time, but if and when it becomes apparent that vaccinated people really aren’t spreading the virus to those around them at all, that will be the point I’ll stop wearing my mask, practicing social distancing, and washing my hands (fine, fine; I’ll keep on washing my hands).
I realize this was a really long-winded way of saying “I have no idea,” but I want to conclude with a few reasons you should get the vaccine even if your main concernis not spreading the virus to others.First, there is already a lot of good data that supports the idea that these vaccines will provide mucosal immunity (and thus decrease transmission), both from studies of the COVID-19 vaccines themselves and from our much more robust knowledge of vaccines in general; it’s hard to say anything with much confidence yet because we’ve had these vaccines for such a short time, but I’m pretty optimist they will. We’ve followed these principles for years; we recommend everyone around a newborn be vaccinated against Pertussis (whooping cough) because the newborn can’t be, and we know that vaccine-derived herd immunity works even for viruses that are primarily spread through respiratory particles. Second, there is no conceivable mechanism by which they would increase transmission. The vaccines cannot make you produce live virus (at all) so they can’t make you contagious, and if you are exposed to COVID-19 later on your body will still respond with a mucosal immune response whether it is augmented by your vaccine or not (and it probably will be); the vaccine won’t stop that. And third, by preventing a severe systemic illness, the vaccine will decrease the amount of time you are shedding virus and prevent transmission in some of the most high-risk settings; aerosol producing procedures like nebulizer treatments or intubation in the hospital. And by preventing symptoms like coughing and sneezing the vaccine will make you less contagious when exposed to the virus, as long as you are still following other transmission control measureslike wearing a mask and quarantining after exposure.
IgA response due to ChAdOx1 nCoV-19 vaccine (the tall red columns are good!)
So no, unfortunately being vaccinated against COVID-19 does not give us carte blanche to schedule giant indoor parties, throw away our masks, and treat the pandemic as if it were over; but they are a huge step in that direction, and in addition to protecting ourselves they do have a fair, if yet unproven, chance of protecting those around us too. And besides, if you don’t get vaccinated, how are you going to get your government tracking microchip?
Bad joke, sorry.
Other Vaccine Posts:
No Vaccine Selfie Yet or “Why I am uncomfortable getting vaccinated”
I’ve actually been thinking about this particular blog post for a while. Ever since I took on the role of being a clinic lead for our system’s very busy outdoor COVID-19 clinic about 6 months ago, I’ve been seeing multiple COVID-19 positive patients, face to face, 3 to 5 (sometimes 6) days a week. Unlike the very high volume, rapid turnover testing-only strategy that is so important from an epidemiology standpoint, these were real medical visits; I heard about my patients’ symptoms and exposure history, we discussed risk factors, we checked vital signs, and I listened to their hearts and lungs. When we needed them, we got blood work or EKG’s, or if the patient was pregnant, listened to the baby’s heartbeat.
COVID-19 is a stressful thing to be seen for, and patients very frequently need more than just a targeted physical exam and a test result. At each visit I provided reassurance, and careful instructions for quarantine or isolation as their clinical situation demanded. I told my patients not to be afraid, and then we discussed what vigilance demanded and a detailed discussion of the signs and symptoms that should lead them to seek further care or go to the emergency department. Sometimes these visits really only lasted 5 or 6 minutes; sometimes they lasted 15-20.
I don’t have an exact count, but I’ve done around 1,500 of these visits since the pandemic started.
Masks are very, very good at preventing COVID-19 transmission, and my N-95 and faceshield are a powerful combination; but they are not perfect. Besides, we know that masks are better at protecting against lower velocity respiratory droplets and work best when worn by both parties. Many times my patients were coughing and sneezing, and some simply couldn’t tolerate wearing their mask for our entire visit because of their shortness of breath or other reasons, so we relied entirely on my own PPE, and the outdoor setting, to mitigate the risk of that face-to-face visit. I knew this would be the case sometimes; it’s the nature of the job.
Because of this, my wife and I have more or less treated my getting COVID-19 as an inevitability (it wasn’t actually inevitable, but it definitely felt that way). So when I recently joked darkly on facebook how nice it was knowing that “if I join the 1,700+ American healthcare workers that have died from the pandemic so far, my $300,000 of med school student loans are non-transferrable to my wife and 4 children,” and then in a blog post on not going home for the holidays said, “My PPE game is strong”and“I’m really, really good at being cognizant of fomites and at personal transmission control,” anybody with even a small amount of Genre Savviness could have told you what would happen next.
Sure enough, following a night of fever and chills and a morning of coughing, sneezing, sore throat, and headaches, I finally tested positive for COVID-19 yesterday afternoon. As someone who diagnoses and treats COVID-19, who writes about COVID-19, and now who has COVID-19, I thought my perspective might be helpful to others, and today I’d like to write about what I willand won’t be doing over the coming days and weeks (specifically as it relates to my diagnosis; nobody wants to read about my Mandalorian costume 3d printing).
5 things I’m not going to do now that I have COVID-19.
1. I am not going to Panic.
One of the biggest communication challenges I face on a daily basis is helping patients understand that a virus like COVID-19 or seasonal influenza can be extremely deadly and devastating in aggregate, but not necessarily dangerous for a particular individual. There are pitfalls on either side; if my patient erroneously believes that there is a 100% chance the virus is going to make them so ill that they end up in the ICU, they will spend the following days and weeks in fear and anxiety, less capable of navigating their symptoms and more likely to over-utilize an already strained emergency medicine system, and easier prey to those profiteering off of the pandemic by selling unproven pharmaceutical and wholistic ‘cures’ (including, sadly, at least a few doctors out there).
But if my reassurances cause them to believe that the virus isn’t dangerous, as many people do despite a now insurmountable accumulation of evidence to the contrary, not to mention the lived experiences of our friends and neighbors, there is a risk that the rest of my cautions and teaching about transmission control will go unheeded.
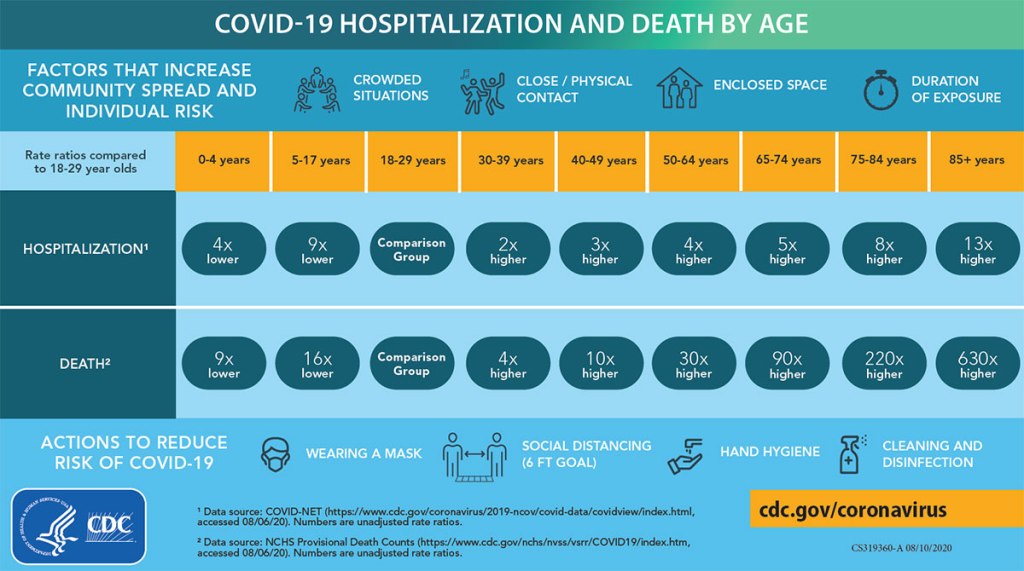
We will look at the numbers in a moment, but this is the most dangerous virus in our lifetimes. The risk an illness presents to a community is based both on how dangerous each individual case is and on how many people contract it. So while any particular COVID-19 case is more dangerous than the flu but far less likely to lead to serious disability, life-long suffering, or death than a case of say Ebola, it is much, much more contagious and will therefore make up the ground easily. And we do not share the burden of risk equitably. We know that the risk of a serious illness and death is greater for those above 50 and far greater for those 65 and older. We know it is greater for those with chronic medical problems, especially those affecting the heart and lungs, multiple medical conditions, and compromised immune systems. But these biological factors are not the only ones at play; people are also more vulnerable if they are part of a marginalized community, and have worse access to healthcare, preventative health, and affordable nutrition. We know they are more vulnerable if they are non-English fluent and therefore have a harder time navigating intricate healthcare systems or having their symptoms and questions understood in a busy clinic or emergency room. We know the poor, especially, bear a greater burden of illness in all diseases, and despite talk of COVID-19 being ‘the great equalizer’, equality just isn’t something American healthcare has been setup to deliver.
I am a white male doctor, 35 years old, in pretty good health, with excellent food access, living in a town with a dozen clinics and two hospitals where many staff know me by sight. I have all the advantages in the world when it comes to surviving this. With COVID-19, sometimes all of that isn’t enough, and we can’t predict and don’t really understand why some healthy young people develop incredibly severe symptoms and die despite our best efforts. But it is, relatively speaking, rare. So I’m not really afraid of this infection for my own sake, but I am taking it deadly seriously because among the many people I love and care about are those who have fewer or none of the privileges I do. And even among those few who are actually at lower risk that me- those who are younger, healthier, and whiter I guess- they are still at some risk, and those characteristics and the privilege they represent are not a perfect protection against this pandemic. So for all of those people, I will be staying home for the next 10 days at least.
2. I’m not going to take unproven medications (and I could get them if I wanted to).
One of the main reasons I have chosen to write about being diagnosed with the virus, instead of just quietly continuing to nitpick viral videos, is because this is really my first opportunity to put my money- or my health- where my mouth is. I’ve been writing about the dangers and sheer impracticability of physicians prescribing unproven treatments like hydroxychloroquine and budesonide since May. Now I have to put those reflections into action, and the outcome will affect myself and my family.
There is a tough kernel of suspicion in the minds of many people that when the doctor tells you there isn’t a specific medicine that will treat your illness, it really just means there’s not a medicine we are willing to give to you. Many people really do believe that there are special treatments reserved only for those who are ‘in the club’: doctors and their families, VIP’s, the wealthy, and those with excellent insurance. If you are a person of color in the US, or belong to any other group that has been marginalized and continues to experience systemic discrimination, there are even good historical reasons to struggle with this suspicion and to find it hard to trust the medical field in general; and not just the Tuskegee Syphilis Study, though it remains the most notorious example. For people with this shared cultural narrative, taking a quick look in my medicine cabinet at home, or those of any of the physicians I have treated for COVID-19 during this pandemic, to see that we are taking the exact same medications and treatments we are offering to our patients may be a good start to dispelling this particular myth; but rebuilding broken trust obviously takes a lot more than that.
I know literally hundreds of doctors; I’ve been learning with them, training with them, and working alongside them for the last decade and a half. This creates a great amount of potential for privileged healthcare access, which we have to be cognizant of and intentional not to abuse (and which is not fully cancelled out by the fact that we are, as a profession, notoriously bad at setting aside time for our own physical, mental, and emotional health). Most of those doctors believe exactly as I do about unproven treatments not supported by evidence; but not all. Even if it took a few phone calls, I could probably find a doctor willing to prescribe me budesonide, hydroxychloroquine, systemic steroids, azithromycin; any or all of the ‘silver bullet’ medicines (besides bleach) that have been touted by viral video doctors convinced by confirmation bias, selection bias, conspiracy theories, and negligible sample sizes.
Why am I not? For the same reasons I haven’t prescribed them (except when they are indicated, like my COPD patients who were experiencing an exacerbation and needed a course of prednisone) for those 1,500 or so patients who have entrusted me with their care during this crisis: Because there is no evidence that they work.
Instead I’m going to do three types of treatments, all of which I recommend for my patients.
Medications I am already taking.
Unless specifically recommended by your doctor, you should not discontinue the medications you need for chronic medical conditions. Although it’s always a good idea to revisit your medicines with your PCP and make sure you still actually need them, especially if you are on many medications per day.
Medications to alleviate my symptoms.
I take fluticasone and cetirizine for sinus congestion and allergies, and recommend them to my patients when they have similar symptoms. I like guaifenesin for chest congestion, and tylenol and/or ibuprofen for headaches, body aches, and fevers. I may call my doctor’s office and ask for some tessalon perles if this cough get’s any worse, though that medicine doesn’t work for everyone. None of these will cure the virus, but with any luck they will make the next week or two a lot less uncomfortable. Before starting any prescription or OTC medication, check to makes sure it doesn’t interact with your other meds and isn’t contraindicated because of a chronic health condition; your PCP is happy to help you with this.
Non-pharmaceutical supportive care treatments.
One day I’ll get around to writing a blog post titled “Your Physician is also a naturopath.” Despite claims that doctors want you ‘locked inside your house’ for the entire pandemic, I encourage my patients to get plenty of sunlight and as much exercise as they can tolerate with their symptoms; just not to do it around people they could infect. We have the privilege of a backyard; for those who don’t we talk about how to be outside but safely distanced while you are under isolation or quarantine. We are also going to talk about the need for additional rest and fluids. If you have a sore throat, we touch on judicious use of chloraseptic spray; but I really emphasize hot water or tea with plenty of honey. I might recommend a nasal decongestant, but I also talk with my patients about safely using a Neti Pot or saline rinse, as long as they don’t have contraindications (and don’t use tap water). I take a multi-vitamin daily and eat a balanced diet, but as long as they aren’t taking amounts that could be toxic or being taken advantage of with expensive, high-profit-margin products, I don’t give my patients any pushback on taking additional vitamins or immune supplements. My recommendations regarding alternative health treatments that don’t have solid evidence are these; they should be safe, they should be affordable, they should not interfere with your evidence-based medical care, and if at all possible they should have a plausible mechanism of action that actually relates to your condition or symptoms. That covers an awful lot, and anybody who claims to be helping you but fails those criteria is probably, quite literally, trying to sell you something.
3. I’m not going to get bored of isolation and decide it’s ok for me to stop early.
That first part is a lie; I’m definitely going to get bored of isolation. I’m strongly extroverted and I’ve been terribly bored of socially distancing for months now. I absolutely love being at home with my wife and four children, it’s my favorite place to be in this present world (besides the Bua Thong “Sticky” Waterfall near Chiang Mai, Thailand); but after 10 days I’m going to be dying (Editor: probably a poor choice of words) to spend an afternoon sitting outside at a coffee shop, or go for a trail run in the park instead of doing laps in our small back yard.
Nevertheless, I’ve heard too many stories of people who decided that since they were asymptomatic or minimally symptomatic, or because they had reached day 6 or 7 and felt better, that their COVID-19 infection didn’t count and they were the exception to those pesky CDC guidelines. Who did I hear these stories from? Mostly from the people they had infected.As much as certain people make ‘freedom’ their rallying cry and rail against so-called draconian restrictions meant to decrease transmission of the virus, the truth is we are pretty much free to follow the guidelines given to us by our doctors and by public health experts, or not, to whatever degree we choose. As much as people talk about the specter of government tyranny related to fighting the pandemic, there really isn’t much we can’t do. I got diagnosed with COVID-19 yesterday, and I could have sat inside at a restaurant or a bar last night; nobody would arrest me. I could sit inside at my favorite coffee shop all day today, and publish this blog entry about me having COVID-19 while sitting there, coughing and sweating and with a hoarse voice, and it’s still extremely unlikely that anyone would say anything to me. Why don’t I? Because of this:
Because with all of that freedom comes responsibility, and because the number of family, loved ones, friends, and neighbors, co-workers, and patients we each lose during this pandemic, which is now in it’s darkest hour, depends on how seriously we each take that responsibility; how deeply we feel the true gravity of our own actions.We are living right now in the failures of our society to do just that. I don’t claim to have been perfect over the past 9 months; but every single one of us needs to stop and honestly consider if there is any area of our lives where we can make different choices in the coming weeks and months to try to prevent even more loss of life.
Deadliest days in US history from a single cause or event. (This list omits individual days from the Spanish Flu Pandemic of 1918-1920, which killed on average 1,000 Americans a day but came in several very bad waves) This meme is less than 48 hours old and is already out of date. Today it would look like this: 1. Galveston Hurricane – 8,000 2. The Battle of Antietam – 3,600 3. Yesterday- 3,055 4. San Francisco Earthquake – 3,000 5. September 11th – 2,977 6. Last Thursday – 2,861 7. Last Wednesday – 2,762 8. The Day Before Yesterday – 2,630 9. Last Tuesday – 2,461 10. Last Friday – 2,439 (11. Pearl Harbor – 2,403) With hospitals getting overwhelmed, by the end of the month it’s possible that only the top 1 or 2 will still be on this list.
4. I’m not going to Church.
Our church, Mosaic Waco, has done an amazing job of meeting safely throughout the pandemic. We have “Drive-In Church” in-person but outside and socially distanced every other week, and staff members, volunteers, and congregants consistently wear masks. Our pastors and other leaders have sought out and listened to the wisdom of epidemiologists, physicians, and other experts, especially those who are brothers and sisters in Christ, and understand acutely the difficult balance of goods in deciding how best to gather as believers. They have rightly considered responsible transmission control measures as an essential part of our responsibility to love our neighbors during a pandemic.
All that said, I skipped last week. We were having Drive-In Church and I had signed up to serve, but we were beginning to see signs of illness in our family, and our policy has been to exercise an abundance of caution when it comes to the health of those around us. I’m skipping this week too, obviously, though we are going to continue to attend online. The worship band probably can’t manage without me running the slides, poor things, but the pandemic demands sacrifices of us all.
I bring it up because there has been a popular and persistent narrative that has invaded the Church in America that choosing not to meet in person, or humbly following expert and even pastoraladvice for social distancing and masking, is somehow a betrayal of Christian values; even when failing to do so is potentially dangerous for those we name as brothers and sisters and claim to love. We are commanded in Matthew 10:16 to be as wise as serpents and as harmless as doves, and seldom has the interrelationship between these two concepts been as obvious as during a viral pandemic, when our ability to be do no harm to those around us is predicated so strongly on the amount of wisdom we practice, and the amount of wisdom we are willing to receive from experts. Attending your local church in-person, and particularly indoors, when you are ill, under quarantine, or have other reasons to believe you might be at risk of transmitting the virus is as unwise and harmful as it is unloving.
5. I’m not going to make my experience normative.
We’ve talked already about all of the privileges I personally have facing this illness. Except for my age and a minor medical problem or two, it would be hard for me to be at lower risk from this virus. And even though I can’t perfectly predict what will happen, statistically I’m probably going to be fine.
And that’s great, but it does leave me open to a big temptation that I have seen so many people fall into; taking the anecdotal experience of one or a handful of people and using it to dismiss the suffering of millions, including 290,000 of our neighbors who have died in the last 10 months. After each warning, each exhortation to take action now to prevent more disease and death, you will inevitably see someone comment “I had COVID and I was fine.” And we are glad for that, but me or you feeling well and having a mild course of illness says absolutely nothing about the experiences of others. Even deeper than the flawed logic at play here and the willful disbelief and disregard of physicians, nurses, EMS workers, respiratory therapists, and all the others who have shared their own and their patients’ experiences with this crisis, this view betrays a deeply seated arrogance; believing that our own personal experiences are somehow more real than the suffering of our fellow human beings, or the grief of their loved ones.
5 things I am going to do.
1. I am going to take precautions in my own home.
The very first question I get from almost every parent when they are diagnosed with or even tested for COVID-19 is, “what about my children.” I’ve had the opportunity to talk with hundreds of patients about what is an extremely personal and complex decision; how much to isolate and distance from their own children if they have the virus. Thankfully, this conversation gets to start off with one piece of very reassuring data; while children have become very ill and died from this virus, it has been rare, and children and adolescents seem to be the people in our society least likely to experience a severe course of COVID-19.
Nevertheless, the risk is not negligible and it should not be ignored. The degree of caution each of us needs to follow in our own homes when diagnosed with COVID-19 depends on many factors; the ages and developmental ages of our children, how much they depend on us for their daily needs, their individual personalities and the ways they experience love and closeness, the available space in our homes, and the amount of support we have, among others. I have a lot of privilege in a lot of these areas, particularly in having a spouse who takes care of everything with the kids by herself for 50+ hours a week at baseline. If we chose to go the route of many doctors and other healthcare workers early in the pandemic and I moved out for 2 weeks, she would make sure that they didn’t lack for anything except actual time spent with their father.
We have decided not to go this route. Instead, we’ve taken these precautions:
I am wearing a mask when I’m in close proximity to my family.
I am washing my hands obsessively.
I am not letting anyone drink after me (if you have kids, you know exactly how difficult that can be).
I am not kissing anybody (if you have kids, you know exactly how difficult that can be).
I am not preparing food (much to everyone’s relief).
They are strictly quarantining; groceries delivered, no visitors, no birthday parties, no trips to the store or quick stops for coffee.
These decisions become even more challenging when you are caring not for a healthy child, but for an aged parent or a chronically ill or immunocompromised loved one. Again, these are difficult decisions, and we each have to decide for our own families what is the right balance between the need to protect them from the virus and their need to be near us and receive our love, affection, and care in person.
2. I am going to keep fighting for my patients.
Most (though not all) of the misinformation I write about here on the blog contains at least a nugget of truth. Those who have said for the past 10 months that the measures we have adopted to fight the virus are worse than the virus itself couldn’t be more wrong; but they are right about the added dangers of interruptions to care, decreased access, and postponing medical visits, which have all been secondary effects of the pandemic. We’ve been working hard for months (and in the early days of the pandemic were literally working around the clock) to make sure our patients could still get the access to care they need. Even so, it continues to be a struggle.
Having your primary care physician out for 10 days, isolating due to COVID-19, is a huge barrier to care; and it would be even if we had primary care doctors to spare, which we definitely don’t. There are some services or interventions I provide that only a handful of our doctors are trained to, and there are patients whose situations and histories I know all the details of, and even with good medical documentation it would take another clinician a lot of additional work to be brought up to speed with them. There are also patients who simply prefer their doctor and are slow to seek help or accept guidance from any other, which says very little about me personally as a physician but an awful lot about the inestimable value of carefully built, mutual trust and respect at the core of the doctor-patient relationship.
So I’m doing what every other doctor I know does when they are sick: in between naps and bowls of chicken noodle soup, I’m making myself a nice hot cup of tea and logging onto our computer system remotely, responding to telephone calls, refilling medications, and following up on lab results, all trying to make sure my patients have access to equitable care and that the interruptions in that care because of my illness are as few, and as mitigated, as possible. I realize that sounds super braggy, but that’s not my point at all. My efforts are hardly heroic (I once watched a pregnant 2nd year resident in charge of the OB unit receive IV fluids for her hyperemesis gravidarum in between helping other women deliver their babies. I’ve got nothing on that); but I think it’s important that anyone reading this knows how deeply their doctor cares about them and how hard they are working on your behalf, even when you can’t see it.
3. I am going to notify my close contacts.
Done. Unless those close contacts don’t read this blog, of course, in which case they are on their own.
Actually, I’m incredibly thankful that I don’t have anyone to notify. I’ve alerted my teams both at my usual clinic and at our COVID-19 outdoor clinic, since we work together every day. We wear our PPE continuously in clinic, are seldom within 6 feet of each other and never for prolonged periods, and if we have lunch it’s outdoors and very physically distanced; I actually don’t count as a close contact for anyone I work with. We are watching my children and wife for symptoms, and have notified a few people that she has been around out of an abundance of caution even though they also don’t count as ‘close contacts’ by the CDC guidelines. Other than that we don’t have any phone calls to make. It’s a good feeling and I highly recommend it.
4. I am going to finally replace the HVAC ductwork under the house.
Not COVID-19 related, but I’ve been promising to get it done for weeks. Check back with me after isolation and I’ll let you know how it went. #fakenews #misinformation
Sexist. Passive Agressive. Accurate.
5. I am going to makes plans in case things go bad, and go to the hospital if my symptoms get severe.
I know this is a two parter, but it’s short and I really wanted to keep the symmetry of ‘5 things I won’t do/5 things I will do’. Back in March when videos began to circulate from overwhelmed hospitals in Italy and France and Katie and I first began to grasp the gravity of the situation, we made a few arrangements. We knew I would be on the front lines one way or another. I made sure she had all of the account numbers for retirement accounts (she handles most of our finances anyway, so bank accounts weren’t an issue), the password to access my life insurance policy, etc. We talked carefully about those non-transferable medical school loans that would be discharged in the event of my death, and about being on guard against predatory offers to “refinance” loans which should, in fact, simply disappear. We talked about burial arrangements and funeral wishes, and how we would want to be remembered to our four young children if we passed. I gave her my list of top 10 guys she was allowed to marry after an appropriate mourning period. We finally got around to making a will.
My wife’s search history shortly after this sobering conversation. (this joke included over strenuous objection and my own better judgement)
I also made e-mail addresses for each of our kids for when they are older, and began to send them the occasional note or letter, letting them know just how much I love them and delight in seeing who they are now and the wonderful people they are becoming.
Now that I actually have the virus, we are revisiting these items, I am writing to my kids again, and we are making sure everything legal and financial is hammered out just in case.
The fact is that we expect me to be fine, but we’d be extremely foolish not to take this illness seriously; many younger and healthier people than me have died from it already. I’ve been giving people guidance about what to watch for at home for almost a year now; chest pain, significant shortness of breath, confusion or altered mental status, severe fatigue and malaise, low oxygen levels (we’ve reclaimed my pulse oximeter from our 3 year old’s Doc McStuffins doctor bag), or any acute worsening in overall status. For once in my life as a doctor I’m going to follow my own advice and treat my health seriously, and I’ll be heading in to the ER for further evaluation if I experience any of these symptoms.
Final Thoughts
Doctors and nurses know they are going to get sick; it’s practically in the job description. We have the incredible privilege of taking care of people on some of their best and some of their worst days, but that also means continuously getting coughed or sneezed on, being exposed to contagious illnesses, and occasionally, despite our best efforts, being exposed to a blood-borne pathogen. When it’s a known entity we are familiar with and have been fighting for years, the uncertainty following those experiences is less hard to bear; and honestly after 10 months of this pandemic, having COVID-19 doesn’t feel much different than any of those other old enemies, even if the ‘what if’ factor is a little higher.
I know this post will be met with sympathy, and I truly appreciate everyone’s thoughts and prayers; but I hope the main take away for anyone who reads this rather long-winded announcement of my illness is that what we are doing to care for our patientsand asking of each and every person we diagnose with this terrible virus are the very same things we ask for, and demand of, ourselves. If you or a loved one gets diagnosed, I hope you will have symptoms as mild as the ones I am currently having- a little fatigue, a little cough and sore throat, a few chills- hopefully even milder, or none at all. But I also hope you will be just as cautious as we are trying to be; taking the risk of transmission very seriously, communicating with those whom you might have unintentionally exposed, and respecting isolation for you and quarantine for your close contacts as a measure that can absolutely save many, many lives. I hope you are not afraid, and I hope you have all the information and support you need from friends, neighbors, and especially your local doctor.
And to the 300,000 people in this country who have died of this awful virus, the tens or hundreds of millions who have lost loved ones, family, and friends to it, and the 15 million others who have suffered from it physically to one degree or another, I am incredibly grateful to have had the chance to fight it with you and to walk through it alongside so many of you, and wouldn’t change any of that just because of this admittedly mild illnessI have now; whether it gets worse in the coming days or not. I’m looking forward to doing it again, as soon as I meet the CDC criteria to do so.
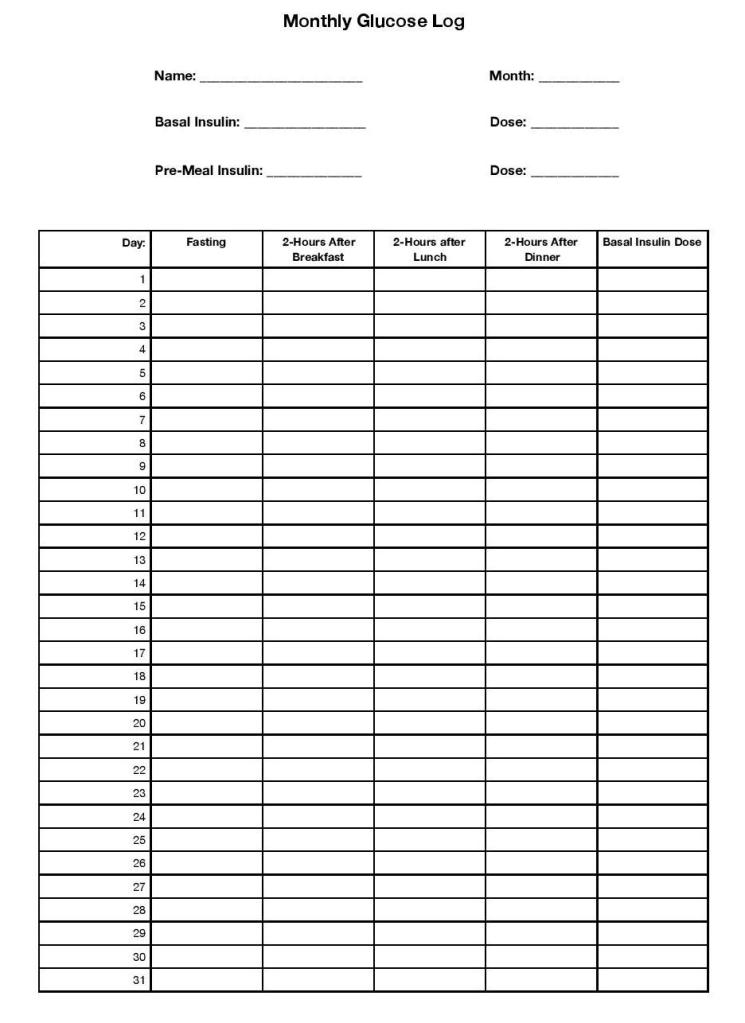
This is a short post because, frankly, I don’t have time to write it (clinic all day, D&D with the kids tonight). Those of you hoping for another 7,000 word in-depth discussion (read: nobody) will have to settle for just 3,000 or so today. Nevertheless, I want to start with a digression and show you this chart I use in my clinic:
This chart is for my diabetic patients who have a very particular treatment regimen; they are taking both a long-acting basal insulin once or twice daily, and they are taking a short or rapid acting insulin before each meal. Because of this, we need some blood sugar numbers; we need to know their fasting blood sugar in the morning so we can adjust their basal insulin, and we need to know their numbers 2 hours after breakfast, lunch, and dinner so we can adjust their meal coverage with the short acting insulin. They are not taking insulin on a sliding scale; those patients will need to check before meals in order to take the appropriate dose.
Now, I work extremely hard to empower my patients to adjust their insulin on their own, and a lot of our visit time is focused on teaching them about the various insulin length of action times, the logic behind basal/bolus insulin dosing, and especially what numbers to look for that should trigger them to increase or decrease their dose. But it’s challenging, and as much as I love it when a patient is on ‘auto-pilot’ with their insulin, we still do a lot of adjusting in clinic, which is where these charts come in. Fasting blood sugar high? We’ll go up on your long-acting Lantus insulin. Taking 5 units of novolog before every meal but the after-lunch numbers are still super-high? We can go up on your pre-lunch and keep the pre-breakfast and pre-dinner numbers the same. You get the idea.
So that’s the glucose log I print for my patients. Now let me show the one I actually hand to them:
You see, like all doctors my approach to any medical problem represents a balance between what my medical training tells me is the best possible treatment plan and the actual, lived experiences of my patients. Some of my patients will check their blood sugar 4 times a day, every day (some of them even if they don’t strictly need to; they just really, really like to know). But I don’t think I could manage to do that, and so I don’t ‘demand’ it of my patients. The reality is, we could get almost all the information that the patient and I need by checking their blood sugar half that much; fasting every day, then checking after a different meal each day. And most of my patients are much, much more likely to follow through with checking twice a day than four times a day (as I certainly would be).
What does this have to do with the quarantine recommendations for COVID-19? Everything, because both the CDC’s new guidelines and my approach to blood sugar logging for my diabetic patients are based on an essential mediator of medical outcomes: Health Behavior.
Where did the original 14 day guidelines come from?
The CDC began to recommend a 14-day quarantine for international travelers coming to the US as early as February, and the same for any household and close contacts of COVID-19 positive persons shortly thereafter. This was based on the incubation period of the virus; the range of time it typically takes an exposed person who becomes infected to develop symptoms. Initially this relied on the already known incubation periods of similar novel Coronaviruses, SARS and MERS, from epidemiology studies that were done following those epidemics in 2003 and 2012. As the COVID-19 pandemic progressed, studies began to emerge which showed similar incubation periods for the SARS-CoV-2 virus as well. A study from The Netherlands in February found the incubation period to be between 2 to 11 days based on a small number of patients in Wuhan, China; very similar to SARS and especially MERS. This was supported by multiple other studies that all showed an apparent incubation period somewhere in the range of 2-12 days.
This begs the question, “if most studies showed the incubation period to end at 10 to 12 days, why were we all told to quarantine for 14 days?” And this is where health behavior comes in. The first (and least important) reason, I think, is because 14 days is just a lot easier to remember. “Your last exposure was last Wednesday, so you can be done with Quarantine after next Wednesday” is easier to remember than 11 days or 12 days because we naturally think in weeks anyway. But much more importantly, the novel Coronavirus was noveland recommendations needed to be made based on very limited evidence. The two studies above had sample sizes of 88 and 158 respectively; enough to be going on with, but not nearly enough to be really confident. Those studies consistently showed that though we thought the average incubation period would be 5-6 days, there was still a possibility that once we had more data it would end up being much longer; and there was a very good chance that even if the average incubation period stayed less than a week, some people would still be contagious for much longer, maybe even greater than 2 weeks. With a virus this contagious, ignoring that uncertainty could be very, very dangerous.
Hence the recommendation to be released from quarantine only once you have been asymptomatic for 14 days since your last exposure; it was easy to remember, it was very likely, based on early evidence, to cover the vast majority of cases (although it does absolutely nothing for fully asymptomatic cases, of course), and it was unlikely to be expanded based on new evidence.
That last bit is really important, because even though epidemiologists, physicians, and other scientists know that it’s exactly how science is supposed to work, we’ve all seen how suspiciously our society looks on any changes in recommendations based on new evidence. If the CDC started with 14 days of quarantine and later decreased it to 12, some people would be a bit irritated and probably lose some confidence in them (we’ve seen this time and time again; the undeserved “they keep changing the guidelines!” and “They don’t know what they’re doing!”), but overall it would be a welcomed change. But if they had started with say 9 days and then, based on new evidence, expanded it to 16 days, how would that have gone down? It would have been pandemonium.
So they picked a timeframe that was 1. Supported by the data available and 2. Unlikely to be expanded later based on new data. But there was still a problem, and it was this: Health Behavior.
14 days of quarantine is hard. It’s hard psychologically, it’s hard physically, and it’s hard economically. I see COVID-19 positive and COVID-19 exposed patients every day and I have to tell you, I feel terrible every single time I have to recommend a 14 day quarantine to someone. I see the irritation or frustration or even despair as they try to figure out what plans they have to cancel, what friends and family they will have to miss, and how they are possibly going to make ends meet if they can’t work for that long. The results of quarantine so often touted by the anti-quarantine, COVID-19 is a hoax folks, like increased depression and anxiety, are real. No one ever denied this, it’s just that the pandemic is not a hoax and has, as of today, killed 1.5 million people worldwide and 271,000 in the US.
And because it’s hard, every single one of us knows somebody whodidn’t quarantine when they were supposed to. Unsurprisingly, that’s one of the main factors I see at play in my outdoor COVID-19 clinic visits; people were exposed to friends or family who had not reached the end of their quarantine period but decided that enough time had passed that they wouldn’t be at risk of spreading the virus. Based on what? Gut feeling, mostly; and also reaching the point where their desire for experiences or people or options precluded by quarantine was simply greater than their will to continue quarantine. For most of us, that point will probably come sometime before those 14 days are up. I even know of doctors who couldn’t make it to 14 days, and drawing on exactly none of there clinical training or basic sciences knowledge decided that they must have ‘dodged a bullet’ when they remained asymptomatic less than a week from their exposure, and resumed life as normal. Who am I to judge. I’m a strong extrovert and even general social distancing has been hard enough on me; there but by the grace of God go I.
And sometimes the guidelines, while valid, seem nearly impossible to comply with. For instance, I have friends who diligently completed their ongoing householdcontact quarantine guidelines, which begin on the day the COVID-19 positive patient is diagnosed and end 14 days afterthat person’s 10-day isolation period. That’s 24 days total for their household contacts.
This is no small problem; studies from previous epidemics requiring self-quarantine measures have found incredibly variable rates of adherence, and often south of 50%. In many ways America was a set-up for poor compliance to these guidelines; highly individualistic culture, a pandemic occurring in the most contentious election year in recent memory, massive campaigns (organized and unorganized) of misinformation about the virus, and with no clear messaging or leadership on a national level. Those last two points are crucial, because the strongest predictor for adherence is not cultural or socio-economic factors, or even fear of the virus; it’s how knowledgeable people are about the virus and the way it spreads, and how well they understand the quarantine guidelines. Which is, uh, why folks like me are doing this sort of thing.
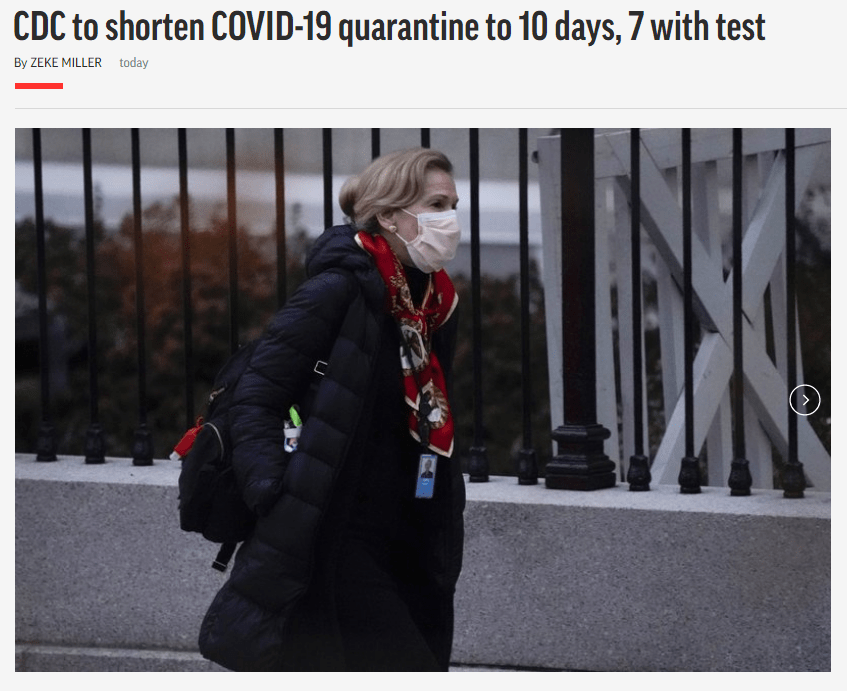
12/2/20: The CDC will update quarantine guidelines.
Which brings us to today, and the new quarantine options from the CDC, which are these:
7 days, as long as they remain asymptomatic and have a negative COVID-19 test.
Why were these changes made? Because they were wrong back in February? Because the election is over (finally)? Not at all. There are two possible reasons: either because enough new evidence has emerged to convince the epidemiologists at the CDC that these timeframes are as safe and effective as the original 14-day recommendations, or because they are convinced that enough people will actually follow through with these less extreme guidelines that there will still be a net decrease in transmission.
Let’s look at the first one. There have been nearly 14 million cases in the US since February and over 64 million world wide; even without access to complete information of each of these individuals and their exposures to COVID-19, we should be able to muster more than the 88 cases that first study was based on. Have all of the newer, more robust analyses of this data changed the picture of COVID-19 incubation so drastically that the CDC was forced to update their guidelines?
Answer: Not really. It’s important to note that when the CDC did finally release the updated guidelines late in the night, they clarified that the new guidelines were alternative options to the 14-day quarantine, which was still their strongest recommendation. I believe this is supported by the evidence.
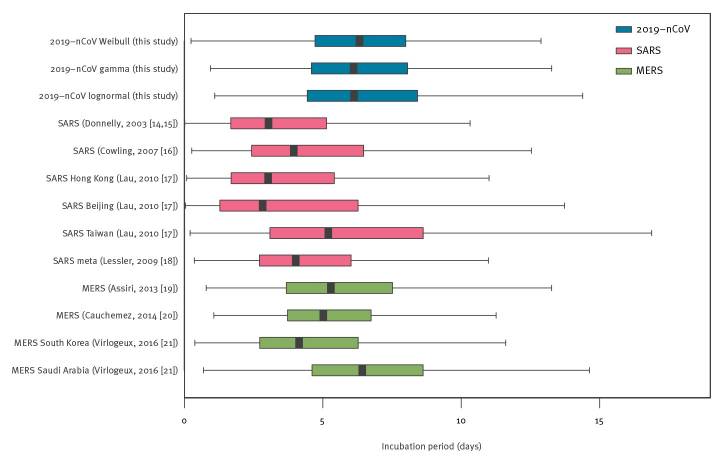
Just like there was nothing magical about day 14 that caused the virus to go, “all righty I guess we’re done here, pack ‘er up boys!” back in March, there’s nothing magical about day 10 or day 7 now. A systematic review and meta-analysis of all the then available estimates of the COVID-19 incubation period, first published in The British Journal of Medicine in August, found an average (mean) incubation period of 5 to 7 days, and 95th percentile estimate between 10 and 14 days…. Remarkably similar to the earlier estimates. The figure below is from that paper and reflects the distribution in all of the studies they could get their hands on. Notice how there isn’t a steep drop off at day 10; in fact, the range of the possible incubation period stretches all the way out to about 3 weeks. Unlike the early observational studies, this meta-analysis involved multiple studies with hundreds of cases each, though that original data was still from early on in the pandemic.
Another meta-analysis from later in the year, first published in October in the online journal Current Therapeutic Research, included 18 studies representing 22,595 participants. That’s a lot more than 88. What did they find? The average incubation period was about 6 days. This paper was advocating for a much shorter quarantine, along with testing, similar to the new ‘7 days with a negative test’ recommendation from the CDC; tellingly, however, it only included analysis of the mean incubation period, not the range of incubation from those studies; it doesn’t address the impact of all of those cases that would cease quarantine on day 7 but become symptomatic within the next few days.
Finally, a relatively small but thoroughly analyzed study from Singapore including 164 cases from January to April and published in the journal Epidemiology and Infection in September shows some cases with an incubation period definitively longer than the 10 day mark set by the CDC, though they were relatively small in number. It also found that the incubation period does seem to be positively correlated with age, with the longest incubation periods among those in their 70’s and older.
To summarize, unless there is some big study that the CDC has access to and I can’t seem to find (and please send it to me if there is, so I can take this post down and not look like an idiot), the current evidence has not revised the known incubation period of COVID-19.
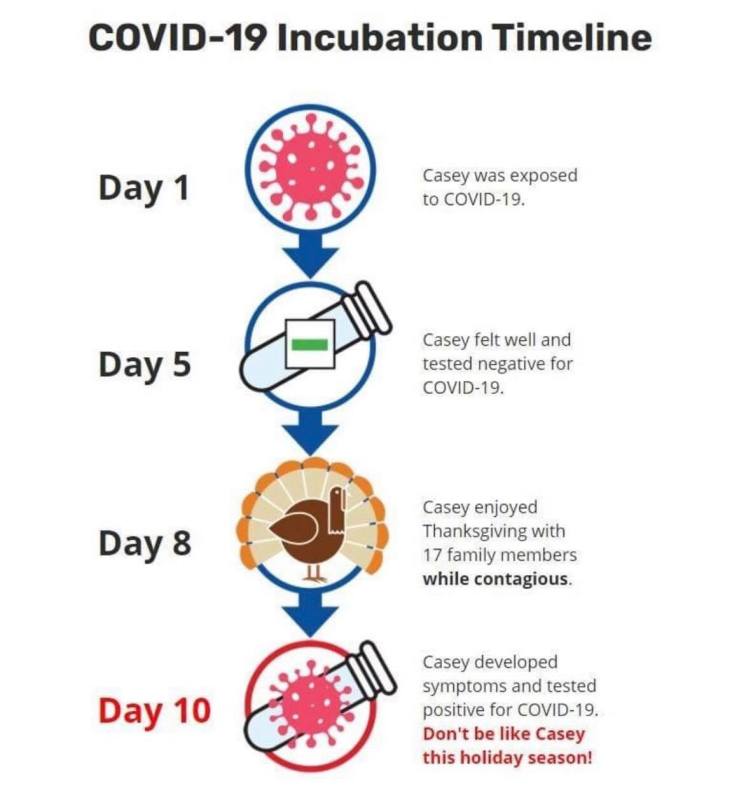
You can still develop COVID-19 symptoms more than 10 days after your exposure.
Q: So why the change? A: Health Behavior
So if the CDC isn’t changing the quarantine guidelines because of some scientific breakthrough that has utterly overturned our understanding of the virus’s incubation period or the way it is transmitted, why make the change at all? Because the 14-day quarantine guidelines aren’t working; not because quarantine doesn’t work, but because people won’t do it. They are banking on the idea that enough people will be willing to comply with a less aggressive quarantine period that still covers the vast majority of cases (compared to a longer quarantine that very few people were willing to follow) to make up for the relatively few cases whose incubation period would have been longer.
I don’t know if they are right or not. Something’s gotta give, so I really hope they are. But overall I actually kind of like this new recommendation because it has the potential to change the behavior of one group of people that has probably been contributing to the pandemic numbers as much as anyone else; asymptomatic COVID-19 carriers who aren’t following quarantine at all. The biggest weakness with the 14-day quarantine was that there was no fail-safe built in for the people who just weren’t willing to quarantine. They might stay home from work or school for 14 days because they had to, but would use some of that time to shop, have parties, or engage in other activities that had a high likelihood of transmitting the virus. I don’t mean to imply it was all from selfish motivations; some people with much less natural laziness than myself probably just couldn’t cope with 14-days off, and have probably been using their quarantine to help others and do good deeds around the neighborhood, or volunteer more at their local church or community center. Good things in themselves, but still very, very dangerous when you have been exposed to a deadly and highly contagious virus. And like I said before, many others very understandably don’t have the margin to be out of work for that amount of time. The new guidelines are helpful because for people very motivated to stop quarantine after day 7, a test for COVID-19 now greatly increases the chances that we’ll catch their infection and modify behaviors that lead to transmission. Even if they weren’t following quarantine before that day 7 test, they might follow isolation guidelines if it’s positive.
We know that asymptomatic and pre-symptomatic people can still spread COVID-19, but asymptomatic testing has always been a double-edged sword. Very wide scale asymptomatic testing would be one of the best possible ways to catch and isolate cases early and really modify the course of the pandemic, and asymptomatic testing targeting people in essential services, like nursing home nurses and doctors, is the best way to prevent pre-symptomatic transmission among some of our most vulnerable populations. But in both of these situations, the test result always leads to either a neutral or a safer set of decisions; if asymptomatic people test positive, they isolate, while negative people continue their standard level of caution. If a nurse or doctor tests positive, she calls in; if negative, she continues to work.
But testing of asymptomatic people who have been exposed and are still under quarantine is completely different, because the test result now has two drastically diverging branches; not safer and neutral, but safer and less safe. If an exposed person does test positive, it is much easier for them to feel the weight of their responsibility to keep those around them safe from it; I’m sure anybody reading this who has tested positive remembers the moment they received that news, and remembers how real the need to isolate suddenly felt. But since they are already under quarantine, there is a very real chance that a negative test will give many people a false sense of security without actually guaranteeing that they won’t become contagious, and instead of continuingwith the same degree of caution they are most likely to exercise far less. There are a hundred different cartoons online right now demonstrating this concept. I like this one because it feels like the person who wrote it really has a vendetta against somebody named Casey.
This is the reason my COVID-19 clinic has shied away from broadly testing asymptomatic close contacts; the value of that test can be a big positive or a big negative, and it entirely depends on what the person plans to do with that information. If they plan to quarantine well regardless of a negative and only want to know so they can alert their close contacts, that’s terrific; but I’ve talked with lots of people, patients of mine and otherwise, and even some healthcare workers, who were under quarantine due to close contact and planned to get tested so that they could go ahead and travel, throw a party, or go back to work early. A negative test, within the incubation period, cannot definitively make these actions safe, and depending on when in the incubation period, might be no help at all. That’s why I carefully counsel every patient about what to do with their test results, symptomatic or not, based on their clinical history. I’m not opposed to asymptomatic testing for exposed individuals; it just has to be accompanied by a very careful discussion of what the test can and can’t be used for.
With all of that in mind, if you are going to do asymptomatic testing for exposed close contacts, 7 days seems like a fair point to test. Again, it’s easy to remember; ‘1 week of quarantine and then get tested’. But more importantly, it’s past the mean incubation period; a test on day 7 covers the incubation period for most people who remain asymptomatic, and has a good chance of catching any pre-symptomatic patients with an incubation period up to day 8 or 9. Between that and of course testing the folks that do have symptoms as soon as they get them, that covers most people. And if that negative test does give a little false sense of security, it’s at a point in the timeline of their exposure where lots of folks are feeling ready to throw caution to the wind anyway.
It’s not perfect, but I wouldn’t call the new quarantine guidelines ‘misinformation’ either. It’s a calculated risk based on the expected health behavior of a population who is absolutely exhausted with this pandemic. I hope it pays off.
So… What do I do then?
Adherence to quarantine is highest when people really have a firm understanding of the quarantine guidelines and the rationale behind them. The rationale behind this decision is that more people will comply with less extreme quarantine guidelines that are still, for the most part, safe. But it doesn’t mean I’ll be counseling my patients differently; I still want them to know that they could become contagious for a few days after that day 10, and that the negative test on day 7 is not a 100% guarantee. I want them to understand the incubation period of the virus and the extra caution they still need to take for those several days after their quarantine is technically over. When I’m writing school and work notes, if their quarantine period under the new guidelines has them going back on a Friday, we are going to push that back (with the patient’s permission) to Monday. When they test negative on day 7, I want them to know that they should still come back and get re-tested if they develop symptoms on day 11 or 12.
And that’s the advice I’m offering to you now. If you have a close contact and need to quarantine, try to make it to at least day 12, if not day 14, before releasing yourself if at all possible; or get tested on day 8 or 9 instead of day 7 if you can. Advocate for those around you by fighting for your right to ere on the side of caution, recognizing that the current guidelines are a compromise with the expected health behaviors of our society. A timely and hopefully effective compromise, but a compromise nonetheless. And just as you wouldn’t act like Casey and use a negative test on day 5 as an excuse to cast aside all precautions, so a negative test on day 7 should be treated as reassuring, but not foolproof.
But as for me and my house, we will quarantine for 14 days.
As the pandemic has escalated over the past several months and almost all of us who had been previously unaffected have now had friends, family members, or other people we care deeply about either pass away or at least become very, very ill from the virus, I’ve noticed a trend in the misinformation that we accept, share, and believe. The nature of a global pandemic is that it robs us of our delusions, and we are now many months out from being able to believe what was commonly said in March and April, that the pandemic is not coming, and that even if it does come it is not deadly. The landscape has shifted, and until more conspiracy theories crop up about vaccines or possible outpatient treatments in the coming weeks and months, the misinformation has settled back into the realm where it is most resilient; into the question of motives. It doesn’t matter what actually happens with medications, vaccines, case numbers, and death rates; believing that the people trying to help you are actually trying to control you is always fair game.
Hmm… Gandalf is pretty sus.
In about a week we are going to see the merger of COVID-19 misinformation and the ever-popular “War on Christmas” conspiracy which annually reminds us that dark forces are at work in the world to destroy my favorite holiday and everything it stands for. But until then, Thanksgiving is the target apparent of the powers that be.
Full disclosure, I’ve waged a small private war against Thanksgiving for years, and it has nothing to do with how many people are gathered. My concern is with the way we celebrate and especially teach children about the history of Thanksgiving and the way we sterilize the history of Native America-European settler relations. I also have some concerns, as the doctor to many patients with diabetes and CHF, about the lack of nuance in our culture’s understanding of feasting, and typically resolve this by telling my patients not to check their fasting blood sugar on Black Friday (unless they take correction dose sliding-scale insulin, of course). For me, it’s the most hypocritical holiday of all, because while I caution moderation to my patients I know I will probably fail to practice it myself. Because you see, despite all of my concerns about Thanksgiving as a holiday, I alsolove turkey and dressing, pumpkin pie, and most importantly (as any true Southerner will tell you) green bean casserole, macaroni and cheese, mashed potatoes and brown gravy (I’ll lose readers over that), and a sweet potato and marshmallow dessert we have hilariously convinced ourselves is a side dish instead of a hedonistic excess and probable harbinger of the end times.
(I also like seeing my family and stuff.)
So the togetherness and joy of the thanksgiving holiday is something I’m loath to give up for any reason, and I would be lying if I told you that I knew all along that we would opt for a small family Thanksgiving day in our own home, or that I immediately made that decision after reviewing the trends in COVID-19 numbers or even after reading Dr. Emily Smith’s excellent, excellent review of the relevant epidemiology facts. We earnestly struggled with it. And as we weighed the medical risks of our extended family members against my daily interaction to COVID-19 positive patients and my wife’s recent exposure to the virus, I could taste the potato casserole fading from my future as we made the difficult call and informed very disappointed (but understanding and supportive) family.
Fine, but when I say “Cancel Columbus Day” I definitely mean it.
And I’ve been counseling my patients to do likewise, just like many physicians, epidemiologists, and other health scientists around the country. And despite the suspicion and mistrust that a doctoral degree elicits these days, it has nothing to do with wanting to control my patients lives, training them for future subservience to the government, my crusade against the idea that our relationship with Native Americans was ever truly mutually respectful and supportive, or even the principle that misery loves company and if I don’t get to eat my grandma’s turkey dressing recipe on Thursday they shouldn’t either.
Instead, it’s because we are living today in the most dangerous window of the pandemic so far, and because there are characteristics of Holidays in general, and Thanksgiving in particular, that makes this week an incredibly dangerous one for our country.
3 Reasons that Thanksgiving is Dangerous.
1. Certain holidays are more dangerous than others. Even allowing for difference of culture and family tradition, the innate characteristics of certain holidays make them more or less dangerous in terms of transmission of a respiratory virus. January 2nd, World Introvert Day, will probably be just fine; but the indoor concert you are planning for National Kazoo Day three weeks later on January 28th should be cancelled because that is a lot of aerosolized spittle in an enclosed space (it should be cancelled anyway regardless of COVID-19, but that’s not my point).
If we are going to discuss the characteristics of Thanksgiving, it would help to compare it to another widely celebrated holiday we’ve experienced during COVID-19, the 4th of July. As a reminder, here is a look at the numbers.
California
Texas
Florida
USA
The two weeks after the 4th of July saw the largest spike in cases of COVID-19 we’ve experienced during the entire pandemic (except for the one we are in now). There’s a strong enough case to be made that the trajectory of that wave was already increasing prior to the holiday; but the public gatherings, parties, and beach trips dramatically contributed to the rise in cases, heightened the severity of that late-July peak, and appreciably altered the curve for the worse in places like Florida and California. In a moment we’ll compare some of the characteristics of these holidays, but that’s really splitting hairs; the biggest reason that Thanksgiving is dangerous is because COVID-19 transmission follows the principles of exponential growth; the more cases you start with going into a time of decreased caution like a holiday, the greater the impact it will have on the curve. We are already close to or above capacity in many hospitals around the country; evenanother 4th of July, with the numbers we have right now, would absolutely drown us. And there’s plenty of reasons innate to the holiday that make Thanksgiving much, much worse.
It’s true that the 4th of July has some characteristics that could make it more likelyto result in spread of COVID-19 than Thanksgiving; mainly that it involved very large events that brought together people from very different spheres of contact. A few cases of COVID-19 could spread easily to multiple social circles and families from one big 4th of July party. But Thanksgiving has some characteristics that make it more dangerous too. First, unlike the 4th of July, most people celebrate Thanksgiving indoors; transmission is more likely indoors than outdoors, all things being equal. Second, contact tends to be prolonged; you aren’t just passing various people for a moment on the way to the beach or grabbing a beer, you are sitting face-to-face for hours while eating and visiting and (unless you are a good-for-nothing-in-the-kitchen family freeloader like me) cooking. If a contact at a 4th of July party has COVID-19, you may or may not have been exposed. If someone at Thanksgiving Dinner has COVID-19, everyone there is definitely an exposed close contact.
This is literally a picture of our Thanksgiving. Except for the 2nd one (I grew up Baptist).
Third, that issue of bringing people together from different spheres of contact is true for Thanksgiving just as much as for the 4th of July. Traveling for the holiday is one of the major things that public health experts are warning against, and even if you aren’t flying or driving across state lines, not everyone’s social circles really overlap much with their cousins’ or grandparents’. One family member who has had an exposure or hasn’t taken precautions in the weeks leading up to Thanksgiving runs the risk of infecting their entire family, and those family members bring their exposure back to the other members of their community. Finally, Thanksgiving brings people together who are not likely to socially distance from one another. It’s all well and good to say ‘we will eat outside and stay 6 feet apart’, but how many times has that actually happened when getting together with family you have been longing to see? There will be hugs, there will be boardgames, there will be long heartfelt conversations- or yelling matches about politics. Not to mention the decision of whether or not to finish off somebody else’s half eaten piece of pumpkin pie if nobody is looking, which is a difficult enough choice even under normal circumstances.
But we don’t have to just take my word for it or guess whether Thanksgiving will be as bad (or worse) as the 4th of July, because Canada has a Thanksgiving too, which they hold (ridiculously) on October 8th.
The Canadian numbers show a miniature warning of exactly what we would expect after a national holiday during a national uptick in cases; a steepening of the curve and a much larger number of new cases over the next month. The difference is that Canada has nowhere near the number of active cases or the amount of community transmission that we have; our increase is going to be much, much more dramatic.
2. Holidays bring together those who are at greatest risk with those who spread the virus best. We talked about the total lack of social distancing between relatives when they finally get together, and nobody is better at not socially distancing than children. If you think about the emotional value we all place on the holidays, probably one of the first images that comes to mind is the sight of your children running to their grandparents and covering them in hugs and kisses. It’s honestly one of my favorite moments each and every time it happens. It’s also a very, very dangerous situation if there’s any possibility those children have COVID-19. Children spread COVID-19 very easily; some studies have shown that children spread it even longer and more efficiently than even the sickest ICU patients. They spread it even when asymptomatic, and are asymptomatic at a higher rate than adults. They are also in school, and schools are full of other small gross people that spread COVID-19 efficiently, and those schools will not be closed for the holidays for any significant period of time prior to Thanksgiving.
And who are they hugging on? Almost certainly the people in your family who are at the highest risk if they do get exposed. We have been discussing the risk factors for severe COVID-19 infection, COVID-19 pneumonia and respiratory distress syndrome, and death on this blog since April and a lot of those factors haven’t changed; age, chronic lung disease, diabetes, heart disease, other chronic medical problems. But age is the first one, and the risk of someone dying from COVID-19 increases dramatically after age 50.
By bringing together the people in your family most likely to have been exposed to COVID-19 over the past few weeks (because of school) and most likely to spread it even when asymptomatic, and the people most likely to get seriously ill if they are indeed exposed to COVID-19, holiday gatherings with extended family really do present a dangerous situation for the most vulnerable members of our families.
I’ve had patients ask my advice on what to do about visiting grandparents and great-grandparents for Thanksgiving over the past few weeks. I hear their anguish, their indecision, their desire to celebrate with family fighting against their fear of spreading the virus to someone they love, and the deeper fear and guilt that they are making the wrong decision by choosing to miss out on those beautiful moments together. My recommendation? If you think that, barring some tragedy, the person you love has some good years of holiday celebrations left, it seems wise to sacrifice thisone in order to safeguard all of the others. This pandemic won’t last forever.
3. It isn’t just COVID. I’ve been reflecting on my very first efforts at writing about COVID-19 back in March, before I even started this blog. At that time the US had 23,604 deaths from COVID-19 and healthcare workers and public health experts were urging caution, which people were generally willing to follow… for a little while. Today it is 260,000 and instead of seeing this as validation of the concern we have had since March about how bad this virus can be, many people havelong since thrown caution to the wind for really no other reason than that we are all incredibly, unbelievably fatigued. I’ll write about that sometime soon; but what I’ve really been thinking about from those first posts is these two short paragraphs, which are just as true today as they were then.
Guess what? We are there.
As I’ve said before, most people don’t understand what an overwhelmed healthcare system looks like because we’ve never experienced it. It means not having access to doctors and nurses when you are in DKA or have a skull fracture. It means your kid can’t get treatment for his seizures or his infected spider bite. It means that every single medical condition is more dangerous (many are more dangerous during the holidays anyway) because medical professionals don’t have the time, the mental energy, the tools and equipment, or even the staffing to deal with them properly. It means not being able to get an ambulance to get you to the hospital or a bed when you get there. At a time when tent hospitals are being put up around the country, we need to decrease COVID-19 transmission right now to prevent permanent injury and death from everything from high-risk pregnancy to Congestive Heart Failure to snow-skiing accidents.
And of course, as we saw in New York, an overwhelmed healthcare system makes the virus itself incredibly more dangerous as well. “I can always go to the hospital if I have a bad case” has never been a good argument against exercising caution; but it is simply not true if you can’t go to the hospital or if they can’t take care of you well once you get there. The death rate has held more or less steady since it started to decline because of our increased understanding of how to fight the virus with targeted, COVID-19 specific ventilator techniques and successful use of medicines like dexamethasone for hospitalized patients. But the biggest factor that will cause it to go up again is doctors who are too tired to think and nurses who are too busy and fatigued to catch their mistakes.
But how can I celebrate Thanksgiving with family safely?
I never want to be accused of being an alarmist, and if we are talking about reliable epidemiology principles and the solid medical realities of how the virus is transmitted, I would say of course there are safe ways to do Thanksgiving together. In theory. We could talk about things like only meeting outside, everyone distancing from people not in their immediate family, no sick people at all being allowed, and everyone strictly quarantining for a full 14 days prior to the Holiday. The problem is, those are things that are hard for anyone to do, let-alone a large group of people, and the chances that every member of your family can or will strictly adhere to those guidelines is very low; and it gets lower with every person you add. If people are working anywhere other than home, or they are traveling at all prior to the holiday, or if you’ve got just one family member that believes the pandemic is a government sponsored hoax meant to force you to wear a mask and will therefore gleefully shirk every precaution the family has agreed upon when the time comes, your gathering has gone from perfectly safe to not perfectly safe; and not perfectly safe is, in aggregate, really really dangerous right now.
Whoever made this meme and then watched it go viral: “Yeah, take that Casey! Hahahaha, hahahaha!”
Or let me put it another way. I’ve seen more patients with COVID-19 than any doctor in my clinic system; maybe more than any doctor in town, though there are those whose exposure risk I would rate as being higher than mine (our pulmonologists and ICU docs, for example, or the young medical residents who are seeing patients with COVID-19 in both the outpatient and inpatient setting and the ICU… and of course our nurses, who typically have more time face-to-face with our patients in the hospital, and in clinic perform procedures like nasopharyngeal swabs that are higher risk for aerosolizing respiratory droplets). I’ve been tested for COVID-19 12 times; half because of symptoms and half because of our internal exposure protocols. I’ve been negative 12 times; my 13th test is tomorrow (and if it’s positive I’m coming back to delete this paragraph). I would never disparage the degree of caution that has been taken by my medical brothers and sisters who have contracted COVID-19 in the line of duty, or imply that I’ve done anything they haven’t; but I’ve been seeing COVID-19 positive patients almost daily since April and have utterly failed to contract the virus. My PPE game is strong. I’m really, really good at being cognizant of fomites and at personal transmission control. I’m confident that if I can design and implement clinic protocols that protect patients and staff 40 hours a week, I could do the same for a 3 hour meal… But I’m staying home for Thanksgiving.
Why? Because it isn’t worth the risk. Because the virus is very, very real and I really care about my relatives and neighbors. I’m not afraid of COVID-19, and I’m not letting it control my life. I’ve heard all of that hyperbolic nonsense and rejected it; prudent action on behalf of those you love is not “living in fear,” and giving up one meal with extended family for one year is not letting it “control your life.” I’ve also heard the rejoinder, “but where do we draw the line?” Somewhere else, obviously. And even though I’ll probably be back here in three weeks encouraging you to have a small family Christmas this year, if you want the best possible chance at a safe Christmas with extended family (after strictly quarantining for 2 weeks and carefully laying out ground rules for everyone attending, and not flying to get there…), the best thing we can do is take wise, collective action to stem the tide now. Turkey and dressing will taste just as good in May or June.
Pretty heavy-handed, I know… But it feels like we are at that point of the pandemic.
I’ve promised at least a dozen people that I would write about this over the past month and have so far utterly failed them. The truth is that it’s such a huge topic, and so fraught with the risk of saying something too extreme and dogmatic, that it’s hard to even know where to start. In a way, being at least a month late to this topic is much, much more comfortable, because not only do we have much more data now, but I can write in the certain and comfortable knowledge that my essay will have no impact whatsoever on what we do about reopening schools (not that it would have anyway). My goal therefore, besides keeping out of trouble, is to provide whatever insight I can into whether or not it’s safe to reopen schools and then what you, dear reader, can do to mitigate the inherent risks within your own scope of influence. I don’t always lay out a thesis statement at the beginning of these essays, because despite what I learned in Freshman honors English, I usually don’t have one (sorry Mrs. Greer!); but today I want to address whether going back to school is going to worsen the pandemic, whether it is worth the risk, and what parents, educators, and we as a society can do to make this situation as safe as possible.
Is going back to school going to make the pandemic worse?
Answer: Yes, absolutely.
Did you want me to elaborate, or is that sufficient? The reality is that I can see no way that this isn’t going to make the pandemic worse. On some level this math is incredibly simple; more people in close quarters means more cases, and more cases means more deaths. The real question is how much worse will reopening schools make the pandemic, and as we discuss below, whether that risk is justified right now. This question is going to answer itself in a few months, maybe even within a few weeks; but right now the best we can do is guess.
When I first started writing about this issue, I wasn’t sure what conclusions I would draw (which is generally a good way to start, if you can do it). I actually expected to arrive at answers that were cautiously optimistic, but as I went through the current data I became more concerned. My goal in writing this was not to sound an alarm or argue a point but to evaluate the evidence, and if you find my conclusions somewhat more discouraging than you had hoped, please know you aren’t alone; I was discouraged too. We are going to look at three types of evidence; what the epidemiological and experimental data tells us about how children and adolescents spread the virus, what has already happened in other places that have reopened schools, and what the risk is to these populations, to educators, and to the family members of school aged children and adolescents.
Can children spread the virus? I’ve said before that for any discussion of whether or not children and adolescents can spread the SARS-CoV-2 virus, the burden of proof would be on the side of proving that they don’t, not proving that they do. We have decades- nay, millennia- of experience with and evidence of children spreading viral respiratory illnesses. I see it literally every day in my clinic and have experienced it within my own body when I have been laid up for days (I’m told this is called a “man-cold”) from a virus that one of my adorable walking fomites brought home from parents-day-out or Sunday School (or whatever your church calls it to avoid having to call it Sunday School). Under normal circumstances we take this very seriously; we cancel birthday parties when one of our kids has a fever and we regretfully reschedule plans with friends when a respiratory virus has affected our family, because we know that we could spread it to their family. In fact, this is such a truism that it is accepted conventional wisdom, and I regularly have parents tell me of a cold or the flu that their children got it from a cousin and are “just passing it around” within the home. Barring some compelling microbiological difference, there is no reason to assume that it would be any different for COVID-19. Without definitive evidence, I simply do not find claims that ‘children don’t spread the virus’ convincing. It is well and good for people like British Epidemiologist Mark Woolhouse to say that there have been ‘no recorded cases worldwide of a teacher catching the coronavirus from a pupil’ (‘pupil’ is a British word for ‘student’), but aside from the problem of seeming to claim categorical knowledge, saying this in July when schools had been closed since the early days of the pandemic in March paints the risk as being low with much more confidence than the evidence warrants. But epidemiology is an applied science, and what we get wrong in our models and assumptions, the virus will correct for us in the bodies of students and teachers.
Nevertheless, the evidence was initially encouraging. A review of available evidence published on July 31st in the journal of the American Academy of Pediatrics asserted that “children most frequently acquire COVID-19 from adults, rather than transmitting it to them,” while acknowledging that this is a significant divergence from transmission patterns in other viral respiratory illnesses such as influenza. The authors concluded, “On the basis of these data, SARS-CoV-2 transmission in schools may be less important in community transmission than initially feared.” This conclusion is based on a study from Switzerland that tracked cases in 39 households, and another in China that included 68 children with confirmed COVID-19.
The same month, a study from Korea that traced contacts of 5,706 individuals with COVID-19 found that the highest transmission rates were for the household contacts of school-aged children with the virus, and concluded that “rates were higher for contacts of children than adults.” Because we are talking about COVID-19, this claim might be considered controversial. If we were talking about literally any other respiratory virus, every parent I know would respond by saying, “well… yeah.”
This finding, from a much larger study, provides a more balanced context for the major enigma from the AAP article; a German experiment that showed that viral loads in the nasopharynx (nasopharynxes? nasophari?) of children were as high as those in older people, “raising concern that children could be as infectious as adults” (Update: this result has since been confirmed by a study at Massachusetts General Hospital released yesterday, August 19th, which actually found viral loads in children with COVID-19 that were higher than that of severely ill hospitalized adults). The AAP article offered a few possible explanations for why this did not line up with the reassuring findings from the small epidemiological studies they reviewed. First, because children are more frequently mildly symptomatic or asymptomatic, releasing fewer infectious respiratory particles during their illness compared to adults. Sure; but adults don’t generally pick their noses and then touch every single muffin before deciding which one they want for breakfast. Maybe with this disgusting example from my life this morning in mind, the AAP article added, “Another possibility is that because school closures occurred in most locations… most close contacts became limited to households, reducing opportunities for children to become infected in the community and present as index cases.” And if that is the analysis of the most optimistic academic article on reopening schools I’ve seen yet, what will be the conclusions of the epidemiological studies from 2 months from now?
Are we actually seeing COVID-19 cases transmitted by children? The second type of data reveals yet another benefit of pathologic procrastination, because if I had written this a month ago we wouldn’t have some of this data at all. A recent analysis showed a surge of nearly 100,000 new pediatric COVID-19 cases in the latter part of July, prompting Pediatric Infectious Diseases specialist Dr. Sean O’Leary of Children’s Hospital Colorado (where I did all of my pediatric rotations in med school) to say “I think it’s showing that, yes, kids can get infected and can spread the infection.” This trend continued this month, with 75,755 new cases from 7/30 to 8/13. To put this in context, that means that nearly half of US COVID-19 cases in children have been confirmed in the last 4 weeks. Still, while some school-related activities and sports camps were happening over this time frame, this was before most schools actually reopened; once they do, these numbers may end up looking small. In places where they have reopened, we have read about high schools, middles schools, and kindergartens shutting down, quarantining massive number of students, or further delaying reopening due to large numbers of exposures to the virus and increasing numbers of confirmed cases among students and staff. This is mirrored in other places where young people are together en masse. University of North Carolina at Chapel Hill has switched entirely to online classes (and now Notre Dame and Michigan State) for the semester due to multiple clusters of transmission on campus, and we have read reports throughout the Summer of camps closing due to massive outbreaks among campers and counselors.
More to the point, I see this all the time. I’ve evaluated hundreds of patients for COVID-19 over the past several months, and there has not been a strange, unexplained phenomenon of patients not getting sick from their kids. I know there are some people who will never believe in COVID-19 transmission in children from studies in Korea that demonstrate thousands of cases; so I’ll just tell you now, I’ve personally seen many people who got COVID-19 from their children. We’ve seen children stay with cousins who tested positive, and then bring the infection to the adults and other children in their own household. We’ve seen families of 5 or 6 all test positive for COVID-19 after one of the children developed symptoms first. I haven’t seen any teachers get COVID-19 from a student; but I don’t think any of our local schools are actually open at this point. But transmission from children is happening and has been happening, and as much as we all wish against it, there is simply no chance that we won’t see community transmission clustered around schools once they are reopened.
Yeah, but children aren’t at a high risk from COVID-19, right? The inevitable questions is, so what? Aren’t kids immune? Or if not immune, at least far less susceptible to COVID-19 than adults? To some degree, the answer is “yes, thank God.” If this were the Spanish Flu of 1918, which disproportionately killed children, our society would not even be dreaming about reopening schools. As a parent of four small children, the fact that children are relatively safe from the virus has been the main reason I have felt comfortable seeing large volumes of patients with COVID-19-like symptoms daily over the past several months. As we discussed in the article addressing the America’s Frontline Doctors video, and again when discussing misinformation around COVID-19 and Human Trafficking, we don’t actually know the exact mortality rate among children. We do know it is much lower than for other groups.
My 5 year old son is 64x less likely than me to die from COVID-19, and 12,364x less likely to throw out his shoulder playing catch.
We also know it is not zero. While 20 of the states included in the latest analysis by the CDC reported zero child deaths, the rest reported at least one, and the mortality rate was as high as 0.6% in confirmed cases. The state with this frighteningly high mortality rate? Texas. Now before we break out our calculators and start to panic at the realization of what a 0.6% case fatality rate in children means, this is definitely an outlier (and I believe drastically overestimates the actual infection fatality rate in children), and of course it only includes identifiable cases; this mortality rate still cannot account for asymptomatic cases or minimally symptomatic children who don’t get tested. Nevertheless, not-zero multiplied by a lot is still a lot, and there is reason to expect that the 400,000 child cases of COVID-19 in the US so far may soon be a drop in the bucket. Some of the children who become infected over the coming weeks and months as schools reopen will, in fact, die, and for many of us who are affected by these deaths, this pandemic will no longer seem to have miraculously ‘spared children’ the way it has over the past 6 months with schools closed and children mostly kept at home.
But more importantly, death rates do not tell the entire story. While we have seen few child deaths, we have seen many children hospitalized for COVID-19, and an analysis of hospitalizations published just last week reveals that out of all hospitalized children with COVID-19, about one-third require ICU level care (though require mechanical ventilation far less frequently than adults). There are many ways to explain and understand this data, some of which are included in their analysis and some of which aren’t; but their conclusion is 100% spot-on:
“Children are at risk for severe COVID-19. Public health authorities and clinicians should continue to track pediatric SARS-CoV-2 infections. Reinforcement of prevention efforts is essential in congregate settings that serve children, including childcare centers and schools.”
Dr. Lindsay Kim, et. al
Finally, at the risk of sounding like a broken record, we aren’t actually most worried about the kids. If you look back at the chart from the CDC above, the groups that we are worried about most are the ones who are 1,400 times, 3,500 times or 10,000 times more likely to die from COVID-19 infection than school age children; their older parents and grandparents. Without any conclusive evidence that children ‘can’t spread the virus’ and more than enough compelling data that they can, we have every reason to believe that the population at greatest risk from reopening schools will be the grandparents of school-age children, not to mention older parents, teachers, and educators. As a society, we are now in the impossible position of choosing whether our children will forego being educated, socialized, fed, and nurtured inside of schools or whether they will be exposed to a deadly virus (soon, two deadly viruses; flu season is coming) that they can bring home to vulnerable family members.
Is it worth the risk?
Answer: I have no idea.
Child abuse So we know that the COVID-19 pandemic is going to get worse when schools reopen, but we don’t know by how much; and the other side of the equation is the risks associated with not reopening schools, which go far deeper than a semester or two of stymied educational attainment and missing out on the various intracranial and orthopedic injuries associated with high school sports (yes, I was on the Quiz Bowl Team. How did you know?). Since the beginning of the pandemic and the early closing of schools, cancelling of Summer programs and camps for children, and other mitigation measures that meant keeping children within the confines of their homes and family circles, we have been talking about, writing about, and worried about the possibility of child abuse and neglect going up during this crisis, especially when combined with unemployment, increased stress and anxiety, and grief related to the pandemic. And while this has been written about extensively by child advocates and physicians (like myself) who are also very concerned about the very real threat of COVID-19, it has also been used, similar to the issue of human trafficking, by people whose only real goal has been to diminish the threat of the virus and fight against any and all mitigation efforts.
So let me be clear. There is something gross and disturbing about people who have done everything within their power to make the pandemic worse, from neglecting social distancing to spreading misinformation and fighting against mask wearing, now saying that it is the people with legitimate epidemiological concerns about reopening schools who don’t care about child abuse. If it weren’t for people like this, we would be in a position to reopen schools much, much more safely and mitigate both threats more effectively. I deal with child abuse and its ramifications every day of my life; peopledon’t get to use it to try to give their deliberate pattern of denialism and irresponsibility throughout this pandemic the moral high ground. Reopening schools in the middle of a pandemic is an incredibly complex and difficult decision; but we are in this position, at least partly, because of them.
Well, so much for not getting myself into trouble.
The question of child abuse during the pandemic is one that remains unanswered. We all intuitively feel the danger of having children at home more and not having teacher’s eyes on children, especially in the midst of all the other risk factors we mentioned above. We all know of cases where a teacher or other educator has been the key person to report an abusive or neglectful situation and allow social services to intervene; I have seen this happen myself. But the idea that keeping children home from school will lead to a drastic rise in missed child abuse cases may overestimate the efficacy of the systems we have in place to report and investigate child abuse under normal circumstances. An in-depth article from The Marshall Project provides a careful analysis of the dynamics of mandated reporting, and while I think this is still an essential function of teachers, articles like this one from Mother Jones that list the huge drop-off in reports of suspected child abuse following school closures in March may be engaging in sensationalism; the vast majority of calls are not found to represent confirmed child abuse or neglect, and saying that, for instance, Illinois officials “received 6,672 reports of abuse in the week before the governor’s order to close, and 3,675 in the week after” does not mean that 2,997 abused or neglected children were missed.
There’s a balance here; early detection is the key to protecting children in child abuse situations, and there have been some reports by ER physicians that while the numbers of children presenting for child abuse are going down, the cases they do see seem to involve more severe or extensive injuries. Intuitively, we may believe that this is because of school closures… But most of this pandemic has so far taken place during months when schools would have been closed anyway, and it seems every bit as likely that the worsened severity of these child abuse cases is due to the other pressures of the pandemic not related to schools, like stress and anxiety and economic hardships. As the article above points out, we saw similar increases in child abuse severity during the 2008 recession even without school closures. Moreover, the long-held belief that child abuse peaks at all times children are home from school – the Summer, Christmas break, etc- seems to be a myth, and we are left to conclude what we really should have known already about the causes of child abuse; that they are complex. Blaming school closures for child abuse ignores this complexity in favor of a narrative that only seems to make the decision to reopen schools easier.
Other risks to children due to school closures I have a friend who spent his entire Fall and Summer, before leaving a few weeks ago for Physician Assistant school, trying to get food to thousands of children who normally rely on school breakfasts and lunches for a substantial part of their weekly nutrition. I should note that he was working with an organization; he wasn’t just making tons of sandwiches and then driving around handing them out across Texas and Louisiana. Without people like Dustin and organizations like Texas Hunger Initiative, many of those children would have faced significant nutritional deficits throughout this pandemic, and many children across our country don’t have access to programs like this. Moreover, school is not just a center of learning; many essential services such as counseling, speech and physical therapy, and support for learning disabilities and learning disadvantages occur within school walls. Moreover, the families who have least need of these services and the least reliance on school lunches are also the families that are most likely to have educational books in the home, stable internet and redundant internet-capable devices that can be used for distance learning, and other privileges that allow them to engage with learning resources regardless of the status of in-person school. The real threat to education posed by the pandemic isn’t the risk of students missing a year of school across the board (what, are we trying to beat the Russians to the moon?), but the risk of perpetuating and amplifying educational disparities.
But to make things murkier still, those are also the same students that are themselves most likely to become seriously ill from COVID-19, and whose parents and grandparents are at the greatest risk from the pandemic, due to healthcare disparities that often cut along the same racial and socio-economic lines as educational disparities, due to the same historical, systemic injustices. I hope you didn’t come here for answers; it really feels like we are stuck between a rock and a hard place, and the only certainty is that the families and children in our society who are already the hardest pressed on all sides at baseline will suffer the most dire consequences from whatever decision we make. Trying to correct this and share our portion of the burden should be at the forefront of whatever policies or personal decisions we make going forward.
What can we do as parents?
Be responsible I hesitate to put this one first because I realize it might sound accusational. Please look at the section heading; ‘what can we do as parents’; please understand that I’m including myself in this category (since I am not an educator or a society) and preaching this mini sermon to myself as well. Nevertheless, this is not an admonishment but a plea, to all of us, to take this virus seriously. As a primary care physician who sees many children, I have some version of this conversation a few times a week:
Me: Good morning, tell me what brings you guys in today. Parent of child: The school called this morning and said he had a fever of 119. Me, panicky: Wait… 101.9? Parent of child: Right. Me, less panicky: Whew… Ok, so when did his symptoms start? Parent of child: He started with a cough 3 days ago and felt warm last night, but I didn’t have a thermometer. They checked him at school today and called me.
As a parent I’ve done this myself; not just misspoke and said the wrong temperature because I had been up with a fussy child all night, but also sent my child to daycare or school because I didn’t really believe they were sick and I was able to rationalize away their symptoms. I’ve received that phone call before; your 2 year old has a fever at parents-day-out, your 5 year old threw up at Vacation Bible School; come and get your child. And the thing is, out of anybody, I should really have known better. But some children have minor coughs and off days so often that under normal circumstances playing a game of chicken with the symptoms and letting the school or daycare be the ones to make the final call that they are really sick is understandable. Not justified, but understandable.
These are not normal circumstances.
As parents, now is the time to take those minor symptoms more seriously and call your PCP or bring your child to their doctor for milder symptoms than you might have otherwise; or even just to keep them home for a day and monitor their symptoms to see if they really do develop into something serious. This is especially important if your job provides sick days or personal days and you have HR policies and supervisors that don’t penalize you for actually using them, which is a privilege so many people simply don’t have. A certain percentage of those runny noses and mild coughs are going to be COVID-19; better my child stay at home and me call in sick, than him give it to a classmate whose parents’ only option when he becomes ill is to leave him with a grandmother already in poor health. As a community, we have to take the responsibility of protecting other people’s children, and families, as seriously as we do the responsibility of protecting are own; and the time to start that is right now.
Consider alternative schooling/home schooling/schooling at home Homeschooling has always involved a good deal of privilege. I say that as someone who homeschooled until 8th grade, whose wife was homeschooled through highschool, and who(se wife) currently homeschools our children. We did not grow up wealthy and my mother enjoys working (and started working again once we had graduated), but my parents made more sacrifices than I realized at the time to allow her to stay home and teach us, and I’m incredibly thankful for that. Most of the homeschooling families I know (and we know a lot) are not wealthy; keeping one parent at home to teach means financial hardships they wouldn’t have to bare otherwise. And the sacrifices aren’t just financial; my wife has left hobbies unpursued, books unread (and unwritten, if I could ever get her to write that series of children’s books), and a nursing career she loves temporarily on hold, all to teach our children at home.
But the fact that we canchoose to make those sacrifices in the first place represents an awful lot of privilege, and there are many, many families for whom homeschooling is just not a viable option. Under normal circumstances, homeschooling is a hard decision for us. We believe in the public school system, and we realize that keeping our children at home means our voices aren’t contributing to the PTA, advocating for issues at the local elementary school or before the school board, or supporting the teachers and students and families that our own children would be interacting with every day. We try to be involved in and advocate for our community in other ways, but there’s no denying that we are less effective in this by homeschooling. It also means that our children miss out on opportunities to show love and kindness to people outside of their family circle every day. Sure, I guess there’s a possibility that my 8 year old would be the Regina George of the local 3rd grade or my 5 year old would be the Flash Thompson of Kindergarten, but I have enough pride as a parent and faith in my kids that I think it more likely they’d be an influence for good than otherwise. I think it’s fairly certain that somewhere in town an 8 year old is deprived of a best friend because my daughter is doing school at home with us.
So far we still feel that that’s the best decision for our family, but it’s definitely an ongoing discussion each and every year. But right now, with COVID-19, the privileges inherent in schooling at home can actually be used on behalf of the other children and families, and the teachers, at the local schools that our children won’t be attending. Each child that can safely be kept at home and successfully educated this year through distance learning or homeschooling makes it that much easier for teachers to maintain social distancing in the classroom, that much safer for teachers and other school staff in terms of transmission risk, and that much less likely that other students will become infected and bring the virus home to parents and grandparents. This year, at least, homeschooling was an easy decision for us; and if you have the resources, financial and otherwise, to successfully school at home for a semester or a school year, this is definitely the year to give it some careful consideration.
What can you do as an educator?
I just want to say, at the outset of this section, that I think that asking teachers and school principals to do the work of epidemiologists and government health officials and keep children safe from the virus is pretty lame. I am sorry that you are in this position; I hear your stress. I taught high school physics and physical science (and theatre!) for 8 months after college, and realized it was not something I was good at and certainly not something I could do for the rest of my life; I admire anyone who does it, and particularly anyone who does it well. When I left teaching to go to med school, I knew on some level that I was signing up to be on the front lines of any global pandemic that might happen to come our way; but when you became a teacher, you weren’t. So even though this shouldn’t be your job, I’d like to share some advice for how you can help keep yourself and your students, and their families, safe. Being months late with this post, I’m certain that any educators who might read this are already far along in the planning and implementation of their COVID-19 response plan, and those who have reached out to me have shared incredible, creative ideas to keep themselves and their students safe that I never would have thought of.
Seek counsel A physician friend and residency classmate reached out to me in May when her child’s school asked her to give recommendations on reopening school safely. At the time we were operating under the assumption that the pandemic would be well in hand by the Fall, and that the biggest concern would be preventing a second surge. Clearly, this is no longer the case. Nevertheless, we brainstormed on the best and most practical ways to reduce transmission between students while interrupting their education as little as possible. We had ideas for reducing transmission during PE, music class, alternatives to all school assemblies, managing bathroom breaks and lunch and hallways during class changes. I briefly considered sharing a big list of ideas here, but the reality is that the changes that would help will be different for every school, every building and class schedule, and every situation. You know your school, I don’t; your ideas will be better than mine. And better still will be your ideas with the input of a physician or epidemiologist or other medical professional who has an intimate understanding of infection control and viral transmission and who takes the pandemic very seriously. Reach out to one in your community and ask them for help; they have a vested interested in keeping your school safe, even if they don’t have a child that attends there. Most would be honored to help with this work (and would be even more honored if you then actually followed their advice!). This works best as a two-way conversation; the medical professional is going to see opportunities for changing processes and physical spaces and creating a safer school that wouldn’t occur to someone without their education and experience; and you, the educator, are going to be in a position to tell them which of their ideas will work for your students and your classroom, and which need to be modified or scrapped. Then, when things have calmed down and we’ve finally got this virus under control, you can reach out again to seek their advice on deescalating the measures you’ve put into place and slowly returning to normal. And then later in the year when you need someone to speak to your students about going into healthcare at the next career day, guess who you are gonna call…
Get clever As I’ve worked on this post, I’ve heard from teachers whose schools have implemented some incredibly clever and ambitious ideas. I’ve been told about schools keeping kids in cohorts throughout their entire daily schedule, even organizing sports activities and lunch and recess around these small, consistent groups. I’ve heard of multi-grade classrooms to keep siblings, cousins, and neighbors together, limiting the network of contacts per child. I’ve heard of classroom modifications, curriculum changes, changes in sports schedules, and restructuring of school-wide events. I’ve also heard of schools that are doing next to nothing (besides enforcing stricter social media policies for teachers), and teachers who are scrambling to keep their own classrooms as safe as possible within a school that is essentially denying that any danger exists. I’ve even heard of teachers taking a break from teaching this year because they couldn’t see any way to keep themselves, aged parents, or at-risk household contacts safe while being in the classroom every day. As a society, there is no denying that we’ve failed these teachers.
The classroom or school-wide plan that protects children from getting and spreading SARS-CoV-2 better than any other plan in the country is probably not “just keep children 6 feet apart,” “put up plexiglass between desks,” “masks at all times,” or “check temperatures at the door,” though it almost certainly will include some of those components. No, the best plan has probably already been devised by some creative, well-informed, scientifically minded out-of-the-box thinker somewhere. With any luck, it has been listened to and implemented; but unfortunately, too often it will probably be ignored by decision makers for being too weird or wonky, too conceptually challenging, or too inconvenient to implement. But now is exactly the moment that we need those creative and wonky ideas, because the stakes are too high to just hope it goes away if we can just ignore it hard enough.
Can your track or cross country team set up a Fitbit team challenge instead of practicing together after school?
Can you use pegboard and cardboard and printouts (that you’ll have to buy yourself, I realize) mounted on the walls of your STEAM class to make an interactive workspace that keeps students facing toward the walls for most of the class period instead of toward the teacher or across a table toward each other?
Or better yet… Also, is this me? I pulled this image off of google, I don’t remember this at all, and I didn’t wear glasses at that age… But from this angle I feel like there’s still a good possibility that that’s me.
Can you recruit that pop culture savvy AV kid (this is an oxymoron; none of us AV kids are pop culture savvy) to create some awesome Cast of Hamilton style video mash-ups so that your Zoom band rehearsals are Youtube worthy instead of unmitigated disasters?
If this is your music class, I’d be willing to substitute.
Can you use your school’s external doorways and internal layout to create a continuous one-way circuit during classroom changes, like Sylvester McMonkey McBean’s star belly tattoo machine?
Bad social distancing there in the middle, but pretty good otherwise.
I don’t know. Some of those ideas are probably things you’re already doing, or that you’ve already thought of and abandoned because there was just no way to make it work at your school or in your class. That’s my point; decreasing transmission right now is going to mean sound epidemiology principles combined with creative teaching ideas and applied to your individual teaching situation. Even for those schools that are very well prepared already, we have to keep in mind that no battle plan survives first contact with the enemy; once schools do reopen, one size fits all solutions or rigid adherence to plans made over Zoom during the Summer are likely to mean insufficient protection and excessive interruption of learning if they aren’t reevaluated and readjusted. It’s a lot, I know; but all of us fighting to stop misinformation and promote mitigation efforts and health behaviors that would have slowed the virus have, so far, pretty much failed; so now it is apparently your problem to deal with. You need bold strokes because we’ve failed to convince more folks.
Advocate, advocate, advocate Me using my blog to tell educators to advocate for each other, their students, and their communities is like hospital administrators pulling doctors aside to tell us how to treat patients (oh wait, that happens literally every day); this is clearly something you are already doing and is, in fact, a major part of your job. Nevertheless, this is now a more important job than ever, because there are so many stake-holders when it comes to reopening schools and not all of them care about the health of your students or their families.
In a moment we are going to talk about what the rest of us can and should be doing to support you during this time. Please keep lending us your voices. I know it feels like society has decided to ignore the collective and individual voices of teachers (I’m a doctor who writes a blog on medical misinformation; trust me, I feel you), but without understanding what’s happening in your schools and classrooms the rest of us have no hope of advocating for you in the ways you need most. We want to help. If your school has enforced social media policies that don’t allow you to say when you are concerned about the safety of your colleagues or your students, find ways to get that information out there anyway. Be sources of good health information and fight misinformation in the classroom every day. One thing I’ve heard from teacher after teacher is that their students have been amazing; wearing masks at a high rate without grumbling or complaining, practicing good distancing in the classroom, and in general being the best of us in taking the pandemic seriously. That is going to fatigue over the next few months without your example and reinforcement, but you are in a much better position than any of the rest of us to help lead this generation in doing the tedious day-to-day epidemiology work that we, their forebears, have failed at.
What can we do as a society?
Fight the virus on every possible front. If I had written this post a month ago when I should have, I’m sure I’d be saying that the best plan to reopen schools safely would be to spend the next month doing everything in our power to decrease community transmission, and then only reopen schools once we knew it was as safe as we can reasonably expect (for a more epidemiology minded discussion of what that would look like, check out Waco Epidemiologist Emily Smith’s post on “Can we open schools safely?“). In fact, this is still what I think, and if I thought there was any chance of getting it to work, I would be strongly advocating for schools to delay reopening while mitigation efforts were redoubled. In cities like my own, where our testing positivity rates have been steadily declining over the past several weeks, this might not even take that long. But if we’ve learned anything through this pandemic it’s that we cannot rely on strategies that require small individual efforts but a large degree of buy-in. So here we are, with schools reopening in the midst of a pandemic, and bracing ourselves to see how much worse it will get as a result. But as one comedian said, I guess all the bad decisions we’ve made up to this point have made this a good one?
But even if school reopenings aren’t going to be delayed until a set community prevalence or test positivity rate is reached, we can still make every effort now to decrease transmission, especially with a few weeks still to go before all of our schools are opened. We need to be practicing good social (physical) distancing and mask wearing. We need to be participating in the work of informing our own contacts when we are diagnosed with COVID-19 since our public health sectors simply have not had the manpower to keep up. We need to practice diligence in our personal mitigation efforts, even though we are all incredibly fatigued from thinking about this virus and how it has affected our lives. As a society we claim that the safety of our children in schools is one of our highest priorities, and we take massive steps to protect them. Yes, I know there are some pretty obvious areas where we haven’t been taking common sense measures to keep kids safe in schools, but we do a pretty good job of slowing down to 20 MPH and putting down our cellphones when we drive through a school zone, and we make sure kids have those safety scissors that won’t actually cut anything just to reduce the chances of one of them losing a finger. Right now, the efforts you can make to reduce community transmission- social distancing, washing hands, getting tested if you are ill, and wearing a mask- are the efforts that will keep children, their teachers,and their families safe in the coming weeks.
What even is this?
Extend Trust We’ve talked a lot about the role of educators and parents in fighting the virus and keeping our schools safe, but the reality is that those groups are limited in the actions they can take, with freedom from judgement and repercussions, without buy-in and affirmation from the rest of us. It’s well and good to tell parents to keep their child home for a day when they think she might be getting sick, but this requires policy changes that refrain from punishing parents for taking such a responsible action and trusting them to occasionally know, without a doctors note, when their child is too sick to come to school. Yes, that trust will be taken advantage of by some families, nobody knows it better than me; but right now I have visits every single week where parents know their child just has a mild illness and shouldn’t be in school, but had to come to the doctor to get a note for school and work; in the eyes of the school and their employer, they are guilty of faking an illness until my note proves them innocent. In the midst of a viral pandemic is exactly the time to reevaluate the wisdom of such policies and return that trust back to parents; and then keep it that way, because even aside from COVID-19 this dynamic is already dangerous during every single flu season.
Also, let’s get rid of perfect attendance awards.
Lower Our Expectations
And the same is true for our expectations of our teachers and school administrators. Being a high school physics teacher was my first real grown up job, and being a doctor was my second. There are plenty of similarities between the two, but one of the most salient is the constant feeling of being asked to do increasingly more with an ever decreasing amount of time and resources. As a primary care doctor, this often means walking out of one patient room and into the next from 8:00 to 12:30 and then from 1:00 to 5:15, providing extensive evaluation, compassionate listening, diagnosis, treatment, and teaching to each patient within a 10-15 minute window, and being expected to complete the documentation and respond to phone messages and refill requests in the often non-existent minutes “between visits” (we often don’t have time to go to the bathroom or get a drink of water “between visits”). As a teacher, it meant trying to make it through more curriculum than could possibly be covered in a year, prepare students for standardized testing, regulate behavior in the classroom, navigate and manage the interpersonal dynamics and conflicts of 13 years old, and provide counseling and interpersonal support for young people in some of the most formative and challenging years of their lives. Oh, and submit grades, which is just… I think I’ve still got some ungraded quizzes in a manila folder somewhere, and I haven’t taught since 2009.
Add to all of that the expectation that teachers will now be fighting COVID-19 transmission on the front lines of the pandemic and, somehow, teaching both in-person and online classes simultaneously, and you’ll realize what a sick joke it is to say that any adjustments we make to our expectations would be “lowering” them. We are asking so much of our teachers, and this year we are asking even more; we need to be comfortable, as a society, with accepting that less can be expected in terms of our students’ educational progress between now and May 2021 compared to years past and years to come. Somehow, in all of these discussions about reopening schools, I’ve missed all of the articles calling for a hiatus on standardized testing (or at least eliminating punitive measures related to those test results), on colleges using alternative evaluation methods for graduating seniors, and on discussions of exactly what percentage of the standard curriculum we expect teachers to be able to cover this coming semester; 50%, or just 35%? Rather than lowering our expectations, what we would really be doing is finally valuing teachers’ time and acknowledging their efforts, and recognizing that since most teachers are already working at maximum capacity as-is, we have to be willing to let something go when we add something on. If we are saying that schools need to be reopened because it is necessary to keep kids safe, detect cases of domestic violence early, and keep children from regressing academically, we need to realize that those goals do not logically imply that we can also somehow expect teachers and students to maintain the same pace of academic attainment, and that that is no longer our primary goal in reopening schools.
Be ready to pump the brakes I think this is the biggest one, and it’s going to take an awful lot of honesty when we look at the epidemiology data that emerges over the coming weeks and months. As schools reopen around the country, we have to fight stronger than ever against misinformation. We will hear that any increase in cases is due to increased testing, even if it is mirrored by an increasing test positivity rate and hospitalizations. We will be told that the overall mortality rate is dropping and it “isn’t as dangerous as we were told,” because the virus is less dangerous for children than older adults, and seeing a decrease in the overall infection mortality rate is a natural artifact of an increasing number of cases in children and adolescents- even as teachers, school staff, and family members of students are hospitalized and die due to those exposures. As flu season approaches, we will be told every possible version of doctors lying to diminish the flu and inflate the pandemic or misattributing flu deaths to COVID-19 to hurt the economy or this or that politician, as though it mattered which preventable deadly respiratory virus your family member died from.
We have to be willing to cut through the noise and look carefully at the trends in cases in our community and ask continuously whether the risk is still justified today. It would be great if I were completely wrong, if cases continued to decrease even when schools start back in earnest; but it’s hard to imagine that happening, and the decisions are likely to get even more difficult, not less, from here on out. We need to drop our agendas and our egos and our politically motivated methods of interpreting data and meet the emerging information with intellectual honesty. We need to consider school closures and audibles and readjustments as the necessary and humble work that the pandemic requires of us, and work together to keep our kids, our teachers, and our communities safe.
I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now in 8-bit Color!
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Question #3: Isn’t a surge a good thing since it will give us herd immunity?
The concept of herd immunity, susceptible persons being protected from infectious diseases by a sufficiently highnumber of people in their community already being immune, was controversial even before the COVID-19 pandemic. I don’t mean it was a controversial area of epidemiology; the science behind it is very well established and pretty straightforward (and if you are going to read about the eradication of smallpox from that link, you should also read about a man called Onesimus, a slave in Boston whose knowledge of West African inoculation saved hundreds or thousands of lives and paved the way for Edward Jenner’s eventual invention of vaccination techniques). I mean it was something that we’ve had to argue about constantly in recent years because the anti-vaccine movement uses herd immunity as one of its many arguments against vaccination, while at the same time undercutting its effectiveness by seeking to decrease the number of people who are immune through being vaccinated. The idea is great in principal; just weather the storm now and then we will all be safe from the virus forever. The problem (one of the problems, for there are numerous) is that we don’t yet know exactly what percentage of the population needs to be immune to confer protection to everyone else. Most estimates have put this number somewhere between 60-70%, but a recent model published in Science estimates it at a much more attainable 43%. These numbers are based on several parameters that tell us both how easy the virus is to spread and whether certain activities, situations, or even individuals are more likely to spread it than others (you can read about the median reproduction value and dispersion factor if you want to dive a bit more into the math of it all). Because these numbers are incredibly hard to definitively determine in the midst of a pandemic, any percentage we arrive at is going to be a best guess; an estimate derived from multiple assumptions that will only be proved wrong if many more people get very sick even after we’ve achieved the required numbers for herd immunity. Herd immunity is a gamble because Virology, during a pandemic, is an applied science; the virus will correct all of our miscalculations and false assumptions for us. (other questions, such as whether immunity to SARS-CoV-2 is indeed long-lasting and whether the virus will mutate in such a way that it causes future outbreaks despite our acquired immunity are also important, but outside the immediate scope of the discussion).
*This is from early in the pandemic, but a great visualization tool
But even more important than the difficulty in calculating the necessary percentage of people being immune to confer protection to everyone else is the question of how dangerous it is to get there in the first place. Let’s talk about measles for one moment. We know that the herd immunity required for measles is somewhere around 93%, which is part of the reason we have seen outbreaks of the disease recently in areas that have a substantial anti-vaccine sub-culture; it isn’t hard to fall below that number. Let’s say there wasn’t a Measles vaccine; that means 93% of people would need to develop immunity by living through the disease. With modern medical advances the case fatality rate for measles is a lot lower than it used to be, but it is still around 2.2%. This means that in a country of 330 million people that had no immunity to measles, 306 million would need to contract the disease to confer herd immunity to everyone else; of those, 6.75 million would die, not to mention the longstanding residual neurological deficits and other health complications in tens of millions more. Without effective vaccination, herd immunity would simply never have been an option for Measles; the cost in human life and suffering would just be too high. But what about COVID-19? We know that SARS-CoV-2 is thankfully less contagious, and we believe less deadly (see the last post for a discussion on this) than measles, but is it enough to make herd immunity a viable option? Let’s apply those same calculations based on the current estimates we have for infection fatality rate. If we accepted a 1% death rate estimate, then to achieve the widely accepted 60% mark for herd immunity we would see 198 million cases and 2 million deaths, while if we accepted the recently released 43% estimate and assumed an even more conservative 0.5% death rate, that would be 709,500 deaths; and neither accounts for the longstanding health deficits or the cost in human suffering of those who survive, or the other deaths and suffering that come with an overwhelmed mid-surge healthcare system. Now, could we devise some clever epidemiology strategy that uses emerging data about the already-immune, super-spreaders, natural resistance, new drug therapies, contact tracing, and protection of the most vulnerable? Of course; assuming that we could get a high degree of buy-in (we can’t even get people to wear masks), that’s exactly what we are all hoping for. But that’s not ‘herd immunity’, and it’s clear that the cost in lives and suffering from a “just get it and get it over with” ‘strategy’ would be astronomical even with our most optimistic estimates. Trust me, I’m tired too; I completely understand the pull towards a roll the dice approach that just gets this over with and lets the chips fall where they may; that approach completely appeals to my intellectual and emotional fatigue. But the longer we can work together to flatten the curve, the more time we create to discover those new therapies, improve our understanding of the virus, and collect high quality data about transmission and vulnerability that can help us develop novel, strategic mitigation approaches (which would probably incorporate something like herd immunity); and we are already seeing the benefits of the work of this kind that we have done so far as a society.
Question #4: What is the RECOVERY Trial?
(Confession: nobody asked about this, but I’m going to write about it anyway)
The RECOVERY Trial is a randomized(poor British researchers spelled it wrong) clinical trial out of Oxford that has shown benefits from using low-dose dexamethasone (a cheap and readily available steroid) for hospitalized COVID-19 patients on oxygen or on a ventilator; you can read a more detailed analysis of the trial from First10EM. This is still in the peer review process but results have been incredibly promising; the study showed a relative decrease in mortality of 20% in hospitalized patients requiring oxygen, and up to a 35% decrease in patients requiring ventilator support. Unlike many of the drug therapies that have been touted up until now, this is based on a randomized trial and not on anecdotal evidence, so it is much more likely that these results will be reproducible when used broadly. Already this has become the standard of care in the hospitals in your city, and if we see these results persist with widespread use it has the potential to save tens or hundreds of thousands of lives. I wanted to write about it for two reasons. First, I want to call on us all now to not let this become the next hydroxychloroquine. The study has established the benefits of this drug therapy only in a specific group of people; hospitalized patients requiring oxygen or ventilator support. They also studied hospitalized patients who were not sick enough to need oxygen, and it showed no benefits whatsoever. There is no reason to infer that this medication is protective in those without severe symptoms or in asymptomatic individuals, and so there is no reason for individuals to ask their doctor for an outpatient prescription or for pharmacies or clinicians to stockpile the medication as we saw done with hydroxychloroquine. We can be thankful that we have at least one helpful medication for our sickest patients without that immediately translating into figuring out a way to get it for ourselves whether it would actually help us or not. And if peer review and follow-up studies and the increased clinical experience that comes with widespread use of dexamethasone ultimately shows that it actually isn’t helpful for COVID-19, that will be tragic; but we should all understand now that that is just how science works, and won’t be part of some big government conspiracy to prevent people from getting the medication, just as it wasn’t with hydroxychloroquine.
But even more importantly, I wanted to talk about the RECOVERY Trial because it illustrates exactly what it looks like to fight this virus by engaging in mitigation and flattening the curve. Since April people have been saying (and we have all been feeling, to some degree or another) that if a certain amount of death and suffering from the virus is inevitable, we might as well just get it over with. We have also heard the slightly more sophisticated position that as long as our hospitals aren’t overwhelmed and we aren’t running out of ventilators and other equipment and resources for sick patients, then we have reduced the danger as much as is helpful and anything more is unnecessary. The RECOVERY Trial is a powerful illustration of why flattening the curve is beneficial even beyond these important goals. If you had a severe case of COVID-19 one month ago and had to be on a ventilator, you would have been treated with hydroxychloroquine and not with dexamethasone; today, you would be treated with dex and not with hydroxychloroquine, and your chance of dying would be 35% less; and that doesn’t even take into account the less quantifiable benefits from all that your doctors have learned about this virus in the meantime. A month from now, with more high quality trials and more clinical experience, who knows what the new standard of care will be and how much better a very sick person’s odds of surviving the virus will be because of it. The reason I wear my PPE with every patient and am a stickler about fomites and transmission, the reason I wear my mask when I’m in public, and the reason I am writing from home instead of a coffee shop today and attended church online this morning, isn’t because I’m afraid of the virus; it’s because when and if (and for me it has always felt more like an ‘if’ than a ‘when’) I get COVID-19, I would rather be treated by doctors and nurses and respiratory therapists who have had ample time to learn how to fight it, who have perfected their approach to ventilator settings and other supportive techniques for this virus specifically, and who have access to medications that have been carefully studied and have been proven to be effective; and because Iwould like to have that knowledge base and those techniques and medications available if and when I have to treat you.
I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now in 8-bit Color!
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Question #2: Do antibody testing and asymptomatic cases prove the virus isn’t as dangerous as we thought?
Asymptomatic Cases
The short answer here is, yes. And also in a very real sense… No. When antibody testing first began to confirm that a certain percentage of people contracted the virus but never developed symptoms, or had symptoms that were so mild they failed to associate them with the virus (‘weird how my allergies just acted for a couple of days’), it was great news for everyone. What it was not (and I’ve been on this soapbox for a while now) was proof that the ‘experts were wrong’ about how dangerous the virus is. I’ve been reading every model and study and expert opinion about COVID-19 I could keep up with for the past 3 months, and I cannot tell you the number of times that physicians and epidemiologists and researchers have either implied or explicitly stated that the mortality rates we were seeing from the virus didn’t account for asymptomatic and minimally symptomatic cases. I’m no expert, but I’ve typed it more times than I can count myself.
Actually I counted; it’s been 6 times. That’s still a lot.
Those scientists anticipated that a certain percentage of the population would contract the virus but never develop significant symptoms, but had to work from the best numbers they had until such testing was actually available. And it’s a very good thing that those assumptions were correct, since the original case fatality rates we were seeing were in the civilization ending range of 8-15% in certain countries. If antibody testing had been developed and found only a negligible amount of asymptomatic and minimally symptomatic cases, it would be devastating news for everyone; not least for the doctors, nurses, epidemiologists, and others who have turned their lives upside down to fight the pandemic. Accounting for asymptomatic and minimally symptomatic cases would clearly yield a much lower death rate, but still firmly in the very, very dangerous range. For instance, large scale antibody testing in New York in April found antibodies in 13.9% of the population (WBUR has an excellent article picking through the wildly varied estimates of asymptomatic cases) , which reduced their overall estimated fatality rate from 6% to 0.5%. Many current estimates place the overall fatality rate between 0.5% and 1.3%. For a virus this contagious, these are still scary numbers. Even here at the end of June, many people are still wanting to compare this to the flu to dismiss the danger, even though these much lower death rate estimates are still 5 to 13 times higher than seasonal influenza’s commonly accepted 0.1% fatality rate, and even though the flu itself regularly threatens to overwhelm our healthcare systems. Please keep in mind that this is at best an apples and oranges comparison. We don’t routinely measure influenza antibodies to determine the percentage of asymptomatic cases, focusing instead on those who are symptomatic, and our death rates for flu are based on a totally separate set of calculations (I talked about this in more detail in my response to the Bakersfield Urgent Care doctors). If you want to compare oranges to oranges we can look at excess mortality for both viruses. Consider the graph below from New York State: the first cluster of red crosses is the peak of the 2017-2018 flu season, the worst flu season I have experienced since starting medical school; the second is COVID-19 during New York’s surge in April.
Not the Flu.
Before we move on from asymptomatic cases, we need to mention two more things. First, while knowing the overall infection fatality rate including data from those who never had significant symptoms is great from an epidemiology standpoint, it doesn’t mean that the case fatality rate for people with symptoms is a ‘fake number’ or falsely elevated. If you develop symptoms and test positive for the virus, and especially if you end up in the hospital, it would be small comfort to know that some people didn’t get sick from it at all. We still need to know what the specific risk is for people with symptoms, and for people with severe symptoms, in order to properly counsel those patients and to inform our medical response. Second, asymptomatic cases are a double edged sword; yes, it means that some people will become immune without actually getting sick themselves, but it also means that some people can spread the virus without ever knowing they’ve had it. We all need to exercise caution even if we don’t have a cough and fever.
I realize this is the same joke from earlier. I just really like it.
Antibody Testing
One of the problems in determining a final overall death rate (besides the fact that we are still in the middle of the pandemic) is the accuracy of antibody testing, since we have to rely on this to tell us how many people had the virus and were either asymptomatic or didn’t get tested for it at the time. And this in turn relies on something called the positive predictive value, how likely it is your ‘positive’ test result has really detected the antibodies, which depends both on how well the antibody tests are designed (and their not being fake, which is apparently a problem now as well), but also on the prevalence, or in this case cumulative incidence, of the virus. The higher the percentage of people who have actually had the virus, the more likely it is that a positive test really represents a true positive and not a laboratory error. It’s a relatively simple concept, but honestly it’s just unintuitive enough that I’ve struggled with it myself for years. Basically, every lab test has some degree of error; sometimes these tests will tell you that you have the antibodies when you don’t, and sometimes it will tell you that you don’t have them when you really do. The more rare the virus has been in your area, the more likely that your ‘positive’ test was the result of such an error instead of actually having the antibodies. Carry this to the logical conclusion; if you brought an antibody testing system back in time to last Summer when nobody had SARS-CoV-2 antibodies, or for that matter back to Medieval England, you would still have some tests turn positive; but they would clearly all be from laboratory error because the prevalence of the disease then would have been 0%. When doing these tests, we cannot ignore the importance of how common or rare the virus has been in the region where we are testing.
Still less useful than bringing Sony Walkman
Calculating positive predictive value based on prevalence can be done with just a few numbers (test sensitivity, test specificity, and prevalence) and the simple equation PPV = (sensitivity x prevalence) / [ (sensitivity x prevalence) + ((1 – specificity) x (1 – prevalence)) ] (Um, there’s also an online calculator if you’d rather follow along that way), and it’s always shocking to me how quickly the lab error for even very good tests becomes relevant when the prevalence of a disease is low. Most manufacturers rate their antibody tests in the extremely accurate range of 95-100% for both sensitivity and specificity (because of course they do); some have performed well in independent testing, but others not so much. Let’s use the online calculator (or the equation above, if you just really like that sort of thing) and plug in a few of these numbers.
Scenario 1: Post-Surge New York City, excellent quality antibody test.
Let’s say you never definitively got diagnosed with COVID-19 during the surge in New York, and wanted to get an antibody test to see if you have already had it and are immune.
This means if you get a positive results from this very accurate test done after your city has survived a severe surge, there’s still about a 17% chance you don’t actually have the antibodies after all.
I hope you guys are having as much fun with this as I am.
Same scenario as the last, but the quality of the test isn’t quite as good as the manufacturer funded studies seemed to promise.
Sensitivity: 88.6% (.886)
Specificity: 90.2% (.902)
“Prevalence”: 4.6% (0.046)
Results:Positive Predictive Value = 30.4%
At this point you are probably better off just switching the ‘positive’ and ‘negative’ labels on the readout…
Now, savvy statisticians will note three things in looking at the above numbers and playing around with the data. The first is that I’ve used the very antibody testing methods I’m questioning to fill in the prevalence, which is itself part of my calculations. Figuring out the real prevalence is a complex problem epidemiologists are still trying to solve; this is a simplification for illustrative purposes. But more importantly, you will notice that as the prevalence goes down so does the likelihood that a positive test was really positive; in fact, it drops quite precipitously, especially as you get below 5%. However, as the specificity– the likelihood that the test correctly calls a negative result negative– approaches 100%, the number of false positives actually drops to 0. If we want to make sure we never tell someone they are immune when they aren’t, we need a very high specificity; but because no test is truly perfect, this will mean some sacrifices in actually being able to detect the antibodies when they are there, which hurts our ability to accurately estimate the number of asymptomatic cases. To get a perfect specificity, you will lose some sensitivity, and vice versa; the right balance depends on what you intend to use the test for.
So all of that to say, when that antibody test you got comes back positive and the manufacturer says their test is “95% accurate,” you may be tricked into thinking it means there’s a 95% chance you really have already had the virus and now have antibodies against it. But they are only telling you half the story, and you either need access to some more data to make your calculations and determine the real positive predictive value, or at the very least you need to take it with a grain of salt and still exercise caution; especially if your area hasn’t actually had anything like a true surge yet. After all, only a great fool would accept what he was given, and you are not a great fool.
I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now in 8-bit Color!
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Question #1: Isn’t the rise in cases just a reflection of more widespread testing?
This is a question that has been on everyone’s minds since the very earliest days of our testing woes, back in March when we had barely any testing available. It has ranged from a very fair question to a rhetorical device for spreading misinformation, with at least one prominent political figure even seeming to say that it would be better if we didn’t test so much so that our numbers looked better. I honestly believe most people really are curious about the relationship between our testing numbers and our numbers of cases and are not asking to try to minimize the appearance of the surge we are facing in Texas right now. In one sense, we will always find more cases of a disease when we test for it than when we don’t; that’s a truism. But if we want to determine whether cases are really going up we can look at a few other parameters than the absolute number of positive tests that will inform our understanding of the ’75 new cases’ or ‘5,747 new cases’ we are seeing in the news and on social media each day (To go through these numbers I highly recommend you spend some time navigating the Texas DSHS COVID-19 Dashboard; both their case data and testing and hospital data sections).
The first number is the percentage of positive tests.Ever since testing became more widely available in April and we were able to shift away from testing only those with a high likelihood of having the disease and/or of developing complications, we have been testing essentially the same types of cases; people with some combination of cough, shortness of breath, fever, loss of taste and smell, etc. and/or known or suspected exposure to the virus. There are many causes of these types of symptoms, from allergies to other respiratory viruses to chronic conditions like asthma and COPD, and in our pre-surge days these explained the symptoms in the vast majority of people we tested. If you look at the Texas testing data from April you will see two things; an overall low number of tests (a very modest 5-10k per day) and a fairly high percentage of tests that are positive, between 10-14%. This reflects our very strict testing criteria at that time; we were only testing the people we already really thought had it. In late April and all through May we see an ever increasing number of daily tests and a falling rate of positive tests, a reflection of liberalizing testing criteria and strong evidence of overall low prevalence in our State. Throughout June, and especially over the last 2 weeks, we continue to see an increasing number of tests each day; but we are now also seeing our percentage of positive cases rising again. This isn’t because we’ve tightened up or restricted our testing criteria again; it’s because more people actually do have the virus.
Percentage of positive tests
This exactly matches my own clinical experiences; back in May I was testing for COVID-19 based on essentially the same criteria and clinical judgement I am using right now, but it was rare to get a positive case; I would know, because being told you have COVID-19 can be a very stressful experience, so I still personally call every patient I’ve tested who has a positive result in order to answer their questions and help them process that information. This past week I have had to make multiple of those phone calls daily and have been feeling the strain on my time that it has created. As a physician I was on the front lines in May just like I am now, and I can tell you that we are definitely feeling this surge in a way we didn’t then; it isn’t a statistical artifact.
The second kind of data that should inform our understanding of that increase in cases is the number of people who are hospitalized with COVID-19; and the number of people who are dying from it. A raw increase in cases without a change in the test positivity rate could certainly be explained by more widespread testing; but it could not explain why more people had severe enough symptoms to be hospitalized, and there is no question that we have seen an increase in hospitalized cases.
Hospitalizations
Many people will quickly point out that we don’t know what percentage of those people were hospitalized for COVID-19 related symptoms and what percentage just happened to have a positive test when they came to the hospital for other reasons. This is a seemingly fair argument on the surface, but it is guilty of two fallacies. First is the idea of COVID-19 infection being a coincidence that doesn’t effect the trajectory of someone’s chronic illnesses. For months now I have heard the argument that the people whom we know have the absolute highest risk of COVID-19 complications, elderly people with chronic heart and lung disease, have not died from COVID-19, just with COVID-19. Yes, they happened to have the virus but actually died, in large numbers, from their chronic illnesses all getting worse at the same time, during a surge in COVID-19 cases in their area. This is the tired conspiracy theory that doctors are misattributing the cause of death to inflate COVID-19 death numbers, and it’s one I’ve had to debunk over and over again on this blog; it willfully ignores the pathophysiology of the virus, the normal course of those illnesses, and the way that doctors understand and report contributing causes of death. The idea that we are suddenly seeing a huge uptick in COVID-19 hospitalizations as an artifact of testing patients when they come in and unrelatedto the virus itself is just another version of that same conspiracy theory. It’s also a very hypocritical argument, considering the types of sources it is coming from. One of the criticisms about mitigation efforts from the beginning was that people who needed care might not come in to the clinic or hospital because of fear of the virus; it’s a very real concern and a problem I’ve fought against daily as a physician, and have been writing about since my earliest social media and blog posts during the pandemic.
Their argument has been that telling people that the virus is dangerous and taking mitigation measures would discourage them from seeking care for conditions that were really dangerous, like congestive heart failure or blood clots in the lungs, because they were more afraid of catching COVID-19 at the hospital. Our argument has been that the virus is dangerous, and that it also makes congestive heart failure more dangerous and actually causes blood clots in the lungs, so we have an obligation to keep people safe from the virus and help them navigate when and how to seek care for other health concerns; it’s work we are doing constantly in our clinics and hospitals. Now these same sources are arguing that in the midst of a dramatic increase in cases and our first real surge in Texas, thousands of people with conditions that put them at risk for complications from COVID-19 suddenly aren’t worried about the virus after all and are all seeking hospital care at the same time, and just happen to test positive for the virus while they are there. There may well be some situations where this actually is the case, and people who were overlooked by our healthcare systems really are now getting very sick from their diabetes or coronary artery disease at the same time as our surge (you can only ignore a worsening chronic illness for so long before hitting a crisis point), but the idea that this would happen on a broad scale, all at the same time, and that enough of those patients would be positive for COVID-19 that it would cause a state-wide spike in hospitalized virus cases is a very, very, frustratingly silly argument.
The final number we need to consider is the number of deaths, and here at least there is some good news; we are not seeing a substantial increase in the people in Texas dying from COVID-19, at least not yet. There are two ways to understand this. The optimistic way is to think that something has changed; either the virus has somehow become less deadly than before, or our increased understanding of COVID-19 has led to a better ability to fight the virus; improved disease-specific ventilation strategies, effective drug therapies, and more efficacious supportive care measures. In fact, there is a great deal of evidence that the latter really is true, as we will discuss in another post. But the pessimistic view (and the truth is probably a combination of both) is to realize that most people do not just get admitted to the hospital with severe COVID-19 infection and pass away the same day. There is a significant lag time as those patients are treated and fight against the virus, and our surge in hospitalized cases is only a little more than a week old.
Many of those hospitalized patients are fighting for their lives in the ICU right now, as the hospitals are starting to fill up around them and their nurses and doctors are becoming fatigued. Many of those people will recover, but many will not; and it will take a couple of weeks, and often times much longer, to see how many, and who. As we’ve seen elsewhere, the ratio of those who don’t recover will only increase if resources and the margin for careful attention and heroic efforts on their behalf begin to run short. Yes, our improved understanding of the virus and more effective therapies gives us a better chance to fight the virus than Italy had in March or New York had in April; but doubling down on the difficult work of mitigation now to prevent our healthcare systems from being overwhelmed in a couple of weeks when more and more patients reach their crisis point is every bit as important.
What will next month’s data look like? It’s still partly up to us.
I had intended to write this weekend on a variety of topics, including herd immunity, the recent RECOVERY trial using low-dose dexamethasone in critically ill COVID-19 patients, antibody testing, and the question of whether the increase in cases is really just due to increased testing (answer: unfortunately, no). But when I woke up this morning the world seemed suddenly, vehemently, and inexplicably divided on just one subject: wearing masks.
Part of this can be accounted for, at least locally; yesterday the City of Waco issued an order requiring businesses to create and post mask policies for employees and customers. As with anything that has been unnecessarily politicized and sensationalized, I recommend you read for yourself what the order actually does and does not require. This morning I had half a dozen messages asking for my thoughts on whether or not masks are an effective strategy, and several people shared pieces of misinformation they wanted to bring to my attention.
So while I would still like to write about all of the above issues, I think this one will have to take priority today.
Are masks safe and effective?
G.K. Chesterton said that he was most convinced by evidence that is ‘miscellaneous and even scrappy.’
“A man may well be less convinced of a philosophy from four books, than from one book, one battle, one landscape, and one old friend. The very fact that the things are of different kinds increases the importance of the fact that they all point to one conclusion.”
G.K. Chesterton, Orthodoxy
So while we will look at scientific studies, journal articles, and other medical evidence, I want to include data from various kinds of research, including both laboratory conditions and real-world epidemiology, and from both prior to and during the COVID-19 pandemic. I also want us to apply some common sense and a good bit of our own past experiences. This can be dangerous in a field like medicine, where realities are often counter-intuitive, but if undertaken cautiously this common sense approach can serve as an anchor for the more academic information.
With that in mind, I think we can start by thinking about the advice we give to children when they are sick or have seasonal allergies (if your children are like mine, these efforts are ultimately futile, but struggling against that futility is a time honored parenting tradition). We tell children to place their hands over their mouths when they sneeze or cough. If we are particularly savvy (and can get past the occult theme; looking at you anti-Harry Potter friends), we teach them the Vampire Sneeze/Cough, where we cough into the antecubital fossa (the bend of the elbow) instead of our hands.
It does work much better if you wear a cloak at all times.
Why? Because respiratory viruses are spread through respiratory droplets; mucous and saliva from the respiratory track that contains the virus. In this article we will look at the filtering ability of various types of masks and whether they are actually able to catch the microscopic particles that cause illness, but you don’t need a microscope to measure the number of microns between a toddler’s fingers when she almost but not quite entirely fails to cover her mouth for a cough; it’s a lot.
Now it’s true that these etiquette maneuvers do not actually stop or absorb all of the particles; they catch some and merely redirect others into the surrounding environment. But you knew that. If you live with a sick child, the odds of yourself or another family member getting sick is high regardless of how good they are at vampire coughing. The goal isn’t to stop 100% of the droplets, but to modify the spatial distribution; to make it less likely that you will get sick from someone coughing or sneezing a few feet away or across the room. Even in science some things are intuitive; if you can feel the spray of respiratory droplets on your face when someone coughs near you, you know your chances of getting sick are higher.
This is the same principal we are talking about when it comes to masks. Nobody is saying that if someone has COVID-19 they can just wear a mask, N95 or otherwise, and cough and sneeze without getting anyone sick; studies have show that the particles still escape. But if someone coughs across the room from you, their mask or their elbow, or even better both, interrupts the momentum of the droplets (50 mph for a cough, 100 for a sneeze according to a study in the Journal of Fluid Mechanics) and decreases the chances of the droplets reaching you, giving you time to move away or at least cover your own face, blocking a few more particles. These are components of an overall risk mitigation strategy that involves things like social and physical distancing, frequent hand washing, sitting outside instead of inside, contact tracing of COVID-19 patients, and staying home if you are sick.
Masks aren’t perfect, but nobody is claiming they are.
It’s also important to note that the studies that have shown only very modest benefits of masks, such as the study that produced the graph above, have focused on the spread of droplets through coughing and sneezing; high pressure, high velocity events that force droplets through and around barriers such as masks and sleeves. However, the City of Waco is not asking 100,000 people to wear a mask in case one of those people happens to cough in HEB. We now know that both asymptomatic and presymptomatic COVID-19 transmission do indeed occur, and the mechanism of transmission still seems to be from saliva and respiratory mucous, including respiratory droplets and aerosols, even in the absence of coughing and sneezing. Talking, forcefully exhaling, singing, yawning, spit talking; all of these are lower pressure events where a mask may actually block, rather than redirect, a higher percentage of these small, lower velocity particles. Again, you already believe this intuitively, because you cover your mouth when your breath stinks.
Or you should.
I also think that revisiting our actual real life experience and common sense is particularly important when dealing with medical misinformation, which is often found to be self-contradictory and manifestly illogical within only a few moments consideration and comparison to facts we already know. It rarely takes being a physician or another scientist to figure out that these wild claims on social media aren’t accurate, though I’m sure it helps.
Unmasking Mask Misinformation (sorry)
A friend sent this to me this morning; it was posted on a public forum (“public forum” sounds so much more legitimate than “Facebook comments”) as a response to our city’s new masking policy. I’ve also been sent a longer paragraph format piece that starts “I am OSHA 10&30 certified.” Since they overlap quite a bit, I won’t re-post that one in its entirety, but it’s just full of contradictions (‘surgical masks only filter on the exhale’ yet ‘become useless’ for protecting you if your breath clogs them), false claims (‘N95 masks can’t filter COVID-19’, ‘asymptomatic spread doesn’t occur’), and nonsensical statements (if you wear a mask and get exposed to COVID-19 you become a walking virus dispenser, cloth masks are worse than no barrier at all). It does make one really excellent point though; if you are relying on wearing a mask to fully protect you from getting or spreading COVID-19, that is indeed a false sense of security. We can’t say that often enough; but it just doesn’t follow that masks are worthless or make the problem worse, which is what they repeatedly claim. I’d like to go through the claims above in order, before concluding with some final arguments for masking.
Claims #1 and #2: Masks decrease oxygen intake and increase carbon dioxide retention.
This is something that has been studied extensively, and there is no evidence that simple surgical or cloth face masks will cause hypoxia or any significant decline in oxygen levels. Oxygen molecules are very small and diffuse easily both around and through these types of masks; they are nowhere near the size of viruses, or the much larger respiratory droplets that carry most of the virus that is exhaled. The same is true about Carbon Dioxide, which is only slightly larger.
But you can also consult your own experience here. Many types of people already wear masks for many hours of the day, from surgeons to certain industrial workers, and women in many cultures wear face coverings as a part of their public clothing. Yet we do not consider these persons to be at high risk for either hypoxic (low oxygen) or hypercapnic (high CO2) injury. A big part of the problem is that we have sensationalized the wearing of masks during COVID-19 and have started to treat it like it isn’t a normal part of our experience already, which it absolutely is. Whether it is the above examples, or Halloween or Comic-Con, or my 5 year old spending three weeks straight in his Spider-Man costume and refusing to wear anything else, the wearing of masks is something we all have some degree of experience with and have never really been concerned about until now, when we are suddenly being told they are extremely dangerous, generally by the same people who have been spreading various types of COVID-19 misinformation since mid-March.
But more to the point, you can study this on your own. A battery powered pulse oximeter is very accurate and costs about $12, and you can use one to do a simple experiment that will reassure you, at the very least, that your face mask is not causing your oxygen levels to drop. Check your oxygen level with your mask off, and then wear it for however long you expect to need it when you are out running errands or whatever scenario you are worried about. Then check it again. In general in a healthy adult, readings above 95% are normal and below 90% are concerning. As an example, I’ve been wearing my properly fitting N95 for the last half-hour and my O2 saturation has fallen exactly one percentage point.
I’ll admit, I freaked out for a minute before I realized the labels are upside down.
There is one group of people we should mention here, and that’s people with chronic lung disease such as COPD or Asthma. For people with these conditions, the increased heat and moisture of the air within the mask, and the decreased air flow directly to the nose and mouth, really can create both real and perceived difficulty breathing (and in these conditions, these trigger each other so easily that drawing a distinction between the physiologic respiratory distress and the anxiety-provoked sensation of respiratory distress is almost a false dichotomy; not being able to breath is scary). These are also conditions that predict a higher likelihood of severe illness in COVID-19, which complicates matters. For these individuals who should already be taking every precaution possible for their own safety in the midst of this pandemic, the decision of whether and what kind of mask they should wear when they do have to go out should be a discussion between them and their doctor. For the rest of us, especially those of us who personally care about someone with Asthma or COPD, it’s important that we take every precaution we can; it should go without saying that our “what about someone with a chronic respiratory illness” should only ever be a legitimate question on their behalf, not a rhetorical ‘gotcha’ to turn off our intellectual honesty on this issue and dismiss the benefits of everyone else wearing a mask.
Claims #3 and #4: Masks shut down the immune system and reactive your own viruses.
The third claim, that masks shut down your immune system, is just a reiteration of the above two, and there is absolutely no evidence for it. As we’ve already said, doctors, nurses, and other medical professionals, and especially those involved in surgery, wear masks all the time without any fear of their immune systems being shut down or weakened. And while these types of people are often fearless when confronting deadly situations or illnesses in order to care for their patients, as we have seen throughout this pandemic, they tend to otherwise be fairly health conscious. I still remember being shocked during a group discussion in medical school when we were asked what it was we valued most highly. I was trying to honestly wrestle with whether I valued my faith, my wife, or my daughter most, and how it was even possible to separate those things from one another, when my friend answered “my health,” and several others nodded in agreement. I have no judgement for that person, but the whole idea was very alien to me (and maybe that shows something of my privilege in having lived overall a very healthy life, often despite my personal choices). Maybe this friend would risk the thing he valued highest on behalf of a patient (in fact I think he would); but if there was any evidence that his health was imperiled by wearing a mask, he would be leading the charge against masking (just checked facebook; he isn’t), and probably would have been doing so since medical school.
The fourth claim is one that I first came across in the Plandemic “documentary” last month, and based on the wording it seems to be taken directly from there (or they are both taken from a 3rd, unknown source, which I’ll call “Q”)(I’m now being told that “Q” is already taken). The actual claim is that wearing a mask will activate dormant retroviruses that live in your body. Retroviruses are a family of viruses that replicate by inserting viral DNA into host cells and hijacking cellular machinery, and only a few known species causes disease in humans, including HIV and Human T-Lymphotropic Virus, which can cause certain cancers. This claim is very specific and very conspiracy-theory oriented, but I suspect that this distinction between retroviruses and common viral illnesses like cold and flu is not being made by the people spreading this meme.
The long and short of it is that this just isn’t the way the immune system works. You don’t have a host of dormant viruses sitting in your lungs that, if breathed into a cloth or small space and then breathed in again, will suddenly become active and cause an infection. Do you get sick when you sit in a car? What about when you hold your breath? What if you sleep with your face too close to a pillow? Is there evidence that we see more respiratory infections in people that wear masks regularly? Of course not. In someone who has a functioning immune system, once your immune system has seen and defeated a virus, you cannot give that virus to you; you already have an effective immune response to it. There are a small number of exceptions, like getting shingles through varicella zoster reactivation, but coronaviruses aren’t one of them and there is no evidence that wearing a mask or breathing out and then breathing in the ‘same air’ has anything to do with viral reactivation; there isn’t even a physiologic mechanism that would make this possible.
Claim #5: The virus is too small to be trapped by the masks!
This is where both the misinformation and the answer get a bit more technical, and if you want all of the scientific details, the blog First10em has an amazing article on masking, viral transmission, the 6 feet apart rule (which they call the “2 meter” rule, whatever that means), and the transmission patterns and particle sizes of both droplets and aerosols. The question of whether various types of face masks besides N95’s actually do filter the COVID-19 virus itself is still an unanswered question, but the answer seems to be, to some degree, yes. Studies have shown different types of masks to have varying filtering efficacy even down to to very, very small particles in the range of 300 nanometers or less, in fact right in the range of the virus itself (the SARS-CoV-2 virus is roughly 120 nanometers; an earlier version of this article incorrectly reported the size of the measured particles in this study as 40 times smaller than the virus, which was just due to me getting my conversions wrong. Sorry; pay attention in 8th grade algebra, kids), but other studies have shown that the virus is still able to transmit through (or around) masks, at least to a few inches away and if propelled by a cough. Taken together these studies seem to reiterate what we have been saying all along; masks aren’t perfect, but they do decrease the risk, especially in short-term contact with non-cough, non-sneeze related transmissions like we would see in asymptomatic and presymptomatic cases. Indeed, this is confirmed by a Hong Kong study in 2011 that found that the protection offered against respiratory pathogens by all types of face masks decreased with higher velocities and prolonged exposure.
Again, Oxygen molecules are < 0.5 nm
Regarding this piece of misinformation though, we can summarize the two main errors pretty succinctly; the virus isn’t floating through the air by itself, it’s suspended in respiratory droplets and aerosols; and the masks aren’t supposed to block 100% of the particles on the microscopic level (though that would great), just trap most of them and slow the others down. The mosquito through a chain link fence analogy is silly because mosquitos can fly around barriers volitionally, and because it uses the size of the virus instead of the size of the respiratory particles, which are much larger (1-100 microns, mostly, instead of 0.12 microns). But if you want to use the analogy, it’s more like hitting golf balls through a chain link fence; yes, the gaps are bigger than the golfballs, and some will go through if they are hit really hard; but many will be blocked outright and many others will be slowed down and redirected.
Claim #6: There is no evidence to support masks.
We have already looked at some of the various types of evidence that I believe we all find somewhat convincing. We believe as a culture that masks are least helpful in preventing infections in some situations, such as surgery, and believe they are safe when we wear them for cultural or religious reasons, as part of our jobs, or as part of costumes. We engage in barrier maneuvers (some better than others) to block large respiratory droplets when we cough and sneeze. We know the masks redirect and lessen such droplets even in these high-velocity conditions, and we’ve seen the evidence from physics and fluid dynamics studies that they can filter the smaller aerosols under low-velocity conditions. For me, the last remaining piece of the puzzle is, “does it actually work, really?”
I want to look at two more types of evidence; epidemiology evidence from before the COVID-19 pandemic, and emerging epidemiological data from right now. An Australian study in 2009, well before the COVID-19 Pandemic (but you knew that), found that the wearing of face masks did diminish the transmission of upper respiratory illnesses even among household contacts, but that there were fairly low rates of compliance with masking. If masks were worn more, they could help significantly.
“Adherence to mask use was associated with a significantly reduced risk of ILI-associated (Influenza Like Illness) infection. We concluded that household use of masks is associated with low adherence and is ineffective in controlling seasonal ILI. If adherence were greater, mask use might reduce transmission during a severe influenza pandemic.”
This study and others like it, 10 years prior to the COVID-19 pandemic, should at least put to rest any ideas that wearing masks is a novel recommendation or a government ploy to control yet another aspect of our lives. Masks have been recommended, and shown to work, for preventing respiratory virus transmission for decades; any suspicion of them now likely comes more from the current hyper-politicized, conspiracy saturated climate than from anything else. But the COVID-19 virus is new and acts very differently from other respiratory viruses in so many ways, so what’s to say that masks will be effective for COVID-19?
It is too early in this pandemic to have robust and definite conclusions about which measures helped most and which showed modest or negligible benefits. We know that social distancing helps from evidence in places like Sweden and Norway, and we now seem to be living the results of relaxing our own social distancing measures without other robust mitigation strategies in place. When it comes to masks, we could compare the United States, which is (apparently) very resistant to masks becoming a social norm to places like South Korea where wearing a mask has been the norm since early in the pandemic; but this comparison is complicated by vastly different healthcare systems and populations and by a strong difference in adherence to other mitigation efforts as well, which we Americans have also been consistently defiant of.
Population: 328 Million
Population: 52 Million
I do agree in principal with the approach by one writer to the CDC’s journal, Emerging Infectious Diseases, in comparing Taiwan to Singapore; but again this is not a perfect comparison by any means.
Update: It has been pointed out to me that there are now several recently published studies, conducted during the COVID-19 pandemic itself, that have looked at the issue of mask wearing to determine if the benefit is significant. You can find two of them here and here (with thanks to Baylor Epidemiologist Dr. Emily Smith, PhD, who has written an excellent summary of the current evidence for masks). I’m sure many more studies are ongoing. Of course none of these are going to be able to perfectly measure the effectiveness of masking under real life pandemic conditions; if you can imagine a scientific experiment that could, it would probably be unethical and immoral (and logistically impossible), such as taking members of a population and randomizing them to wearing or not wearing masks and then measuring how many become sick from each group. Those types of study designs are entirely off the table, so we analyze epidemiological data; looking at what happened in countries, regions, and cities where masks were adopted early, and what happened in other places after they were adopted later on. It isn’t possible to know how well the mask policies were followed from such data, or to perfectly tease out confounding factors like social distancing measures, the success of contact tracing, and the robustness of testing programs; it wouldn’t be possible to say masks are the most important thing if they are always or nearly always used in conjunction with other mitigation strategies, which is exactly how they should be used. But these studies do conclude that implementing mask policies (and following them!) makes a significant difference in the trajectory of this pandemic, and taken as just one important kind of the multiple kinds of evidence we have looked at, I do think they contribute to a convincing case for wearing masks.
Ultimately, once this turns the corner, we will never be able to say with certainty what the real answer was; whether it was wearing masks that helped the most or the heightened caution in other areas when cases began to climb, whether reopening resulted in a surge here in Texas or if it was our bucking of social distancing all along, whether each of our mitigation measures individually made a difference or not. What we can say for certain is that the American method so far has not been working. By denying the disease’s existence and danger, producing conspiracy theory after conspiracy theory, claiming we beat it prematurely, and fighting tooth and nail against every reasonable recommendation and rule meant to protect ourselves and our neighbors, we have taken a global pandemic and made it largely into an American pandemic, with the highest number of cases and deaths in the world.
There is plenty of evidence that masks are safe, and that they stand a fair chance of helping, especially against asymptomatic and presymptomatic spread. If you are sick, get tested, stay home, and isolate; make sure you get the medical care you need. If you are well and can physically distance yourself from others, then distance yourself from others while finding ways to still care for your community and your own mental and physical health. If you cannot distance because of strong religious or moral convictions or the realities of your job, or due to strong personal preferences, then please wear a mask and wash your hands frequently.
This is just one of the ways we can do better during the rest of this pandemic; myself included.