This is a short post because, frankly, I don’t have time to write it (clinic all day, D&D with the kids tonight). Those of you hoping for another 7,000 word in-depth discussion (read: nobody) will have to settle for just 3,000 or so today. Nevertheless, I want to start with a digression and show you this chart I use in my clinic:
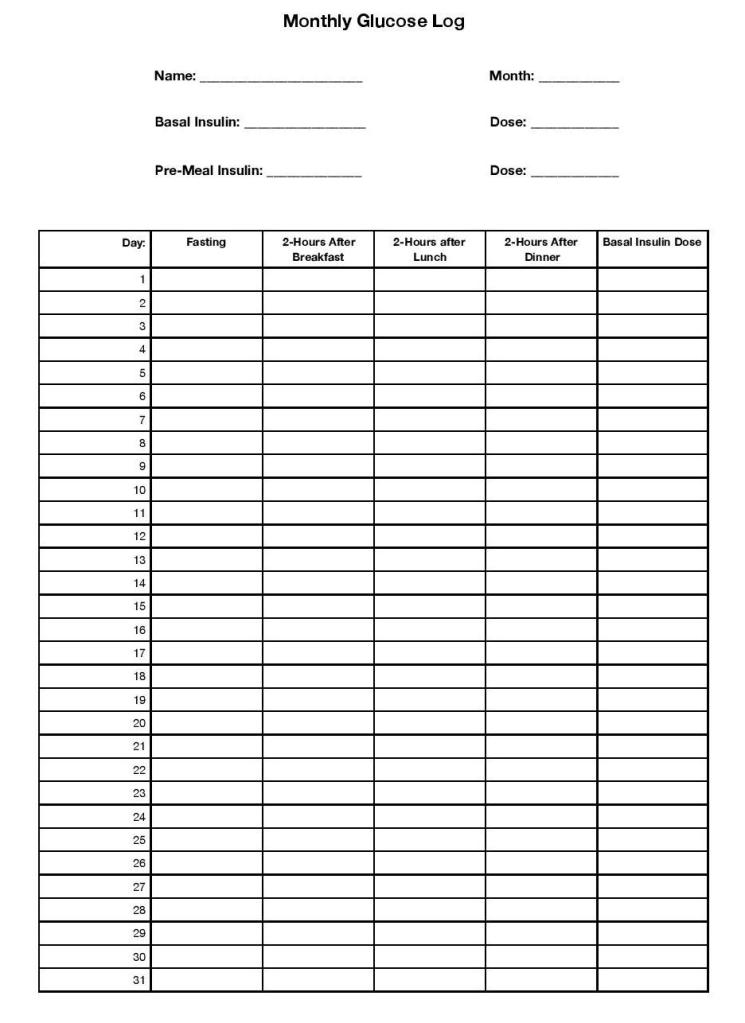
This chart is for my diabetic patients who have a very particular treatment regimen; they are taking both a long-acting basal insulin once or twice daily, and they are taking a short or rapid acting insulin before each meal. Because of this, we need some blood sugar numbers; we need to know their fasting blood sugar in the morning so we can adjust their basal insulin, and we need to know their numbers 2 hours after breakfast, lunch, and dinner so we can adjust their meal coverage with the short acting insulin. They are not taking insulin on a sliding scale; those patients will need to check before meals in order to take the appropriate dose.
Now, I work extremely hard to empower my patients to adjust their insulin on their own, and a lot of our visit time is focused on teaching them about the various insulin length of action times, the logic behind basal/bolus insulin dosing, and especially what numbers to look for that should trigger them to increase or decrease their dose. But it’s challenging, and as much as I love it when a patient is on ‘auto-pilot’ with their insulin, we still do a lot of adjusting in clinic, which is where these charts come in. Fasting blood sugar high? We’ll go up on your long-acting Lantus insulin. Taking 5 units of novolog before every meal but the after-lunch numbers are still super-high? We can go up on your pre-lunch and keep the pre-breakfast and pre-dinner numbers the same. You get the idea.
So that’s the glucose log I print for my patients. Now let me show the one I actually hand to them:

You see, like all doctors my approach to any medical problem represents a balance between what my medical training tells me is the best possible treatment plan and the actual, lived experiences of my patients. Some of my patients will check their blood sugar 4 times a day, every day (some of them even if they don’t strictly need to; they just really, really like to know). But I don’t think I could manage to do that, and so I don’t ‘demand’ it of my patients. The reality is, we could get almost all the information that the patient and I need by checking their blood sugar half that much; fasting every day, then checking after a different meal each day. And most of my patients are much, much more likely to follow through with checking twice a day than four times a day (as I certainly would be).
What does this have to do with the quarantine recommendations for COVID-19? Everything, because both the CDC’s new guidelines and my approach to blood sugar logging for my diabetic patients are based on an essential mediator of medical outcomes: Health Behavior.
Where did the original 14 day guidelines come from?
The CDC began to recommend a 14-day quarantine for international travelers coming to the US as early as February, and the same for any household and close contacts of COVID-19 positive persons shortly thereafter. This was based on the incubation period of the virus; the range of time it typically takes an exposed person who becomes infected to develop symptoms. Initially this relied on the already known incubation periods of similar novel Coronaviruses, SARS and MERS, from epidemiology studies that were done following those epidemics in 2003 and 2012. As the COVID-19 pandemic progressed, studies began to emerge which showed similar incubation periods for the SARS-CoV-2 virus as well. A study from The Netherlands in February found the incubation period to be between 2 to 11 days based on a small number of patients in Wuhan, China; very similar to SARS and especially MERS. This was supported by multiple other studies that all showed an apparent incubation period somewhere in the range of 2-12 days.
This begs the question, “if most studies showed the incubation period to end at 10 to 12 days, why were we all told to quarantine for 14 days?” And this is where health behavior comes in. The first (and least important) reason, I think, is because 14 days is just a lot easier to remember. “Your last exposure was last Wednesday, so you can be done with Quarantine after next Wednesday” is easier to remember than 11 days or 12 days because we naturally think in weeks anyway. But much more importantly, the novel Coronavirus was novel and recommendations needed to be made based on very limited evidence. The two studies above had sample sizes of 88 and 158 respectively; enough to be going on with, but not nearly enough to be really confident. Those studies consistently showed that though we thought the average incubation period would be 5-6 days, there was still a possibility that once we had more data it would end up being much longer; and there was a very good chance that even if the average incubation period stayed less than a week, some people would still be contagious for much longer, maybe even greater than 2 weeks. With a virus this contagious, ignoring that uncertainty could be very, very dangerous.
Hence the recommendation to be released from quarantine only once you have been asymptomatic for 14 days since your last exposure; it was easy to remember, it was very likely, based on early evidence, to cover the vast majority of cases (although it does absolutely nothing for fully asymptomatic cases, of course), and it was unlikely to be expanded based on new evidence.
That last bit is really important, because even though epidemiologists, physicians, and other scientists know that it’s exactly how science is supposed to work, we’ve all seen how suspiciously our society looks on any changes in recommendations based on new evidence. If the CDC started with 14 days of quarantine and later decreased it to 12, some people would be a bit irritated and probably lose some confidence in them (we’ve seen this time and time again; the undeserved “they keep changing the guidelines!” and “They don’t know what they’re doing!”), but overall it would be a welcomed change. But if they had started with say 9 days and then, based on new evidence, expanded it to 16 days, how would that have gone down? It would have been pandemonium.
So they picked a timeframe that was 1. Supported by the data available and 2. Unlikely to be expanded later based on new data. But there was still a problem, and it was this: Health Behavior.
14 days of quarantine is hard. It’s hard psychologically, it’s hard physically, and it’s hard economically. I see COVID-19 positive and COVID-19 exposed patients every day and I have to tell you, I feel terrible every single time I have to recommend a 14 day quarantine to someone. I see the irritation or frustration or even despair as they try to figure out what plans they have to cancel, what friends and family they will have to miss, and how they are possibly going to make ends meet if they can’t work for that long. The results of quarantine so often touted by the anti-quarantine, COVID-19 is a hoax folks, like increased depression and anxiety, are real. No one ever denied this, it’s just that the pandemic is not a hoax and has, as of today, killed 1.5 million people worldwide and 271,000 in the US.
And because it’s hard, every single one of us knows somebody who didn’t quarantine when they were supposed to. Unsurprisingly, that’s one of the main factors I see at play in my outdoor COVID-19 clinic visits; people were exposed to friends or family who had not reached the end of their quarantine period but decided that enough time had passed that they wouldn’t be at risk of spreading the virus. Based on what? Gut feeling, mostly; and also reaching the point where their desire for experiences or people or options precluded by quarantine was simply greater than their will to continue quarantine. For most of us, that point will probably come sometime before those 14 days are up. I even know of doctors who couldn’t make it to 14 days, and drawing on exactly none of there clinical training or basic sciences knowledge decided that they must have ‘dodged a bullet’ when they remained asymptomatic less than a week from their exposure, and resumed life as normal. Who am I to judge. I’m a strong extrovert and even general social distancing has been hard enough on me; there but by the grace of God go I.
And sometimes the guidelines, while valid, seem nearly impossible to comply with. For instance, I have friends who diligently completed their ongoing household contact quarantine guidelines, which begin on the day the COVID-19 positive patient is diagnosed and end 14 days after that person’s 10-day isolation period. That’s 24 days total for their household contacts.

This is no small problem; studies from previous epidemics requiring self-quarantine measures have found incredibly variable rates of adherence, and often south of 50%. In many ways America was a set-up for poor compliance to these guidelines; highly individualistic culture, a pandemic occurring in the most contentious election year in recent memory, massive campaigns (organized and unorganized) of misinformation about the virus, and with no clear messaging or leadership on a national level. Those last two points are crucial, because the strongest predictor for adherence is not cultural or socio-economic factors, or even fear of the virus; it’s how knowledgeable people are about the virus and the way it spreads, and how well they understand the quarantine guidelines. Which is, uh, why folks like me are doing this sort of thing.
12/2/20: The CDC will update quarantine guidelines.
Which brings us to today, and the new quarantine options from the CDC, which are these:
Following close contact or exposure to COVID-19, an individual may self-quarantine for:
- 10 days, as long as they remain asymptomatic,
or - 7 days, as long as they remain asymptomatic and have a negative COVID-19 test.
Why were these changes made? Because they were wrong back in February? Because the election is over (finally)? Not at all. There are two possible reasons: either because enough new evidence has emerged to convince the epidemiologists at the CDC that these timeframes are as safe and effective as the original 14-day recommendations, or because they are convinced that enough people will actually follow through with these less extreme guidelines that there will still be a net decrease in transmission.
Let’s look at the first one. There have been nearly 14 million cases in the US since February and over 64 million world wide; even without access to complete information of each of these individuals and their exposures to COVID-19, we should be able to muster more than the 88 cases that first study was based on. Have all of the newer, more robust analyses of this data changed the picture of COVID-19 incubation so drastically that the CDC was forced to update their guidelines?
Answer: Not really.
It’s important to note that when the CDC did finally release the updated guidelines late in the night, they clarified that the new guidelines were alternative options to the 14-day quarantine, which was still their strongest recommendation. I believe this is supported by the evidence.
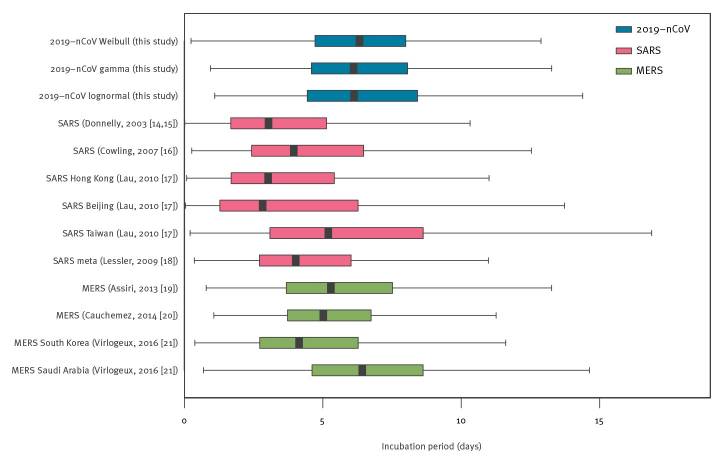
Just like there was nothing magical about day 14 that caused the virus to go, “all righty I guess we’re done here, pack ‘er up boys!” back in March, there’s nothing magical about day 10 or day 7 now. A systematic review and meta-analysis of all the then available estimates of the COVID-19 incubation period, first published in The British Journal of Medicine in August, found an average (mean) incubation period of 5 to 7 days, and 95th percentile estimate between 10 and 14 days…. Remarkably similar to the earlier estimates. The figure below is from that paper and reflects the distribution in all of the studies they could get their hands on. Notice how there isn’t a steep drop off at day 10; in fact, the range of the possible incubation period stretches all the way out to about 3 weeks. Unlike the early observational studies, this meta-analysis involved multiple studies with hundreds of cases each, though that original data was still from early on in the pandemic.

Another meta-analysis from later in the year, first published in October in the online journal Current Therapeutic Research, included 18 studies representing 22,595 participants. That’s a lot more than 88. What did they find? The average incubation period was about 6 days. This paper was advocating for a much shorter quarantine, along with testing, similar to the new ‘7 days with a negative test’ recommendation from the CDC; tellingly, however, it only included analysis of the mean incubation period, not the range of incubation from those studies; it doesn’t address the impact of all of those cases that would cease quarantine on day 7 but become symptomatic within the next few days.
Finally, a relatively small but thoroughly analyzed study from Singapore including 164 cases from January to April and published in the journal Epidemiology and Infection in September shows some cases with an incubation period definitively longer than the 10 day mark set by the CDC, though they were relatively small in number. It also found that the incubation period does seem to be positively correlated with age, with the longest incubation periods among those in their 70’s and older.

To summarize, unless there is some big study that the CDC has access to and I can’t seem to find (and please send it to me if there is, so I can take this post down and not look like an idiot), the current evidence has not revised the known incubation period of COVID-19.
You can still develop COVID-19 symptoms
more than 10 days after your exposure.
Q: So why the change?
A: Health Behavior
So if the CDC isn’t changing the quarantine guidelines because of some scientific breakthrough that has utterly overturned our understanding of the virus’s incubation period or the way it is transmitted, why make the change at all? Because the 14-day quarantine guidelines aren’t working; not because quarantine doesn’t work, but because people won’t do it. They are banking on the idea that enough people will be willing to comply with a less aggressive quarantine period that still covers the vast majority of cases (compared to a longer quarantine that very few people were willing to follow) to make up for the relatively few cases whose incubation period would have been longer.
I don’t know if they are right or not. Something’s gotta give, so I really hope they are. But overall I actually kind of like this new recommendation because it has the potential to change the behavior of one group of people that has probably been contributing to the pandemic numbers as much as anyone else; asymptomatic COVID-19 carriers who aren’t following quarantine at all. The biggest weakness with the 14-day quarantine was that there was no fail-safe built in for the people who just weren’t willing to quarantine. They might stay home from work or school for 14 days because they had to, but would use some of that time to shop, have parties, or engage in other activities that had a high likelihood of transmitting the virus. I don’t mean to imply it was all from selfish motivations; some people with much less natural laziness than myself probably just couldn’t cope with 14-days off, and have probably been using their quarantine to help others and do good deeds around the neighborhood, or volunteer more at their local church or community center. Good things in themselves, but still very, very dangerous when you have been exposed to a deadly and highly contagious virus. And like I said before, many others very understandably don’t have the margin to be out of work for that amount of time. The new guidelines are helpful because for people very motivated to stop quarantine after day 7, a test for COVID-19 now greatly increases the chances that we’ll catch their infection and modify behaviors that lead to transmission. Even if they weren’t following quarantine before that day 7 test, they might follow isolation guidelines if it’s positive.
We know that asymptomatic and pre-symptomatic people can still spread COVID-19, but asymptomatic testing has always been a double-edged sword. Very wide scale asymptomatic testing would be one of the best possible ways to catch and isolate cases early and really modify the course of the pandemic, and asymptomatic testing targeting people in essential services, like nursing home nurses and doctors, is the best way to prevent pre-symptomatic transmission among some of our most vulnerable populations. But in both of these situations, the test result always leads to either a neutral or a safer set of decisions; if asymptomatic people test positive, they isolate, while negative people continue their standard level of caution. If a nurse or doctor tests positive, she calls in; if negative, she continues to work.
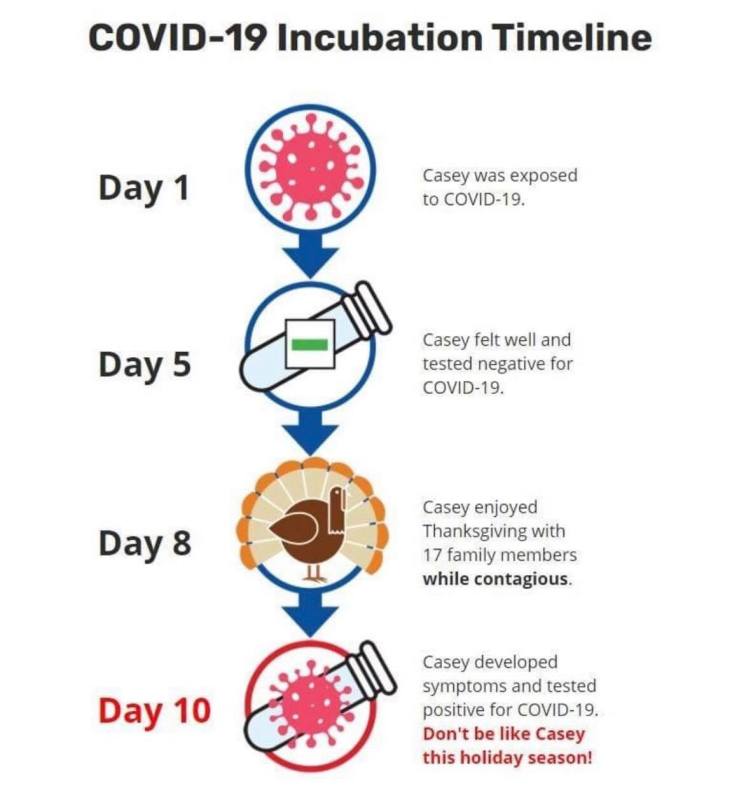
But testing of asymptomatic people who have been exposed and are still under quarantine is completely different, because the test result now has two drastically diverging branches; not safer and neutral, but safer and less safe. If an exposed person does test positive, it is much easier for them to feel the weight of their responsibility to keep those around them safe from it; I’m sure anybody reading this who has tested positive remembers the moment they received that news, and remembers how real the need to isolate suddenly felt. But since they are already under quarantine, there is a very real chance that a negative test will give many people a false sense of security without actually guaranteeing that they won’t become contagious, and instead of continuing with the same degree of caution they are most likely to exercise far less. There are a hundred different cartoons online right now demonstrating this concept. I like this one because it feels like the person who wrote it really has a vendetta against somebody named Casey.
This is the reason my COVID-19 clinic has shied away from broadly testing asymptomatic close contacts; the value of that test can be a big positive or a big negative, and it entirely depends on what the person plans to do with that information. If they plan to quarantine well regardless of a negative and only want to know so they can alert their close contacts, that’s terrific; but I’ve talked with lots of people, patients of mine and otherwise, and even some healthcare workers, who were under quarantine due to close contact and planned to get tested so that they could go ahead and travel, throw a party, or go back to work early. A negative test, within the incubation period, cannot definitively make these actions safe, and depending on when in the incubation period, might be no help at all. That’s why I carefully counsel every patient about what to do with their test results, symptomatic or not, based on their clinical history. I’m not opposed to asymptomatic testing for exposed individuals; it just has to be accompanied by a very careful discussion of what the test can and can’t be used for.
With all of that in mind, if you are going to do asymptomatic testing for exposed close contacts, 7 days seems like a fair point to test. Again, it’s easy to remember; ‘1 week of quarantine and then get tested’. But more importantly, it’s past the mean incubation period; a test on day 7 covers the incubation period for most people who remain asymptomatic, and has a good chance of catching any pre-symptomatic patients with an incubation period up to day 8 or 9. Between that and of course testing the folks that do have symptoms as soon as they get them, that covers most people. And if that negative test does give a little false sense of security, it’s at a point in the timeline of their exposure where lots of folks are feeling ready to throw caution to the wind anyway.
It’s not perfect, but I wouldn’t call the new quarantine guidelines ‘misinformation’ either. It’s a calculated risk based on the expected health behavior of a population who is absolutely exhausted with this pandemic. I hope it pays off.
So… What do I do then?
Adherence to quarantine is highest when people really have a firm understanding of the quarantine guidelines and the rationale behind them. The rationale behind this decision is that more people will comply with less extreme quarantine guidelines that are still, for the most part, safe. But it doesn’t mean I’ll be counseling my patients differently; I still want them to know that they could become contagious for a few days after that day 10, and that the negative test on day 7 is not a 100% guarantee. I want them to understand the incubation period of the virus and the extra caution they still need to take for those several days after their quarantine is technically over. When I’m writing school and work notes, if their quarantine period under the new guidelines has them going back on a Friday, we are going to push that back (with the patient’s permission) to Monday. When they test negative on day 7, I want them to know that they should still come back and get re-tested if they develop symptoms on day 11 or 12.
And that’s the advice I’m offering to you now. If you have a close contact and need to quarantine, try to make it to at least day 12, if not day 14, before releasing yourself if at all possible; or get tested on day 8 or 9 instead of day 7 if you can. Advocate for those around you by fighting for your right to ere on the side of caution, recognizing that the current guidelines are a compromise with the expected health behaviors of our society. A timely and hopefully effective compromise, but a compromise nonetheless. And just as you wouldn’t act like Casey and use a negative test on day 5 as an excuse to cast aside all precautions, so a negative test on day 7 should be treated as reassuring, but not foolproof.
But as for me and my house, we will quarantine for 14 days.
