I’ve had quite a few questions about COVID-19 put to me by friends and family members recently, and so last week I had intended to begin trying my best to answer them. This plan had to be put on hold when Waco (and various other cities in Texas) issued a requirement to wear a face mask inside of businesses and restaurants, and the whole world sort of lost it’s collective mind. I think things have calmed down now, at least locally, and as I’ve driven to clinic and back and the one or two other places I couldn’t really avoid going, I’ve thankfully seen a noticeable increase in masking, either in compliance with this decision or in response to the efforts of so many to share reliable information on the benefits and safety of wearing a face mask. Thank you all for fighting the crazy amount of misinformation out there. For my take on wearing masks you can read my previous blog post on masking.
Now that we’ve made it through another week without another viral misinformation video, I’m finally taking the time to sit down and write that original post I had planned on. I’ve tried to limit myself to just two paragraphs for each topic (paragraph length unspecified), but given just how many questions
Due to length, I’ve broken this post up into multiple parts.
Warning: These got really ‘mathy’ on me before I realized it was happening.
Part 2: Do antibody testing and asymptomatic cases prove the virus isn’t as dangerous as we thought?
Part 3: Isn’t a surge a good thing? Herd Immunity and the RECOVERY Trial.
Question #1: Isn’t the rise in cases just a reflection of more widespread testing?
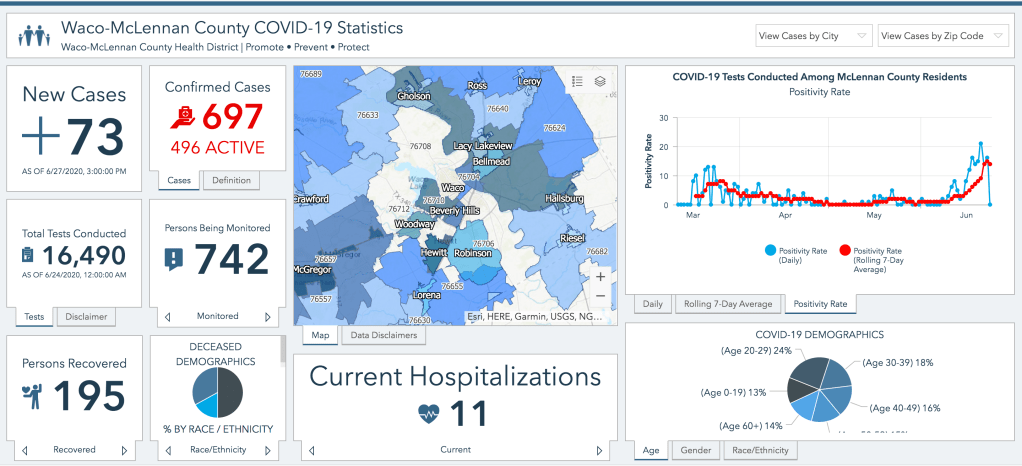
This is a question that has been on everyone’s minds since the very earliest days of our testing woes, back in March when we had barely any testing available. It has ranged from a very fair question to a rhetorical device for spreading misinformation, with at least one prominent political figure even seeming to say that it would be better if we didn’t test so much so that our numbers looked better. I honestly believe most people really are curious about the relationship between our testing numbers and our numbers of cases and are not asking to try to minimize the appearance of the surge we are facing in Texas right now. In one sense, we will always find more cases of a disease when we test for it than when we don’t; that’s a truism. But if we want to determine whether cases are really going up we can look at a few other parameters than the absolute number of positive tests that will inform our understanding of the ’75 new cases’ or ‘5,747 new cases’ we are seeing in the news and on social media each day (To go through these numbers I highly recommend you spend some time navigating the Texas DSHS COVID-19 Dashboard; both their case data and testing and hospital data sections).
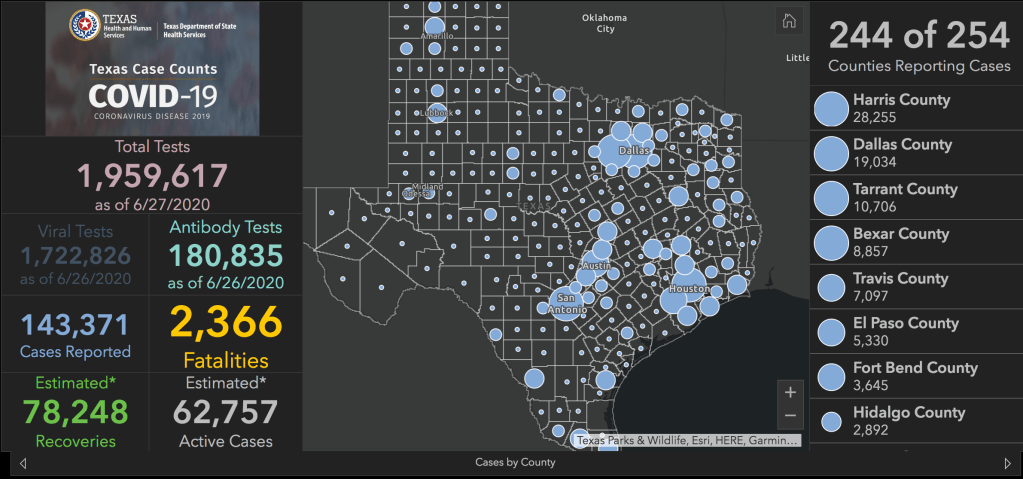
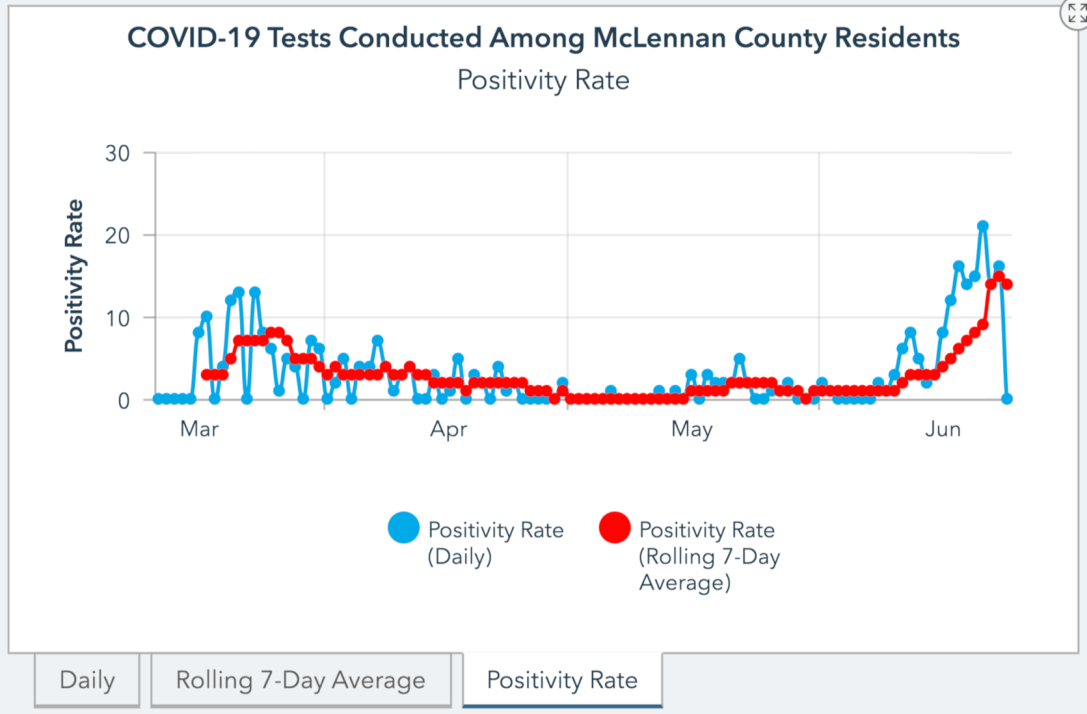
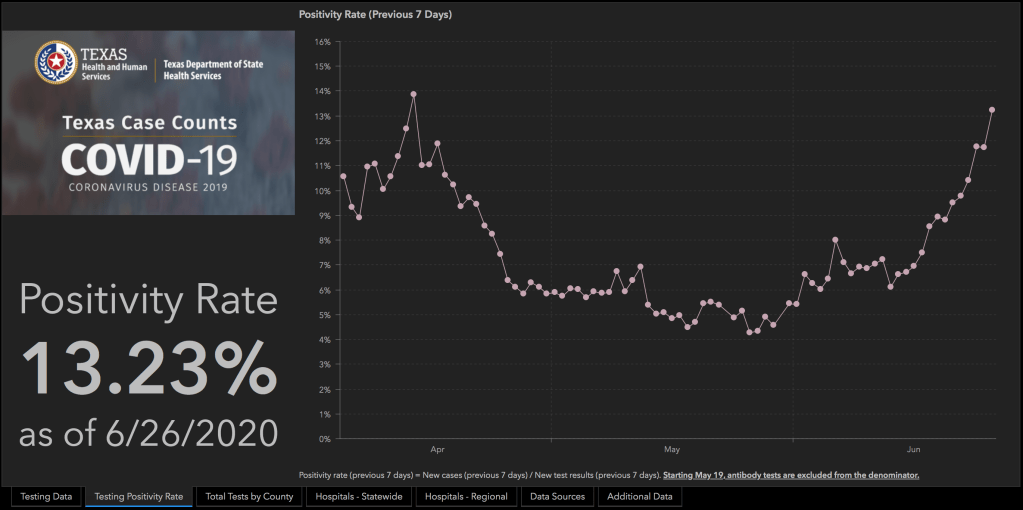
The first number is the percentage of positive tests. Ever since testing became more widely available in April and we were able to shift away from testing only those with a high likelihood of having the disease and/or of developing complications, we have been testing essentially the same types of cases; people with some combination of cough, shortness of breath, fever, loss of taste and smell, etc. and/or known or suspected exposure to the virus. There are many causes of these types of symptoms, from allergies to other respiratory viruses to chronic conditions like asthma and COPD, and in our pre-surge days these explained the symptoms in the vast majority of people we tested. If you look at the Texas testing data from April you will see two things; an overall low number of tests (a very modest 5-10k per day) and a fairly high percentage of tests that are positive, between 10-14%. This reflects our very strict testing criteria at that time; we were only testing the people we already really thought had it. In late April and all through May we see an ever increasing number of daily tests and a falling rate of positive tests, a reflection of liberalizing testing criteria and strong evidence of overall low prevalence in our State. Throughout June, and especially over the last 2 weeks, we continue to see an increasing number of tests each day; but we are now also seeing our percentage of positive cases rising again. This isn’t because we’ve tightened up or restricted our testing criteria again; it’s because more people actually do have the virus.
This exactly matches my own clinical experiences; back in May I was testing for COVID-19 based on essentially the same criteria and clinical judgement I am using right now, but it was rare to get a positive case; I would know, because being told you have COVID-19 can be a very stressful experience, so I still personally call every patient I’ve tested who has a positive result in order to answer their questions and help them process that information. This past week I have had to make multiple of those phone calls daily and have been feeling the strain on my time that it has created. As a physician I was on the front lines in May just like I am now, and I can tell you that we are definitely feeling this surge in a way we didn’t then; it isn’t a statistical artifact.
The second kind of data that should inform our understanding of that increase in cases is the number of people who are hospitalized with COVID-19; and the number of people who are dying from it. A raw increase in cases without a change in the test positivity rate could certainly be explained by more widespread testing; but it could not explain why more people had severe enough symptoms to be hospitalized, and there is no question that we have seen an increase in hospitalized cases.

Many people will quickly point out that we don’t know what percentage of those people were hospitalized for COVID-19 related symptoms and what percentage just happened to have a positive test when they came to the hospital for other reasons. This is a seemingly fair argument on the surface, but it is guilty of two fallacies. First is the idea of COVID-19 infection being a coincidence that doesn’t effect the trajectory of someone’s chronic illnesses. For months now I have heard the argument that the people whom we know have the absolute highest risk of COVID-19 complications, elderly people with chronic heart and lung disease, have not died from COVID-19, just with COVID-19. Yes, they happened to have the virus but actually died, in large numbers, from their chronic illnesses all getting worse at the same time, during a surge in COVID-19 cases in their area. This is the tired conspiracy theory that doctors are misattributing the cause of death to inflate COVID-19 death numbers, and it’s one I’ve had to debunk over and over again on this blog; it willfully ignores the pathophysiology of the virus, the normal course of those illnesses, and the way that doctors understand and report contributing causes of death. The idea that we are suddenly seeing a huge uptick in COVID-19 hospitalizations as an artifact of testing patients when they come in and unrelated to the virus itself is just another version of that same conspiracy theory. It’s also a very hypocritical argument, considering the types of sources it is coming from. One of the criticisms about mitigation efforts from the beginning was that people who needed care might not come in to the clinic or hospital because of fear of the virus; it’s a very real concern and a problem I’ve fought against daily as a physician, and have been writing about since my earliest social media and blog posts during the pandemic.

Their argument has been that telling people that the virus is dangerous and taking mitigation measures would discourage them from seeking care for conditions that were really dangerous, like congestive heart failure or blood clots in the lungs, because they were more afraid of catching COVID-19 at the hospital. Our argument has been that the virus is dangerous, and that it also makes congestive heart failure more dangerous and actually causes blood clots in the lungs, so we have an obligation to keep people safe from the virus and help them navigate when and how to seek care for other health concerns; it’s work we are doing constantly in our clinics and hospitals. Now these same sources are arguing that in the midst of a dramatic increase in cases and our first real surge in Texas, thousands of people with conditions that put them at risk for complications from COVID-19 suddenly aren’t worried about the virus after all and are all seeking hospital care at the same time, and just happen to test positive for the virus while they are there. There may well be some situations where this actually is the case, and people who were overlooked by our healthcare systems really are now getting very sick from their diabetes or coronary artery disease at the same time as our surge (you can only ignore a worsening chronic illness for so long before hitting a crisis point), but the idea that this would happen on a broad scale, all at the same time, and that enough of those patients would be positive for COVID-19 that it would cause a state-wide spike in hospitalized virus cases is a very, very, frustratingly silly argument.

The final number we need to consider is the number of deaths, and here at least there is some good news; we are not seeing a substantial increase in the people in Texas dying from COVID-19, at least not yet. There are two ways to understand this. The optimistic way is to think that something has changed; either the virus has somehow become less deadly than before, or our increased understanding of COVID-19 has led to a better ability to fight the virus; improved disease-specific ventilation strategies, effective drug therapies, and more efficacious supportive care measures. In fact, there is a great deal of evidence that the latter really is true, as we will discuss in another post. But the pessimistic view (and the truth is probably a combination of both) is to realize that most people do not just get admitted to the hospital with severe COVID-19 infection and pass away the same day. There is a significant lag time as those patients are treated and fight against the virus, and our surge in hospitalized cases is only a little more than a week old.

Many of those hospitalized patients are fighting for their lives in the ICU right now, as the hospitals are starting to fill up around them and their nurses and doctors are becoming fatigued. Many of those people will recover, but many will not; and it will take a couple of weeks, and often times much longer, to see how many, and who. As we’ve seen elsewhere, the ratio of those who don’t recover will only increase if resources and the margin for careful attention and heroic efforts on their behalf begin to run short. Yes, our improved understanding of the virus and more effective therapies gives us a better chance to fight the virus than Italy had in March or New York had in April; but doubling down on the difficult work of mitigation now to prevent our healthcare systems from being overwhelmed in a couple of weeks when more and more patients reach their crisis point is every bit as important.

