“TJ Webb, nice to meet you”
I’ve actually been thinking about this particular blog post for a while. Ever since I took on the role of being a clinic lead for our system’s very busy outdoor COVID-19 clinic about 6 months ago, I’ve been seeing multiple COVID-19 positive patients, face to face, 3 to 5 (sometimes 6) days a week. Unlike the very high volume, rapid turnover testing-only strategy that is so important from an epidemiology standpoint, these were real medical visits; I heard about my patients’ symptoms and exposure history, we discussed risk factors, we checked vital signs, and I listened to their hearts and lungs. When we needed them, we got blood work or EKG’s, or if the patient was pregnant, listened to the baby’s heartbeat.
COVID-19 is a stressful thing to be seen for, and patients very frequently need more than just a targeted physical exam and a test result. At each visit I provided reassurance, and careful instructions for quarantine or isolation as their clinical situation demanded. I told my patients not to be afraid, and then we discussed what vigilance demanded and a detailed discussion of the signs and symptoms that should lead them to seek further care or go to the emergency department. Sometimes these visits really only lasted 5 or 6 minutes; sometimes they lasted 15-20.
I don’t have an exact count, but I’ve done around 1,500 of these visits since the pandemic started.
Masks are very, very good at preventing COVID-19 transmission, and my N-95 and faceshield are a powerful combination; but they are not perfect. Besides, we know that masks are better at protecting against lower velocity respiratory droplets and work best when worn by both parties. Many times my patients were coughing and sneezing, and some simply couldn’t tolerate wearing their mask for our entire visit because of their shortness of breath or other reasons, so we relied entirely on my own PPE, and the outdoor setting, to mitigate the risk of that face-to-face visit. I knew this would be the case sometimes; it’s the nature of the job.
Because of this, my wife and I have more or less treated my getting COVID-19 as an inevitability (it wasn’t actually inevitable, but it definitely felt that way). So when I recently joked darkly on facebook how nice it was knowing that “if I join the 1,700+ American healthcare workers that have died from the pandemic so far, my $300,000 of med school student loans are non-transferrable to my wife and 4 children,” and then in a blog post on not going home for the holidays said, “My PPE game is strong” and “I’m really, really good at being cognizant of fomites and at personal transmission control,” anybody with even a small amount of Genre Savviness could have told you what would happen next.
Sure enough, following a night of fever and chills and a morning of coughing, sneezing, sore throat, and headaches, I finally tested positive for COVID-19 yesterday afternoon. As someone who diagnoses and treats COVID-19, who writes about COVID-19, and now who has COVID-19, I thought my perspective might be helpful to others, and today I’d like to write about what I will and won’t be doing over the coming days and weeks (specifically as it relates to my diagnosis; nobody wants to read about my Mandalorian costume 3d printing).
5 things I’m not going to do now that I have COVID-19.
1. I am not going to Panic.

One of the biggest communication challenges I face on a daily basis is helping patients understand that a virus like COVID-19 or seasonal influenza can be extremely deadly and devastating in aggregate, but not necessarily dangerous for a particular individual. There are pitfalls on either side; if my patient erroneously believes that there is a 100% chance the virus is going to make them so ill that they end up in the ICU, they will spend the following days and weeks in fear and anxiety, less capable of navigating their symptoms and more likely to over-utilize an already strained emergency medicine system, and easier prey to those profiteering off of the pandemic by selling unproven pharmaceutical and wholistic ‘cures’ (including, sadly, at least a few doctors out there).
But if my reassurances cause them to believe that the virus isn’t dangerous, as many people do despite a now insurmountable accumulation of evidence to the contrary, not to mention the lived experiences of our friends and neighbors, there is a risk that the rest of my cautions and teaching about transmission control will go unheeded.
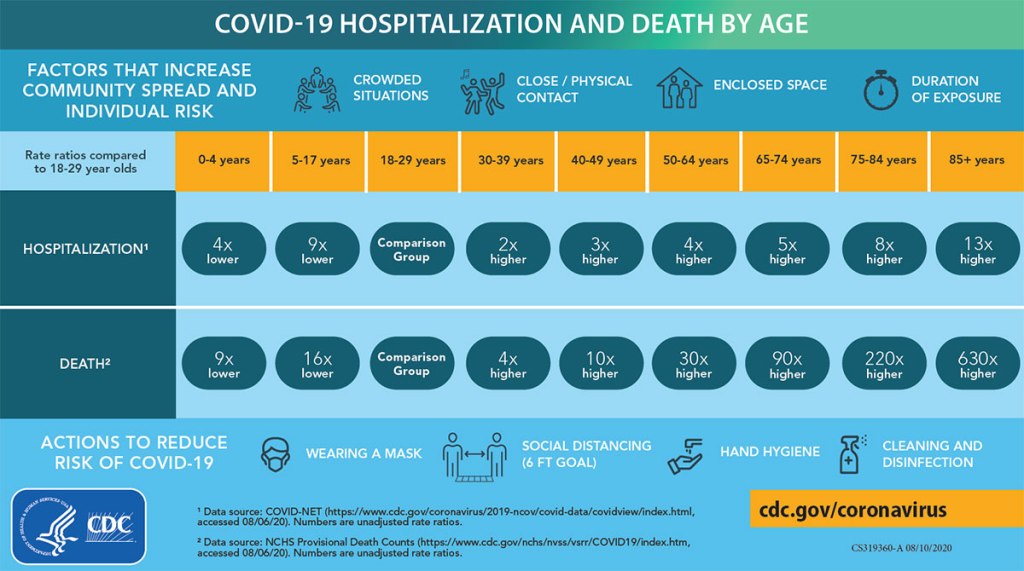
We will look at the numbers in a moment, but this is the most dangerous virus in our lifetimes. The risk an illness presents to a community is based both on how dangerous each individual case is and on how many people contract it. So while any particular COVID-19 case is more dangerous than the flu but far less likely to lead to serious disability, life-long suffering, or death than a case of say Ebola, it is much, much more contagious and will therefore make up the ground easily. And we do not share the burden of risk equitably. We know that the risk of a serious illness and death is greater for those above 50 and far greater for those 65 and older. We know it is greater for those with chronic medical problems, especially those affecting the heart and lungs, multiple medical conditions, and compromised immune systems. But these biological factors are not the only ones at play; people are also more vulnerable if they are part of a marginalized community, and have worse access to healthcare, preventative health, and affordable nutrition. We know they are more vulnerable if they are non-English fluent and therefore have a harder time navigating intricate healthcare systems or having their symptoms and questions understood in a busy clinic or emergency room. We know the poor, especially, bear a greater burden of illness in all diseases, and despite talk of COVID-19 being ‘the great equalizer’, equality just isn’t something American healthcare has been setup to deliver.
I am a white male doctor, 35 years old, in pretty good health, with excellent food access, living in a town with a dozen clinics and two hospitals where many staff know me by sight. I have all the advantages in the world when it comes to surviving this. With COVID-19, sometimes all of that isn’t enough, and we can’t predict and don’t really understand why some healthy young people develop incredibly severe symptoms and die despite our best efforts. But it is, relatively speaking, rare. So I’m not really afraid of this infection for my own sake, but I am taking it deadly seriously because among the many people I love and care about are those who have fewer or none of the privileges I do. And even among those few who are actually at lower risk that me- those who are younger, healthier, and whiter I guess- they are still at some risk, and those characteristics and the privilege they represent are not a perfect protection against this pandemic. So for all of those people, I will be staying home for the next 10 days at least.
2. I’m not going to take unproven medications (and I could get them if I wanted to).
One of the main reasons I have chosen to write about being diagnosed with the virus, instead of just quietly continuing to nitpick viral videos, is because this is really my first opportunity to put my money- or my health- where my mouth is. I’ve been writing about the dangers and sheer impracticability of physicians prescribing unproven treatments like hydroxychloroquine and budesonide since May. Now I have to put those reflections into action, and the outcome will affect myself and my family.
There is a tough kernel of suspicion in the minds of many people that when the doctor tells you there isn’t a specific medicine that will treat your illness, it really just means there’s not a medicine we are willing to give to you. Many people really do believe that there are special treatments reserved only for those who are ‘in the club’: doctors and their families, VIP’s, the wealthy, and those with excellent insurance. If you are a person of color in the US, or belong to any other group that has been marginalized and continues to experience systemic discrimination, there are even good historical reasons to struggle with this suspicion and to find it hard to trust the medical field in general; and not just the Tuskegee Syphilis Study, though it remains the most notorious example. For people with this shared cultural narrative, taking a quick look in my medicine cabinet at home, or those of any of the physicians I have treated for COVID-19 during this pandemic, to see that we are taking the exact same medications and treatments we are offering to our patients may be a good start to dispelling this particular myth; but rebuilding broken trust obviously takes a lot more than that.
I know literally hundreds of doctors; I’ve been learning with them, training with them, and working alongside them for the last decade and a half. This creates a great amount of potential for privileged healthcare access, which we have to be cognizant of and intentional not to abuse (and which is not fully cancelled out by the fact that we are, as a profession, notoriously bad at setting aside time for our own physical, mental, and emotional health). Most of those doctors believe exactly as I do about unproven treatments not supported by evidence; but not all. Even if it took a few phone calls, I could probably find a doctor willing to prescribe me budesonide, hydroxychloroquine, systemic steroids, azithromycin; any or all of the ‘silver bullet’ medicines (besides bleach) that have been touted by viral video doctors convinced by confirmation bias, selection bias, conspiracy theories, and negligible sample sizes.
Why am I not? For the same reasons I haven’t prescribed them (except when they are indicated, like my COPD patients who were experiencing an exacerbation and needed a course of prednisone) for those 1,500 or so patients who have entrusted me with their care during this crisis: Because there is no evidence that they work.
Instead I’m going to do three types of treatments, all of which I recommend for my patients.
- Medications I am already taking.
- Unless specifically recommended by your doctor, you should not discontinue the medications you need for chronic medical conditions. Although it’s always a good idea to revisit your medicines with your PCP and make sure you still actually need them, especially if you are on many medications per day.
- Medications to alleviate my symptoms.
- I take fluticasone and cetirizine for sinus congestion and allergies, and recommend them to my patients when they have similar symptoms. I like guaifenesin for chest congestion, and tylenol and/or ibuprofen for headaches, body aches, and fevers. I may call my doctor’s office and ask for some tessalon perles if this cough get’s any worse, though that medicine doesn’t work for everyone. None of these will cure the virus, but with any luck they will make the next week or two a lot less uncomfortable. Before starting any prescription or OTC medication, check to makes sure it doesn’t interact with your other meds and isn’t contraindicated because of a chronic health condition; your PCP is happy to help you with this.
- Non-pharmaceutical supportive care treatments.
- One day I’ll get around to writing a blog post titled “Your Physician is also a naturopath.” Despite claims that doctors want you ‘locked inside your house’ for the entire pandemic, I encourage my patients to get plenty of sunlight and as much exercise as they can tolerate with their symptoms; just not to do it around people they could infect. We have the privilege of a backyard; for those who don’t we talk about how to be outside but safely distanced while you are under isolation or quarantine. We are also going to talk about the need for additional rest and fluids. If you have a sore throat, we touch on judicious use of chloraseptic spray; but I really emphasize hot water or tea with plenty of honey. I might recommend a nasal decongestant, but I also talk with my patients about safely using a Neti Pot or saline rinse, as long as they don’t have contraindications (and don’t use tap water). I take a multi-vitamin daily and eat a balanced diet, but as long as they aren’t taking amounts that could be toxic or being taken advantage of with expensive, high-profit-margin products, I don’t give my patients any pushback on taking additional vitamins or immune supplements. My recommendations regarding alternative health treatments that don’t have solid evidence are these; they should be safe, they should be affordable, they should not interfere with your evidence-based medical care, and if at all possible they should have a plausible mechanism of action that actually relates to your condition or symptoms. That covers an awful lot, and anybody who claims to be helping you but fails those criteria is probably, quite literally, trying to sell you something.

3. I’m not going to get bored of isolation and decide it’s ok for me to stop early.
That first part is a lie; I’m definitely going to get bored of isolation. I’m strongly extroverted and I’ve been terribly bored of socially distancing for months now. I absolutely love being at home with my wife and four children, it’s my favorite place to be in this present world (besides the Bua Thong “Sticky” Waterfall near Chiang Mai, Thailand); but after 10 days I’m going to be dying (Editor: probably a poor choice of words) to spend an afternoon sitting outside at a coffee shop, or go for a trail run in the park instead of doing laps in our small back yard.
Nevertheless, I’ve heard too many stories of people who decided that since they were asymptomatic or minimally symptomatic, or because they had reached day 6 or 7 and felt better, that their COVID-19 infection didn’t count and they were the exception to those pesky CDC guidelines. Who did I hear these stories from? Mostly from the people they had infected. As much as certain people make ‘freedom’ their rallying cry and rail against so-called draconian restrictions meant to decrease transmission of the virus, the truth is we are pretty much free to follow the guidelines given to us by our doctors and by public health experts, or not, to whatever degree we choose. As much as people talk about the specter of government tyranny related to fighting the pandemic, there really isn’t much we can’t do. I got diagnosed with COVID-19 yesterday, and I could have sat inside at a restaurant or a bar last night; nobody would arrest me. I could sit inside at my favorite coffee shop all day today, and publish this blog entry about me having COVID-19 while sitting there, coughing and sweating and with a hoarse voice, and it’s still extremely unlikely that anyone would say anything to me. Why don’t I? Because of this:



Because with all of that freedom comes responsibility, and because the number of family, loved ones, friends, and neighbors, co-workers, and patients we each lose during this pandemic, which is now in it’s darkest hour, depends on how seriously we each take that responsibility; how deeply we feel the true gravity of our own actions. We are living right now in the failures of our society to do just that. I don’t claim to have been perfect over the past 9 months; but every single one of us needs to stop and honestly consider if there is any area of our lives where we can make different choices in the coming weeks and months to try to prevent even more loss of life.

(This list omits individual days from the Spanish Flu Pandemic of 1918-1920, which killed on average 1,000 Americans a day but came in several very bad waves)
This meme is less than 48 hours old and is already out of date.
Today it would look like this:
1. Galveston Hurricane – 8,000
2. The Battle of Antietam – 3,600
3. Yesterday- 3,055
4. San Francisco Earthquake – 3,000
5. September 11th – 2,977
6. Last Thursday – 2,861
7. Last Wednesday – 2,762
8. The Day Before Yesterday – 2,630
9. Last Tuesday – 2,461
10. Last Friday – 2,439
(11. Pearl Harbor – 2,403)
With hospitals getting overwhelmed, by the end of the month it’s possible
that only the top 1 or 2 will still be on this list.
4. I’m not going to Church.
Our church, Mosaic Waco, has done an amazing job of meeting safely throughout the pandemic. We have “Drive-In Church” in-person but outside and socially distanced every other week, and staff members, volunteers, and congregants consistently wear masks. Our pastors and other leaders have sought out and listened to the wisdom of epidemiologists, physicians, and other experts, especially those who are brothers and sisters in Christ, and understand acutely the difficult balance of goods in deciding how best to gather as believers. They have rightly considered responsible transmission control measures as an essential part of our responsibility to love our neighbors during a pandemic.
All that said, I skipped last week. We were having Drive-In Church and I had signed up to serve, but we were beginning to see signs of illness in our family, and our policy has been to exercise an abundance of caution when it comes to the health of those around us. I’m skipping this week too, obviously, though we are going to continue to attend online. The worship band probably can’t manage without me running the slides, poor things, but the pandemic demands sacrifices of us all.
I bring it up because there has been a popular and persistent narrative that has invaded the Church in America that choosing not to meet in person, or humbly following expert and even pastoral advice for social distancing and masking, is somehow a betrayal of Christian values; even when failing to do so is potentially dangerous for those we name as brothers and sisters and claim to love. We are commanded in Matthew 10:16 to be as wise as serpents and as harmless as doves, and seldom has the interrelationship between these two concepts been as obvious as during a viral pandemic, when our ability to be do no harm to those around us is predicated so strongly on the amount of wisdom we practice, and the amount of wisdom we are willing to receive from experts. Attending your local church in-person, and particularly indoors, when you are ill, under quarantine, or have other reasons to believe you might be at risk of transmitting the virus is as unwise and harmful as it is unloving.
5. I’m not going to make my experience normative.
We’ve talked already about all of the privileges I personally have facing this illness. Except for my age and a minor medical problem or two, it would be hard for me to be at lower risk from this virus. And even though I can’t perfectly predict what will happen, statistically I’m probably going to be fine.
And that’s great, but it does leave me open to a big temptation that I have seen so many people fall into; taking the anecdotal experience of one or a handful of people and using it to dismiss the suffering of millions, including 290,000 of our neighbors who have died in the last 10 months. After each warning, each exhortation to take action now to prevent more disease and death, you will inevitably see someone comment “I had COVID and I was fine.” And we are glad for that, but me or you feeling well and having a mild course of illness says absolutely nothing about the experiences of others. Even deeper than the flawed logic at play here and the willful disbelief and disregard of physicians, nurses, EMS workers, respiratory therapists, and all the others who have shared their own and their patients’ experiences with this crisis, this view betrays a deeply seated arrogance; believing that our own personal experiences are somehow more real than the suffering of our fellow human beings, or the grief of their loved ones.
5 things I am going to do.
1. I am going to take precautions in my own home.
The very first question I get from almost every parent when they are diagnosed with or even tested for COVID-19 is, “what about my children.” I’ve had the opportunity to talk with hundreds of patients about what is an extremely personal and complex decision; how much to isolate and distance from their own children if they have the virus. Thankfully, this conversation gets to start off with one piece of very reassuring data; while children have become very ill and died from this virus, it has been rare, and children and adolescents seem to be the people in our society least likely to experience a severe course of COVID-19.
Nevertheless, the risk is not negligible and it should not be ignored. The degree of caution each of us needs to follow in our own homes when diagnosed with COVID-19 depends on many factors; the ages and developmental ages of our children, how much they depend on us for their daily needs, their individual personalities and the ways they experience love and closeness, the available space in our homes, and the amount of support we have, among others. I have a lot of privilege in a lot of these areas, particularly in having a spouse who takes care of everything with the kids by herself for 50+ hours a week at baseline. If we chose to go the route of many doctors and other healthcare workers early in the pandemic and I moved out for 2 weeks, she would make sure that they didn’t lack for anything except actual time spent with their father.
We have decided not to go this route. Instead, we’ve taken these precautions:
- I am wearing a mask when I’m in close proximity to my family.
- I am washing my hands obsessively.
- I am not letting anyone drink after me (if you have kids, you know exactly how difficult that can be).
- I am not kissing anybody (if you have kids, you know exactly how difficult that can be).
- I am not preparing food (much to everyone’s relief).
- They are strictly quarantining; groceries delivered, no visitors, no birthday parties, no trips to the store or quick stops for coffee.
These decisions become even more challenging when you are caring not for a healthy child, but for an aged parent or a chronically ill or immunocompromised loved one. Again, these are difficult decisions, and we each have to decide for our own families what is the right balance between the need to protect them from the virus and their need to be near us and receive our love, affection, and care in person.
2. I am going to keep fighting for my patients.
Most (though not all) of the misinformation I write about here on the blog contains at least a nugget of truth. Those who have said for the past 10 months that the measures we have adopted to fight the virus are worse than the virus itself couldn’t be more wrong; but they are right about the added dangers of interruptions to care, decreased access, and postponing medical visits, which have all been secondary effects of the pandemic. We’ve been working hard for months (and in the early days of the pandemic were literally working around the clock) to make sure our patients could still get the access to care they need. Even so, it continues to be a struggle.
Having your primary care physician out for 10 days, isolating due to COVID-19, is a huge barrier to care; and it would be even if we had primary care doctors to spare, which we definitely don’t. There are some services or interventions I provide that only a handful of our doctors are trained to, and there are patients whose situations and histories I know all the details of, and even with good medical documentation it would take another clinician a lot of additional work to be brought up to speed with them. There are also patients who simply prefer their doctor and are slow to seek help or accept guidance from any other, which says very little about me personally as a physician but an awful lot about the inestimable value of carefully built, mutual trust and respect at the core of the doctor-patient relationship.
So I’m doing what every other doctor I know does when they are sick: in between naps and bowls of chicken noodle soup, I’m making myself a nice hot cup of tea and logging onto our computer system remotely, responding to telephone calls, refilling medications, and following up on lab results, all trying to make sure my patients have access to equitable care and that the interruptions in that care because of my illness are as few, and as mitigated, as possible. I realize that sounds super braggy, but that’s not my point at all. My efforts are hardly heroic (I once watched a pregnant 2nd year resident in charge of the OB unit receive IV fluids for her hyperemesis gravidarum in between helping other women deliver their babies. I’ve got nothing on that); but I think it’s important that anyone reading this knows how deeply their doctor cares about them and how hard they are working on your behalf, even when you can’t see it.
3. I am going to notify my close contacts.
Done. Unless those close contacts don’t read this blog, of course, in which case they are on their own.

Actually, I’m incredibly thankful that I don’t have anyone to notify. I’ve alerted my teams both at my usual clinic and at our COVID-19 outdoor clinic, since we work together every day. We wear our PPE continuously in clinic, are seldom within 6 feet of each other and never for prolonged periods, and if we have lunch it’s outdoors and very physically distanced; I actually don’t count as a close contact for anyone I work with. We are watching my children and wife for symptoms, and have notified a few people that she has been around out of an abundance of caution even though they also don’t count as ‘close contacts’ by the CDC guidelines. Other than that we don’t have any phone calls to make. It’s a good feeling and I highly recommend it.
4. I am going to finally replace the HVAC ductwork under the house.
Not COVID-19 related, but I’ve been promising to get it done for weeks. Check back with me after isolation and I’ll let you know how it went. #fakenews #misinformation

5. I am going to makes plans in case things go bad, and go to the hospital if my symptoms get severe.
I know this is a two parter, but it’s short and I really wanted to keep the symmetry of ‘5 things I won’t do/5 things I will do’. Back in March when videos began to circulate from overwhelmed hospitals in Italy and France and Katie and I first began to grasp the gravity of the situation, we made a few arrangements. We knew I would be on the front lines one way or another. I made sure she had all of the account numbers for retirement accounts (she handles most of our finances anyway, so bank accounts weren’t an issue), the password to access my life insurance policy, etc. We talked carefully about those non-transferable medical school loans that would be discharged in the event of my death, and about being on guard against predatory offers to “refinance” loans which should, in fact, simply disappear. We talked about burial arrangements and funeral wishes, and how we would want to be remembered to our four young children if we passed. I gave her my list of top 10 guys she was allowed to marry after an appropriate mourning period. We finally got around to making a will.
(this joke included over strenuous objection and my own better judgement)
I also made e-mail addresses for each of our kids for when they are older, and began to send them the occasional note or letter, letting them know just how much I love them and delight in seeing who they are now and the wonderful people they are becoming.
Now that I actually have the virus, we are revisiting these items, I am writing to my kids again, and we are making sure everything legal and financial is hammered out just in case.
The fact is that we expect me to be fine, but we’d be extremely foolish not to take this illness seriously; many younger and healthier people than me have died from it already. I’ve been giving people guidance about what to watch for at home for almost a year now; chest pain, significant shortness of breath, confusion or altered mental status, severe fatigue and malaise, low oxygen levels (we’ve reclaimed my pulse oximeter from our 3 year old’s Doc McStuffins doctor bag), or any acute worsening in overall status. For once in my life as a doctor I’m going to follow my own advice and treat my health seriously, and I’ll be heading in to the ER for further evaluation if I experience any of these symptoms.
Final Thoughts
Doctors and nurses know they are going to get sick; it’s practically in the job description. We have the incredible privilege of taking care of people on some of their best and some of their worst days, but that also means continuously getting coughed or sneezed on, being exposed to contagious illnesses, and occasionally, despite our best efforts, being exposed to a blood-borne pathogen. When it’s a known entity we are familiar with and have been fighting for years, the uncertainty following those experiences is less hard to bear; and honestly after 10 months of this pandemic, having COVID-19 doesn’t feel much different than any of those other old enemies, even if the ‘what if’ factor is a little higher.
I know this post will be met with sympathy, and I truly appreciate everyone’s thoughts and prayers; but I hope the main take away for anyone who reads this rather long-winded announcement of my illness is that what we are doing to care for our patients and asking of each and every person we diagnose with this terrible virus are the very same things we ask for, and demand of, ourselves. If you or a loved one gets diagnosed, I hope you will have symptoms as mild as the ones I am currently having- a little fatigue, a little cough and sore throat, a few chills- hopefully even milder, or none at all. But I also hope you will be just as cautious as we are trying to be; taking the risk of transmission very seriously, communicating with those whom you might have unintentionally exposed, and respecting isolation for you and quarantine for your close contacts as a measure that can absolutely save many, many lives. I hope you are not afraid, and I hope you have all the information and support you need from friends, neighbors, and especially your local doctor.
And to the 300,000 people in this country who have died of this awful virus, the tens or hundreds of millions who have lost loved ones, family, and friends to it, and the 15 million others who have suffered from it physically to one degree or another, I am incredibly grateful to have had the chance to fight it with you and to walk through it alongside so many of you, and wouldn’t change any of that just because of this admittedly mild illness I have now; whether it gets worse in the coming days or not. I’m looking forward to doing it again, as soon as I meet the CDC criteria to do so.
-TJ Webb, Patient
