
You all remember what it was like in January and February before the COVID-19 virus had come to the United States, and before we began to treat it like a pandemic. It seemed like everyone was getting the flu, just like any normal year. The flu shot for that flu season only had about a 45% efficacy- not the worst we’ve ever had, but certainly less effective than we’d hoped- and hospitals were busy treating children, adults, and elders for complications of Flu A and Flu B. And then a couple of short months later…. *POOF!* It was like the flu had just disappeared. We didn’t hear about it anymore, nobody was talking about it; everything was COVID-19.

In March and April we began to see memes questioning why the flu had seemingly gone away. And then a few weeks after that… The memes were gone too, like magic! And for 7 whole months nobody mentioned or thought about the flu. Until a couple of weeks ago, when memes like this began to circulate again:
And although it’s only December 15th and the people posting these memes and #whereistheflu conspiracy theories are shooting their shot a bit early, I think now is a great time to answer the question, “Where is the flu?”
Contents:
-What does a normal flu season look like?
-Why doesn’t the ‘where is the flu’ theory work?
-What did happen to all the flu cases?
-What would you have to believe for these memes to be true?
What does a normal flu season look like?
The reality is that there’s really no such thing as a “normal” flu season. While different strains of influenza circulate in our communities each year, they are all unique in their own horrible ways, and we can’t predict ahead of time when we will have a mild flu season, like in 2015-2016, or when we will have a terrible flu season that threatens to overwhelm our healthcare systems like in 2017-2018, the worst I’ve experienced as a physician. But we can draw some generalizations about flu season:
- It’s going to happen during the Winter.
- People are going to die.
- It’s going to suck.
I hate the flu, and even if we as a society have mostly relegated it to sitcom B plots and ‘man cold’ jokes, the reality is that it’s a killer, and I have patients with chronic respiratory diseases, compromised immune systems, or just poor overall health that I worry about every single year as flu season begins to ramp up.
We typically expect flu season to begin in early Winter, usually November, peak between December and March, and typically to be ended by April. A late flu season might last until May, but that’s fairly rare. However, the last flu season we’ve seen peak in December was back in 2014, and for the past 6 years it has been in January, February, or even mid-March.
So while I’d never fault anyone for trying to get work done early, those ‘Where are the Flu?” memes really would make more sense in January or February, when we would be expecting flu season to be peaking. Nobody finds misinformation claiming that doctors are padding the COVID-19 numbers with flu cases convincing in June and July, so I’m sure they wanted to take advantage of the cold weather for as long as possible.
And honestly I hope we are still seeing those “where is the flu?” conspiracies in February and March because the flu cases stay ridiculously low. That would be a lot better than internet memes saying “oh man, remember back in 2020 when we only had one deadly respiratory virus epidemic to deal with?”
Why doesn’t the ‘where is the flu’ theory work?
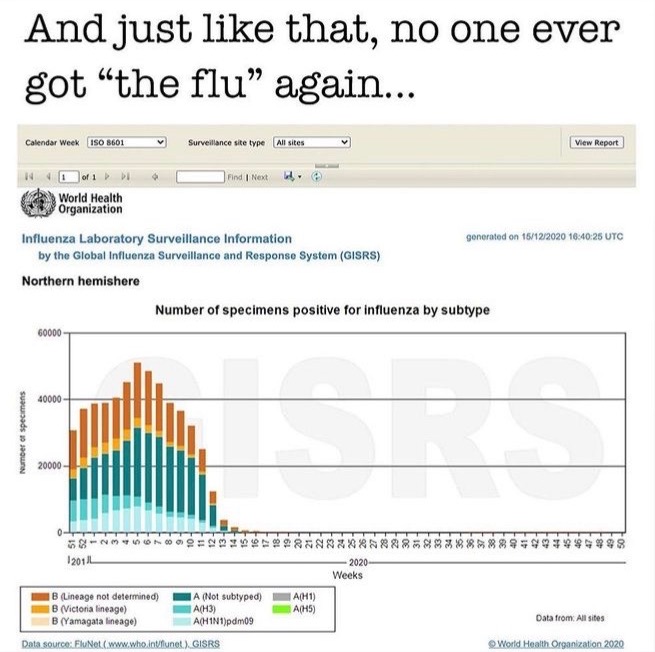
Let’s go back to that first meme at the beginning of the article, which deserves a bit more of our attention. It comes from the WHO FluNet, and anyone in the world can go to that website and look at reported flu cases for any date range going back to 1995. The first thing you’ll notice about the image is that it is on the order of tens of thousands; each major division of the Y axis is 20,000 cases. The image is supposed to convince you that the WHO just forgot to record flu cases at all as a part of this big hoax, but still published their flu numbers with empty charts for the whole world to see. Pretty incompetent conspiratoring if you ask me. But the truth is, that seemingly empty section of the graph is not empty; the 2nd image below is that same ’empty’ time frame, just with a smaller scale.

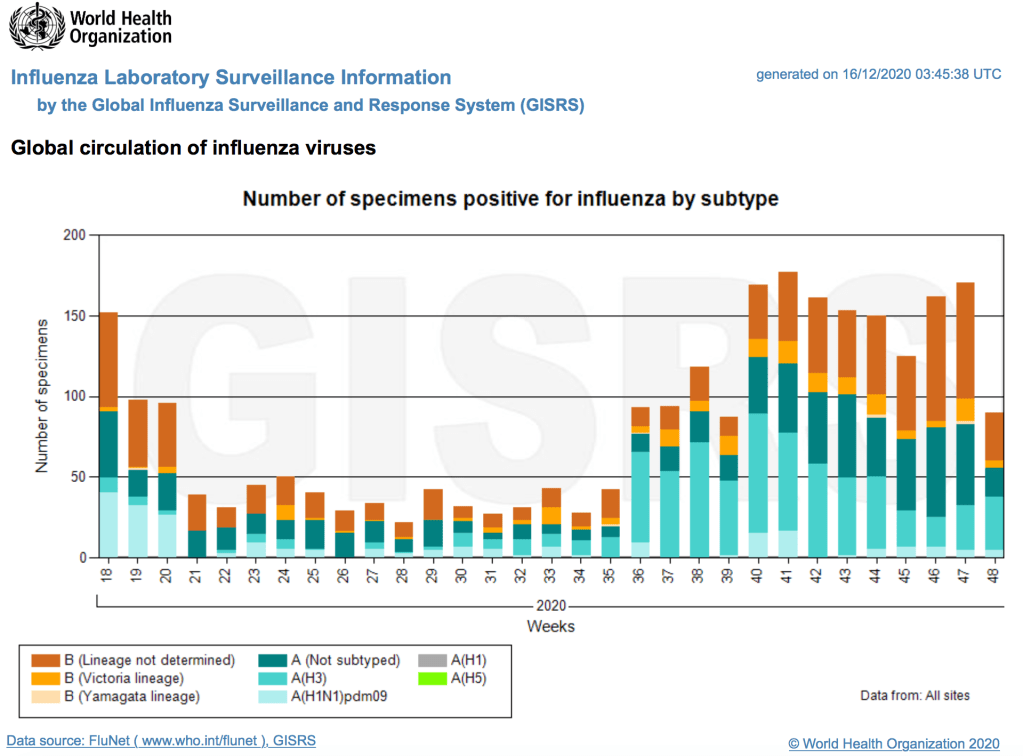
This is still an incredibly small number of cases, but it demonstrates the same week-to-week and seasonal variability flu cases normally follow; that part of the graph isn’t empty, and the data checks out.
In this context, the original image is suppose to convey two ideas; either that doctors have stopped checking for the flu altogether, or that they are ‘stealing’ flu cases and filing them under COVID-19.
The first is easy enough to answer; we haven’t stopped checking for the flu. I’ve just logged onto our electronic health record and I have a message from a colleague about a positive Flu case. We are ordering the tests, and some of them are positive. How reliable flu testing is at baseline is a topic for another day; at the very least it can be compared from year to year to help us understand how relatively bad the flu season is. As a physician I rarely order flu tests, but I’m not the one driving this data; and in fact, with COVID-19 causing similar but not identical symptoms to influenza, I’ve personally been testing for flu more in 2020 than in any year before, because differentiating between flu and COVID-19 is now an additional utility of the flu test; I know several clinicians who are doing the same. We can look at the CDC numbers to see if we are outliers here in Waco, or if doctors are in fact still testing for the flu.

So far, labs that participate in CDC influenza monitoring have tested 232,452 Americans for the flu. At the same point last year, the number of tests reported was 265,670, but instead of having only 496 positive results and a 0.2% positivity rate, we had 15,027 positive results and a 5.7% positivity rate. And while this clearly does not include all flu tests that have been ordered since September, it is a representative sample. So we know that doctors at ordering the tests; the tests are just negative.
That leaves us with the flu cases being stolen somehow. One way for this to happen is for the flu analyzers to be calibrated to call flu tests negative so we can count them as COVID-19 instead (and by logical extension, the COVID-19 machines calibrated to detect flu and call it COVID). The problem with that is that every lab has a different strategy for testing these two viruses. Many labs use completely different machines to test for COVID-19 and flu, and their flu machines have been utterly uninvolved with their COVID testing strategy; untouched, with no updates or software downloads that would cause them to stop detecting flu. There are even lots of clinics that don’t test for COVID-19 at all; have they had their rapid flu tests updated to stop detecting flu, and are now just going through the motions of collecting flu swabs to make some other lab’s COVID-19 results more believable? It’s not just far fetched because of the unbelievable extent of involvement such a conspiracy would require, but because so many people would have to be a part of it even when they are far removed from the COVID-19 testing process and apparently have nothing to gain.
A more parsimonious theory is that the tests are being run as normal, but the CDC is changing the numbers. We track flu tests in the US to determine the positivity rate and understand when flu season begins, when it peaks, and when it ends. We use other metrics like excess mortality to really understand the full impact of a flu season and estimate the number of cases. Right now, the laboratory result tracking is telling us that there just isn’t appreciable community transmission; but what if the CDC has moved all of the positives over to COVID-19? By this point last year there had been 15,027 positive flu tests reported to the CDC. In that same time period this year, we’ve had 9,755,813 new COVID-19 cases (including me!). So those flu cases would represent approximately 0.15% of all of the new laboratory confirmed cases of COVID-19 reported in the US since monitoring for the new flu season began at the end of September. Shifting the flu tests we track to COVID-19 wouldn’t just be a dishonest and transparent strategy for inflating the pandemic numbers, it would also be entirely ineffective and unnecessary. If they just reported flu cases like normal, the COVID-19 numbers would be almost exactly the same, and they’d be far less likely to get caught. If you are trying to embezzle millions of dollars from the bank, you don’t cook up a fake set of books and then turn around and stiff your customers a couple of bucks when they come in to cash their checks, too (I am currently in the market for a much better financial analogy. Please send suggestions to tjwebb@tjwebbmd.com).
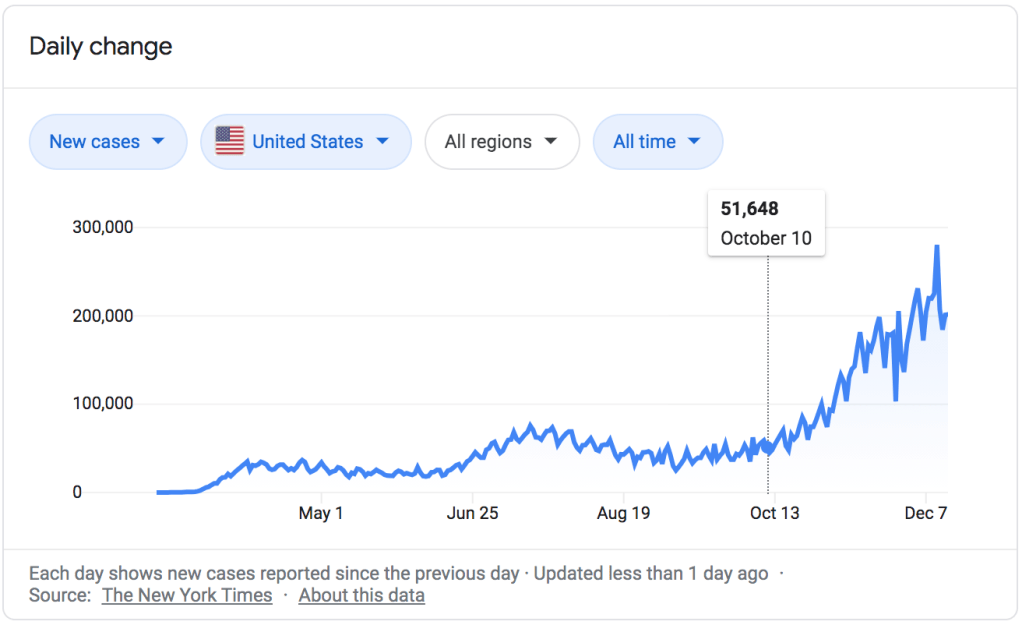
Claiming that the COVID-19 numbers are being inflated with influenza cases also does absolutely nothing to explain two important facts about the pandemic; the pattern of cases over time, and the number of deaths. If we were ever to see even a fraction of the number of deaths due to seasonal influenza that we are right now from COVID-19, especially this early in flu season, we would be dealing with the worst flu since the Spanish Flu of 1918. If that were the case, the flu itself would be a pandemic exactly as bad as COVID-19… So why all the pretending? The numbers also don’t fit the pattern of seasonal flu at all. Look on the graph below and tell me when ‘they’ would have switched to using the flu to generate COVID-19 numbers. October 10th? That’s when cases really began to climb, and that’s too early for flu season. What about the cases in April, or the nationwide surge in July?
The “What Happened to the Flu?” conspiracy is extremely weak because not only does it have no explanatory power, it also has to be combined with multiple other conspiracy theories (like “the doctors are lying on the death certificates“) to work at all.
I think a lot of people find the apparent absence of the flu convincing, and I think I understand where they are coming from. Most of us aren’t used to thinking like epidemiologists. I’m not. We know people who had COVID and were fine, just like we know people every year who get the flu and are fine. If we know someone who died of COVID, as I do, it’s a tragedy; just like it’s a tragedy if we know someone who died of influenza. But we aren’t actually very good at looking at the world around us and intuitively understanding the scale of a normal flu season versus the scale of a global pandemic. So noticing a decrease in one is enough to allow us- if we really want to be convinced- to dismiss or explain away the other; until we actually look at the real numbers.
What did happen to all the flu cases?
The reality is that the CDC and the WHO are reporting such a small number of positive flu tests because… there are a lot fewer cases of the flu. And although experts have told us to expect a particularly light flu season for months, it begs the question; is it really possible for it to be this light?
The answer is yes, thankfully, and for some very good reasons. First, as we’ve been saying, it’s still very early in flu season; we just don’t know how bad the peak will end up being yet, though these early numbers are a very good sign. Second, flu vaccination rates are actually higher this year than last. With the flu vaccine typically being between 40 and 60 percent effective, even a modest increase in flu shots will result in millions of fewer cases. But more importantly, we can expect a light flu season because every single measure we use to decrease COVID-19 transmission decreases transmission of the flu too. Decreased indoor gatherings, wearing masks that block respiratory particles, a significant portion of the population working from home, doing remote learning, and sheltering in place; all of these are going to decrease transmission of influenza even better than transmission of COVID-19. Why better? Because the flu is less contagious, for one thing; it is less efficient at spreading from person to person and therefore it is easier to mitigate with masks and distancing. But even more important is the fact that some of our strategies that are only modestly effective for COVID-19 are actually very effective for influenza.
Take symptom monitoring for instance. Right now every school, daycare and university, and most businesses, are carefully monitoring their students and employees for infectious symptoms like cough, nausea, and fever, and insisting they miss school or work and see a doctor if they are ill. Because COVID-19 is spread even by people who are asymptomatic or who have not yet developed symptoms, this strategy is only effective for symptomatic COVID-19. There is also a long lead time for COVID-19 during which a pre-symptomatic patient can spread the virus before they are sick enough to screen positive and be told to stay home; the incubation period of the virus is up to 14 days or longer, with most people developing symptoms around day 6-7 on average. Prior to this, they are at work and school and don’t realize they can infect others. That’s why this strategy absolutely has to be paired with excellent contact tracing and quarantine for close contacts. But our contact tracing system in the US failed early on, and between American individualist culture and misinformation and conspiracy theories about the virus, quarantine of close contacts has been the single hardest measure to generate buy-in for.

Contrast this with influenza, which has a 1-4 day (average 2 days) incubation window and is far less transmissible in asymptomatic or pre-symptomatic patients. By the time a person is able to spread the flu, they have symptoms of the flu. In normal years a fever or vomiting might cause them to stay home, but they can continue to work or go to school with mild to moderate flu symptoms like cough and sore throat; but not in 2020, when even the social condemnation attached to coughing in public is enough to keep a lot of us at home when our allergies are acting up. Keeping people who feel well in quarantine because of exposure to the virus was always going to be a hard sale, even when that advice is based on solid epidemiology principles. Fortunately, slowing the flu doesn’t depend on that particular strategy.








Is that enough memes? That feels like more than enough. You get the idea.
It also bears pointing out that the mitigation measures for COVID-19 actually have worked, and are working. Those who want to minimize or deny the realities of this horrible pandemic are fond of pointing to the early models that predicted greater than 1 million deaths in the US and asking, “what happened to all the deaths?” But those were predictions about what would happen without mitigation, and having already reached 307,000 deaths with extensive mitigation efforts, those early numbers now feel like low estimates instead of end-of-the-world scenarios. Because strategies to reduce COVID transmission are being followed or ignored to more or less of a degree not in different states or cities but in different houses on your street (and even by different people in your own house), we will never really know which mitigation measures were most effective or how effective they might have been with higher engagement; but it is clear that even with actual levels of adherence, they are even more effective for the flu than for COVID-19, which makes perfect sense when you compare the characteristics of the two viruses.
What would you have to believe for these memes to be true?
Finally, I want us to really stop and ask ourselves, if these memes and commentaries were true, what would we have to believe? First, let’s reiterate that the people creating these mean one of 3 things:
- Where are the flu cases? The flu cases are there, but doctors and the CDC have decided to ignore them altogether.
- Where are the flu cases? A lot of the tests for COVID-19 are actually positive tests for the flu, but they aren’t being reported that way.
- Where are the flu cases? Oh wow! It’s so wonderful that we aren’t seeing much flu activity right now.
Since we can rule out the 3rd one (even thought it is, actually, the one supported by the facts), it has to be some combination of the first two. And in order to find those ideas convincing, here’s what you have to believe.
Warning: Most of what follows is sarcasm.
(so please don’t quote me on any of this out of context)
– Your local clinic doctors (including me), who hate the flu and COVID-19 and have lost patients to both, are waking up every morning, going into work in full PPE, and seeing patients for cough and fever.
– They are spending 10-15 minutes talking face to face with patients about COVID-19, about the safety precautions and how to do isolation and quarantine, what red-flags to watch out for, and offering heartfelt reassurance and telling their patients not to be afraid, but to stay vigilant in monitoring their symptoms. Sometimes they are even praying with them at the end of those visits.
– This is all a waste of breath and they know it. It’s a big sham, and they are play-acting their part. They know full well that whether their patient has a cold, or seasonal allergies, or the flu, they are going to call it COVID-19 anyway (and go ahead and ignore the fact that we are telling people ‘hey I think this is actually just your allergies’ all the time. If we wanted to inflate COVID-19 numbers we could do it all day long. But we don’t and we aren’t). They’ve spent all these years trying to help people fight disease, and now they are going to spend their time lying to people, leaving them less prepared for and knowledgable about the disease they actually have. And because they don’t give you a new patient panel when you sign up for a global conspiracy, they are actually lying to the same people they’ve spent all of those years trying to help as their primary care doctor.

I just really like this movie.
– They order a COVID-19 test and the nurse collects a sample and brings it to the lab tech, who places it in a machine to test for COVID-19; maybe they are also running a flu test for that patient. But the flu analyzer has been programmed to call the flu test negative and the COVID-19 analyzer has been programmed to call the flu COVID instead. Why test for anything at all; why not just call a certain percentage positive and have done?
– The clinic doc gets the fake COVID-19 test back and tells you it’s positive, and advises you to isolate for 10 days. This is because they… Hate your job, I guess, and want to make you stay home so you won’t get paid? I mean, I write letters for patients to help them get work accommodations for their medical conditions all week long, and I even call managers, bosses, and HR reps to make sure my patient isn’t at risk of losing their job because of a medical issue. I’ve helped people with their depression and anxiety every day for years, a lot of it because of financial difficulties. I’ve even connected people with legal resources so they could fight to keep working when they were wrongfully terminated because of their health. But sure, I guess it makes sense that I want my patients to face more financial hardships and want their lives to be worse. That’s what really lights the fire under us to make all those sacrifices in medical school and residency.
– The doctor knows you have the flu, but instead of seeing if you are one of the people that might benefit from Tamiflu (it’s not as good of a medicine as you might think), they withhold that medicine because offering it to you would give away the game, and of course their commitment to this fake pandemic is greater than their commitment to helping their patients or their Oath.
– You ask the doctor about your young children; are they going to be ok? Even though they know that children under 5 (including two of my own), and especially under 2 are at high risk for complications from the flu, they go ahead and offer fake reassurances. “I don’t want you to be afraid,” they say, “thankfully, your children are at much lower risk from this virus than even a healthy young adult.” That probably eats at them a bit, lying to you about whether or not your kids are in danger; but they are just really committed to this conspiracy.

– Meanwhile, by the way, their colleagues in the hospital are spending even more hours and making even more personal sacrifices to treat incredibly sick hospitalized patients. Instead of treating them like normal pneumonia, flu, and heart attack patients, they are calling them all ‘COVID-19’ and treating them with steroids, prone positioning, anti-virals, and convalescent plasma; all to maintain the ruse. It wouldn’t look good for the numbers to only be bad in clinic.
– Finally it’s time for the doctor and the nurse and the lab tech to send their fake lab results to the county health department, and then on to the CDC. Here the CDC, rather than reporting fake numbers that perfectly match their false narrative, will carefully tabulate the fake lab results they’ve received from all over the country, throwing in a few positive Flu cases and different flu strains (including some their experts didn’t recommend we vaccinate against) just for good measure. Seems like an awful lot of trouble.
Also, by having an incredibly mild flu season and diverting all of those flu numbers to COVID-19 (even though, again, they aren’t really needed), they allow graphs like the one in this article that make it really obvious to any conspiracy theorist on the internet what’s going on. Such an intricate conspiracy, but so poorly executed.
And why do we do all of this? Well, because fear of the pandemic helps shutdown the economy and hurts your political candidate, according to one theory (I still don’t know how they convinced all of my conservative, Republican doctors to go along with it). You would think there’d be an argument that two contagious killer viruses might convince people to stay home even better than one… Or, according to another theory, to sell COVID-19 vaccines for big pharma. Because everyone knows I get daily instructions from my pharmacy sales rep masters, instead of, you know, barely tolerating being forced to occasionally interact with them so I can get some free insulin samples for my patients. I suppose flu shots just aren’t as profitable.

Which brings up another good point. Besides the doctors and nurses and lab techs and of course the CDC, who else would need to be complicit in this scheme? Well, Hoffmann-La Roche Inc. and Gilead Sciences, for one, the manufacturers of Tamiflu. I don’t prescribe it much myself, but during flu season it’s one of the most commonly prescribed medications. That company also makes Remdesivir, one of the medicines used for certain COVID-19 patients; but only in the hospital. Bad work on their accounting department, sacrificing most of their sales from a widely prescribed outpatient medication to focus exclusively on an inpatient medication prescribed only for some patients.

I’m not willing to put anything past drug companies, but it does seem like allowing for a ‘normal’ flu season would at least help them hedge their bets a bit. Then again, Tamiflu is available as a generic now too, so maybe this is a corporate high risk, high reward gamble. Let’s move on.
Who else would have to be complicit in it? These guys:
Sanofi Pasteur, Inc
Seqirus, Inc.
GlaxoSmithKline Biologicals
Protein Sciences Corporation
MedImmune, LLC
Recognize them? Those are the top manufacturers of seasonal flu vaccines, and none of them has a COVID-19 vaccine (at least not one close to being approved). The companies that make the two vaccines currently approved or about to be approved for COVID-19, Moderna and Pfizer, do not have seasonal flu vaccines.
You write the script. Powerful, multi-billion dollar pharmaceutical companies that have lost the race to create a vaccine against a hoax virus (or didn’t even try), and now are missing out on all of that sweet, sweet COVID money. They know it’s a hoax and more than likely have some proof. So what do they do? They expose it for what it is, involving their competitors in scandal and allowing them to grab a greater market share and keep their flu vaccine as the most important vaccine of 2020. Except that’s not what they’ve done; if you go to any of their websites, you are going to see messages saying, basically, “good job on developing those COVID-19 vaccines you guys, we are rooting for you.” Sincere? Who knows. But definitely not the type of corporate warfare you would expect if they knew the virus wasn’t really that dangerous and were missing out on all the fear-monger profits.
Now, I know what you are going to say. ‘Fine, maybe it isn’t the doctors and nurses, maybe it’s just the CDC and the WHO. And hey, thanks for not including me in your global conspiracy. Let’s say that this is a regular flu season, or even a particularly bad flu season. That means that say hundreds of people a day are dying (or 3,000, if you are saying all COVID-19 cases are really the flu), and hundreds of thousands are getting the flu, and the doctors are… What? Too dumb to know the difference? Too lethargic to figure out what’s flu and what’s COVID-19? If we aren’t in on it, then we are either too dumb or too complacent to notice it; you know, the two primary things doctors are known for, being stupid and lazy. Every day at our COVID-19 outdoor clinic I hear the same conversation between doctors that are floating there to help; “have you guys seen much flu yet?” And every day I hear the same answers; “not really” and “I’ve had a couple.” If we were in the midst of a bad flu season right now and it were being covered up, you’d have hundreds of thousands of doctors, nurse practitioners, physician assistants, nurses, and all sorts of healthcare workers blowing the whistle, not just a couple of drug reps posting their text messages on Parler. Instead what those clinicians are saying is, “COVID is really bad right now. Please wear a mask. Our hospitals are overwhelmed; thank God the flu isn’t bad right now too.”
