
Contents:
How do these vaccines work? 12/24/2020
Will the vaccines have any lasting effect on my body? 12/26/2020
What about infertility? 12/26/2020
Aren’t the vaccine ingredients toxic? 12/29/2020
If I get the vaccine, can I still transmit/spread the virus? 1/7/2021
Other COVID-19 vaccine posts and links
Intro: Talking about vaccines as a Family Medicine doctor
As a Family Medicine Physician, helping patients navigate uncertainty and doubt around vaccines has been a part of my day-to-day job since long before the COVID-19 pandemic. I have always tried to approach those conversations with patience and understanding (not that I’ve succeeded each and every time), knowing that behind their questions and even suspicion there is, without exception, a deep desire to do what is best and safest for themselves and their families. I get it; vaccines can feel scary. They are pretty mysterious for most people, and there is so much controversy over them that our intuition tells us surely some of it must be true (even though the people who creating it are often intentionally deceitful). I am a father of 4 myself and understand how strange and frightening it can feel to have your child undergo any medical procedure; but unlike an infusion of antibiotics or a dose of tylenol, or the sedated lumbar spine MRI my daughter needed for tethered cord syndrome when she was 1 year old, vaccines are given to children who are healthy to prevent future illness; it makes the decision harder, because the reason for the treatment isn’t readily apparent or at the forefront of our minds.
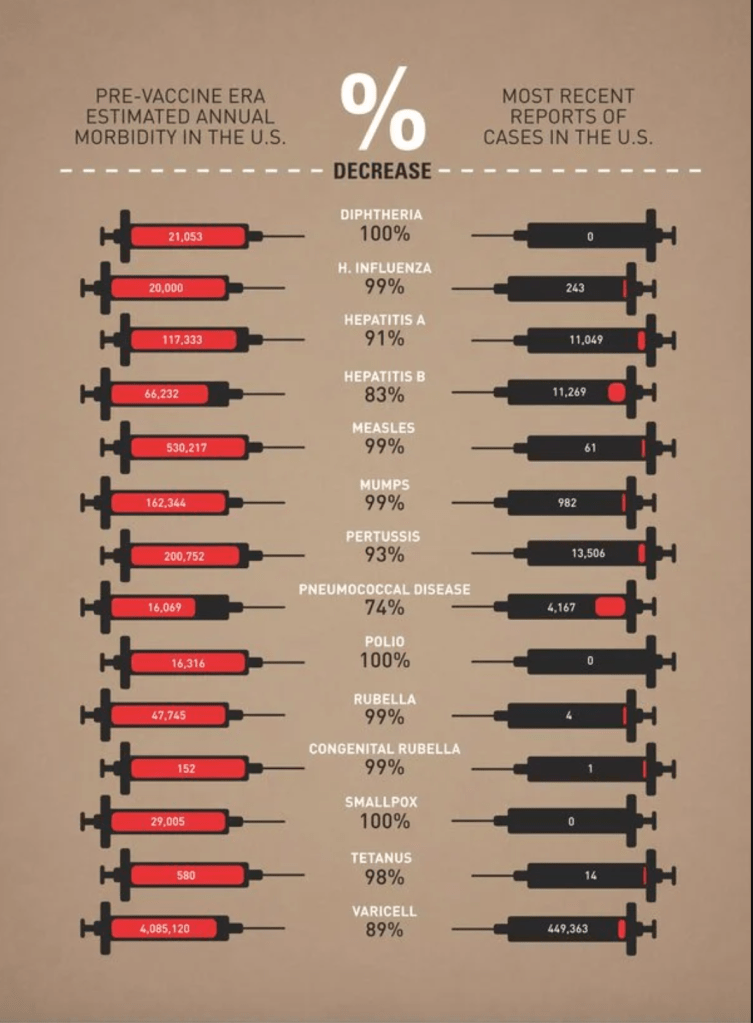
Vaccines are also one of the single most important innovations of modern medicine, and have saved millions of adults and children from dying of some of the worst and most painful infectious diseases that afflict humanity.
That’s why it’s incredibly important to me that my patients have the time to ask their questions and why I believe they deserve careful, sincere, and thorough explanations. So when I think about all of the medical misinformation that is out there right now around the COVID-19 vaccines and how we can possibly alleviate those fears, I start by imagining a patient sitting across from me in my clinic exam room with doubts, uncertainty, or even trepidation about these new and rapidly developed vaccines, and try to write out how I would try to answer their questions.
𝐇𝐨𝐰 𝐝𝐨 𝐭𝐡𝐞𝐬𝐞 𝐯𝐚𝐜𝐜𝐢𝐧𝐞𝐬 𝐰𝐨𝐫𝐤?
Updated 12/24/2020
When discussing vaccines with my patients, I always, always start with a brief discussion of how they work. It’s not uncommon to hear someone say “I think it’s better to rely on my own immune system” when discussing vaccine preventable illnesses. We’ll talk about this in more detail later on, but my first response is usually to help my patients understand that that is exactly how vaccines work; by relying on your own immune system.
Our immune system is designed with two strategies for fighting infections. The first is non-specific but immediate; in addition to our innate protective barriers like skin, hair, and mucous, we have cells like macrophages, mast cells, and natural killer cells that are able to detect and attack any foreign invader that the body recognizes as not being part of itself. This is a good system and prevents you from getting sick all the time; without it, we would be constantly fighting illness and infection from normal everyday exposures, just as many do who have compromised immune systems.
But even more powerful is our adaptive immunity, which is directed specifically against infections our body recognizes and has dealt with before. This is an incredibly robust system of B and T lymphocytes and antibodies that recognize the invading pathogens and kill them with a higher degree of efficiency and precision. The only problem with it is that it takes time to kick into gear the first time your body is exposed to a new infection; and then it’s a race to see whether it can become active enough, fast enough to prevent an illness from becoming severe. On subsequent exposures, that response is much, much more rapid; so much so that you usually don’t even know you’ve been re-infected with that bacteria or virus because you don’t get sick.

The principle behind vaccines is simple; what if we could safely teach the adaptive (specific) immune system to recognize the deadliest infectious diseases, so when someone is exposed the first time they can mount that powerful, targeted immune response right away and not even get sick?
And that’s exactly what these COVID-19 vaccines are designed to do, just like all of the vaccines before them; they give the body the information it needs to mount a robust immune response with the adaptive immune system as well as the innate immune system, without any possibility of causing an infection in the process. So when someone asks, “wouldn’t it be better to rely on our own immune system?” my answer is, “Yes, absolutely! And vaccines allow us to rely on our entire immune system, not just the weaker half, without even getting sick.”
We will talk about the differences between how traditional vaccines and the mRNA vaccines accomplish this later (and whether or not they re-write your DNA). For now I’ll just say that the new vaccines are even closer to naturally acquired immunity than traditional vaccines, because they trigger our immune system almost exactly like the viruses themselves do.
Will the vaccines have any lasting effect on my body?
Updated 12/26/2020
Hopefully! That’s sort of the idea. While the messenger RNA only survives for a few minutes before degrading, the antibodies that are produced will circulate for months, and some of the other cells of the adaptive immune system, specifically the antibody-producing plasma cells, will hopefully migrate to the bone marrow and lie dormant for decades, which is how vaccines given in childhood continue to provide protection many years later. This is true of the annual flu vaccine too, by the way; the issue isn’t that those vaccines don’t provide lasting immunity, but that influenza is a rapidly mutating virus and different strains are more common every flu season. So your flu shot from 1997 or 2008 is still providing you with protection… But only against the flu strains that were chosen for the vaccine in 1997 and 2008. They’ve even done studies that showed people who survived the Spanish Flu Pandemic of 1918 could still produce an antibody response 100 years later! Coronaviruses mutate much more slowly than the flu, but it is too early to know whether SARS-CoV-2 will mutate enough or in the right way to require additional, regular vaccinations. If we can judge by the SARS and MERS epidemics of 2002 and 2012, it seems unlikely.
As far as other changes to our bodies, thankfully there is no plausible mechanism by which the COVID-19 vaccines could cause other chronic changes than the desired immune response. The mRNA only codes for a few specific proteins and cannot produce an active virus, and the fats, sugar and salts in the vaccines do little else than package the mRNA and help it get into the cell.
What about Infertility?

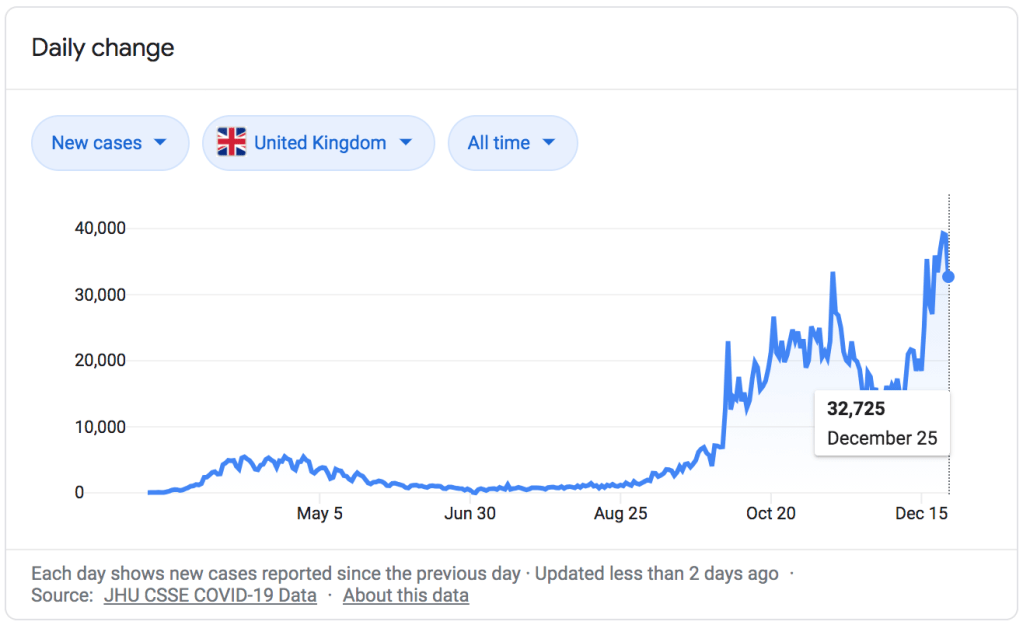
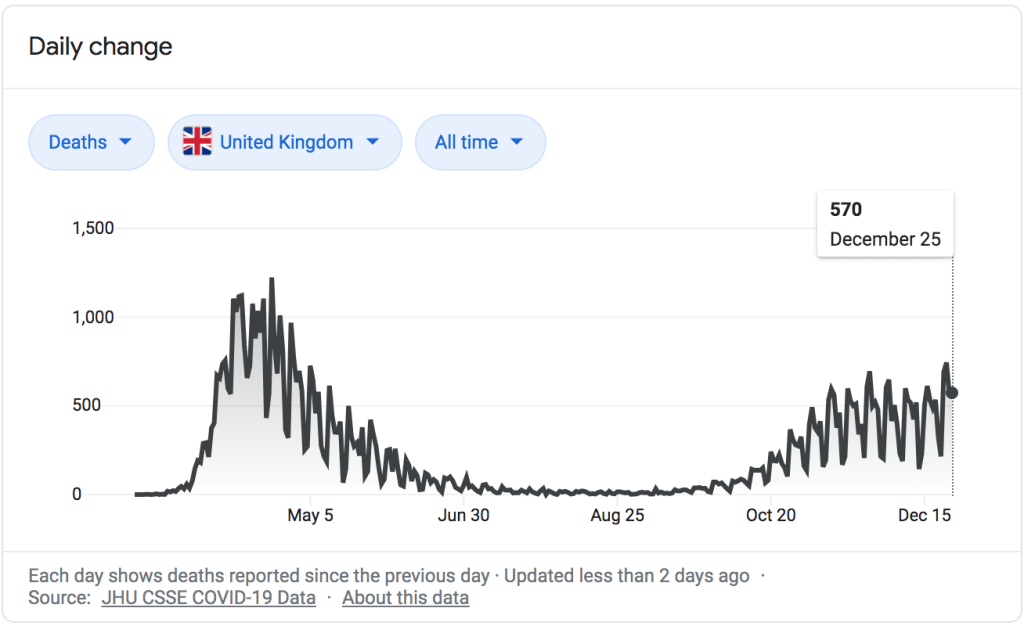
There has been misinformation circulating online about the vaccines causing female infertility, but these are baseless. The original claim can be traced back to Michael Yeadon, a former Pfizer researcher and COVID-19 denier who has also posted videos claiming that the pandemic really ended in late Spring, at least in the UK, because most of the population was already immune due to having antibodies to other coronaviruses, which cause the common cold (as of today there have been over 70,000 deaths in the UK from COVID-19). This is an extremely ironic idea in light of his claims about the vaccine causing infertility, as we shall see shortly. He has not worked for Pfizer since 2011, and calling him the “Head of Pfizer Research” is just as deceptive as the rest of the headline and article.
The vaccine does not contain a spike protein called Syncytin-1, at all; the article above is simply lying at that point. The actual theory claims that the COVID-19 spike protein the vaccines code for shares similar amino acid sequences with a human protein, Syncytin-1, which is important in placental development. They reason that antibodies trained to attack COVID-19 would also attack Syncytin-1, causing infertility. This is illogical and scientifically invalid for a few reasons.
First, we have already had 80 million cases of COVID-19 worldwide and there has been no evidence of infertility as a side effect; yet the body of any infected person is going to produce antibodies against multiple COVID-19 proteins, including the spike protein in question. If the antibodies we develop against the spike protein from having the virus don’t attack Syncytin-1, there is no logical reason to believe vaccine-induced antibodies would either.
Second, we have evidence from the COVID-19 vaccine trials themselves that pregnancy occurs at similar rates between those vaccinated and those not vaccinated. The vaccine trials did not include pregnant women or women who intended to become pregnant, and all women of child-bearing age that participated had a negative pregnancy test before their first dose and committed to using a method of birth control throughout the study. Thirty-nine women became pregnant anyway; twenty-three in the Pfizer trial and sixteen in the Moderna trial, and the rate of unintended pregnancy in those who received the vaccine was about the same as in the placebo group. Those numbers are too small to draw serious conclusions, but the point is that we already have examples of women who became pregnant after receiving the vaccine, even though they were actively preventing pregnancy; in the coming months as more and more people receive the vaccines, we will have many more examples, and because this misinformation has been popular there are already studies planned to track the pregnancy rate following vaccination.
Third, the number of amino acids in the shared sequence is actually tiny; a segment of 5 amino acids, with only the first two and the last two being shared. Syncytin-1 has a full sequence of 538 amino acids, and the COVID-19 spike protein itself is 1,273 amino acids long. We have an analogy in human disease; one explanation for rheumatic heart disease following streptococcal infection is that certain proteins in the Group A strep bacteria share similar amino acid sequences with myosin, a protein found in heart muscle, allowing antibodies against the bacteria to cross-react with heart tissue. However, in that case there are not only much longer sequences of shared amino acids, but multiple sequences that repeat multiple times each. The section of shared amino acids in the case of Syncytin-1 and COVID-19 antibodies just isn’t significant, and you will find many viruses and bacteria in nature that share such similarities with a great many proteins in humans.
Finally, SARS-CoV-2 is not the only coronavirus in existence; not by a long shot. Coronaviruses are one of the main groups of viruses that cause the common cold, and you and I have both had many coronavirus infections throughout our lives. You still have antibodies to those coronaviruses, as Dr. Yeadon points out in his other videos. Every single coronavirus has spike proteins (that is what gives them their name; they form a halo, or corona, around the virus when you look at it through an electron microscope), and all of those spike proteins share as much or more similarity to Syncytin-1 as the COVID-19 spike protein, because they play similar roles in viral replication to what Syncytin-1 does in placental development (they are fusion proteins). So you have already developed antibodies against coronavirus spike proteins all throughout your life, maybe even every single year, just like everyone around you; and yet this has never been identified as a contributing factor in human infertility.

So yes, the vaccine will have a lasting impact on your body, assuming you respond well like 95% of clinical trial participants. The lasting effects will be the same as the lasting effects of surviving the virus: immunity to COVID-19, and hopefully long-lasting immunity. The difference is that the vaccine doesn’t carry a risk of serious illness or death to you or transmission to those around you. And thankfully, neither immunity from getting the vaccine nor immunity from getting the virus itself will cause infertility.
Aren’t the vaccine ingredients toxic?
Updated 12/29/2020
Those whom I interact with regularly who are undecided or hesitant about vaccines are typically patients and parents with sincere, legitimate questions, who deserve the time it takes to hear their concerns, answer their questions completely, and offer reassurance. But unfortunately, there are also people out there who are promoting anti-vaccine propaganda and deliberately creating false narratives. One common strategy to increase unease or paranoia about vaccinating our children is to simply list the scientific sounding ingredients and then ask, “do you really want to put that into their bodies?” Usually this approach will ignore benign sounding ingredients like “sucrose” or “gelatin”, and focus in on lengthy or scientific-sounding ingredients like “nicotinamide adenine dinucleotide” or “cetyltrimethylammonium bromide,” which register emotionally as more intimidating, less safe, and less natural. Of course we know that logically a chemical with a long name would not necessarily be any more or less dangerous than one with a short name; “ricin” has a short name, and it’s the 5th most dangerous chemical in the world (that is just an example; there is NO ricin in your vaccines. I do not want to see a bunch of memes next week claiming they put ricin in vaccines). But fear mongering is not always logical.
They might also home in on a naturally occurring and well known chemical that most people think about in conjunction with another of its uses, counting on that association alone to create fear. A good example is formaldehyde, which most of us think of in the context of embalming, but is also used in applications from color photography to deodorants; and of course, as an anti-bacterial and anti-fungal in certain vaccines. Some vaccines contain about .005 to .01 mg per dose; a 2 month old baby produces up to 200 times more than that every single day as a part of their normal metabolism (for adults, it’s more like 3,000 times more). Yet because our culture so strongly associates formaldehyde with death, merely invoking it’s name is enough to create unease.

Most of the ingredients in vaccines are there to keep the attenuated or killed virus pieces from decaying long before they are injected. Others are there to prevent the growth of bacteria or fungi in the vaccine vials themselves. Still others are used to stimulate the body’s immune cells around the injection site to make them more likely to produce an adequate response that leads to long-term immunity. All chemicals we encounter in our lives are toxic under certain circumstances; none of the ingredients in vaccines are toxic at the doses or in the manner given. I think people often forget that the scientists who design the vaccines, and the doctors and nurses that counsel patients about them and inject them, are human beings who also vaccinate ourselves and our children; we want vaccines to be safe for selfish reasons, too, not just altruistic ones.

That all applies to traditional vaccines; the new mRNA vaccines are made differently, and so they don’t need a lot of the same additional chemicals to ensure they work. In fact, what’s shocking about them is just how few ingredients they actually have. In addition to the messenger RNA molecules themselves, the Pfizer vaccine has just 4 synthetic fats (lipid nanoparticles) meant to deliver the mRNA into the cells that will build the COVID-19 spike protein, 4 salts to make sure the vaccine is at the same acidity and osmolality as the tissue it is being injected into so it can get absorbed (and hurt less), and 1 sugar, sucrose, to protect the vaccine during cold storage.
Salt, fat, sugar. And that’s it.
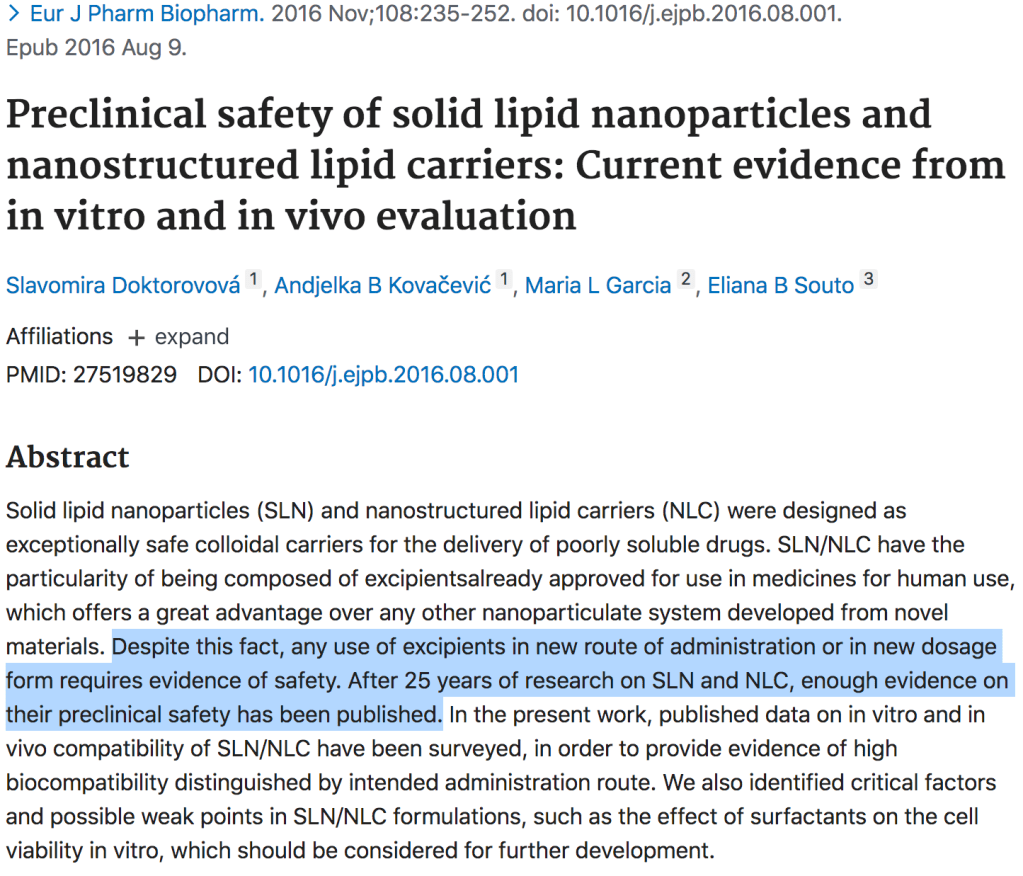
Some of the substances can still cause a reaction; the leading theory right now is that the few anaphylactic reactions to the Pfizer vaccine were likely due to polyethylene glycol, a common chemical we give in huge doses for constipation, but which can cause an extremely rare, but serious, allergic reaction. This chemical is used to create the lipid nanoparticles through some Tony Stark level methods I can’t hope to understand. The lipid nanoparticles (very small fat molecules that can protect the mRNA) themselves are indeed new technology; which in science terms means about 30 years old. Over that time period their safety has been studied extensively and found to be safe, non-toxic, and biocompatible/biodegradable. And because the world is crazy, no, they are not tiny robots (but how cool would that be?!).

The math checks out.
I can’t claim to be familiar with every anti-vaccine meme and article out there, but I haven’t seen as much about ‘toxic ingredients’ with the COVID-19 vaccine, and I think that’s because even compared to the safe ingredients of traditional vaccines, the ingredients of the COVID-19 mRNA vaccines just sound very unimpressive, and thus feel less intimidating.
If I get the vaccine, can I still transmit/spread the virus?

This is a question I’ve heard frequently, especially from those who themselves work in healthcare or have vulnerable friends and loved ones. It is a question driven by compassion. In this blog we have been trying to address the fears and concerns that arise not only from conspiracy theories and misinformation, but also from the very small but real risk associated with the vaccines; yet I know that many people would brave whatever degree of risk to themselves (again, It’s very small) if it meant protecting their family and community. If they could be guaranteed that their choice to get vaccinated meant they could safely visit an unwell grandparent or have coffee face to face with a friend without any risk of spreading the virus, it would be a no brainer even if there was a considerable risk it might cause significant side effects like Bell’s Palsy (there isn’t).
And I wish I could give that reassurance today, but while I can say that the chances are very good this vaccine will not only protect you but also protect those around you, we still need much more data to be able to quantify the degree of that protection.
The point of the vaccines is to provide your systemic adaptive immune system, the part that acts powerfully and rapidly against specific disease, with the information it needs to produce the antibodies you need to keep you from getting very sick. A common misconception is that after you get say the flu shot, you can’t get the flu. It’s not true. The flu shot doesn’t give you a magical forcefield around your body that blocks flu virus, it just helps you fight it much, much more quickly and efficiently when you do get it; often to the point that you never even know you are infected, or at least only have very minor symptoms. Vaccines drastically reduce the chances of you becoming extremely ill from deadly disease like influenza, measles, or COVID-19; that’s their job.

He’s the best he is at what he does; but what he does is not immunology and pathophysiology.
This main function of vaccines is what underpins the epidemiology strategy of giving the COVID-19 vaccine to healthcare workers and the most vulnerable first. The medically vulnerable, because they are the most likely to require high levels of care, to suffer long-term problems from infection, or to die from COVID-19; and healthcare workers because as the pandemic worsens it becomes more and more important to preserve our medical workforce, and vaccinated folks are less likely to need sick time (much less become seriously ill and require hospitalization themselves) for COVID-19. The other reasons for vaccinating healthcare workers go back to courage, trust, and solidarity with our patients in the face of any new treatment. We are prioritizing vaccinating the vulnerable instead of say pathologic extroverts because the effectiveness of the vaccines at preventing significant illness is known (90-95%), but their effectiveness at preventing transmission is still unknown.
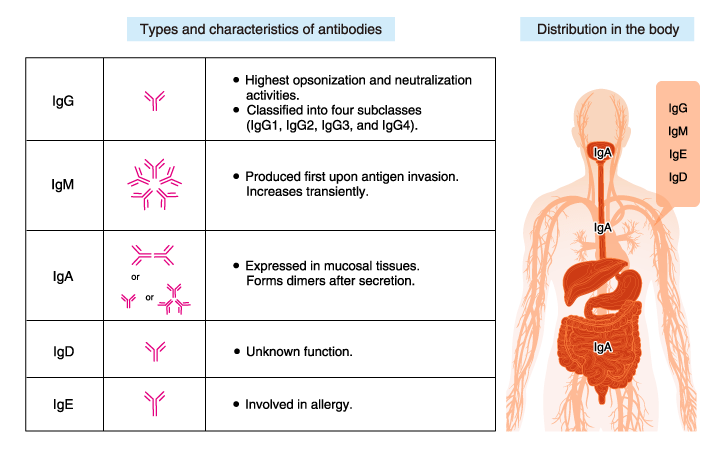
So how do we find out so that Dustin can get his vaccine? Well, the big question mark is IgA antibodies. Most of the research on antibody production from COVID-19 vaccination focuses on IgM and IgG because they predominate in the blood and represent, respectively, our short-term and long-term antibody protection against systemic (whole body) illness. But IgA is the main antibody in the mucous membranes; your mouth and throat, nasal passages, lung surfaces, and digestive track (it’s also the antibody responsible for passive immunity transmitted through breastmilk), and we know that the IgA response to infection is a big, big part of what neutralizes the virus and decreases transmission in those first 10 days of symptoms. If the vaccines “only” cause a significant IgG and IgM response during that post-vaccine exposure to the COVID-19 virus, it will prevent severe infection; and may still prevent enough viral replication to slow transmission. But if it produces a strong IgA response too (or a strong enough mucosal IgG response), it will almost definitely neutralize any live virus in the upper airway as well, making transmission as unlikely as severe illness. In other words, the degree of IgA response is a strong predictor of whether the vaccine protects those around you as well as it protects you.
Because of this, researchers are already studying the degree of production of mucosal IgA against COVID-19 in vaccine recipients, with some promising results, and at least one intranasal vaccine (which produce a very strong IgA response) is under development. And while the best information we could get would be to see exactly how well someone develops IgA and neutralizes the virus by studying them when they are exposed to COVID-19 after vaccination, it’s sort of hard to catch people in that window. In the end we will probably have to settle for epidemiology data instead; carefully watching to see if clusters of infection occur around exposed, asymptomatic vaccinated people at the same rate that they do around unvaccinated people. That will take time, but if and when it becomes apparent that vaccinated people really aren’t spreading the virus to those around them at all, that will be the point I’ll stop wearing my mask, practicing social distancing, and washing my hands (fine, fine; I’ll keep on washing my hands).
I realize this was a really long-winded way of saying “I have no idea,” but I want to conclude with a few reasons you should get the vaccine even if your main concern is not spreading the virus to others. First, there is already a lot of good data that supports the idea that these vaccines will provide mucosal immunity (and thus decrease transmission), both from studies of the COVID-19 vaccines themselves and from our much more robust knowledge of vaccines in general; it’s hard to say anything with much confidence yet because we’ve had these vaccines for such a short time, but I’m pretty optimist they will. We’ve followed these principles for years; we recommend everyone around a newborn be vaccinated against Pertussis (whooping cough) because the newborn can’t be, and we know that vaccine-derived herd immunity works even for viruses that are primarily spread through respiratory particles. Second, there is no conceivable mechanism by which they would increase transmission. The vaccines cannot make you produce live virus (at all) so they can’t make you contagious, and if you are exposed to COVID-19 later on your body will still respond with a mucosal immune response whether it is augmented by your vaccine or not (and it probably will be); the vaccine won’t stop that. And third, by preventing a severe systemic illness, the vaccine will decrease the amount of time you are shedding virus and prevent transmission in some of the most high-risk settings; aerosol producing procedures like nebulizer treatments or intubation in the hospital. And by preventing symptoms like coughing and sneezing the vaccine will make you less contagious when exposed to the virus, as long as you are still following other transmission control measures like wearing a mask and quarantining after exposure.

So no, unfortunately being vaccinated against COVID-19 does not give us carte blanche to schedule giant indoor parties, throw away our masks, and treat the pandemic as if it were over; but they are a huge step in that direction, and in addition to protecting ourselves they do have a fair, if yet unproven, chance of protecting those around us too. And besides, if you don’t get vaccinated, how are you going to get your government tracking microchip?
Bad joke, sorry.
Other Vaccine Posts:
No Vaccine Selfie Yet or “Why I am uncomfortable getting vaccinated”
“𝐀 𝐂𝐎𝐕𝐈𝐃-𝟏𝟗 𝐕𝐚𝐜𝐜𝐢𝐧𝐞 𝐰𝐢𝐭𝐡 𝟗𝟓% 𝐄𝐟𝐟𝐞𝐜𝐭𝐢𝐯𝐞𝐧𝐞𝐬𝐬… 𝐓𝐞𝐥𝐥 𝐌𝐞 𝐀𝐧𝐨𝐭𝐡𝐞𝐫 𝐁𝐞𝐝𝐭𝐢𝐦𝐞 𝐒𝐭𝐨𝐫𝐲.”
Dr. Emily Smith, Friendly Neighbor Epidemiologist Vaccine Series
1. Herd immunity and vaccines: Vaccines 101 – https://tinyurl.com/y27txvro
2. Vaccine distribution info and how well do the current vaccines work? – https://tinyurl.com/y2vte5lz
3. Whoa, these were made quick, right? How can we make sure they are safe? https://tinyurl.com/y2awosyn
4. When will I get the vaccine? Who decides who gets a vaccine first? And, a note on solidarity versus individualistic thinking. – https://tinyurl.com/y39cbptv
5. Myth-busters for vaccines (we talk about fertility questions, 5G/micro-chips, fetal cells, and why the mRNA won’t change your DNA) – https://tinyurl.com/y2woz462
6. Explaining the FDA review and talking about the final Pfizer study results. https://tinyurl.com/y22jd32f
7. Should we be worried about the side-effects seen in the UK? – https://tinyurl.com/yxvb36y4
8. Let’s talk about the FDA panel meeting- https://tinyurl.com/y6hzmcgt
9. Reflections on the EUA Pfizer FDA meeting – https://tinyurl.com/y4k2o6kc
10. Pfizer EUA approval, vaccine ingredients, and recommendations – https://tinyurl.com/yyvzeynx
11. Pfizer vaccine Q&A – https://tinyurl.com/y7e3jar8
12. Will I have to get a shot every two months? Should I worry about mutations? https://tinyurl.com/y83wd84k
13. Info on the Moderna vaccine – https://tinyurl.com/y7x2hvn8
14. Let’s compare the Pfizer and Moderna vaccines – https://tinyurl.com/ybzdnqo5
