A physician friend recently brought to my attention the First Trust COVID-19 Tracker, a weekly 1-page document released by First Trust, a Wheaton Illinois based blog on *checks notes*… Financial Advising? Ok, that’s fine; COVID-19 has affected everyone in profound ways, and if a financial blog wants to use its resources and time to share important information about COVID more power to them.
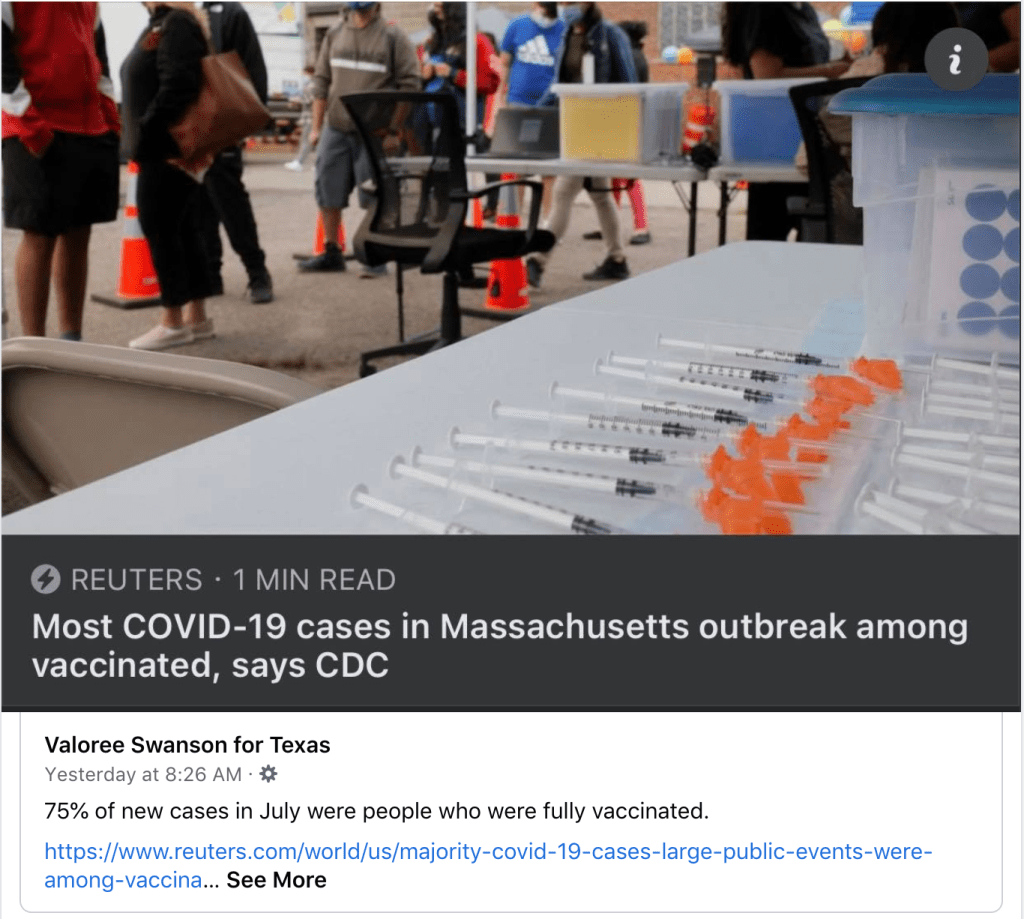
The fact that my friend lives in Texas and is being confronted with this information on a weekly basis does raise concern, however, specifically on the questions of source authority and nitpicking data and sources. Throughout the pandemic we have seen people spread misinformation from non-medical, non-scientific sources far removed from their actual location for the simple reason that they had to look far and wide for data that seemed to support position when the data for their own hometown did not. We saw this on a large scale with the Massachusetts Outbreak in August, which people all over the country pointed towards as proof that the vaccines were ineffective, at the same time that they wouldn’t be able to get an ICU bed in their own city because of the surge of unvaccinated hospitalizations for COVID. There may well be a perfectly legitimate reason that this individual in Waco Texas uses First Trust as their go-to source of COVID-19 information. Many blogs have followers from all over the world (or so I have been told); maybe they have followed the First Trust blog for years and it was already a resource they trusted prior to the pandemic, or maybe they like the attractive layout and graphics. But when someone ignores their local county health department’s COVID-19 dashboard in favor of a weekly COVID tracker from over a thousand miles away (trust me; I drove all 1,000 of those miles a few weeks ago), we do have to stop and ask, “Why? Why look so far away?”
There are some things I definitely likeabout the First Trust COVID-19 Tracker. First, it really is a lovely document; the layout and graphics are eye catching and superb; if I were creating COVID-19 statistics handouts for social media I would want them to look just like this. More substantially, there is nothing overtly partisan about the presentation. We will exam the way that First Trust has selected and chosen to present their data, which is either intentionally or unintentionally misleading at times; but it is data, not conspiracy theories or outrageous lies, and they even include some of the data that weakens their evident position. In that sense it is sort of a breath of fresh air. My overall impression of the First Trust COVID-19 Tracker is ‘bias but honest’, and it’s hard to say how much of the misrepresentation of the information is deliberate vs. accidental; I personally believe it’s mostly the latter.
With the pleasantries now dispensed, let’s take a look at the COVID-19 Tracker segment by segment.
Hostile Behavior over COVID-19 Safety Measures
The inclusion of this data on the hostile behavior experienced by service industry workers over masking and other virus safety measures is the earliest evidence we have of the essentially honest intentions of the writers of the First Trust blog. The fact that hostile and belligerent behavior over masking and other safety measures is so widespread certainly paints a negative picture of those who are opposed to such policies, yet these will by and large be the same people that follow the COVID-19 information put out by the First Trust blog. It meets the criterion of embarrassment and speaks to at least their intention to take a balanced stance.
I realize that there is at least one other possible interpretation, but it’s so cynical- and so transparently flawed- that I wasn’t willing to lead with it. They could be saying, “look at how these masking and social distancing measures have resulted in violence and hostility towards people in the service industry! We need to end these mandates so that people don’t have to experience this hostility any more!“ If you find that argument compelling I’m not really sure what I can tell you. It seems blaringly self-evident that the responsibility for deciding to respond with hostility, intimidation, and violence towards employed individuals simply enforcing the policies of their state, city, or place of business rests solely with the person choosing to respond that way. Placing the blame on the policies themselves and absolving those doing the bullying of any culpability is obtuse in the extreme, and while I am sure some of their readers will take this data that way, I don’t really think it’s what First Trust meant in including this data.
I know people who are against masks and social distancing; I even know and love people who feel persecuted when they are asked to wear a mask (and tell me so, forgetting that I was wearing a surgical mask for hours a day to protect people against pathogens long before the COVID-19 pandemic). Those folks are wrong about masks being dangerous or ineffective, but I don’t for a minute think that they are out there in the world bullying waiters and cashiers over it. But the data shared in the First Trust COVID-19 Tracker shows that somebody is. So if you are one of those folks who are against masks and you happen to be reading this; here’s the take home message from this section of data; get your people. When you see this behavior occurring, don’t cheer it on or be a passive bystander, intervene. As an anti-masker yourself you may have a unique voice to de-escalate a situation where someone who shares your views is acting out towards somebody who is just doing their job.
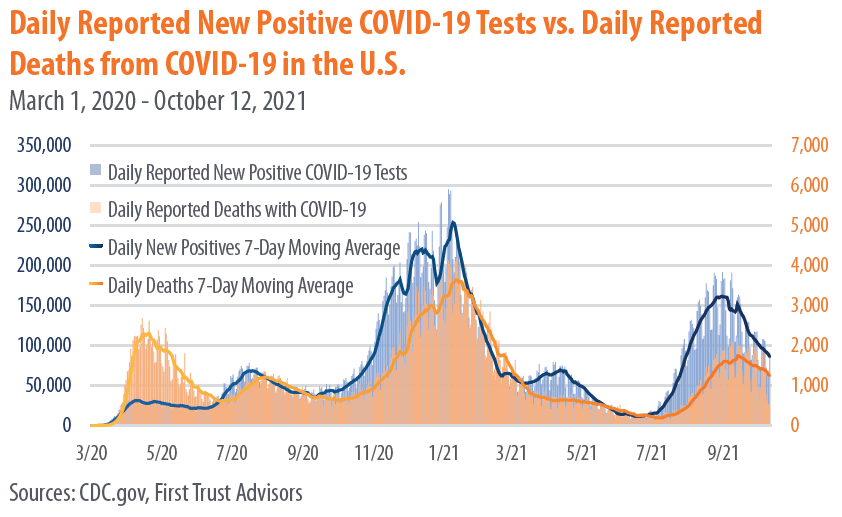
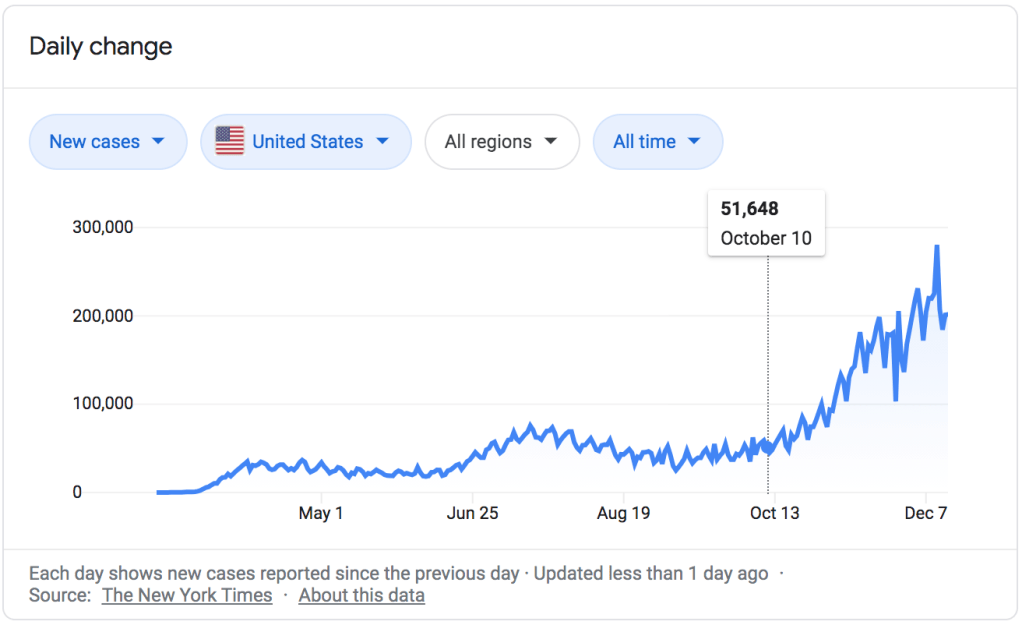
New COVID-19 Cases and Daily Deaths
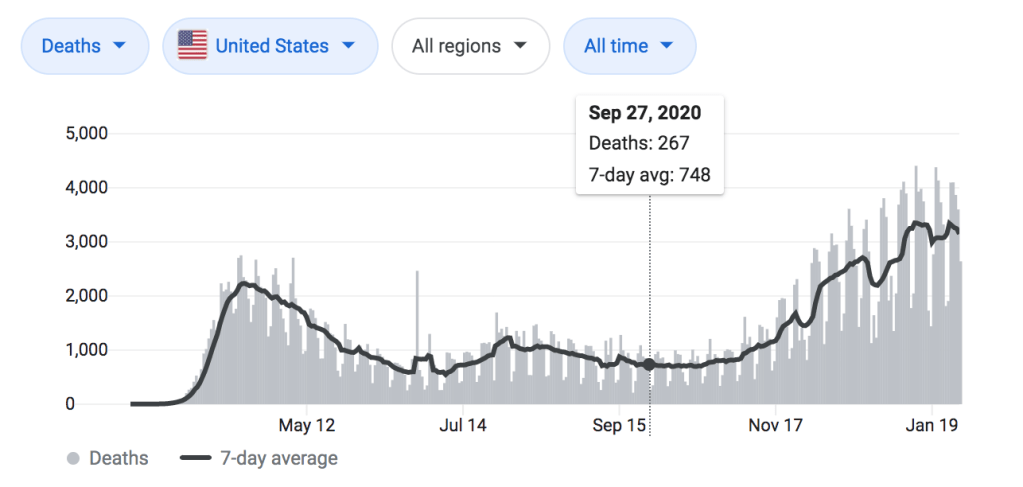
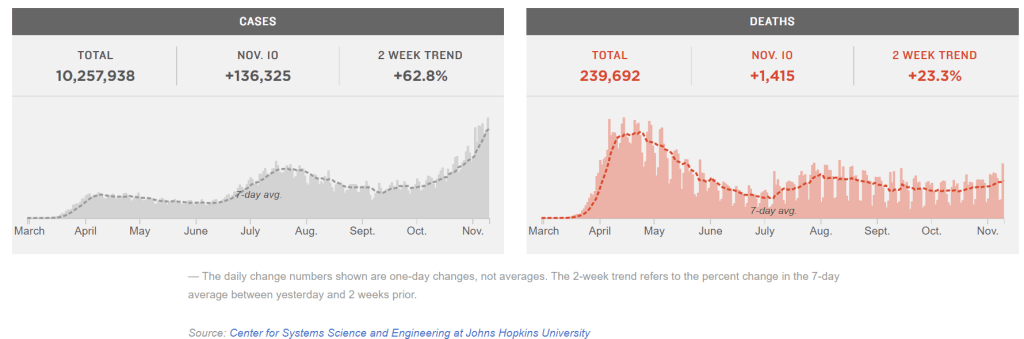
There’s nothing to criticize here, this data was clearly taken directly from the CDC and demonstrates that we are still very much in the middle of a deadly pandemic. Over 2000 Americans died yesterday from COVID-19, and we have now surpassed 728,000 deaths from the virus less than 2 years.
We are so used to seeing this graph, or something similar, that we have become numb to the enormity of this pandemic, and our tendency is to skip right over it and look for other data that either confirms or contradicts our position. But if there are still people out there claiming that the pandemic is exaggerated and that the virus is basically as deadly as the flu (and there are), then it’s worth pausing to look at this data.
Yesterday 2,011 deaths were recorded from COVID-19. The day before that it was 1,890. Each day in the US an average of 1,805 die of heart disease, and about 1,600 from cancer. The way that deaths are reported means that those 2,011 deaths represent people who died sometime in the preceding couple of weeks, and the people who will die tragically from this virus today will be represented in that data up to a few weeks from now; statistics can’t be reported instantaneously. So it’s most accurate to think of these as averages over time, and based on this we can see that more people are still dying from heart disease and cancer each day, on average, than from COVID-19. But it’s really, really close. And the fact that our healthcare system is stressed to the breaking point by the number of primarily unvaccinated people with severe COVID-19 symptoms means that both heart disease and cancer, and every other illness, are more dangerous now because patients are so much less likely to have access to the are that they need.
Again, we need to recognize that including this data is more evidence of the desire for fairness and balance on the part of First Trust. They didn’t have to include this, and many of the memes, blogs, and videos we have seen spreading misinformation over the past year have deliberately used outdated information and statistics from early in the pandemic, before it had spread significantly in most parts of the country, to ‘prove’ that COVID-19 isn’t dangerous. This data shows how dangerous it really is, and those who use the First Trust COVID-19 Tracker to prove otherwise need to take a closer look at their own resources.
Vaccines Administered by Type
Again, nothing controversial here; this matches the data I have. I’ll just add that the now 409,438,987 doses of COVID-19 vaccines given as of today represents 57.5% of the US population, which is encouraging. We should see that number skyrocket soon, once the vaccines are approved for children ages 5-11. My two oldest will be first in line, and my 3rd, who turns 5 this winter, will be right behind them.
Mask Usage vs. Daily Positive Tests
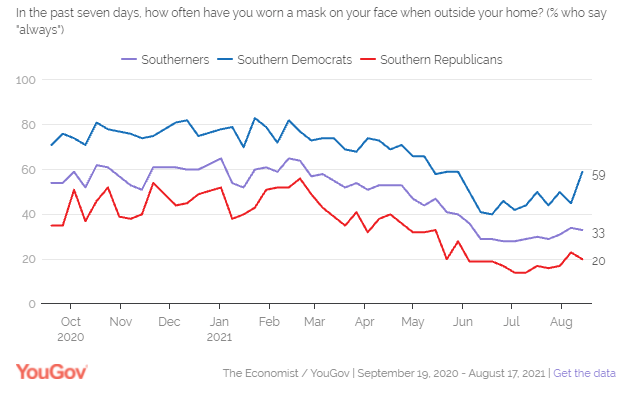
All good things must come to an end, and this is the point where the data presented in the First Trust COVID-19 Tracker begins to drift towards the highly suspect. Take a moment and look at this graph, and ask yourself whether the numbers you are seeing seem right to you.
Statistics are not always intuitive. The fact that meticulously collected and cautiously interpreted data transcends the limited observations we have to draw from in our own realms of experience is the reason they are so powerful. Sometimes our own circles or spheres of influences are outliers, and data from a wider selection of the population upends our expectations. Nevertheless, when a piece of data is so contrary to our experience that it actually seems impossible, we need to at least pause and consider the source, how it was collected, and what it means- good habits to get into with all data, to be perfectly honest.
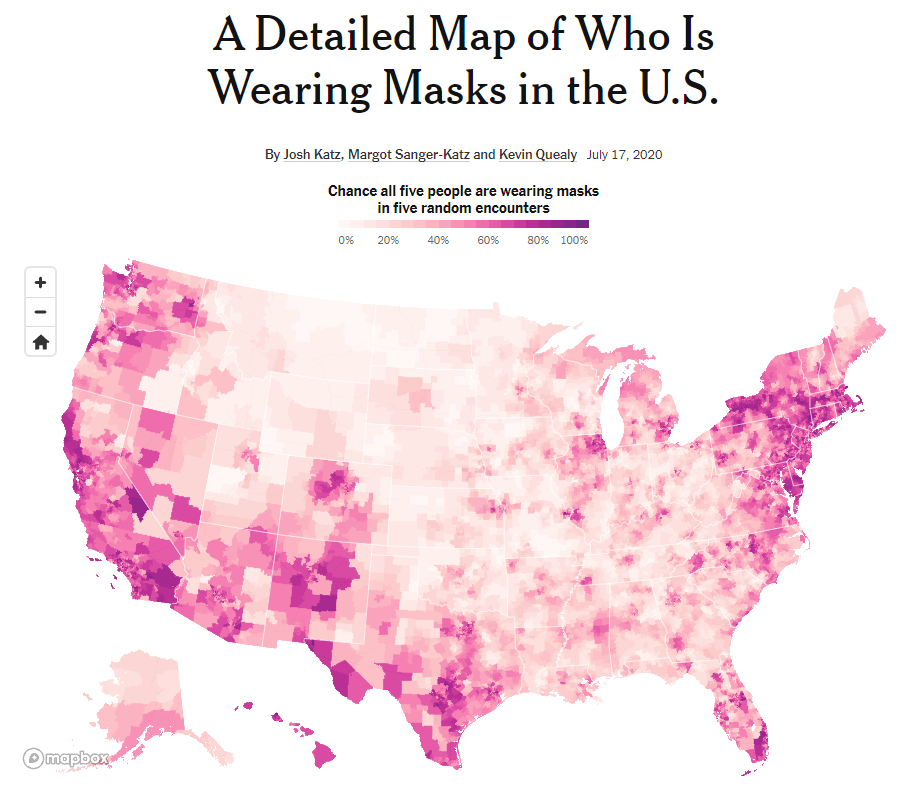
If you live in Texas (as I did until very recently), what might jump out at you from this data is the idea that up until May 70-80% of people were wearing masks indoors consistently when they left their homes.I’m not sure if you’ve been to the grocery store in Texas recently, but that number seems… High. Without a statewide mask mandate, I have frequently been inside of a place of business where I was the only person wearing a mask, and at best the numbers seem split about 50/50. Again, my personal experience might not be normative; we have to look at the data, which in this case comes from YouGov.com online poll data.
You may live in another part of the country (like, say, the suburbs of Chicago) and are saying to yourself, ‘no, that looks about right to me.’ And the reason is pretty simple; the USA is not anywhere close to a homogenous society, and health behaviors around COVID-19 are subject to dramatic regional differences, both due to and apart from varying State and local regulations.
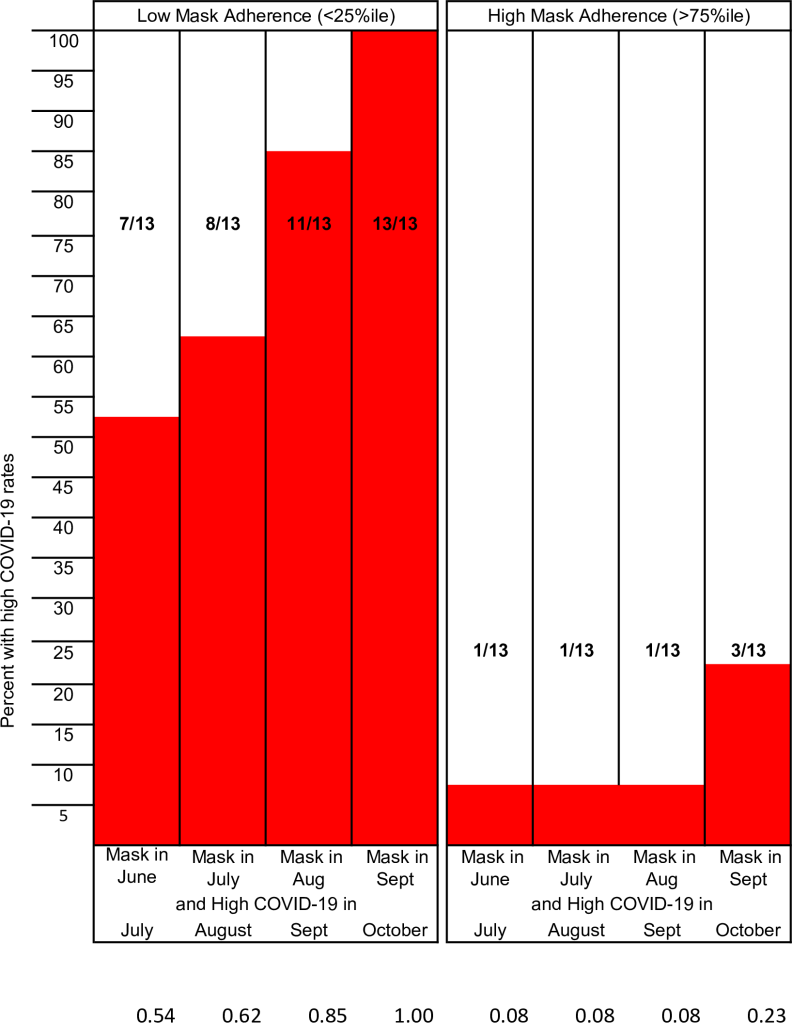
Why does it matter? It would be easy for someone to look at the data from the Mask Usage vs. Daily Positive Tests graph from the First Trust COVID-19 Tracker and come to the conclusion that mask wearing is generally high in the US (close to 80% throughout the Winter) and that it makes very little difference in the ebb and flow of the pandemic. As you look towards the Summer of 2021 this illusion breaks down a bit; there is a definite drop in mask wearing prior to the Delta Variant surge beginning in mid-July. But because this data ignores the regional differences in mask wearing, it is telling a very one-dimensional version of the story; we also need to ask where the cases have been high, and where mask wearing has been prevalent. YouGov.com has some data that helps with this, even though the graph shown in the First Trust COVID-19 Tracker isn’t one of them. For instance, at the end of August, during the peak of the Delta Varint surge, only 33% of Southerners stated they consistently wore a mask. Yes, that feels much more like the Texas I know and love.
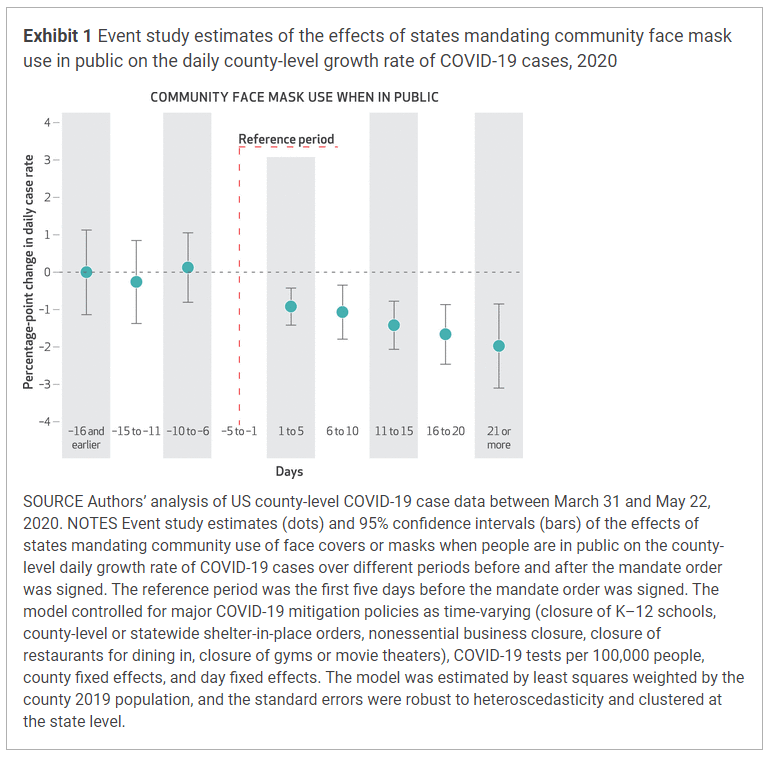
It’s a challenging question to study because demographics and climates vary, and surges are affected by not just state residents but also visitors and tourists and the people living in surrounding states. But there are studies that have done the work of comparing the rate of COVID-19 cases to adherence to masking at the state and local levels. The methodologies have been different, but each has shown what we already knew from comparisons between nations with varying mask policies early in the pandemic; in regions where mask adherence is high, COVID-19 cases are lower. And in regions that adopt mask mandates or similar policies, COVID-19 cases begin to fall.
It’s impossible to fully tease out the effects of different behaviors that commonly occur together. People who are more likely to wear a mask at the grocery store are also more likely to eat outside whenever they can, to stay home from work when they feel ill, and to generally treat the pandemic with more caution in order to protect themselves and those around them. And though human beings are complex and nuanced in their actions and behavior, it’s still fair to say that in general those who do not believe in masking are also less likely to observe other mitigation measures as well. The question of percentage wearing a mask helps vs. what percentage coughing into your elbow or eating outside helps will probably never be answered with a high degree of precision; but they don’t really need to be. The point is that these efforts do prevent infection and death from COVID-19, especially when done together, and especially when used in conjunction with widespread vaccination.
Flu Vaccine Effectiveness
I’ll be honest, I have no idea why this graph is here. It is approaching flu season, so maybe First Trust wants you to see the importance of getting your flu shot? Or maybe they don’t want you to get your flu shot because it is never 100% effective? I don’t really know. If you want to read more about the differences between COVID-19 and Influenza, and why Influenza has been so unpredictable since the pandemic began, I have an article on that here: What Happened to the Flu? (Hint: It’s not because doctors are ‘changing flu cases to COVID’).
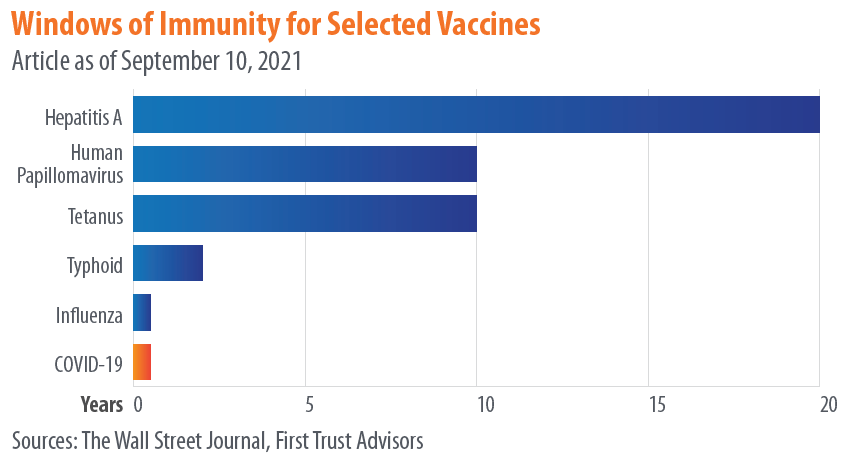
Duration of Immunity from COVID-19 Vaccines
We saw earlier how the comparison between mask wearing and COVID-19 cases juxtaposed data in a way that obscured rather than elucidated the relationship between masking and prevention of COVID. It told a false narrative, sure, but using real and related data, just data that was too generic to actually draw conclusions from. This is the first example of what I would really call misinformation, and it falls under the category of comparing apples to oranges.
While I applaud First Trust for listing their sources, the problem is that their manner of referencing doesn’t actually allow to get back to primary data. They list their source for this data as “The Wall Street Journal,” without listing a specific article. When you find the article on the Wall Street Journal, they just have the same exact chart up but instead list their source as “The CDC,” again without linking to any specific publication, announcement, article, or study. Why not just list “The Internet” for your source and call it a day guys?
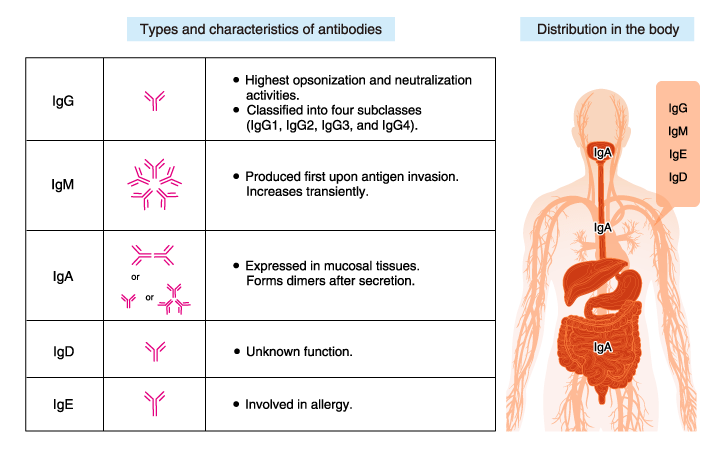
What this graph seems to be showing is not how long you are immune against various infections following vaccination, but how long you have detectable antibodies after vaccination. Calling these “windows of immunity” is highly problematic and misleading (whether it’s being done by the Wall Street Journal or the CDC), because- and I cannot stress this enough- presence or absence of antibodies is not the same thing as immunity.
So much has been written explaining this; here is an article, and another, and another, and another. Antibodies are one of the main, active end-products of your immune response to both infection and to vaccination, but they are proteins, and they do not live forever. Most antibodies will die between 3-6 months after they are created, and then they have to be replaced by newly produced antibodies. If you have been exposed to a virus, either through vaccination or infection, and are then exposed to it later, your ability to mount a robust, effective immune response does not depend on the present of antibodies, but on your ability to make antibodies.
This is determined by a variety of immune cells that your body makes in response to the presence of a pathogen, including plasma cells. An essential strategy that your body uses to fight illness is that it can remember what infections you have already fought off in the past; it doesn’t have to keep circulating antibodies to every disease, but it does keep long-lived cells that can produce a rapid and robust immune response- including the rapid production of massive amounts of antibodies- if you are exposed again in the future. Showing a chart of how long antibodies last has absolutely no bearing on whether or not the vaccines that produced those antibodies will protect you for years to come. Thankfully, the studies that have been done so far give us compelling reasons to believe they will.
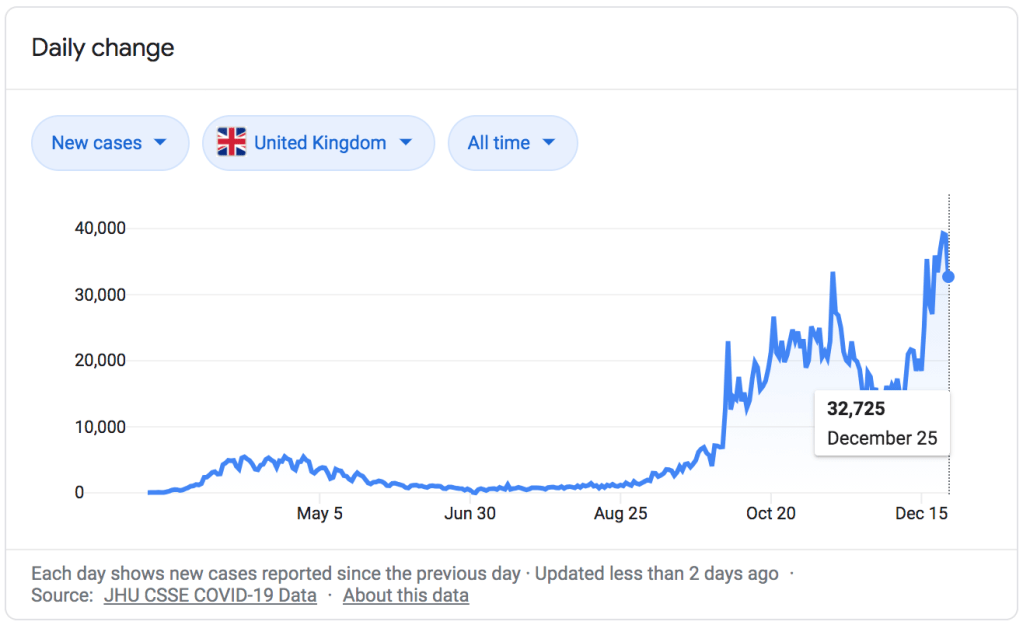
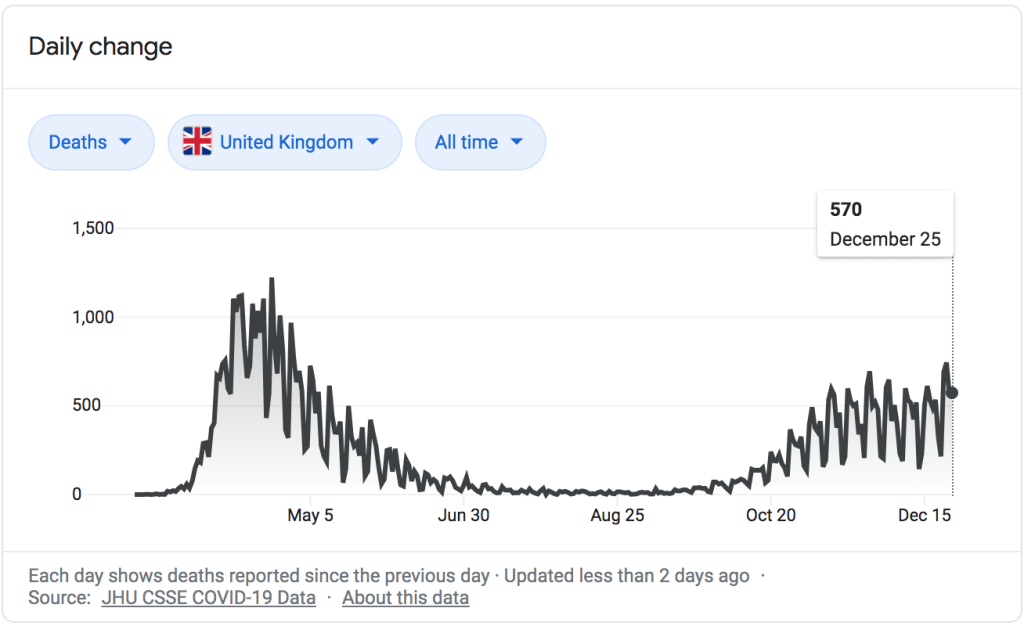
Let’s leave aside for the moment the question, which this chart seems to beg, of why someone in Texas is confronting my friend with a publication from Chicago comparing COVID-19 statistics between The UK and Seattle. There may be a very rational explanation, I just have no idea what it is. Why did they choose these locations? And why is it more compelling to this person than data from their own state?
I think there are two impressions that someone might walk away from this chart with (though I would like to add a third).
First, one might compare these side-by-side graphs where the death rate seems to be about 100 times high in the UK, and determine that for whatever reason our risk of death from COVID-19 in America (or at least Seattle) is far lower than in other countries (or at least the UK). The problem with this is pretty clear, and I’m surprised it wasn’t caught before First Trust published this infographic: the graph from the UK shows total death rate per 100,000 people for a selected time period (the UK is currently experiencing a sustained surge of the virus), while the Seattle graph shows the death rate per 100,000 people per day. And that daily rate is an average of 9 months, including months where cases were very low and months where the Delta Variant was causing a significant surge. If you want to get the total death rate for the Seattle graph for that entire time period, you would need to multiply the daily rate by 261, the number of days from January 27th to September 29th.
This would give you numbers like a death rate of 80.91 out of every 100,000 for unvaccinated people ages 50-64, and 467.19 out of every 100,00 for unvaccinated people aged 65+. This is still comparing apples to oranges with the UK numbers (9 months with and without surge vs. 1 month of sustained surge), but it seems like maybe the point is to just make the numbers look small, regardless of what they actually mean. “Hey,” you might think, “it’s less than 0.5 for people my age! That’s not bad!” Except that 0.5/100,000 risk of dying from COVID-19 is every single day and includes the days where there very few COVID cases. It’s important to know what this data means before you use it to inform your decisions about the pandemic.
The 2nd impression you might walk away with is that the virus is very dangerous for people in their 50’s, 60’s, or older, somewhat dangerous for people in their 30’s and 40’s, and not as dangerous for children, teenagers, and young adults. This is absolutely true; age is a huge risk factor. But one of the effects of choosing a daily death rate is that you can get the numbers on the graph as close to zero as possible, to leave someone with the impression that practically nobody has died from COVID-19 which isn’t the case.
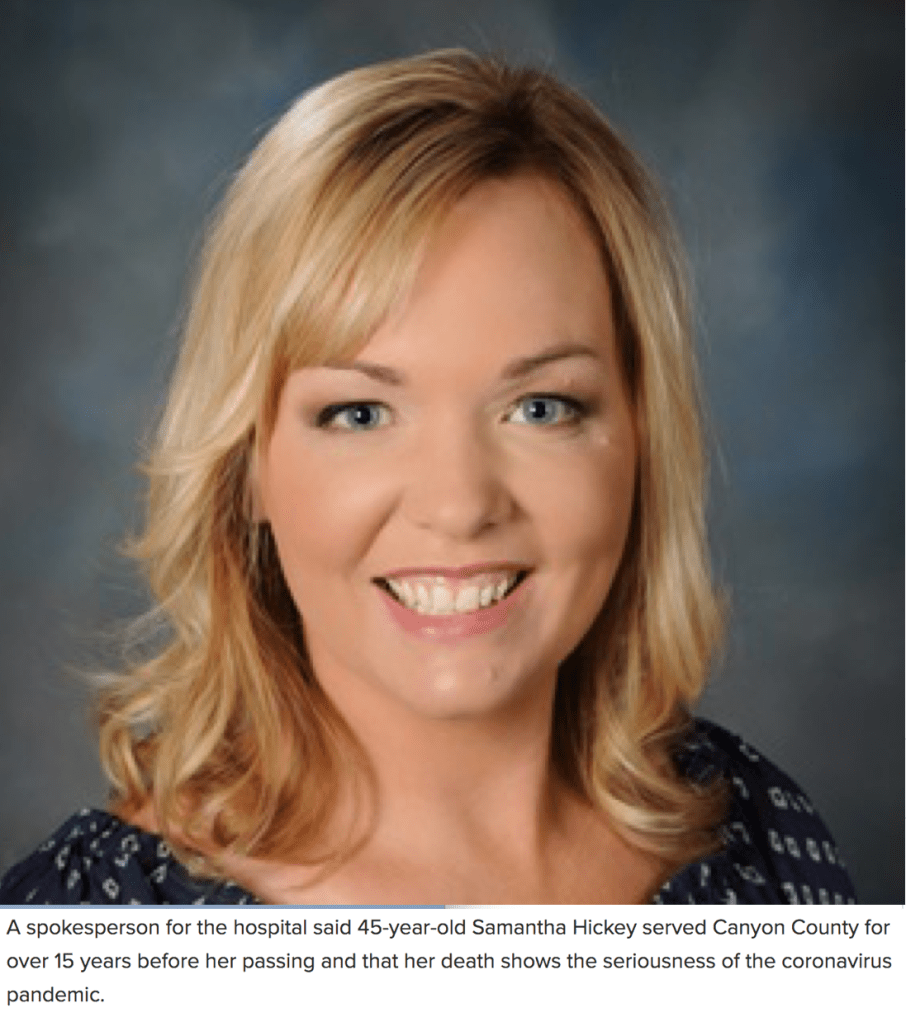
When one child dies we call it a tragedy, and it affects the course of their family’s life forever. As a father of four, I can’t imagine what it would be like to lose one of my children. The COVID-19 pandemic has killed 513 children in the US. When a young person dies we call it a tragedy, and their parents, loved ones, and friends are left devastated. The COVID-19 pandemic has killed 3,888 young people. Those 712,930 people who we have lost to the virus all represented lives cut short; live full of purpose, filled with people who loved them. Yes, a disproportionate number of those who have died were elderly, and a disproportionate number of the younger people died had chronic illnesses or disabilities. If you’re here to make the argument that their lives were somehow less valuable, that they were less deserving of a society’s efforts to protect them from the virus, or that it was somehow less of a tragedy that they died from it, you can exit my blog right now and go read something else.
Finally, the third impression you could take from this data (and again, props to First Trust for not trying to alter this data in any way), is just how effectivethe COVID-19 vaccines really are. Whether you are looking at the Seattle data or the UK data, there is a hug difference in the height of those orange ‘not fully vaccinated’ bars and those blue ‘vaccinated’ bars. I’m still not sure why they chose King County Washington, but here’s some additional data from the same county COVID dashboard that produced these graphs.
If you can take one salient, actionable piece of wisdom from the First Trust COVID-19 Tracker, it would be this: the COVID-19 vaccines work. You should go get vaccinated.
It’s rare for me to be able to muster the time to write two misinformation blog posts in the same month, let alone in two days. Between moving across the country, fighting a global pandemic (still), and the unbelievable amount of take-home work created by practicing Family Medicine five days a week, it’s unfortunately a lower priority than I’d like for it to be. But when friends all over the country send me the same video and a friend in Louisiana, which is utterly overwhelmed by COVID-19 right now, posts it as proof that vaccines are ineffective and dangerous, watching and dissecting the video becomes a higher priority.
For those of you who would prefer a quick 8 minute video in response to this quick 6 minute video, I’ll refer you over to ZDoggMD. We cover some of the same ground and he is much, much more fun to listen to compared to reading however many thousand words I can manage to write this evening.
A few preliminaries. Dr. Dan Stock practices Family Medicine (the same specialty I practice) in Hancock County, Indiana, just east of Indianapolis. Unlike many early medical misinformation sources, he appears to be fully licensed. His website is currently down (no doubt flooded with new patients in the wake of this viral video) so there is no way to know if his practice is evidence based in its approach to science and medicine. His speech here is to the Mt. Vernon school board… Sorry, “Community Education Corporation.” It’s essentially a rapid-fire review of misinformation we have seen shared throughout the pandemic, up to and including the recent misinformation regarding the Massachusetts “Outbreak.”
Many people still see the removal or censorship of any misinformation, no matter how dangerous or how full of lies and half-truths, as proof of it’s absolute validity. I have mixed feelings on taking down these misinformation videos, but since my (self-appointed, unpaid) job is to debunk the videos and my preferred method of doing so is going through them minute-by-minute, I tend to include a direct link to them on my blog posts. It’s the method I personally find most convincing, and that I believe best arms others with the information and insight they need to engage in conversations about viral misinformation like this with their friends and relatives.
The Video: Dr. Dan Stock at the Mt. Vernon Community School Corporation
0:25 “We’re getting our information from the Indiana State Board of Health and the CDC, who don’t read any science.” In my opinion Dr. Stock has severely harmed his credibility here within the first 30 seconds. By stating that the Center for Disease Control, a federal agency comprised of researchers, epidemiologists, laboratory based scientists, virologists, statisticians, experts in every field of biomedical science and physicians of every specialty, and his own state-level department of the same composition “don’t bother to read science,” he is making a statement that is obviously ridiculous. I would submit to you that Dr. Dan Stock does not believe this. He knows that both the CDC and the ISDH read scientific literature, closely follow and analyze epidemiological studies, conduct extensive studies of their own, and in fact maintain rigorous standards of evidence on which they base their recommendations. He knows it, and he could have chosen here to say, as ZDoggMD says about his ambivalence about children wearing masks (an ambivalence I do not share; my kids are definitely wearing masks if we have to take them anywhere right now), that he earnestly disagrees with some of the CDC’s recommendations or conclusions. That is a credible and understandable stance, and many doctors I know have taken issue with some one or another of the CDC recommendations for various reasons. But Dr. Stock chose instead to make a statement he can’t possibly believe because he knew it would be appealing to certain people; the people in the room speaking out against vaccination, for instance, and whether he knew it or not many people across the country who would like to believe that any scientific finding or recommendation they disagree with is simply fake. Saying the CDC “does not bother to read science” is a signal of what team you are on, and nothing more; and it’s an unfortunate harbinger of what is to come in the rest of his speech.
0:39 “Everything being recommend by the CDC and the State Board of Health is actually contrary to all the rules of science.” Again, these blanket statements should begin to make your misinformation Spider-Sense tingle pretty early on. Everything the CDC has recommended throughout the pandemic has contradicted the “rules of science”? Social distancing and staying home when sick don’t decrease transmission? Quarantining when exposed to a deadly and contagious pathogen doesn’t save lives? Dr. Stock would be on a much stronger footing if he said that he opposed specific recommendations- for instance masking and vaccinations- and then told us why he opposes them on scientific grounds. This “CDC is BAD” signaling is sure to get applause and video shares, but it’s hardly a good start for reasonable, precise debate.
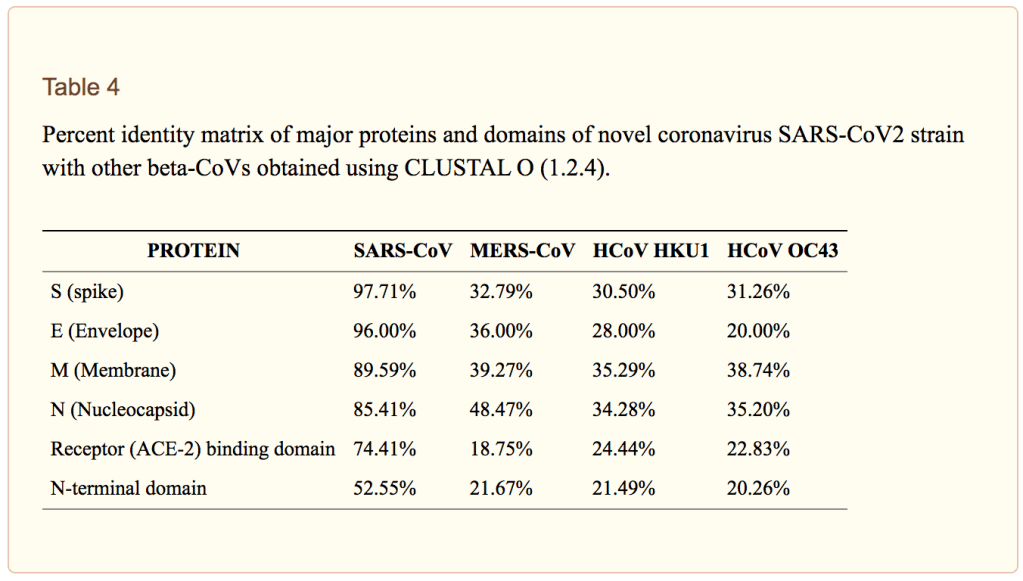
0:43 “Things you should know about Coronavirus and every other respiratory virus…” I would be incredibly suspicious of anyone lumping SARS-CoV-2 in with “all other respiratory viruses”… or lumping ‘all respiratory viruses’ together at all, for that matter. The virus that causes COVID-19 has behaved unpredictably throughout the course of this pandemic in more ways than we could count. It is a strange and unpredictable virus, which is why we had an even harder time treating it effectively in the hospital early on and why our transmission control measures, which have worked astoundingly well for Flu, have only ever managed to take the edge off of it’s transmission.
Dr. Stock would like to lull you into thinking that there is a set of regularities that viruses called “upper respiratory viruses” all follow, and that COVID-19 follows all of these as well. He may be lulled into believing it himself; he says later that he has seen only 15 COVID-19 patients. Last March many of us, myself included, believed that the ‘new coronavirus’ in China and parts of Europe was just media medical sensationalism. “Coronaviruses aren’t that dangerous,” we said (forgetting all about SARS since many of us had never actually seen a case of it), “they cause the common cold; there’s nothing to be worried about.”
Then we started treating it. I still remember the night I sat in bed watching videos from ICU’s in Italy, completely overwhelmed and without the medical equipment, supplies, rooms, or staff to care for all of the patients dying in respiratory distress, and I realized for the first time, “this is real.”
When Dr. Stock tells you throughout this video, “we shouldn’t do x, y, or z for COVID-19 because we’ve never done it for respiratory syncytial virus (RSV),” you need to remember that we have never seen RSV kill 600,000 Americans of all ages in 18 months. It’s the grossest kind of false-equivalence.
0:45 “Coronaviruses are spread by aerosol particles that are small enough to go through every mask.” It’s been 18 months and it’s really hard to believe we are still talking about whether or not masks work, considering the abundance of data from epidemiology, physics, microbiology, and virology. I wrote about this extensively in June of 2020, and the evidence was already robust then. Yes, while masks like N95’s do a reasonably good job of stopping even small aerosolized particles that contain live viruses, surgical masks, simple cloth masks, and other options have a much lower filter efficacy at the 50-140 nanometer range, the size of the Sars-CoV-2 virions. A surgical mask will not stop every viral particle; but the mask that you are wearing will filter out a percentage of them depending on the type of mask; more for an N95, less for a surgical mask, and even less for a bandana or scarf. And the mask the infected person is wearing both block respiratory droplets from normal talking and will greatly decrease the velocity and spread of respiratory droplets, including the smaller aerosolized particles, and ensure that they hang around in the air for a shorter period of time.
I have never heard a scientist or physician claim that if 100% of people wore masks it would completely halt COVID-19 transmission; I’ve certainly never made that claim. But it does help, a lot, and the evidence for it is supported by far more than the three studies referenced by Dr. Stock (to be fair, he mentions these are the 3 that were funded by the CDC; he surely has more). This article on masks and COVID-19 transmission from Sri Lanka from last June cites 139 articles on upper respiratory viral transmission, particle size and dynamics, and prevention; a pretty good benchmark for that sort of paper. Saying “the masks don’t work” at this point in the pandemic is a call-back to the COVID-19 anti-mask skepticism of last Summer.
1:03 “Even though the CDC and the NIH have decided to ignore the very science they paid to have done.” The CDC and the NIH fund literally tens of thousands of research studies each year; many of them are looking at the exact same or very closely related issues, and many times different studies that they fund produce differing conclusions; data that requires analysis, synthesis, and careful parsing. We would be extremely worried if they didn‘t. The fact that the CDC and NIH sponsor many studies and then carefully analyze the results, as well as the results of studies they didn’t pay for, before giving recommendations is a very good thing. If the CDC were to either ‘not read the science’, or cherry-pick the information they believe based on what agrees with their presuppositions- as Dr. Stock is doing with these studies he references- they would not be a reliable source of medical and epidemiological guidance. Thankfully, they don’t do that.
1:15 “The history of all respiratory viruses is that they circulate all year long waiting for the immune system to get sick through the Winter or become deranged as has happened recently with these vaccines.” Dr. Stock practices something called “functional medicine”; basically the idea of addressing the root causes of disease and using the body’s own systems, as much as possible, to fight illness. It isn’t different than the practice of medicine in general, but it is a neat field that certainly has a more intentional focus on underlying causes. Because the emphasis so often lies on the patient’s own immune system fighting any infectious illnesses, the functional medicine doctors I know are very pro-vaccine; vaccination is as much in-line with the concept of letting the immune system do what it was designed to do as any medical practice. Unfortunately, functional medicine also attracts some doctors who are embracing certain anti-medicine or anti-science narratives, either because they have come to believe them themselves or because they see what a lucrative market there is for someone willing to offer all the benefits of modern medicine from an anti-modern medicine perspective and without the restrictions of having to follow the scientific evidence when it’s inconvenient. Good functional medicine doctors don’t do that, and I have heard recently from those practicing functional medicine who feel that doctors like Ben Edwards and now Dan Stock who spread misinformation give their discipline a bad name.
Because Dr. Stock has embraced a perspective that emphasizes the immune system above all else (yet somehow he doesn’t embrace the vaccines that give the immune system the data it needs to fight COVID?), his perspective on the seasonal pattern of respiratory viruses here is extremely incomplete. I thought about skipping this section, but it’s such subtle misinformation that it might get past people and lay the groundwork for more direct misinformation he shares in a few minutes.
Dr. Stock claims that respiratory viruses are worse in the Winter because the immune system is weaker, or because we get seasonal vaccines (like the flu shot or COVID-19 vaccines) that ‘derange’ the immune system. The latter part is nonsense; we’ll talk about it more later but it’s like saying that a construction crew becomes deranged when given a set of blueprints, or a sniper becomes deranged when given a photograph of her target. There is some truth to the first part; the immune system does work better during the Summer for a number of reasons, including sunlight exposure and increased exercise. But of the three major reasons for respiratory illnesses being worse during the Winter (or during the rainy season in temperate climates), it is probably the least influential in the seasonal pattern of these types of viruses.
First, viruses spread more during the Winter because of our behavior. How often have you heard the cultural myth that someone became ill with flu or pneumonia because they went out in the cold or got wet out of doors? It’s the opposite; they got ill with an infectious illness when they came back in to warm-up or dry-off, and were around someone with the virus. We spread respiratory viruses person to person through contact, sneezing, coughing, and touching surfaces while contagious. That transmission happens more easily indoors because of the close proximity and decreased air-flow compared to outside, and we spend most of our time indoors during the Winter. Think of your last Summer event; say spending the day at the lake. Yes, there were many people there, but you could spread out, the wind was blowing, and your conversations tended to happen with some space between you. Now think of your last Winter event- say a Christmas party. The same number of people, but this time inside, talking less than a couple of feet away, sharing the same air. Both events are wonderful (and I missed the latter this past year more than I can tell you), but there is no denying that one is a better opportunity for respiratory viruses to be transmitted than the other.
But the second reason is because of the behavior of the viruses themselves. Viruses are living organisms and like all living organisms they respond to their environment. Viruses like RSV and influenza are more stable in colder temperatures, meaning they can survive longer outside of the body when it is cold; both on surfaces and in the air. They also are more effective as aerosolized droplets when the humidity is low, because the droplets tend to be smaller. There are also effects of sunlight exposure on the viruses themselves, with the UV radiation damaging the genetic information of the viruses (just like it does ours; please wear sunscreen!), inactivating them to a certain degree. If anyone remembers last April, we all hoped that COVID-19 would disappear during the Summer because of these environmental factors. SARS-CoV-2 is an incredibly contagious, previously unknown virus; we hoped that it would display strong seasonal patterns like the flu and we would have a reprieve during the Summer. And maybe we did; but it wasn’t enough of a reprieve to prevent outbreaks, including here in Texas. In a little while Dr. Stock will tell you that the COVID-19 vaccines are the cause for the virus causing outbreaks this Summer. This is a myth, plain and simple. These outbreaks happened last year too, before anyone outside of clinical trials had access to the vaccine. The outbreaks this Summer are simply due to the fact that, unfortunately, COVID-19 does not display as strong seasonality as many of the other respiratory viruses we liken it to, and even more importantly, because the Delta variant is probably the most contagious dangerous respiratory in human history.
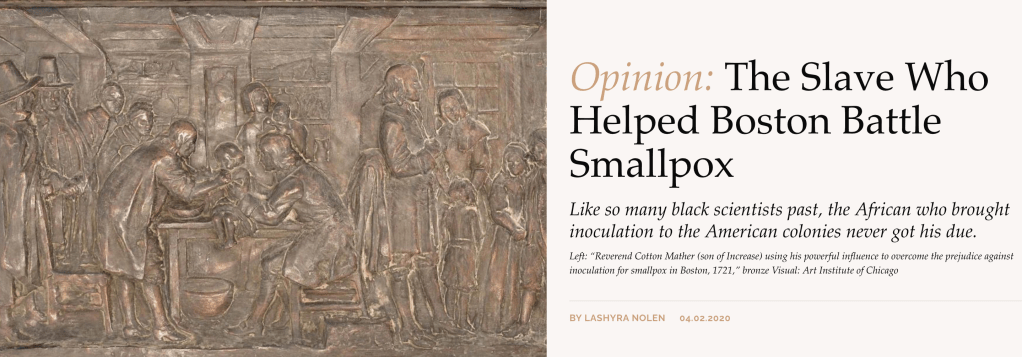
1:25 “The CDC has managed to convince everybody that we can handle this like we did smallpox.” The CDC and public health experts, and those of us fighting COVID-19 every day, have not felt a sense of extreme urgency to promote effective vaccinations against COVID-19 in order to eradicate it, but to prevent people from dying from it. Vaccination was invented by Dr. Edward Jenner, and was taken directly from the practice of inoculation- deliberately exposing the person to a small amount of the disease or a similar disease and hoping they would survive if they were exposed later. The practice of inoculation- or variolation when we are referring specifically to smallpox- was dangerous; since it was a live, active infection, it was possible to become sick with the disease when inoculated, and possibly to die from it. Nevertheless it was effective, and when American doctors were first given the idea to use inoculation to combat smallpox by an enslaved African man in 1721, his knowledge of traditional African healing practices saved hundreds of people during a smallpox epidemic in Boston.
Vaccination was different; it exposed the person to enough of the virus to trigger an immune response without the risk of the person contracting the virus. Traditionally this has been done by weakening or killing the virus, or by giving very closely related viruses that cannot cause disease (cowpox, in the case of smallpox vaccination). We now have the technology to teach cells to build specific, non-dangerous viral proteins so the immune system can learn to recognize them and build antibodies against them without exposing the body to any virus at all. This is a natural progression of the principal of inoculation that humans have used for thousands of years; live virus to weakened virus, weakened virus to dead virus, and now dead virus to no virus at all. The mRNA vaccine technology feels unknown or unnatural to many people, because it came about in their lifetime (I was 6 years old the first time scientists successfully used mRNA technology to teach cells to express viral proteins); but it is really the logical next step along the path set for us by traditional African, Indian, and Asian healing practices; the path of using the body’s own immune system to fight disease.
Dr. Edward Jenner’s personal goal, oft stated, was to eradicated Smallpox. But that was not the only or even the primary goal. The goal of inoculation, variolation, and vaccination has always been to prime a person’s immune system to fight an illness so that they have a less severe course of illness and a lower risk of dying from it. That was the goal of variolation in Western African and later in Boston, it is the goal of the childhood vaccinations we give against measles, whooping cough, and tetanus, it is the goal of the annual flu shot, which has saved millions of lives, and it is the goal of the COVID-19 vaccines; a goal they have seen incredible success at achieving, for those who have received them. We may not be able to eradicate COVID-19; but we can very effectively protect people from it.
2:04: “I would hope this board would start asking itself, before it considers taking the advice of the CDC, the NIH, and the State board of health, why we are doing things about this that we don’t do for the common cold, influenza, or respiratory syncytial virus?”
Seriously Dr. Stock? That’syour question?
2:16 “Why is a vaccine that is supposedly so effective having a breakout in the middle of the Summer when viral respiratory syndromes don’t do that? It’s a little tricky to understand what he is talking about right here. First of all, the vaccine isn’t having an outbreak. That would actually be awesome, if just suddenly there was this uncontrollable surge of people getting vaccinated. What he means is, ‘the virus is having an outbreak because of the vaccines.’ He is subtly shifting responsibility for the outbreaks away from the virus itself, the incredibly contagious delta variant, the general lack of caution and transmission control measures being exercised, abysmally low vaccination rates, and widespread conspiracy theories and disinformation, and onto the vaccines, which is a tactic from the “it’s so crazy it just might work” school of misinformation. He is asking you to shorten your memory and ignore the fact that we already knew pre-vaccine that this is how COVID-19 behaves, since this is what it did last Summer. He wants you to think something like this; “COVID-19 is really bad this Summer. Dr. Stock says that shouldn’t happen during the Summer. A lot of people I know have been getting those vaccines… I bet that’s why.” It’s a logically bankrupt argument with no foundation in reality… But it just might convince some people.
In a moment Dr. Stock is going to offer a seemingly plausible explanation for his false narrative in the form of “antibody-mediated viral enhancement.” Dr. Simone Gold shared this same misinformation a few months ago, so below I will copy my discussion of the phenomenon from that time.But the best cure I have for Dr. Stock planting this sort of deliberate misunderstanding is just data. The vaccines are working well, and anywhere that you see high vaccination rates you see fewer and less severe cases, not higher numbers and more severe cases. All of the evidence says the vaccines are working against COVID-19. If we had higher vaccination rates in Texas and Louisiana, we would have smaller and less severe outbreaks this Summer, plain and simple.
2:28 “You need to know the condition called “antibody-mediated viral enhancement. That is a condition done when vaccines work wrong…” There’s a lot of misinformation here. For instance, he implies that COVID-19 has low pathogenicity- a low rate of causing illness- which is totally disconnected from reality. He also implies that the current COVID-19 vaccines caused antibody mediated enhancement in previous studies, which they absolutely did not. In fact, even though Dr. Stock presents this as though he were blowing the lid off of this hitherto-unheard-of fatal flaw in COVID-19 vaccines, avoiding the risk of this phenomenon was foremost in researchers minds when designing these vaccines; he would have you believe that the scientists designing the vaccines had never heard of it before, simply because you might not have heard about it before.
Immune enhancement is a very real concerned, and one that has been hotly debated within research circles since the beginning of the pandemic, especially in regards to severe COVID-19 cases and the potential role of vaccines. Here’s an article from way back in May 2020 (what is that, like 8 years ago now?) about this exact issue. The specific proteins chosen for the mRNA vaccines were chosen carefully and specifically to avoid this problem, and moreover, this is exactly why we do animal studies and clinical trials.
The Moderna and Pfizer trials were simply huge, with ten times the number of people participating than is typical in a vaccine trial; and no evidence of Antibody-Dependent Enhancement was found. The Nerdy Girls over at Dear Pandemic have a short but great social media update on it from just a few months ago:
Moreover, we have now given 352 million COVID-19 vaccine doses in the US alone and over 4 billion doses worldwide, and there is still no evidence that the COVID-19 vaccines cause antibody-dependent or antibody-mediated enhancement. The entire course of the pandemic shows exactly the opposite; those who have the vaccine get less sick, less often, and have drastically lower rates of severe illness, hospital and ICU admission, or death from COVID-19.
3:10 “75% of people who had COVID-19 positive symptomatic cases in the Barnstable Massachusetts outbreak were fully vaccinated.” And 4 of them were hospitalized, and none of them died. I wrote about this just yesterday so I won’t rehash it; it’s a very short post and the link is just below. The long and short of it is, the Barnstable “outbreak” is proof of how well the vaccines work, not of the contrary. What we saw in Barnstable is the opposite of antibody-dependent enhancement; it’s a clear demonstration of the effective protection against severe illness and death for those with the vaccine, and an example of what might have been if we had such high vaccination rates in Texas, Louisiana, and Florida before the Delta variant hit.
3:23 “Therefore there is no reason for treating any person fully vaccinated any differently than any person unvaccinated.” In a sense, he’s correct; morally we absolutely should be aiming to treat all people the same regardless of their personal health choices. I am reminded of the quote by C.S. Lewis:
“There are no ordinary people. You have never talked to a mere mortal. Nations, cultures, arts, civilizations – these are mortal, and their life is to ours as the life of a gnat. But it is immortals whom we joke with, work with, marry, snub and exploit – immortal horrors or everlasting splendors.”
― C.S. Lewis, The Weight of Glory
Your unvaccinated neighbor, your vaccinated friend… They are equal in dignity and honor; they are equal bearers of the Imago Dei. Yet our very respect for that Image of God in each person does require us to weigh many factors in the balance as we consider our approach to this complex pandemic. I believe that profound respect for the dignity of all people requires us to “treat” vaccinated and unvaccinated people differently in two ways.
First, we need to recognize that, regardless of Dr. Stock’s subsequent comments, the COVID-19 vaccines do prevent transmission of the virus. The jury is still out on how well they do this; most of our data just establishes how good they are at preventing symptomatic infection and especially severe infection and death, and there are studies happening right now to see to what degree vaccinated folks can still pass the virus along when symptomatic and when exposed but asymptomatic. The Barnstable MA outbreak is warning enough for all of us who are vaccinated to continue to take precautions like wearing masks and staying home and getting tested when we are ill, if anyone had any doubts. But it was also a contained, small outbreak and we don’t actually know how much of it was transmitted by vaccinated residents of Barnstable county vs. out-of-state visitors; and there’s no way to go back and find out. Nationwide we are seeing Delta surging, and surging most in the states with the lowest vaccination rates. All of the physiology of how our immune systems fight viruses when primed with vaccines suggests that vaccinated people will transmit the virus at a lower rate, and for a shorter duration, than those who are unvaccinated. Vaccines don’t teach your immune system how to ignore the virus, while it multiplies and gets passed along to others; it teaches your body how to kill it. And this, married to the epidemiology evidence of how the surge is progressing in highly vaccinated vs. poorly vaccinated areas constitutes strong evidence that the vaccines do confer protection not only against getting sick from the virus, but against passing it along to others as well.
This is not how your antibodies and the COVID-19 virus interact.
Does this mean that I treat my unvaccinated friends and family like second-class-citizens, barring them from my home and preventing them from ever spending time with my children? While I understand and sympathize with those who feel forced to do so, my answer is a definite “no.” But it does mean that the complex balance of goods and risks that determine in what way I and my family interact with others- which always existed even prior to COVID- has one more important factor. My children are unvaccinated (though I am trying to enroll them in clinical trials so they can get a COVID-19 vaccine as soon as possible), and there is already anecdotal evidence that the Delta variant effects children more than the original strain. I have a basic moral responsibility to protect my children, and the reality is that factors like community transmission rates and the personal health choices of others do have to be factored into our decisions. For us it’s not a question of, “who do we cut out of our lives because they won’t get vaccinated?”, but a question of, “how can we best build and maintain relationships while limiting risk?” That answer is going to vary to some degree with the current prevalence of COVID-19, with the level of caution those in our lives are themselves following, and with their vaccination status.
But I think the second way we treat unvaccinated people differently is arguably much more important. The reality is that, whether they believe it or not, they are more vulnerableto the virus. As a physician, the rapidly branching mental decision tree I follow when helping a patient decide what level of caution to exercise, what treatments to pursue, what symptoms to watch out for, how aggressive to be in seeking further care, and how closely to follow-up is determined by many factors. For COVID-19 care, vaccination status is a big one. My vaccinated patient’s chances of dying from COVID-19 are far, far lower than my unvaccinated patient’s chances, all other things being equal. As a society, our decisions about protecting people from the virus need to be centered on those who can’t be vaccinated, like children or those with true vaccine allergies, on those like the immunocompromised for whom the vaccines might not be as effective, and on those who decide not to be vaccinated. They are still at risk, and nowhere in my medical training can I recall an ethical precedent that says we don’t take excellent care of people if their personal health choices led to their illness (though I do realize that, far too often in modern medicine, we treat patients poorly if they are perceived as contributing to their own health problems or ‘not caring enough’. It’s a huge problem, and trying to address it is one of the reasons I’ve taken a new job teaching at a medical school).
In general I don’t agree with measures that say, “if you are vaccinated you can do this, if not you have to do this.” I understand that from an epidemiology standpoint some of these distinctions are logistically impossible to get around; but the tenets of my faith call for humility and self-sacrifice on behalf of others. If their decision to not get vaccinated means that I have to endure some ongoing inconveniences- like wearing a mask while buying groceries or sitting outside and socially distanced at my favorite coffee shop in the middle of August, when it would be more pleasant inside- I’m here for it. If I knew for a fact that everyone at that store or everyone inside the coffee shop were vaccinated, I might loosen those measures, as I do in small gatherings where I do know that everyone is vaccinated (just ask my Dungeons and Dragons group; we had this exact conversation last week!). I wouldn’t advocate for stricter transmission control measures imposed only on the unvaccinated, but I would advocate for us all following those strict measures, and then dropping some of them that are no longer needed when we know the unvaccinated aren’t going to be potentially hurt by doing so. If that still means I’m “treating them differently,” I guess guilty as charged; I’m treating them like their lives are in danger, because they are, and well, that’s something I really do care about.
3:27 “No vaccine ever stops infection.” By “infection” Dr. Stock does not mean the virus multiplying significantly in your body for any specific period of time, or the onset of any specific symptoms; only the state of having the virus enter your body and begin to reproduce itself. This is what I’ve been trying to help patients understand for the past 9 months as we have talked about the COVID-19 vaccines: vaccines don’t place a forcefield around you that prevents the virus from entering your system; they prime your immune system to defeat it.
But saying that infection still occurs whenever you are exposed to the virus is not the same as saying that transmission occurs, or occurs at anywhere near the same rate, if you are vaccinated. We’ve just talked about how the evidence on this is still evolving for COVID-19, but that it’s very clear that those areas with higher vaccination rates have lower transmission rates. Yes, some people who are vaccinated still get COVID-19, but tend to have shorter illness, lower viral loads, and less severe symptoms. It’s unclear exactly how well they spread the virus, just as it’s still unclear whether the vaccinated are sometimes asymptomatic carriers. But we do know that both of those types of transmissions occur, and occur at extremely high rates, in the unvaccinated who become infected with COVID-19. The current surge of the Delta variant is being driven by transmission from and to unvaccinated individuals.
I won’t keep rehashing the same points, but I will add this; Dr. Stock iswrong about vaccination ‘never stopping infection’ (the virus getting into your system in the first place); it stops infection for the next person, by decreasing the chances that you’ll get sick and pass it along. Please catch the contradiction he has created for himself; Dr. Stock is painting a picture of viral infections moving from person to person uninhibited by their immune systems, with those who get the vaccine (or at least, the vaccines he agrees with) not getting sick but still invisibly passing it around as much as anybody as it lives rent-free in our systems forever.
But a couple of minutes ago he admitted that vaccines eradicated smallpox.
I’ve never been vaccinated against smallpox. Hardly anyone in the US has since 1972. So where is it? High vaccination rates literally stopped it from infecting anyone. If it only suppressed disease and not infection and transmission, we should have seen a smallpox resurgence decades ago, once we stopped vaccinated for it; thankfully, there is still no evidence of smallpox transmission anywhere in the world. No, I don’t think we’ll eradicate COVID-19 the same way, even with high vaccination rates; it’s a very different sort of virus, and the best we can probably hope for is to remove its teeth. But since he brought up smallpox in the first place, I think it’s fair to point out how the history of smallpox vaccination and eradication blows his picture of how vaccines work right out of the water.
3:38 Mumps Outbreak in the National Hockey League. In 2014 there was an outbreak of mumps in the NHL that affected 24 players. The mumps vaccine is not 100% effective, but it is very, very effective as Dr. Stock admits. Prior to the mumps vaccine, almost all children got mumps at some point during childhood. After vaccination against mumps became common, the rate of mumps infection dropped by 99 percent. Yes, it is still possible to get or spread a virus if you are vaccinated, no one has ever said otherwise; but it is far less likely. Why is Dr. Dan Stock currently citing contract tracing for a so-called outbreak that affected 24 people, when just 50 years ago most people got mumps during childhood? Because vaccination against mumps is so effective.
How effective? Well, two doses of the mumps vaccine is about 88% effective at preventing this previously ubiquitous illness. 88% is also how effective the mRNA vaccines seem to be against the Delta variant of COVID-19. Ask yourself, when was the last time you worried about mumps? Wouldn’t it be great to get to that point with COVID-19 too?
4:12 “You get infected, you shed pathogen; you just don’t get symptomatic from it.” We’ve talked this false idea that vaccinated people spread the virus just as well as unvaccinated people to death in the last few paragraphs, so I’ll just add this; when “getting symptomatic” from COVID-19 has resulted in 617,000 deaths in the US in just 18 months, doesn’t “not getting symptomatic” sound like a really, really good thing?
4:14 “You cannot stop spread, you cannot make these numbers that you’ve planned on get better by doing any of the things you’re doing, because that is the nature of viral respiratory pathogens.” All of the epidemiological evidence, from all over the country, says he’s wrong. The vaccines are slowing the spread and making the numbers better. He’s also wrong that the nature of viral respiratory pathogens means that you can’t slow them with basic transmission control efforts like wearing masks and strict sick policies in schools; those very efforts helped us kick influenza’s butt last year. COVID-19 is trickier to beat since it is so much more contagious and has so much asymptomatic transmission, but there’s no doubt that when these measures are followed, they do help. There’s ample evidence of that all over the world, both pre- and post-vaccine.
I’ve said it before and I’ll say it again; there is something deeply disingenuous about people who refuse to wear masks or follow transmission control measures, and have refused to do so since the beginning of the pandemic, pointing to increasing case counts and saying, “see! these masks (I won’t wear) and transmission control measures (I won’t follow) don’t work!”
4:26 “You will be chasing this the rest of your life until you recognize that the Center for Disease Control and the Indiana State Board of Health are giving you very bad scientific guidance.” And what does Dr. Stock place in opposition to this scientific guidance? Other expert organizations with teams of researchers and epidemiologists devoted to finding the very best ways to slow the pandemic and combat COVID-19? A specific, innovative plan of attack that none of the experts have thought of yet (hey, it could definitely happen!)? No; his e-mail, and the other people in the room who have presumably come to the board meeting to protest mask mandates or vaccines or whatever specific measure was originally on the table for discussion that night.
4:47 “That’s why you’re still fighting this with this vaccine that was supposedly going to make all of this go away...“ “The vaccine I won’t get and am telling all of my patients not to get. Why hasn’t it worked yet?”
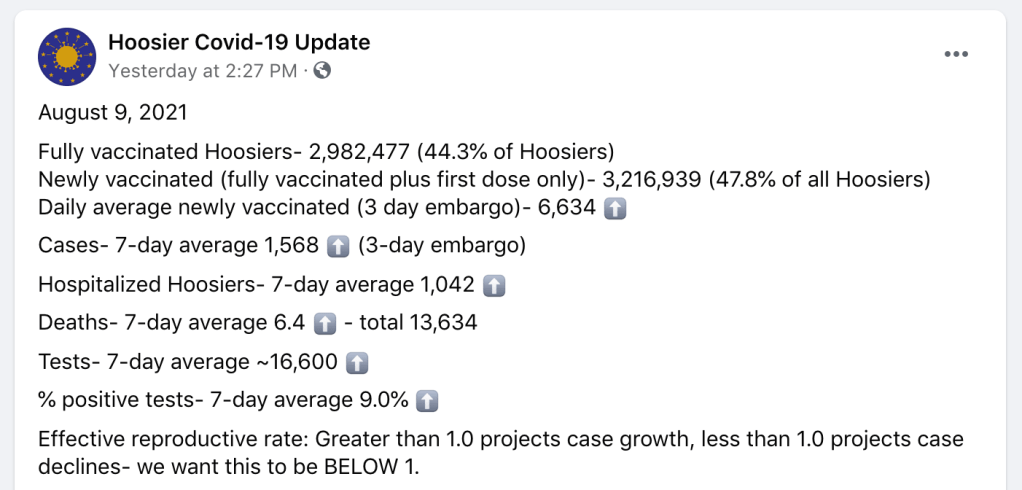
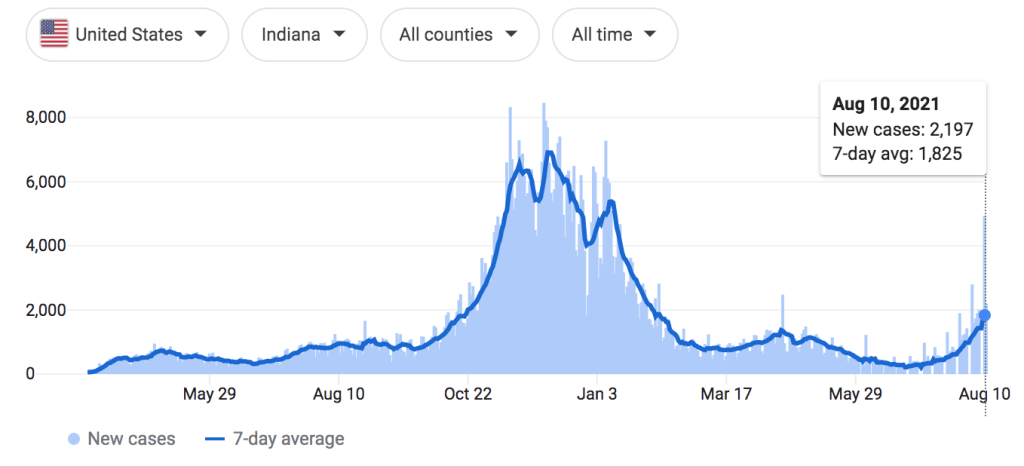
Indiana has only a 44.3% vaccination rate. They are in the middle of a COVID-19 outbreak; not as bad Texas or Louisiana, but still on the rise.
Again Dr. Stock blames the vaccines, instead of the virus and our low vaccination rates, for the outbreak, reinforcing his false narrative that vaccines have caused the outbreak through antibody mediated viral enhancement instead of reduced or prevented outbreaks wherever vaccination rates are high. If his “outbreak in the middle of the Summer” reference is to his own state of Indiana, I would paraphrase G.K. Chesterton; ‘the vaccines have not been tried and found wanting; they have been found shrouded in disinformation, and left untried.’
On the other hand, if he is again referencing the contained “outbreak” in Barnstable Massachusetts, one would ask why he feels compelled to rely on epidemiology data about the pandemic from a county a thousand miles away, when the evidence from his home state shows how effective the vaccines are? I submit that it is because theoutbreak in Massachusetts is the data that best seems to support his claims (again, we’ve seen already that it doesn’t), and he would go to the ends of the earth to find it. When you are committed to misinformation, the experiences of people affected by the virus all around you simply aren’t important unless they fit into your narrative.
5:05 “I can tell you having treated over fifteen COVID-19 patients…” Listen, I know no misinformation video would be complete without touting the latest en-vogue, unproven therapies. But 15 patients? Fifteen?!
I’ve treated hundreds. Nobody wishes that we had a safe and effective prophylactic or early symptomatic treatment regimen more than I do. I spend so much time kneeling on pavement next to cars in the Texas heat, counseling my patients on what to look out for with COVID, helping them establish a posture of vigilance and discernment but without fear or anxiety, helping them navigate the different options for considering monoclonal antibody therapy, and helping them make decisions about work, school, and how to prevent transmission to loved ones. This narrative that we are refusing to give effective treatment to our patients is deeply frustrating and not at all based in truth; I have never withheld a medicine I believed my patient needed, not once in my life; and I spent a lot of my time trying to help them figure out how to get those medicines regardless of expense or other barriers. We are giving them the best that we have to offer; we have been since the beginning of the pandemic and long before.
This “clinical experience” that these doctors like Simone Gold or Ivette Lozano who have treated a small handful of COVID-19 patients (or in their own words, people who thoughttheymight have COVID-19; many times these doctors don’t even bother to test because they don’t believe the tests work) share about how they’ve found a universally effective treatment against COVID aren’t even anecdotal evidence; they are just sampling bias. They see a couple of patients, some of them have COVID and some of them don’t. They put them all on a cocktail of drugs, none of which have been shown to be effective in clinical trials. Those patients recover, as most patients with COVID-19 do without these unproven treatments; but then these doctors tell themselves “without my treatment, that patient would have died.” Except there is no evidence they would have; for some of these docs, there isn’t any evidence those patients who “would have died without my treatment” even had COVID-19 to begin with. They were doing this same nonsense last March and April in areas that hadn’t even seen their first surge of COVID-19 yet, drawing customers (they aren’t your patients when you are just selling them something) from all over the state and saying things like, “yeah, you probably have it, take all of these medicines”, then adding that person’s “survival” to their “evidence.”
I don’t know if this is what Dr. Stock is doing or not. Maybe his patients all had laboratory confirmed COVID-19, or a convincing combination of symptoms and exposure history. Maybe they had really significant risk factors for severe illness, and their recovery turned him from a skeptic to a believer; I don’t know. He certainly seems sincere in his beliefs. but the fact of the matter is, 15 patients with COVID-19 is not enough to base your case on. That’s one of the principals of evidence-based medicine, having the humility to give our own personal experiences only the weight they are due, and respecting our colleagues, our patients, and people from around the country and world enough to recognize when our experiences are atypical or, as in this case, just way, way too small to actually draw conclusions from. I’ve had many days in clinic when I took care of more than 15 patients with COVID-19. Sometimes I’ve been surprised by how sick a young, previously healthy person got with the virus, and sometimes I’ve been surprised by how light a course of illness someone with many risk factors experienced. I can’t draw conclusions from those experiences any more than Dr. Stock can; even my vastly more extensive experience with COVID-19 pales in comparison to our collective experiences as a medical field, compiled as evidence and then analyzed carefully.
And look, I get it. If I were seeing less than 1 patient a month for COVID-19, I might be tempted to abandon evidence and just throw whatever the current theoretical treatment was at them too. These medicines like hydroxychloroquine, zinc, Azithromycin (remember when that was a thing?), and Ivermectin are generally safe, and I’ve prescribed them all for different illnesses in the past. If I gave out one prescription a month because I though there was a chance they would help, I wouldn’t be doing something morally wrong. But it’s not evidence based medicine, and it only feels excusable to practice on gut instinct or social media hearsay like that when you are talking about incredibly small numbers of patients. But because there is no evidence that they do work against COVID-19, prescribing them routinely, prescribing them for thousands of patients with COVID-19, COVID-19 exposure, or COVID-19 like symptoms like I would have to do as someone who fights this virus every single day, would be no different than throwing antibiotics at viral infections because it’s quicker than explaining the difference being a viral and a bacterial infection, doing unnecessary surgeries because it “might help the pain,” or adding more and more medications because you are too busy or too lazy to help your patient find a diagnosis and understand their illness. It isn’t the practice of medicine.
If I’m going to prescribe a medication to a thousand patients, I have to have evidence that it works. And if I’m going to hold a certain high standard of care for a thousand patients, my one patient deserves that same standard of care; they don’t deserve to be the guinea pig for the ‘Ivermectin study I’m doing in my head.’ Right now there is no evidence Ivermectin prevents severe COVID-19. I hope that changes. It didn’t change for azithromycin or hydroxychloroquine, but I hope it does for ivermectin so I can start prescribing just tons of it. And if it doesn’t, I hope the next hot-button medicine really does work, so that I’ll finally have the silver bullet many patients are looking for when I give them the anxiety provoking news that they have COVID-19, instead of ‘just’ careful counseling, reassurance, guidance, and symptomatic treatment.
You know what is safe and does work extremely well at preventing severe COVID-19? Vaccination. As a functional medicine doctor, Dr. Stock’s entire ethos should revolve around identifying root causes, relying on our own body to produce a state of health (a privilege not everyone has), and prevention rather than treatment whenever possible. In stating that we should abandon training our immune systems to fight COVID-19 with the vaccines for all of the erroneous reasons he has offered because unproven treatment is available, he has abandoned functional medicine altogether.
5:45 “People who have recovered from COVID-19 infection get no benefit from vaccination.” Dr. Stock’s very last point is that people who have already had COVID-19 get no benefit from vaccination. This is a question I am asked frequently, and the epidemiology data about who is getting COVID-19 and who is not, and who is getting the most sick from it, does show that those who have already recovered from COVID benefit from the vaccine. The truth is that, if you have already had COVID-19 (just as I did back in December) and then are subsequently vaccinated (just as I was, also back in December, about 2 weeks later), you probably have the best immunity out of just about anybody. Seriously, I wouldn’t encourage anyone to go out and get COVID, but if you’ve already had it and decide to vaccinate, you are getting protection against COVID-19 that money can’t buy. Studies of antibody titers have shown that the immune response elicited by vaccination is equal or greater than that from natural immunity from previous infection. These vaccines are very, very good at what they do, and they work incredibly similarly to how our body’s learn how to defeat viruses from natural infection, only without the risk of illness since the vaccines contain no actual SARS-CoV-2 virus.
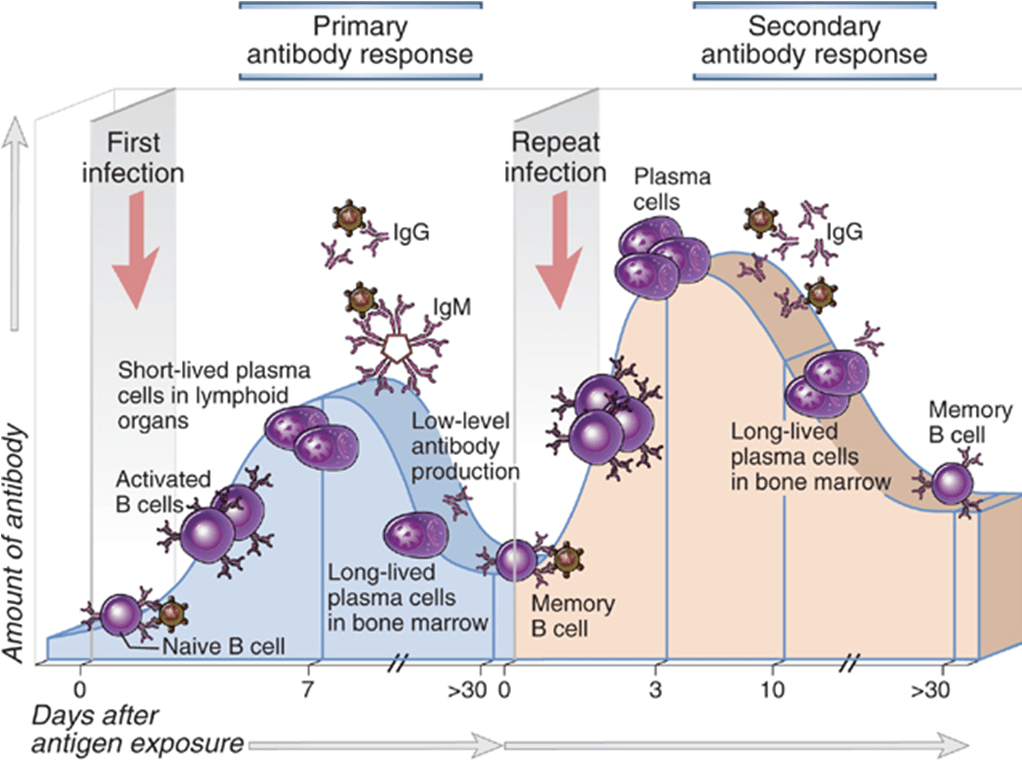
When you have an infection, your body responds with a host of inflammatory and immune cells. It’s a very good system, and if we are lucky enough to have a healthy immune system, it prevents us from becoming seriously ill from the various pathogens in our environment most of the time. But just like Sherlock Holmes, it needs a lot of information before it can produce its most incredible work.
To be perfectly honest, I prefer the BBC version of your immune system.
During that initial infection, the body is building antibodies, memory B and T cells, and other other specific immune cells targeted at that virus specifically. The next time you are exposed to that virus, the secondary immune response leaves the first one standing. With repeated exposures, the body learns that a threat is real and something you need to be prepared for; cells created after the first exposure, whether it’s from an infection or a vaccine, respond to the immune cells reacting to the 2nd exposure to create and even more robust response; cells that produce massive amounts of antibodies, cells that are incredibly active against the virus, and cells that move to the bone marrow and live for decades; maybe even your entire life.
If you’ve been lucky enough to avoid COVID-19 so far, the vaccines give you the opportunity to teach your body how to effectively produce this robust immune response without having to actually suffer through or take on the risk of getting the virus that has killed over 617,000 Americans in the past 18 months. If you’ve been unlucky enough to have COVID-19, but have recovered from it, the vaccines give you the opportunity to take that immune response you have already started building and ensure that you don’t just have some immunity, but that you actually have robust, probably very-long-lasting immunity. Your body doesn’t check Facebook or watch the news; the vaccines are your best and safest way of telling your body, “Remember COVID-19? Yeah, so that’s still a thing… Might want to be really prepared for it.”
It’s been a difficult pandemic. And while our COVID-19 cases and the severity of illness we faced as a community was undoubtedly worse over the Winter, the hardest time period for me professionally has been the past 3 or 4 months, as we have dealt with the emotional, psychological, spiritual, and physical fallout of the pandemic’s worst season, trying to help people rebuild while still managing chronic medical problems and, of course, trying to keep everyone safe from the possible threat of another surge.
Healing is hard. Anyone who has done Primary Care Medicine, and especially those who have served a community that faces a great deal of healthcare injustice, knows that those 10 or 15 minutes the doctor gets with the patient in the exam room are not nearly enough to address their mental and physical health needs. The extra time has to come from somewhere, and since there’s another patient already waiting in the next room, for me it tends to come out of evenings, weekends, and early mornings. The number of hours your Family Doctor (or PA, or NP) works on your behalf behind the scenes is hard to calculate. Just check out Dr. Glaucomflecken’s take on Family Medicine:
Or maybe ZDoggMD puts it best when he simply says, “We love our patients, hate the system.”
I last published on medical misinformation back in February. Since that time I have had to choose between writing and carving out some amount of time with my family, and even with such an important topic as COVID-19 and vaccine misinformation, it was a pretty easy choice. So consider this my apology to anyone who has sent me conspiracy theory videos and disinformation memes that I haven’t had time to write about over the past few months; I hope you found the answers you needed.
But when a doctor in your clinic texts you at 7 AM, and it’s a video of a former Chief Resident from your own residency program sharing outrageous disinformation about the COVID-19 vaccines in front of the Texas state senate, it’s probably time to pick up the pen (or keyboard) again and do your part to debunk it.
Can we all just agree to collectively ignore how cringey it is that I went with this GIF?
Dr. Ben Edwards Testifies in front of the Texas Senate Committee on State Affairs
I first saw this video this morning; it’s from earlier in the week and was sent to me by a Physician that actually trained with Dr. Edwards. It’s short, barely over 8 minutes long, and in keeping with my longstanding policy I have shared it below. If it does get taken down by YouTube, which seems unlikely since it was a testimony before a government body and part of the public record, I will make efforts to find another active link to it. Even though it is short there is a lot of misinformation to unpack here, so I’ll be following a time-stamp format below as we dive in.
0:09 “The Chair calls Dr. Ben Edwards” For context, this was part of a Texas Senate Committee on State Affairs hearing to consider a proposal by State Senator Bob Hall regarding what measures or policies public and private entities can and cannot implement based on COVID-19 vaccination status. It is part of a broader misinformation campaign trying to portray those who choose not to get the COVID-19 vaccine as experiencing widespread prejudice and portray basic epidemiology measures based on vaccination status as a form of discrimination.
Of course there’s a balance here; while the evidence that the vaccines are very safe is overwhelming, I don’t know any doctor that would be comfortable with people being vaccinated against their will (something that has never been on the table despite the alarmist misinformation to the contrary) or becoming second-class citizens based on a personal health choice. There’s a discussion to be had about which measures are reasonable for government and private entities to take based on vaccination status and which are not; absolutely there is. But as I’ve been saying since the beginning of the pandemic, any such balance has to be struck on the basis of truth; that is, on firm evidence and an honest understanding of how dangerous the COVID-19 virus really is. State Senator Bob Hall, a consistent promoter of myths and misinformation throughout the pandemic, is not a man I would trust to strike such a balance. The balance we need to find is not a middle-ground between truth and lies.
Evidence Based Medicine
0:29 “Ben Edwards, trained as a Family Physician” Family Medicine is a noble and challenging field of medicine. We take care of patients of all ages, we are trained in obstetrics and pediatrics, we perform many outpatient surgical procedures, and have experience in every field of medicine. Working in underserved care, we help carry some small fragment of our patients’ burdens and fight for healthcare justice on their behalf on a daily basis. It’s a struggle sometimes, but I am incredibly proud to be a Family Medicine Physician.
From what I can tell, Dr. Ben Edwards no longer practices Family Medicine. Or least, he doesn’t just practice Family Medicine. While the point of this post is to address Dr. Edward’s arguments in the video and not his philosophy of medicine, it is important to understand that despite the credentials and training background he shares at the beginning of his testimony, he now practices fringe, non-evidence-based medicine.
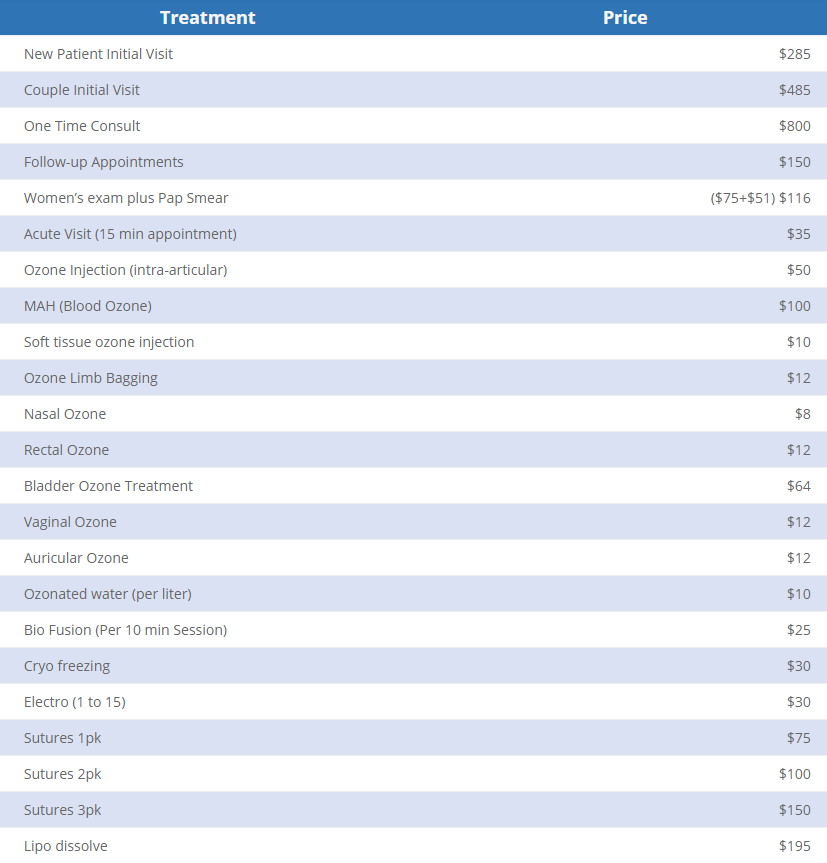
Take a look at the price sheet from his clinic’s website. Yes, there are some evidence-based services here; I am very thankful that his clinic is providing cervical cancer screening, and I certainly do cryotherapy for appropriate skin lesions in my own clinic. But they also provide a variety of unproven services like ozone infusions and ultraviolet blood irradiation.
As Dr. Edwards essentially states in the video, he does not believe in limiting his practice to only what is supported by scientific evidence. Maybe you believe in some of these treatments and maybe you don’t. Maybe you are curious about UV blood irradiation therapy or you believe that in vitro studies on the effects of ozone against cancer cells means it will really cure cancer (fire also kills cancer cells in a petri dish, but you wouldn’t inject it into your body). Maybe you are like me and believe this is essentially modern day snake oil. At the very least, I hope we can all give Dr. Edwards the benefit of the doubt and assume that he, at least, believes in his own medicine. Honestly it doesn’t really matter, because the main point is this; when a doctor tells you that he doesn’t believe in scientific evidence, why would you give credence to his testimony about scientific evidence?
0:30 “Did my undergrad at Baylor” I love Baylor University, despite its flaws. I have great friends that work there, men and women I greatly respect and admire who are working tirelessly to help it become the best university it can be. I’ll even be teaching a class there in the Fall. Still, I never studied there and am only a Baylor Bear by proxy, so this doesn’t hit too close to home.
0:31 “UT Houston Medical School” Great, fine. I went to UC Denver.
0:33 “And then Waco for Family Practice Residency where I was Chief Resident.” Uh-Oh.
The reunion is going to be awkward.
Now, Dr. Edwards and I trained more than a decade apart and we’ve never actually met; but I know doctors who trained with him, and I feel like a doctor who trained in my clinic, who probably even saw some of the same patients I’ve cared for, sharing false information before the state legislature definitely puts me in a position of “come get your people.”
0:57 “I’d like to begin with a reminder to everyone on the definition of Evidence Based Medicine“ When I first watched this video I did not know about Dr. Edwards’ alternative practices, so I was expecting something pretty standard and uncontroversial here. Most of the doctors I’ve argued with on this blog (I should say “argued against“, not with, since none of them know I exist) have portrayed themselves in the position of sharing scientific evidence, even when such evidence was anecdotal or when their analyses were utterly incorrect. None that I know of have actually come right out and said that evidence doesn’t matter to them, which is why I was so surprised by what came next.
1:09 “The elements of Evidence Based Practice are the integration of best research evidence with clinical expertise and patient values.”
Here’s the full quote if you want it. The landmark article was published in 1996; I’m assuming he found a later quote of the same article, which is where the 2002 in his citation comes from. So far, we are all on the same page.
“Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research.”
-David L. Sackett, OC FRSC, et al. Evidence Based Medicine: What it is and what it isn’t. British Medical Journal, 1996
Whoa, whoa, whoa. Hold up a second. Is that what Dr. Sackett meant? Is that what “integrating” means in the original quote, that one always trumpsthe other? Of course not. Yes, patient values always overrule anything else we do in medicine; but that’s the ethics principle of patient autonomy, not the best practice for harmonious, evidence-based patient care, where the physician and the patient work together to find an evidence-based treatment that corresponds to the patient’s goals and values. In order to understand Dr. Edwards’ subsequent comments better, let’s look at what that quote actually means, and how his interpretation of it completely turns it on its head.
Example 1: Insulin for Diabetes. Integrating patient values, evidence, and clinical expertise. I will use this illustration becomes it’s a conversation I have multiple times a month. Let’s say you have a diabetic patient whose blood sugar is still not well controlled despite taking multiple oral diabetes medications. The best evidenceon helping that patient prevent the terrible long-term effects of uncontrolled diabetes says it is time to talk about starting insulin. And for most patients, that’s what ends up happening. But the principle of integrating evidence with clinical expertise and patient values means that decision is a discussion, not something you can arrive at with a flow-chart or a “Idiocracy” style medical computer interface.
That discussion is focused on your patient’s values. How do they feel about insulin? What is their personal or family history with insulin? For many people who have a family history of diabetes, insulin carries an emotional weight; it represents the point where their loved one’s diabetes began to take a more severe toll on them. Of course there’s good reason for that, we give it for more serious cases of diabetes; but I’ve often spoken with patients who genuinely believed that insulin would make you lose your leg or your eyesight based on associations they have had since childhood. Even when we carefully discussed that this was actually due to the uncontrolled blood sugar levels the insulin was prescribed to treat (and my patients typically see that distinction right away once I really explain it), the emotional impact of starting insulin remains. For others, the inconvenience of daily or multiple-times-per-day injections or the barriers involved in administering the medication may represent an insurmountable barrier.
And this is where clinical expertise comes in, to help bridge the gap. The doctor, who has (hopefully) earned the patient’s trust and proven themselves a reliable source of health information and wise counsel, now has to figure out how this evidence relates to this specific patient. The person is a person and people always fit imperfectly into diagrams and algorithms. Maybe the evidence says insulin is indicated at this point, but you also know this patient was recently on a long taper of steroids for resistant poison ivy; steroids that drove up the blood sugar and gave the impression of worsening diabetic control. Maybe your patient has such a negative association with insulin that this discussion itself was the wake-up call they needed to take greater ownership of their health, and you truly believe they are going to be able to get their blood sugar down through dietary changes, exercise, and better adherence to their other medications even without the insulin. Or maybe you are seeing not just the high blood sugar numbers, but also the early signs that the diabetes is taking a toll on their body; the early signs of neuropathy in the feet, the subtly worsening renal function, the minor scrapes and wounds that just aren’t healing like they used to. In that case, integration of evidence, expertise, and patient values may mean helping your patient find a way to be ok with starting insulin, and walking alongside them knowing it’s a really difficult decision for them; or helping them fully grasp the medical realities they are facing so they can make the most informed choice possible, even if it’s not the one you were hoping for. Your medical expertise doesn’t mean practicing against the evidence or ignoring the evidence any more than it means trying to overrule your patient; it means combining your understanding of the evidence with your relationship with the patient to help the patient thrive. It’s why we have doctors in the first place.
Contrast this to Dr. Edwards’ misrepresentation of these concepts.
“Patient values trump clinical expertise, and clinical expertise trumps the scientific evidence.”
Dr. Ben Edwards, Just Now
Example 2: Antibiotics for Viruses. Patient values trump clinical expertise; clinical expertise trumps evidence. There are a million examples we could use to illustrate the model Dr. Edwards seems to espouse, but this one is prototypical. Let’s say you have a patient come in for upper respiratory symptoms; cough, runny nose, slight fever, etc. (for the sake of argument let’s say it isn’t in the middle of a global respiratory viral pandemic). You have diagnosed the patient with an upper respiratory virus, and they tell you they would like a prescription for antibiotics. Since they have no indication for needing an antibiotic, prescribing one would be a medical error; probably not a dangerous error, but it’s possible; antibiotics are notbenign medications. Normally, this would be an opportunity to educate your patient. This is one of the most important roles physicians have; we have the privilege of years of high level medical training that almost none of our patients had access to; it is a true joy to see your patients more empowered and more knowledgeable because of their relationship with you. Under Dr. Sackett’s model, this would be part of integrating patient values and medical evidence.
Or you could take a different approach. If you believe that “patient values trump clinical expertise, and clinical expertise trumps scientific evidence,” you could do some pretty modest mental gymnastics to convince yourself that your patient wanting an antibiotic is part of their “values,” and therefore the right medical decision despite there being no evidence that it will actually help them, and plenty of possibility that it will harm them. By treating preference or assumption as though they were values and autonomy, you have moved from evidence based, patient-centered care to retail medicine; just give the people what they want. A doctor who has fully embraced this philosophy of medicine won’t help you reach a diagnosis, won’t help you get treatment supported by the full weight of thousands of years of learning about the human body that humans have acquired, and won’t help you face harsh realities about your health and learn to cope with them. Such physicians, whoever they may be, have apparently decided that their hard-won medical degrees and board certifications were really just a means to gain the power to prescribe treatments; not to take on the responsibility to use that knowledge and experience in the best interest of their patients.
Thanks Uncle Ben, we needed to hear that.
But the second part of Dr. Edwards’ quote is even more disturbing, if only because it is seemingly so much more common. “Clinical Expertise trumps Scientific Evidence.” In the best light, this mindset seeks to portray the Physician as the Lone Ranger, a maverick that plays by their own rules and uses common sense instead of all that med school learning. They don’t need fancy books and studies to tell them how to care for their patients, they just know. The went to the Med School of Hard Knocks, etc. And the scary part is that we are all really at risk to fall into that mindset and paint ourselves in this light.
But every single time, it’s because we as Physicians have fallen into one of three professional sins; hubris, avarice, or laziness. The former abandons evidence, holding their own clinical experiences higher than the accumulated experiences and careful analysis of their peers around the world, because they think that they alone are capable of intuitively navigating the minefield of confirmation bias and tunnel vision that constantly threatens those who seek to heal. The second abandons evidence because it simply isn’t profitable; a lot of evidence based treatment involves sitting with the patient in the midst of pain and difficulty, helping them find internal resilience and make healthy choices, or prescribing simple, affordable (with the right advocacy) medications that you will never see a dime from (your doctor doesn’t get a cut of your prescription medications!). Instead choosing to push designer, unproven and unregulated treatments can be incredibly lucrative; all doctors know that our medical degrees could be incredibly profitable if we abandoned medical ethics; it’s a temptation we all see coming a mile away, but some still fall into it. The third; well, it’s the easiest of all to understand. I would love to tell myself that my clinical expertise trumps scientific evidence because it’s comforting; it means it’s ok if I can’t keep up. Medicine is hard, and there’s a lot of it; human health and disease is a vast and complex field. If arrogance and greed aren’t my bugbears, this one definitely is; I know I have the tendency, like Dick Van Dyke’s character in Scrubs, to rest on my laurels and lean on my own understanding because I just don’t have the energy. I have to fight that temptation every day.
Saying my clinical expertise trumps the evidence is really just a self-assuring way of me saying that my clinical expertise trumps everyone else’s.
Vaccine Safety
1:29 “I am also concerned that the forced and coerced COVID-19 vaccinations would be a violation of the Nuremberg Code, etc.” I completely agree, and as a Physician I would never support any forced or coerced medical treatment of any kind; patient autonomy is sacred.
I also don’t know what he’s talking about; I’ve heard exactly zero evidence that anyone is being forced or coerced into being vaccinated against COVID-19. When patients come to see me and we discuss the vaccines, we look at the evidence together and I help them integrate their values with the best available evidence. We don’t shoot needles in their arms as they walk in; we don’t deny them services if they don’t want the vaccine. Right now, I don’t know of any businesses that deny service if you aren’t vaccinated, and I certainly don’t know of any government services vital to health and human thriving that do so either. I’ve heard of some sporting events- huge gatherings that are entirely voluntary to attend and have the potential to become super-spreader events- having separate entrances or seating sections for unvaccinated and vaccinated attendees. Surely we do not consider this to be tantamount to forcing or coercing vaccines? I always want to look at the strongest argument from the other side; if you know of a situation that comes closer to truly forcing COVID-19 vaccinations on people, please send it my way.
2:00 “According to the CDC’s vaccine adverse event reporting system (VAERS), 4,178 deaths are now being reported.“ I think this is the most important point in the entire video, and it’s worth spending some time on. This is a similar claim to one that’s been circulating on social media, and even repeated earlier this month by Tucker Carlson. And the thing is, it’s a fascinating bit of misinformation. Let’s dive into it.
Dr. Edwards shares a number that is incredibly easy to find; the number of deaths reported in VAERS for all people who have received a dose of the COVID-19 vaccine. You can find the numbers for yourself; start by going to https://vaers.hhs.gov/data.html and clicking through until you find an option to search the VAERS data, then select the COVID-19 vaccines and run a report on ‘deaths’. It took me less than 5 minutes to figure out how to run the report, and I’ve never used the system before. Nobody is trying to hide this data. I will note, however, that you have to indicate that you agree that you have read and understood a disclaimer that you can’t use this data the way Dr. Ben Edwards is using it in this video because that’s not what it means at all. At the very least, Dr. Edwards is guilty of breaking the website’s end-user agreement.
Running the report right this second gives me a figure of 3,919 deaths of persons who have received at least one dose of the COVID-19 vaccine; close enough to Dr. Edward’s 4,178 that we won’t split hairs about it. So we agree on the numbers, which are publicly available. The more important question is what the numbers mean.
Remember last year when we repeatedly saw the claim that deaths from COVID-19 were being inflated to make the pandemic look more dangerous, and that all deaths at any point following COVID-19 infection were being called “COVID Deaths,” even if someone got shot or hit by a car or died of cancer. I debunked this one over and over again, but the key to understanding that misinformation hinged on understanding death certificates. Those numbers of COVID-19 deaths were not raw data of ‘everyone who had died’ around the time they had COVID-19; there were based on the detailed reports of physicians, coroners, and other medical experts who had to analyze the cause of death and file a report, with their name attached, in a specialized system that not everyone has access to. If a death is reported as being from COVID-19, it is because a medical expert believed that COVID-19 contributed to or caused the death.
But the VAERS system is the exact opposite. As the disclaimer on the VAERS website says outright, this is raw data without any analysis attached. It can be submitted anonymously and by absolutely anyone. And it absolutely includespeople who happened to die from car accidents and gun shot wounds at some point after receiving the COVID-19 vaccines.
And I find this really fascinating because it really seems like after a year of saying the CDC and WHO and your Family doctor down the street were just attributing every death to COVID-19 to inflate the apparent danger, which wasn’t true at all, the medical misinformation spreaders decided that was actually a great idea and decided to do that exact thing with the COVID-19 vaccines! “If you can’t beat ’em, join ’em!”
So now that we understand a little better why the VAERS data can’t be used the way Dr. Edwards is trying to use it, to say that those 4,178 deaths are due to the COVID-19 vaccine, let’s look at what that data does mean.
The first question we have to ask ourselves is, is this more deaths than we would expect in this population even if people didn’t get the vaccine? This is a concept called attributable mortality, and it’s been one of the major proofs of the real danger of the COVID-19 virus against all of the misinformation claims over the past year. We can’t get perfect data from the VAERS system (because, again, that’s not what it’s for), but what we basically need to ask ourselves is whether the death rate in those who received the COVID-19 vaccine is any higher than the rate we would have expected from all causes anyway. Let’s do that math.
To date, 158.4 million Americans have received at least one dose of the COVID-19 vaccine, which became available to the public just over 5 months ago on December 14th, 2020. That’s just below half of the US population. Half the US population with at least one vaccine dose; 4,178 deaths reported on VAERS since we started vaccinating. In that same time period, there have been over 1.4 million deaths in the US. Or to put it another way, in a population of 158.4 million people we would expect about 517,924 deaths in the amount of time since we started vaccinating people. And that’s based on pre-COVID mortality rates.
So among the people who receiveda dose of the COVID-19 vaccine, VAERS reports far fewer deaths than would be expected in the normal population in that time period. Does that mean that the doctors and nurses are lying about vaccine safety? Does it mean that the CDC is changing the numbers? Does it mean the COVID-19 vaccines are protecting people against more than just COVID? Does it mean they are bestowing some degree of immortality or vitality on people, protecting them from heart disease and diabetes and gunshot wounds?
No. It just means you can’t use the data that way because it doesn’t represent what Dr. Edwards is telling the senate it represents. That’s it.
2:00: “Over the past 20 years, all vaccinations combined there were a reported 4,182 deaths.”
The second question we have to ask is why the deaths reported on VAERS (I won’t say ‘the deaths associated with the COVID-19 vaccine’ the way he does, since we just saw why that is not accurate) in the past 4 months rival the deaths reported from all vaccines in the past 20 years. Surely that, regardless of the small number of deaths compared to the general population, indicates that these vaccines are far more dangerous than ‘traditional’ vaccines we’ve been using for years, right?
No. Again, it entirely depends on what those numbers mean, and the fact that we are reporting adverse events differently for the COVID-19 vaccines than we have for vaccines in the past. This is not clandestine or hidden information; it’s right there on the VAERS website under the reporting instructions. Look at the instructions for medical professionals for reporting adverse events following vaccines, from the VAERS reporting FAQ:
For most vaccines, we report adverse events that have a credible link to the vaccine itself, such as an allergic reaction, and any serious events that occurred within a specific, limited time period following the vaccine. Here’s a preview of the table they mention and link to above:
So for the DTaP vaccine, for instance, I would obviously report a severe reaction like anaphylactic shock, if it occurred within 7 days of the vaccine. Anaphylactic shock doesn’t occur a week after a vaccine, and yes this would mean that I would still report it if the patient got a vaccine on Monday and had an anaphylactic reaction to a bee sting on Sunday… But that’s really unlikely, and they have to set a reasonable, liberal time-period. If the patient dies from that anaphylaxis or complications of the reaction, that gets reported too. If the patient is shot, or they develop sepsis from a pneumonia, or their heart failure claims their life, those events don’t get reported because there is no theoretical link between those events and the vaccine; that data is being filtered through clinical reasoning. Which makes sense, because in the past 20 years about 60 million Americans have died; some of those folks happened to receive a vaccine of some sort around the time of their death, but with no plausible causal link there would be no reason to report those deaths on VAERS; it would be entirely unreasonable and misleading to do so.
Now look at the instructions for COVID-19 vaccine adverse event reporting, from the same FAQ:
If a patient dies at some point after receiving the COVID-19 vaccine, healthcare professionals are required to report it. Even if there is no theoretical link; even if there is no possible causal link, such as the reports in VAERS involving traffic accidents and end-stage cancers. If a patient dies and the clinician knows they have been vaccinated against COVID-19, they are required to report it in VAERS, full stop. That’s not the case with other vaccines, so it makes sense that many, many more of the deaths that occur every day as a part of normal human life will be reported on VAERS than ever before. And that’s a good thing; it’s better to have that data than not have that data. But using that data in a way it was never intended, to scare people away from safe and life-saving vaccines, is either ignorant, unethical, or both; you are told before you even pull of the data what it represents, and my hope for Dr. Edwards is that he simply didn’t understand this when he testified in front of the state senate; to knowingly misrepresent this data is simply lying.
The other thing you’ll notice from the above instructions is that, unlike with the TDaP or MMR vaccines, there is no time limit on COVID-19 vaccine adverse event reporting. That means that, while deaths within a week or two of the vaccines are more likely to be reported because the professional treating the patient is more likely to be aware of their recent vaccine, it is still technically required to report deaths on VAERS even 4 or 5 months after vaccination. The same goes for all adverse events. And lest you think it’s far fetched that any of the data on VAERS is coming from that long after people got vaccinated, just remember that if you signed up for V-SAFE to report adverse events to the CDC on your smartphone, you were still getting these texts months later:
I was vaccinated in December
So to summarize, those 4,178 deaths that Dr. Edwards mentions are an incredibly small percentage of the people who have actually died in the US in the past 5 months, those deaths reported on VAERS are explicitly stated by the reporting system itself to not represent a causal link with the vaccines, and out of 1.6 million people who have been vaccinated it is a statically insignificant figure. And the rules for reporting adverse events to VAERS are different for the COVID-19 vaccines than for other vaccines, both in the types of events reported and in the length of time since vaccination that a report is required; comparing the “deaths associated with the COVID-19 vaccines” on VAERS to the “deaths from all vaccine over the past 20 years” isn’t just comparing apples to oranges; it’s a total misrepresentation of the data. It’s a scare tactic, plain and simple.
2:29 “This includes a 15 year old boy in Colorado, two 16 year old girls in Wisconsin, a 17 year old girl in Wisconsin, and a 17 year old boy, all healthy, in New Hampshire.” If these 5 teenagers have died it is absolutely a tragedy. At this point we do not know anything about them; their names, their medical conditions, their history, or what led to their deaths. We don’t have that information because it isn’t in VAERS, and because there are no independent, verified reports of these deaths available. You can search for local news stories or articles about these individuals and so far there don’t seem to be any details of these situations; no information other than that they died at a tragically young age, and that they had receive the COVID-19 vaccine at some point; and all of that only from VAERS itself. Remember that the VAERS reporting system is anonymous, open to anyone, and that none of the reports are verified. In fact, though we know that the COVID-19 vaccines have never been given to children younger than age 2, even in clinical trials, when you run the numbers on VAERS there are well over 200 reports of adverse events to the vaccines in that age group. This is raw, unverified data from the public and it has to be understood as such.
The CDC really does investigate these cases; far from the conspiracy theories about the CDC trying to cover up vaccine injuries, the whole goal of V-Safe and VAERS is to help us make sure the vaccines are safe, and a lot of resources are devoted to following-up on these reports. When there are reports of deaths in teenagers who have received the COVID-19 vaccine, that deserves attention and an assumption of authenticity; but there is no reason to believe that the COVID-19 vaccine they received contributed to the death; VAERS can’t tell us that. What we actually have is basically, “someone went online and reported a death in a teenager who had been vaccinated against COVID-19. We need to look into this.” By transforming this into “the COVID-19 vaccine killed this teenager,” Dr. Edwards is not advocating for the teenager and their family. He is not bringing light to their situation. He is simply using the report of that death in VAERS to create fear, with no understanding of the circumstances around that death and no knowledge of the people affected by that tragedy. We cannot use other people’s tragedies, which we know nothing about, to promote our own political agendas.
2:42 “The evidence is pretty clear that VAERS grossly underestimates the adverse events that are reported... Only 1% of adverse events are ever reported to VAERS.” This is absolutely true, but before you let Dr. Edwards guide you into inaccurate assumptions, you need to realize the subtle switch he’s just made.
Up until now Dr. Edwards has been talking about deaths reported in VAERS. He’s given numbers, he’s given tragic examples. He’s been trying to convince you that the number of deaths “from” the COVID-19 vaccines has been astronomical. Without any clarification or verbal signal, he has now switched from deaths to adverse events.All adverse events, including mild reactions. So when he tells you that ‘4,178 people have died from the COVID-19 vaccines’ (which isn’t true), and then immediately tells that “less than 1% of adverse events are reported to VAERS,” he wants you to do some quick head math and say to yourself, “Wait, that means that over 400,000 people have died from the vaccines!” If that number sounds crazy to you, it’s because it is. We passed 400,000 deaths from COVID-19 in January of this year (we are now pushing 600,000). It took 11 months from the first American COVID-19 death in February 2020 to get to that point, and at various times in the pandemic our hospital systems were utterly overwhelmed. If we were now seeing 400,000 deaths from the COVID-19 vaccines in 5 months, you wouldn’t have to watch Dr. Ben Edward’s testimony on Facebook or YouTube to hear about it; you would be seeing it in your hometown, you’d be hearing about it from your friends and family who were affected by it personally. Your local hospitals would be on divert and over-capacity like they were because of COVID-19 back in December. No, the COVID-19 vaccines are not causing massive numbers of deaths. In fact, they are very, very safe.
So where does that 1% statistic come from? Well let me ask you; when you had a sore arm from the Flu shot last year, or your child spiked a mild fever due to their MMR shot and you had to give them tylenol, did you report it on VAERS? No; I didn’t either. We could have, it would have been totally reasonable to do so; but since those were expected, mild, self-limited reactions to the vaccines it never occurred to us to report them. The more serious reactions are reported at much higher rates, which is exactly the way VAERS is designed. There’s a great discussion of this phenomenon on Vaxopedia, and since they’ve done the literature review already I’m going to steal some of the studies they cite.
Serious reactions, and especially deaths that clinicians believe might be linked to a vaccine, are going to be reported at high rates, while mild, expected reactions will be reported far less than 1% of the time. Dr. Edwards uses “deaths” and “adverse events” almost as synonyms in this section by not clarifying what that 1% statistic really means. At the end of the day, the Vaccine Adverse Event Reporting System is doing exactly what it is supposed to do; providing huge amounts of raw data that we can search for unexpected patterns and then form hypothesis. Unfortunately, any time raw data is publicly available, there is the risk that people, including physician scientists who trained in Waco, will latch onto the data and use it to weave false narratives, stoking unfounded fear and panic.
3:44 “Personally I have received numerous reports from family members of my patients, close friends of my patients, that within hours to days of receiving the vaccine they have suffered from stroke, heart attack, pulmonary embolism, blood clots, and death.”
I also see patients every day, and many of my patients have received their COVID-19 vaccines. I couldn’t give you an estimate of how many. My patients are typically excited to show me their vaccine card and we celebrate together that they now have better protection against the virus. I always ask if they had any side effects, and I often hear about body aches, chills, nausea, fevers, malaise, and fatigue; “All the things you told me to expect, Dr. Webb.” I also talk to plenty of patients who had a sore arm, or no side effects at all. I have had no patients tell me about a dangerous side effect or death they believed was related to the COVID-19 vaccine.
How do we reconcile this? One of two ways. Either one of us, me or Dr. Edwards, is lying; or at least exaggerating. Or else, we are receiving the types of narratives from our patients that they expect we will resonate with and appreciate. My patients know I am a vaccine advocate and I want to see them protected against COVID-19. Some of them know I write about COVID-19 misinformation. Many decided to get vaccinated after we talked about the vaccines and I answered their questions. It’s entirely possible that my patients are more apt to tell me about their minor symptoms. But isn’t the opposite at least as true for Dr. Edwards? My population of patients are from all walks of life, all backgrounds; his are self selected; they have specifically chosen his clinic because they are strong believers in homeopathic and alternative medicine and want those services. Their doctor is against vaccines and they likely know it just as much as my patients know I am for them. Wouldn’t his patients be apt, even anxious to share vaccine horror stories they had heard with him? And of course, referencing these stories later while trying to make a point, how much verbal precision can we expected someone to exercise in distinguishing between “my patients have told me they’ve heard stories about serious adverse events from the vaccines” and “my patients’ friends and family members have experienced serious adverse events from the vaccines.” It’s the most important distinction in the world; it’s also exactly the kind of distinction most of us wouldn’t scruple to make if we really believed our point was valid and wanted to emphasize it as strongly as possible. Adverse events, like jokes, are best when told in the 1st person.
Vaccine Immunity vs. Acquired Immunity
4:19 “Studies have shown a 2-3 fold increase risk of adverse reactions to this vaccine if you’ve already had COVID.” I am not familiar with the studies he is referencing here, but I don’t doubt this for a moment. We already expected this because of the more robust set of side effects we’ve seen with the second shot in the Moderna and Pfizer vaccine series; in fact, I’ve been counseling my patients to expect more robust side effects if they’ve already had COVID-19 for months. It certainly matches my experience; I had COVID-19 in December and got the vaccine a few weeks later; I had body aches, chills, and nausea after both doses, not just the 2nd, and I’m sure it was because I had already had COVID-19.
Remember, he is not saying there is a 2-3 fold increase in injury or death from the COVID-19 vaccines if you’ve already had the virus; just in adverse reactions. Most of the adverse reactions we experience are related to our body’s immune response to the vaccines; they are part and parcel of that robust immunity we are hoping for. We get fevers after vaccines because of Interleukin-1, which the macrophages that pick up the viral proteins release to stimulate B and T cells. We get body aches and headaches because of the Interleukin-6 those cells produce to turn the B cells into antibody producing plasma cells. We feel tired because… Well, nobody really knows; but all of that immune response does take up a lot of energy. Yes, you are more likely to have adverse events after the COVID-19 vaccine if you’ve already had COVID-19, because your immune response is more robust; those “adverse events” are the symptoms of your immune system working.
4:26 “Natural immunity confers a more robust immunity than vaccine immunity could.” Dr. Edwards repeats this idea multiple times in the next minute, and there was a time I would have agreed with him; intuitively it seems like that would always be the case. But it isn’t true. This is an area where I was skeptical at first, but the data has forced me to change my mind; the COVID-19 vaccines really do create a stronger immune response than our own natural response to COVID-19 once we’ve recovered from it. My friend and medical misinformation hero Dr. Emily Smith has written bout this before, and she’s better at explaining things than I am:
So Dr. Edwards is simply incorrect on this point. But it’s not a competition between your body’s response to COVID-19 and your body’s response to the vaccine, because his assertion that it is dangerous or unwise to vaccinate someone who has already survived COVID-19 is inaccurate; it’s actually the best immunity you can get, if you were unfortunate enough to already get sick from COVID-19 like I was.
This kid gets it; disease acquired immunity and vaccine acquired immunity together is the best protection you could hope for.
5:03 “God gave us an amazing, robust immune system, and I don’t think you can improve on God.” Absolutely! I complete agree. I was writing about how awesome our immune system is, and how we ought to treat it, back at the beginning of the pandemic. I’m a big, big fan of my immune system.
You know who else was a fan of the immune system? The folks who invented vaccines. Vaccination came to the United States from, among other sources, an enslaved African man in Boston whose knowledge of the African traditional medicine practice of inoculation helped save hundreds, maybe thousands from Smallpox in the 1720’s. We don’t know his true name, but his slave name was Onesimus, and it’s only in recent years that his insight and knowledge is bringing him the credit that was previously received only by the man he shared these with, the Boston doctor who owned him.
Onesimus, like the traditional healers before him and the vaccine pioneers since, understood that the immune system is an incredibly powerful defense against disease, but that it works best when it knows what it is fighting. By giving the immune system a template- previously by injecting a small amount of live pathogen into the body through inoculation, but now by presenting it with just a few key proteins (that cannot cause disease) through vaccination- we unlock the immune system’s full, robust, God-given disease-fighting potential. Vaccines are not an improvement on God’s design; that’s just anti-vax propaganda. They are the best way we have to arm the immune system with the information it needs without having to actually get sick in the process.
Imagine you want to assassinate someone (for the sake of argument), and you hire the world’s best assassin. You pay her exorbitant asking price, all up front and in unmarked bills, and receive her guarantee that the job will be done. Finally, you try to tell her the name of the target, maybe even hand her a picture and dossier; she plugs her ears and won’t look at the picture. “I’m the world’s greatest assassin,” she says, “I don’t need to know who the target is.”
That’s what it sounds like, saying we shouldn’t try to “improve on God’s design” of the immune system with vaccines.
The full, ironic title of this blog post is actually “Why would any Black American trust these new vaccines? A white doctor’s perspective (because, you know, that’s exactly what we need more of),”but it was too long to fit in the title heading.
As a white, male doctor, I am not the best person to write this blog post. Thankfully I am not the only person writing and talking about this, and am in fact a late comer both to the issue of higher rates of vaccine skepticism within medically marginalized communities and to the larger issues of racial health equity and healthcare justice in general. Much of the work that has already been done in this area comes directly from Black physicians, scientists, healthcare workers, and community leaders who are concerned about the disproportional impact the COVID-19 pandemic has had on people of color, and have been working hard on behalf of their communities to verify that the vaccines are trustworthy and effective, and to ensure equal access to this lifesaving intervention.
I believe those voices are far worthier of your time than this post, whether you yourself are a member of a medically marginalized group trying to decide about the new vaccines or, like me, someone who just wants to gain a deeper understanding of the ways that American medicine’s history of racial discrimination and research exploitation have contributed to ongoing healthcare disparities and earned mistrust. That’s why I’ve flipped the usual structure for this post and have placed additional resources and reading as the first proper section, instead of tacking them on at the end or dispersing them throughout the essay. Many of the resources I’ve included come directly from my Black peers in medicine, or our colleagues in research or community health.
So I write about this topic today not because I believe my perspective is the most important one or because I believe I have something particularly unique to add to the conversation, but rather because I believe this issue is soimportant that we should all be talking about it. Further, I am writing because a certain number of African American men and women have already entrusted me, as their primary care doctor, with the the sacred responsibility of helping them navigate these issues as they make decisions about whether or not to trust the vaccines, and because a good portion of my time over the past few weeks has been spent doing that work. And finally, I am writing because the vast majority of those medical research atrocities that laid the groundwork for the dilemma many Black Americans face today were committed by people within a group I belong to: white, male, American doctors. And even though I claim no kinship with their ilk, and believe that in breaking their sacred oath and committing grievous harm against their fellow man they have forfeited the title of “Physician,” nevertheless I have benefited in various ways from those crimes, and believe that a responsibility rests specifically with white doctors to do whatever we can to bring that history to light and mitigate its consequences. We should not strive to dominate the conversation, as we have so often done; but neither can we stay silent and remain complicit in that exploitation.
COVID-19 Vaccine Resources from Black Medical Experts
If like me you find that you only have a limited amount of time to read today, I would recommend the following resources; you can always come back to my blog post later. In other words, start here.
BCAC19 is a DC area coalition of Black doctors, scientists, healthcare workers, community leaders, academics, and political voices working together to stop COVID-19 misinformation and rebuilt trust in medicine, in order to help Black communities fight the pandemic.
On their website they host public health resources, a COVID-19 FAQ, and town hall videos with medical and community leaders discussing issues around the COVID-19 vaccines.
The Black Coalition Against COVID-19 has also produced this short but important video touching on the importance of trust and accountability in every step of the vaccine creation and rollout process.
This video and article focus on Jeff Fard, founder of the Brother Jeff Cultural Center in Denver, and his work on combatting the health consequences of COVID-19 on his community. It then branches out to look at what Black-led medical institutions and organizations are doing to support communities of color across the country during the pandemic.
One of the many excellent articles about Dr. Kizzmekia Corbett, PhD, Virologist and one of the team leads who helped develope Moderna’s mRNA vaccine (the one I and so many of my colleagues and patients have already received).
A featured essay in Business Insider magazine, written by Infectious Disease expert Dr. Lisa Fitzpatrick. “I’m a doctor who volunteered to get one of the first coronavirus shots. Here’s why I got involved, and what the side effects have been like.”
Local Resource: This is a Waco COVID-19 Vaccine town hall led by African American community leaders, from just a couple of weeks ago. It features Dr. Terri Woods-Campbell, a former teacher from my days in medical residency, and one of several Black, female Physicians who trained me in surgical skills over the years.
This one is more academic but offers such an important perspective on the vaccines. It shares an account I first discovered in the pages of Medical Apartheid; the story of an African man known only by his slave name, Onesimus, and how his knowledge of traditional African healing practices and the techniques of variolation saved hundreds of lives from Smallpox and pointed the way toward the future of vaccination science.
The Problem: A History of Racist Medical Research Abuse
I’ll start with a personal story (so bear with me). During my first clinical rotation during 3rd year of medical school, I worked with an upper level resident who despised me. And she had good reasons. I was really struggling academically at the time and my medical knowledge was far behind my peers. Just as importantly, I was a rotation behind them in 3rd year clinicals; it was my 1st rotation, but their 2nd, a lifetime in terms of clinical experience and ability to contribute to a medical team. All of this together meant I was a weak medical student (in medical education we inexplicably still use words like “weak” and “strong” to describe people who struggle withdifferent aspects of the incredible burden of practicing medicine) and, in all honesty, a big drain on her teaching time and resources.
One day during lunch, the program director was lecturing on the history of Gynecology and the techniques and instruments invented by Dr. J. Marion Sims, the “Father of Modern Gynecology,” in Montgomery Alabama in the early 1800’s. The program director posed this question, seemingly rhetorical: “Historically, medical researchers have not always had access to enough volunteers for new techniques and medicines, so who have they used when volunteers weren’t available?” I was a weak med student but I at least had a liberal arts education and knew a little about history, sociology, and moral philosophy, so I answered; “minorities and the poor.” My upper level resident clearly interpreting this as either an off-color joke or even an endorsement of such practices, and generously wanting to save me from immediate expulsion from medical school, shot out her hands in a gesture meant to quell the coming storm and exclaimed to the whole table, “He’s joking. You’re joking, right? Tell them you’re just joking”
But I wasn’t joking, and said so; those groups were exactly who had been used for medical research when the experiments were too dangerous or degrading to recruit volunteers, and it was pretty clear that that was exactly where the program director was headed in that talk. We spent the rest of the lecture learning about the abuse and violent exploitation of poor, Black slave women that had enabled Dr. Sims to perfect his techniques before using them on the patients actually meant to benefit from his research; wealthy whites. These techniques, practiced on slaves without anesthesia and often resulting in infection or other severe complications, eventually made his name famous and led to his becoming the president of the American Medical Association. Only recently has Dr. Sims lost some of the celebration he attained in life because of this history. (The brief slideshow below shows his statue being removed from New York’s Central Park in 2018; you can read about it on NPR from the link provided)
A woman stands beside the empty pedestal where a statue of J. Marion Sims used to stand. Multiple groups demanded the removal of the statue, which sat on a pedestal praising his achievements as “brilliant” without acknowledging the women who endured his painful experiment
But before I run the risk of anyone thinking the above is a story of my wokeness as a medical student (exploitation of allyship, anyone?), I was anything but. I had got the answer right that day (probably for the first and last time during that 2 month rotation) more because I was good at guessing what a lecture was about from the intro than any actual insight into issues of race and justice. I had learned about the Tuskegee Syphilis Study in college, I learned about J. Marion Sims that day in med school; and later during residency I was confronted constantly with the realities of racial healthcare disparities today. And that was it. I was aware of three ‘situations’ out of a 400 year history of abuse, violence, neglect, and exploitation. And for several years, though I grew slowly in this area and fought for healthcare justice 80+ hours a week, I remained essentially ignorant to the actual scope of American Medicine’s racist history (and, you know, racist present).
And if I’m being perfectly transparent and honest, I was at times really frustrated by how my African American patients sometimes seemed to be slower to trust me as their doctor, or to be more suspicious of treatments I recommended, than a lot of white patients. Like many people, I no doubt would have responded to the recent revelation that only 25% of Black Americans planned to get vaccinated against COVID-19 with knowing sagacity; ‘for some reason, Black patients are just more suspicious of modern Medicine. Hmm, oh well… I guess it will always be a mystery.‘
Then in 2020 a chance recommendation led me to download an audiobook (and then later purchase a hardcopy and an E-Edition) of Harriet Washington’s Medical Apartheid. A keen historian and a lover of science and medicine, Ms. Washington started with J. Marion Sims like we did that day in medical school; but then instead of jumping ahead a hundred years to Tuskegee or Henrietta Lacks, carefully traces a thorough but not exhaustive (as she herself states, that undertaking would take a lifetime and would fill volumes) history of clinical and especially research abuse towards Black Americans, beginning with the medical abuses towards slaves that were so common on the plantation and continuing through emancipation and reconstruction, Jim Crow, the Civil Rights movement, into the modern era and the exportation of medical research abuse to Africa where researchers can more easily get around ethics regulations, and finally concludes in the 1990’s and early 2000’s (it was published in 2006) with exploitative research in topics from drug dependence to human reproduction to criminality, all of which continue to pick and choose data to portray ethnic minorities, and especially those of African descent, as less developed, more aggressive, and in many ways less human (though less overtly than the “research” of the 1700’s and 1800’s) than the “normal;” that is to say, white people.
I’ve been thinking of the best way to distill this incredible, earth shattering, 512 page work into a single section of a blog post, and I’m at a loss. We could choose any of the hundreds of examples she gives in the book as reasons why Black Americans might be slower to trust American medicine than their white neighbors.
One that stood out to me was the section “Racism by Numbers” in Chapter 6 when she discusses the US Census of 1840 which showed significantly higher rates of mental illness and disease in free Blacks compared to those still in Slavery; proof, according to Southern plantation owners and their political allies, that freedom was unhealthy for Blacks, that they were too mentally feeble to handle making their own daily life choices. That scientific data was a huge blow to the abolitionist movement against slavery… Until it was utterlydebunked as false and based on horrible methodology and underlying racism, by an African American Physician, Dr. James McCune Smith (the first Black American to earn a medical degree, though he had to go to medical school in Scotland to be allowed to do it) and a white Physician and statistician, Dr. Edward Jarvis. I mentioned listening to Medical Apartheid on audiobook; I was listening to this section during a run, and as someone who spends a considerable amount of my time fighting misinformation, was literally whooping and fist pumping throughout the story of how Dr. McCune Smith and Dr. Jarvis systematically dismantled the failed assumptions and overt racist methods of census takers, who had relied on the reports of plantation owners and slavers to collect data on the health of their slaves, and in many Northern cities reported several times more free “negro lunatics and idiots” (medical vernacular of the time) than the actual total free Black population of those towns. If someone had seen me on my run, they would think I was listening to my favorite team winning a big match; and in a way I was, though in this case even the thorough work of these two brilliant scientists was not enough to erase the damage done by the 1840 census, and chattel slavery continued for another 25 years and only ended with the conclusion of the Civil War.
Or we could look at the display of Black bodies- both living and dead- for popular curiosity and scientific study throughout the 1700’s and 1800’s that she outlines in Chapter 3: Circus AfricanusandChapter 5: The Restless Dead. Or radiation experiments conducted without informed consent on Black Americans throughout the early to mid 1900’s, which she outlines in Chapter 9: Nuclear Winter. Or at Chapter 11: The Children’s Crusade, where she reviews the research conducted throughout the 1990’s attempting to link criminality to genetics and hence to Blackness; research conducted on children and under extremely questionable scientific methodologythat strived to prove Black Americans were genetically predisposed towards all manner of violence and anti-social behavior.
But instead of a doomed effort to recreate the progression of Ms. Washington’s meticulously researched review of medical research abuse of Black Americans from the dedication to the epilogue, I want to strongly encourage you to buy a copy and read it or listen to it. Below I share the section and chapter titles, but you have to read it for yourself to discover how richly and clearly she explains the long, relentless violence of medical research towards our Black neighbors, friends, and loved ones.
Introduction: The American Janus of Medicine and Race
Part 1: A Troubling Tradition Chapter 1 Southern Discomfort: Medical Exploitation on the Plantation Chapter 2 Profitable Wonders: Antebellum Medical Experimentation with Slaves and Freedmen Chapter 3 Circus Africanus: the Popular Display of Black Bodies Chapter 4 The Surgical Theater: Black bodies in the Antebellum Clinic Chapter 5 The Restless Dead: Anatomical Dissection and Display Chapter 6 Diagnosis: Freedom: The Civil War, Emancipation, and Fin de Siècle Medical Research Chapter 7 “A Notoriously Syphilis-Soaked Race”: What Really Happened at Tuskegee?
Part 2: The Usual Subjects Chapter 8 The Black Stork: The Eugenic Control of African American Reproduction Chapter 9 Nuclear Winter: Radiation Experiments on African Americans Chapter 10 Caged Subjects: Research on Black Prisoners Chapter 11 The Children’s Crusade: Research Targets Young African Americans
Part 3: Race, Technology, and Medicine Chapter 12 Genetic Perdition: the Rise of Molecular Bias Chapter 13 Infection and Inequity: Illness as Crime Chapter 14 The Machine Age: African American Martyrs to Surgical Technology Chapter 15 Aberrant Wars: American Bioterrorism Targets Blacks
Epilogue: Medical Research with Blacks Today.
Though full agreement might be impossible until you have read the book for yourself, it is at least clear to me that the history of medicine in the United States, and particularly of medical research, is sufficient reason for Black Americans to have increased wariness of anything in medicine that is seen as experimental or unproven. But a natural objection presents itself; “But TJ,most Black Americans haven’t read Harriet Washington’s Medical Apartheid, so that history can’t possibly be the cause of their unease or suspicion.“
Reasonable enough on the surface, this objection fails to recognize the fact that Black Americans, generation after generation, have experienced medical apartheid, whether they have read Ms. Washington’s seminal work or not. Most American’s have at least heard of the Tuskegee Syphilis Study*, and in a hundred news articles talking about African American hesitancy towards the COVID-19 vaccines you will read phrases like “the legacy of Tuskegee” or “almost 50 years since the Tuskegee study.”
This was from today.
But for Black Americans that notorious series of events is not a one-off episode or anomaly in an otherwise untarnished history of medical altruism and benevolence, but part of a shared cultural narrative of the potential dangers of trusting too readily in scientists, researchers, and lamentably, doctors. Harriet Washington says it better than I can:
It is a mistake to attribute African Americans’ medical reluctance to simple fear generated by the Tuskegee Syphilis Study, because this study is not an aberration that single-handedly transformed African American perceptions of the health-care system. The study is part of a pattern of experimental abuse, and many African Americans understand it as such, because a rich oral tradition has sustained remembrances of pain, abuse, and humiliation at the hands of physicians. We should remember that, as Vanessa Northington Gamble, M.D., director of Tuskegee University’s National Center for Bioethics in Research and Health Care, averred, “many African Americans fear and distrust Western medicine who have never heard of Tuskegee.”
So yes, that ‘25%’ statistic is incredibly disheartening, but it’s also understandable once we know something of the historical context of the relationship between modern medicine and people of color. And while these new vaccines are notexperimental and fears of being a “guinea pig” by taking the vaccine really are unwarranted for anyone, those concerns are common among many people of all racial and ethnic backgrounds in our current climate of mistrust and disinformation; and it is not a mystery that those fears might be stronger among Black Americans, with the weight of 400 years of medical and research abuse behind them.
*A note on Tuskegee I would be remiss if I didn’t at least touch on a the basics of the Tuskegee Syphilis study, though Medical Apartheid does a much better job than I can. This was a study that was run by the US Public Health Service in Macon County, Alabama from 1932 to 1972. The full title of the study was “The Tuskegee Study of Untreated Syphilis in the Negro Male“, and as awful as that sounds it’s probably even worse than what you’ve heard. The public health service initially recruited 600 Black men from among poor sharecroppers in an impoverished county in Alabama; they chose 400 with evidence of latent syphilis and 200 without syphilis as a control group. There were some treatments for syphilis available in 1932 when the study began, but none of them were particularly effective; nevertheless, not even these were offered to the men in the study at any point, even though they were given dummy pills and told they were being cured. The intention was never to cure them, but to carefully observe and document the progression of the disease from its early stages all the way until death, and then conduct post-mortem examinations to see which organs and body systems had been deranged or destroyed by the unchecked bacteria. Of course, this was not only done without consent, but through active and ongoing deception of those involved in the study.
It gets worse. Alexander Fleming discovered Penicillin in 1928, just 4 years before the Tuskegee experiment began; but it wasn’t used clinically until the 1930’s and early 1940’s. It became standard of care for all manner of bacterial infections by the mid 1940’s, and by 1947- 15 years into the 40 year Tuskegee study- was both widely available and a known cure for syphilis. Not a treatment; a cure. The researchers and even the administrators over the Public Health Service met to discuss whether the research project should end and all of the participants be offered Penicillin. Appallingly, they decided that, no, the study would continue. Their reasoning? Now that a cure for the disease had been discovered, this was the only chance to find out what the long-term affects would be if it was left untreated. Please… Stop and process that reasoning for a moment.
The study continued for another 25 years. Participants became wise to the fact that syphilis was now being treated elsewhere with a simple injection instead of countless check-up visits, seemingly ineffective medications, and steady progression of the disease. Many of the men sought treatment elsewhere at other Public Health Service clinics, one of the few places they could receive affordable care; only to find that their names and information had been sent ahead of them. Those in charge of the study had sent a list throughout the Public Health Service network: these men were part of a PHS study; they should not receive treatment for syphilis outside of the study. I hope I do not have to pause here and explain how antithetical this study was to every ethical principle in medicine, every moral imperative towards our fellow human beings. Participants were tricked and lied to, denied effective, curative medication, and then when they discovered the grift and sought care elsewhere they found that steps had already been taken to block their treatment there as well. Some did manage to get treated, by seeking care in other clinics or providing assumed names in order to get the penicillin; but most had already suffered the devastating neurologic effects of late syphilis… Just as the study designers had intended. The study finally ended in 1972 when news of it was leaked by the media (you know, that mainstream media you just can’t trust…); it was popular outrage that finally shut it down, not any moral or ethical consideration by the Public Health Service or the individual researchers, scientists, or doctors that were involved.
That,in a nutshell, is the history of the Tuskegee Syphilis Study. Medical Apartheid’s seventh chapter, “A Notoriously Syphilis-Soaked Race”: What really happened at Tuskegee does it more justice, and by itself is worth the price of the book. That history is more or less known, especially among Black Americans; and even were it just that, wouldn’t it be enough?
The Other Problem: The Unequal Burden of COVID-19
A recent viral video of Dr. Simone Gold, one of the founders of the COVID-19 disinformation group “America’s Frontline Doctors,” featured a long segment where she accuses the CDC of overt racism for stating explicitly that they both aim to make COVID-19 vaccines widely available in communities of color, and for listing strategies to increase acceptance rates and combat vaccine hesitancy in those communities, including recruiting celebrities and other influential people to encourage vaccination.
On the surface, her claims actually sound fairly reasonable; given the history above, any efforts for medical treatments to target specific racial demographics, and especially a historically (and concurrently) oppressed group, has to be carefully scrutinized. Erroneously believing that vaccines are poison, and that these COVID-19 vaccines are “experimental”, Dr. Gold (had she read Medical Apartheid) would make the claim that the CDC’s efforts today are just the latest in the long sequence of medical research efforts that, intentionally or not, resulted in the exploitation, humiliation, and harm of Black Americans.
And she would be wrong.
The key difference, as Harriet Washington herself points out over and over again throughout her work, is that these efforts by the CDC are therapeutic, not experimental. Dr. Gold’s claims about the experimental nature of the vaccines is demonstrably incorrect (see my most recent blog post), as she herself is well aware. Calling them “experimental” or unproven, or referring to vaccine recipients as ‘guinea pigs’, is merely a scare tactic; and one that could be particularly effective when targeted at groups who already have legitimate grievances against American medical research. It goes without saying, but Dr. Gold is also wrong about the vaccines being dangerous; the safety trials were extensive and rigorous, and the protection offered by the vaccines against a horribly deadly virus is excellent. Rather than being a malevolent attempt to test the vaccines on Black people to make sure they are safe for whites, as was the case with Dr. J. Marion Sims’ surgical procedures in the 1800’s and the radiation trials in the 1990’s, this is an altruistic attempt to ensure that Black Americans have equal access to a treatment that has already been proven safe and effective. Finally, in contrast to those experiments, the efforts to address vaccine hesitancy and combat misinformation within Black communities are being done with not only buy-in, but active leadership by Black physicians, scientists, researchers, and public health experts. This is certainly the case on the national level, where organizations like BCAC19 are working with government and healthcare organizations across the country. But it is also being done on the local level in many places. My own clinic has a list of resources similar to the one in this blog that I often provide to Black patients in the context of a conversation about the COVID-19 vaccines and America’s history of racist medical research abuse. It was created specifically at the behest and encouragement of one of our African American physicians, and vetted by a work group dedicated to race health equity.
Treatment, not experimentation. Beneficence, not malevolence. Black leadership, not subjugation.
The effort to help Black Americans get vaccinated against COVID-19 is the polaropposite of the very real history of medical research exploitation Dr. Gold wishes to link it to.
But why is it necessary at all? Because despite what Dr. Gold implies in her video by factoring out the health outcomes associated with our long history of racial discrimination, healthcare inequality is a very real factor in America today. And if you need proof, look no further than the data around COVID-19.
Black and Hispanic Americans are far more likely to die of COVID-19 than their white counterparts, and the gap only widens when you factor for age. This is because non-white Americans have consistently faced discrimination and unequal access in healthcare, both individually but especially systemically, and this has resulted in a greater burden of disease for many illnesses and conditions that are independent risk factors for a bad outcome from COVID-19 infection.
Compared to whites, Black Americans are twice as likely to be uninsured. They are more likely to die from cancer despite many of those cancers occurring at higher rates in other groups. The rate of infant mortality is 11 for every 1,000 live births, compared to the national average of 5.8 for every 1,000 live births, and Black mothers are 2-3 times more likely to die from pregnancy-related complications than white mothers. Black men have the lowest rates of survival 5-years after receiving a diagnosis of heart failure. Black men and women are less likely to receive cancer screening and preventative health services. And Black Americans are less likely to have a primary care doctor or clinical home and get their care piecemeal in the emergency room setting, and not surprisingly, consistently report higher levels of distrust in doctors and healthcare.
Dr. Gold and others wish to ignore these factors, to make it seem that there is no need for efforts to ensure the vaccine gets to Black communities. After all, if such efforts are not desperately necessary, they must just be inherently racist. It’s a clever enough ploy, but look at all the history that has to be white-washed in order to eliminate the unequal burden of COVID-19 on Black Americans.
Dr. Gold and others say the difference in death rates between races decreases if you adjust for socioeconomic status and poverty. Manipulating the statistics in this way erases 246 years of chattel slavery, 89 years of Jim Crow, and 67 years of unequal wages, discriminatory hiring practices, and unequal higher education access.
Dr. Gold and others say the difference in death rates between races decreases if you adjust for conditions that increase transmission; crowded neighborhoods, multi-family buildings, use of public transportation, and cramped living conditions. Manipulating the statistics in this way erases 247 years of Black American not being allowed to own property, 67 years of over legal housing discrimination, 35 years of redlining, and 53 years of ongoing housing discrimination even after the Fair Housing Act.
Dr. Gold and others say the difference in death rates between races decreases if you adjust for chronic medical conditions. Manipulating the statistics in this way erasestheover 400 years of medical exploitation and ongoing healthcare disparities we’ve already discussed.
We could go on. It’s well and good to say that, all things being equal, the COVID-19 virus doesn’t seem to have any race-based predisposition to harm people of color more than whites. But all things are not equal. Our longterm investment in the destruction of Black Americans’ health is now paying compound dividends, as our seemingly impenetrable barriers to access and long neglect of Black healthcare needs places Black communities in a position of heightened vulnerability to devastation by the COVID-19 pandemic, and our sinister history of medical research abuse rightfully increases the wariness many already feel about the new vaccines, our best protection against it. Those who deliberately spread COVID-19 vaccine disinformation are banking on this dynamic increasing acceptance of their false and fantastic claims, and there is something particularly evil about using the lasting wounds of centuries of medical victimization, neglect, and exploitation of Black Americans to further victimize them by damaging their access (medical misinformation is a healthcare access issue) to the best life-saving interventions we currently have available.
My Conversations with Black Patients
So this is the double-edged sword facing our Black friends, neighbors, and loved ones, and my Black patients; on the one side, ongoing disparities that put them at greater risk from the virus, and on the other a history that legitimately causes mistrust in the best tools we have to fight it. Each and every day in my clinic I am talking with Black patients who are aware of Tuskegee, who are aware of Henrietta Lacks, who are aware that these cases are not isolated incidents, and who are seeing all of the same anti-vaccine propaganda and fear-mongering that you and I are on social media.
Many are not at all fooled. They have been navigating this dynamic their entire lives and are used to making these sorts of difficult decisions. They are well aware of the threat COVID-19 poses to themselves and their loved ones. Many of my Black patients at highest risk- healthcare workers, those who are older or have medical complications- have already been vaccinated through our clinic. We are working daily (a physician friend of mine is working literally day and night) to create vaccine access for still more. Often my patients bring it up without me even asking; “Dr. Webb, when do you think the clinic will have the vaccine available?” Others, when I ask, are excited to be scheduled, or added to our call list for when more doses do come in.
For others (and certainly not just among my Black patients), hesitancy about the vaccines is indeed a factor, and I have been intentional about carving out time in the midst of busy clinic days to have these conversations.
For me, the first step in any conversation about vaccine or treatment hesitancy is acknowledgment, and this is particularly true when speaking with my Black patients. Though I was becoming aware of this area of our medical history for a long time, I was hesitant to discuss it openly, fearing it would come off as insincere or virtue signaling; until one day it just burst out.
I was in the COVID-19 outdoor clinic and discussing a patient’s cough and cold symptoms. My patient, an African American woman, was hesitant to get a nasal swab to test for COVID-19 despite having very classic symptoms (though thankfully her test ended up being negative). When asked about her concerns, she said something I had heard from hundreds of patients of every race, age, gender, and background; “I just have a hard time trusting doctors” (I should mention here that the fact I, a doctor, had heard it hundreds of times points to how widespread this problem is; how many thousands of patients felt that exact way but didn’t feel like they could say it to me?). Normally I would respond by saying “I understand” or “I think a lot of people feel that way, let’s talk about it”; measured and time-honored responses that preempt any defensiveness I might feel and allow the conversation to keep moving forward. But that morning I had gone for a run before clinic and listened to Medical Apartheid for about a half hour, and without thinking whether it was wise, instead I burst out with, “Well how could you as a Black woman, when there’s been so much research abuse by the medical field?!” Before I even had time to consider whether I had just stuck my foot directly in my mouth, she grabbed my arm and said “Yes! Exactly!”
Without adopting it as a stratagem, since then I’ve felt much more free to discuss that history with my Black patients (and not just in the context of the COVID-19 vaccines), who of course already know it but might not think I know it- or am willing to admit it- as a white doctor. And I’ve been disappointed, thought not surprised, at how many times my Black patients have told me it’s the first time they’ve heard a doctor even acknowledge Tuskegee, much less all the rest; historical groundwork that has shaped a huge part of their paradigm for interacting with modern medicine, and their doctors, including me, have never even mentioned it or recognized that it exists. When we confess that history we are working to rebuild trust, and we sincerely signal our intent to do the difficult work, individually and as a field, to correct the abuses of the past and present and ensure they never happen again.
Next, I will often share my personal experience of being vaccinated (and that of my wife, a nurse) with my patients. I received my first dose of the Moderna vaccine on Christmas Eve, and my second just last week. As a healthy, 35 year old man with no major risk factors, even my privileged access to the vaccine is understandably controversial, and there is a strong argument to be made for my doses going to someone who needed them more. I wrestled with this for days before getting vaccinated. Ultimately, I decided I needed the vaccine because as a primary care doctor it is vital that I can look my patients in the eye and tell them I would never recommend that you accept a medical intervention, vaccine, or medicine I wouldn’t takemyselfor advise for my own family.
This is absolutely true, though it isn’t always possible; so far I haven’t needed my appendix removed or required anti-seizure medications or chemotherapy, yet of course I would recommend those for patients who need them. But it is true about the vaccines, and vitally important in the context of our climate of medical disinformation. But with my Black patients in particular there is an additional layer of significance; to the extent that these vaccines are seen as “unproven” (they are not unproven, just commonly understood as such: safety trials involved 10 times the number of participants than normal vaccine safety trials!), it was important for me as a white doctor to show my patients that I am willing to go first on their behalf, when historically it has been Black Americans that have been tricked or forced into going first in order to protect people who look like me. As Harriet Washington says, it is only since Western Physicians and researchers have abandoned the tradition of subjecting themselves to potential harms before they were willing to subject others that research abuse has become so common.
Then I will spend some time, if the patient has specific concerns, answering questions about the COVID-19 vaccines and helping them see through the misinformation around them. The same legitimate misunderstandings and unanswered questions, wild speculations, deliberate lies and mischaracterizations, and outlandish conspiracy theories that I see every day and try to combat on my blog (see my slowly expanding COVID-19 Vaccine Questions & Answers and more importantly the list of resources there) are being sent to my patients, regardless of their skin color or background. We talk about those myths and I try to use this area of semi-expertise to benefit their decision making as well as I can. I often share a two page handout on the most common COVID vaccine myths, that goes into far less excruciating detail than I do on the blog, knowing my patients can ask me for clarification if they want more information. We also talk about the efficacy of the COVID-19 vaccines, the dangers of the virus, and my firm belief that this is our best path forward out of this pandemic.
Finally, I point my patients towards exactly the same types of resources I shared at the beginning of this article; but here is where my relationship with the patient is a key factor. I have been practicing for 5 years now since completing my residency and have many patients, including many Black patients, who trust me as their primary care physician more than they trust any other individual who could speak into their medical decisions or their healthcare fears or anxieties. Though I will still point them towards the incredible resources that come from my Black colleagues, it is to support the work of trust-building that we have already been doing within our patient-doctor relationship for years. Those resources are influential and reassuring, but my word is also valuable to them specifically because they have seen me work diligently on their behalf and engage with them in a partnership to further their healthcare goals and protect their dignity and autonomy.
Other patients I don’t have that kind of relationship with yet. Either we’ve only had a few visits together or I am seeing them in a context outside of their usual clinic; our COVID-19 outdoor clinic or covering for their normal doctor. In those settings we still work to build trust, but I have to be humble and realistic about how much this can be accomplished in 15 minutes (though you’d be surprised). When I and a Black patient I barely know talk about the COVID-19 vaccines, I explicitly state the fact that we are probably both thinking: that I can’t as a white doctor tell them ‘you should get vaccinated’ and expect to be believed by default, or feel entitled to be believed, by virtue of my title or position, my medical education, or my presumed expertise. And though I hope that through our conversation about the history above and just as importantly through sincerely listening to their concerns and working hard to care for their medical needs I will have built some degree of confidence and trust in my recommendations, nevertheless it is in those situations that I have to lean most heavily on the outstanding work that my Black physician and scientist brothers and sisters have already done in dispelling the COVID-19 vaccine myths and empowering fellow Black Americans to make the best and most informed, empowered choices about getting vaccinated. At the end of those conversations, like the beginning of this blog post, my most important role is getting the resources that have already been created by those Black leaders, without any input from me whatsoever, into the hands of people who share with them a history of medical abuse and subjugation but are striving to claim ownership of their health narratives and use every good tool and resource available to defeat this pandemic and end its inequitable impact on Black Americans.
The video below is going viral right now, spread mostly by private text and social media messages. I’ve had it sent to me by several people in the last week, both doctors who were frustrated with the obvious untruths but too busy (with the pandemic) to formulate a response, and bdiy people with less scientific training who knew the information didn’t sound right but didn’t quite know why.
The talk is from The Stand, a mass faith healing and miracle event put on by known religious hucksters in Florida. False Teachers and theological misinformation are another passion of mine and have been for much longer, ever since I attended a Benny Hinn crusade for a Sociology course. But even though there’s also a pandemic of heresy in the United States right now, it’s the medical aspects of Dr. Gold’s talk at The Stand on January 3rd that we are focused on today.
For an introduction to Dr. Gold and her organization I would encourage you to glance at the response I wrote to their most popular video, a press conference they gave at Capitol Hill back in July. This was the video where Dr. Stella Immanuel from Houston spoke about hydroxychloroquine.
This group has been speaking and writing about COVID-19 since at least May, when they wrote a letter comparing the COVID-19 pandemic to a Mass Casualty Event, where presumably the 437,000 Americans who have died from the pandemic so far would be in the “black” category of mass casualty triage; not worth trying to save. The group also includes Dr. Dan Erickson, the California urgent care doctor who spoke out about how the virus is not-dangerous and how most of California had already had it… Back in April. To Dr. Erickson’s credit, his later statements have been much more measured, and based on his sincerity in the original press conference I actually wouldn’t be surprised if he at some point quietly recants his analysis, which was founded on extremely flawed epidemiological assumptions. To date, there have been 40,192COVID-19 deaths in California.
Finally, you may have read about Dr. Gold’s recent arrest for her involvement in the attack on the US Capitol, which occurred just 3 days after her appearance at The Stand, during which she gave a brief speech again condemning the vaccines and encouraging people to get ahold of hydroxychloroquine. Dr. Gold has since stated that she regrets being involved in that event. My sincere hope for Dr. Gold is that this series of events will force her to consider not just that particular action, but also her stance on the pandemic over the past year as a whole, and to reexamine the evidence, reflect on the harm that has been done by medical misinformation and the people who have died as the result of attending to it, and maybe even become a leading voice for reform from withinthe COVID-19-denial movement. Dr. Gold is sincere, funny, and winsome as a public speaker; it would be the greatest thing in the world if after this she chose to use her platform to help people take the pandemic seriously and love their neighbors by following common sense, effective transmission control measures.
She, in this case.
Layout of this post
This is a very long post and I don’t expect everyone to read it all the way through. I’ve divided it up into a minute-by-minute breakdown with time stamps for easy reference. If there’s a section of the video you want to read a counterargument or clarification for, just look at the time on the video and scroll to that part of the post.
I’ve also separated it into large sections which I’ve hyperlinked below in the “contents” section. Though Dr. Gold jumps around a bit (that’s not a criticism, I jump around way more when I speak in public), it is possible to separate her talk into some big chunks, so that if you are really only interested in particular topics from her video you don’t have to watch the whole video or read the whole post.
Finally, I’ve included the video itself in my blog post. Just as we have to fight the COVID-19 pandemic on an individual level by providing excellent patient care to those affected and on a population level by encouraging transmission control measures like masking and social distancing, misinformation can be fought in two ways; containing the spread by taking down harmful and misleading content, and by engaging with that content and providing thorough analysis. I have mixed feelings about the first method, and as a primary care engaging directly has been the focus of all of my training and my life’s work. So if Dr. Simones Gold’s video gets taken down on other platforms, it will be up here; and all I ask is that if you are going to watch the video on my blog you’ll also read the blog. Not doing so is tantamount to admitting you are only willing to consider one side of these arguments, and I’m betting that’s not consistent with how you see yourself; all of us want to be fair and reasonable in our judgements.
1 Thing I’m going to do and 1 Thing I’m not going to do
First, I am goingtotry to be very fair to Dr. Gold in this analysis. I know that Dr. Gold has a lot to gain from her minority position on COVID-19 issues (becoming the niche go-to medical expert for millions of people who want to believe what you are telling them can be very profitable), but also a lot to lose, which she touches on in the video. Yes, it’s almost a certainty that we will see a book or another political bid from Dr. Gold in the future, and someone whose videos have been shared tens of millions of times and who has successfully sold medication from her website before being forced to stop might sound a bit hollow when complaining about what a risk she is taking by “speaking out”. But the truth is that there isrisk. She has been arrested, albeit for her involvement in an attack on the US Capitol and not for anything she has said about COVID-19, and considering everything she has said and written over the past year I’ll honestly be surprised if she keeps her medical license, and I could honestly argue either way as to whether or not that’s actually fair. A doctor friend and I have often morbidly joked that if we didn’t care about morality or medical ethics, we could make lots of money as MD’s; we’ve all seen people do it, endorsing some expensive supplement or offering unproven treatments at exorbitant prices. But I donot believe that Dr. Gold has simply conducted a market analysis and decided there is more money in spreading COVID-19 misinformation than in quietly working as an ED doc, treating disease and alleviating suffering. She must earnestly believe at least some portion of what she has said in this video and has been saying since early in the pandemic, or she would not take the risks; and that is a sympathetic position. I disagree with her on many points, I think it’s pretty clear that she is wrong and why, and that as a physician I think she ought to know better; but I believe she is sincere in a certain way, and wish rather that she could see the truth than that she would simply stop spreading falsehood.
So I’m going to try to be fair. When I perceive that Dr. Gold is speaking from a sincerely held belief I’m going to say so, and when I can’t tell I’m going to assume that she is. We will look at why, in her personal experience and clinical practice, she might be justified in believing some of those things (though as a doctor she has as much access as any of the rest of us to high quality information to put her limited personal observations into a broader context). But there are also times in this video that it is clear she is either lying, engaging in shameless hyperbole, or spreading misinformation she doesn’t believe because she thinks her audience will. Indeed, her conviction in this video seems to be that no COVID-19 myth, no matter how far out, is too ridiculous to include. She basically admits this at several points and I want to be fair and give her credit when we get there; but I’m also not going to shy away from stating that she is almost certainly lying at the times when that is clearly the case. Peoplewill die because they attend to this video, and I think being fair to her context and intentions has to cut both ways.
Second, I am not going to rehash arguments that have been made thoroughly and extensively elsewhere. I’ve written on the evidence of hydroxychloroquine’s ineffectiveness for COVID-19 (Budesonide too) more times than I can count and won’t do it again. Instead I will shamelessly link to my old posts, or better external sources, which you can read if you wish. I’m also not going to argue with every point Dr. Gold makes because she throws out almost every COVID-19 conspiracy theory and myth at some point in the course of the video, even those that have been systematically disproven over and over again. I may touch on masking and other issues very lightly and provide links, and other sections I may skip over almost entirely. This video is 1 hour long and the focus needs to be on the vaccine misinformation, which she begins sharing at about 23 minutesin; so I’m going to pass some things by. Silence does not imply agreement or ceding the point, but I’ve got a full time job and a family I really like, and don’t have 10 hours to spend debunking this video. If there’s a point she makes that you find particularly salient but that I don’t get to, please say so in the comments and I’ll see what I can do.
3 Things Dr. Gold is going to do
I usually like to only debunk/analyze as we go, but this video is so long that we will save a lot of time by touching on the 3 most common “tricks” Dr. Gold uses in her talk. I don’t mean “tricks” as in deception, though some are that; I mean these are debate tactics or rhetorical maneuvers that make her arguments more convincing to the unwary listener without really adding to the actual content of her presentation. I think if you’ll watch the video with these 3 things in mind and can see when she is doing them, you’ll find a lot of this content far less convincing than if we merely reacted to each particular instance.
1.The COVID-19 virus is dangerous or not dangerous when it suits my point. This is one we’ve seen consistently with misinformation throughout the pandemic, especially from doctors and especially when talking about unproven treatments. The very same doctors who will tell you that the virus isn’t really dangerous and you shouldn’t wear a mask or social distance will then turn around and rely on extremely small numbers of patients to prove that their intervention is the cure, assuming those patients would have had a bad outcome without it.
But you can’t have it both ways. You can’t use a high recovery rate among certain demographics as proof that preventing the virus simply isn’t necessary, and then use a patient in that demographic recovering as proof that your treatment works. You can’t say that the death rate for a 25 year old patient is “0.02%” so you shouldn’t even worry about it, as Dr. Gold states later in the video (will look at the context and impact of these numbers at that time), and then turn around and say that the 25 year old you treated not dying proves your treatment saved their life.
This is a true contradiction, but it’s explicable when you realize that the doctors who hold these contradictory views derive them from two separate thought processes. When talking about the pandemic being blown out of proportion, they are speaking from a political and economic standpoint that wishes, as we all wish, to get life back to normal as soon as possible; the evidence of the danger of the pandemic, which has now killed over 430 thousand Americans, simply cannot change that philosophical belief, no matter how overwhelming the evidence becomes. But when they are talking about their favorite treatment being ‘the cure’ for COVID-19, they are consulting extremely small samples of patients that constitute nothing like substantial anecdotal evidence, much less reliable data. Besides the fact that most of America’s Frontline Doctors are nowhere near the front line (no pay wall but you have to register for that article. Sorry), the way they have admitted to selecting their patients and “diagnosing” COVID-19 make their clinical experiences entirely unreliable. We talked about that more with Dr. Stella Immanuel’s and Dr. Ivette Lozano’s viral videos.
Watch for this as you go through Dr. Gold’s talk. In each section, is she working from the assumption that the virus isn’t really dangerous and therefore you don’t need masks or vaccines, or that the virus is universally deadly and therefore it’s vital that you have access to unproven treatments for it? Most importantly, is she working from a consistent assumption or does it fluctuate based on the point she is trying to make?
2. Everyone is lying to you but me. I know it feels really calloused to even point this out, but I’d argue it’s more calloused to actually engage in this type of argument. But Dr. Gold does this over and over again. Each time she tells you that historically truthful sources of information like the WHO or the CDC are known for dishonesty or unreliability, each time she tells you that all the doctors and scientists are ‘in on it’ or ‘have fallen for it’ or ‘have drunk the Kool-Aid’, she is saying the traditional sources you would get your health information from can’t be trusted anymore because they are either lying or have been deceived themselves. This is a transparent, mean-spirited, and petty rhetorical trick; it’s also devastatingly effective when you are the one telling people what they want to hear. “Trust me, not them” is not a good standard of evidence, but it works when someone already wants to trust you, as the people she is speaking to almost certainly do. They are comforted because it alleviates the cognitive dissonance of going against the medical experts and what you are being told by people in your own community. If you don’t know them or don’t like them they are lying; if you like them and know them, they have been duped. It gives you a position of both moral and intellectual superiority to believe that you alone are in a position of being both knowledgeable and truthful, and that is the gift Dr. Gold is giving to her audience. It is seductive.
There is also no counterargument that works against it, because if you don’t know me then you can just think that my whole rebuttal is simply lies (ouch), and if you do know me and like me you can think that I’ve been duped myself; that’s the whole point of the ‘you can’t trust anyone but me’ trap. The only way to avoid being deceived by this is to consistently think of this video in the context of your own life and not in a vacuum. You know people who have been harmed by COVID-19, even though Dr. Gold would tell you those were anomalies or they were really harmed by something else altogether. You probably knew people who died from it who weren’t going to die this year otherwise, even though she claims that’s the only people this hurts, people who would have died anyway.
Andyou know medical professionals. Dr. Gold and a handful of doctors are taking an extreme minority position and telling you that over a million other doctors are wrong or lying; that we are part of the medical establishment and being told what to do by the government, big pharma, and whoever else (by the way, I’ve literally never been told what to do by either the government or a pharmaceutical company when it comes to practicing medicine. Not once). Butyou know some of those people and you don’t know Dr. Simone Gold. Those other doctors aren’t nameless, faceless, nefarious intellectuals. They are your local Family Medicine doc or Pediatrician you go to and bring your kids to and ask for advice on medical issues ranging from the deeply concerning to the fairly mundane to the kind of embarrassing. They are the nice young resident who took care of you in the ER that time, or the grumpy specialist that nevertheless got to the bottom of your problem. And yes, they are the doctor you didn’t trust or had a bad experience with; but so Dr. Simone Gold’s allies might be. For hundreds of people in Minden, Louisiana, they are that goofy but good natured kid you taught in Sunday School and Youth Group or bought Boy Scout popcorn from for all those years. For some church members in East Texas, they are that son-in-law of the church secretary who visits with his beautiful family whenever they are in town. And for lots of random people across the country, they are that young man who stopped to help you change a tire or gave you a lift when you were hitching, or helped you pick out an over-the-counter medication when you were confused at the local pharmacy even though he absolutely shouldn’t be giving out medical advice in the middle of Wal-Mart. Maybe you don’t know TJ Webb, MD, but you probably knew people as children or as teenagers or young adults who went on to careers in science, epidemiology, and medicine. Those are the people Dr. Simone Gold says are lying to you, and you only have her word to prove it.
That is the context in which you have to think about this claim that ‘everyone is lying’; the context of the real world, where each of those ‘lying or duped’ medical professionals and scientists come from somewhere and have real-life relationships, souls, and histories. We are nota nameless, faceless, monolithic establishment; and disagreeing with Dr. Gold doesn’t make us one.
3. Calling misinformation “truth” and truth “misinformation.” This is the simplest one but also the most insidious. Dr. Gold spreads misinformation throughout this video, but she is going to claim that her talk is specifically intended to correct or debunk misinformation. This is a false equivalence; she wants to put the information she is sharing, which is believed by a tiny handful of doctors and scientists, on equal footing with the research and clinical experience of millions of scientists, physicians, nurses, epidemiologists, and researchers. Speaking from a widely debunked and extreme minority position, she wants to turn all things COVID-19 related into a ‘he said / she said’ situation and ask you to choose between the two as equally valid and scientifically supported views.
And in a way that’s ok; when presented with false information like that which Dr. Gold shares in this video, you really should decide for yourself based on the evidence. But please keep in mind what the implications are of accepting one or the other. If you decide that Dr. Gold is truthful then you are in effect saying that you agree that there is a wide-ranging conspiracy to deceive the public and cause mass suffering, which involves almost every single doctor, nurse, and scientist you know. And if you believe that, that’s fine; some people do prefer conspiracy theories, or even just want that to be true because it would mean that life could get back to normal sooner. But let’s not pretend that the real life experiences of millions of generally altruistic doctors and nurses is equivalent to the fringe view of a few overtly political physicians. At the very least, the burden of proof rests with the latter.
*WARNING* The Below Video Contains oh just tons of incorrect and misleading information.
If you are going to watch the video, please also read a counter-argument; either mine or someone else’s.
Minute By Minute Analysis
Part 1: Preliminaries, Hydroxychloroquine, and Masks
0:39 “Experimental Vaccines” Well that didn’t take long. Dr. Gold will consistently call these vaccines “experimental” because all of us are afraid of being guinea pigs in some science experiment. She is mischaracterizing them and we look at that in detail later on, but she wants you to adopt her terminology now because even the idea of the vaccines being experimental will convince some people not to get them. People will die because of this video.
1:03 America’s Frontline Doctors Dr. Gold’s organization has been spreading misinformation about the pandemic for going on a year now; here is the first instance of her claiming that they are trying to combat it. Truth is lies, lies are truth.
1:25 “Groups of physicians, scientists, and government agencies lying to the American people” This is the first instance of “everyone is lying but me”, but certainly not the last.
1:50 ‘The NIH is lying when it says that unless you are in the hospital requiring oxygen there is no treatment available‘ Dr. Gold is going to spend the next few minutes talking about hydroxychloroquine, and you can read my analysis of these claims in any of the many posts where they’ve already been addressed.
But this claim specifically is that the NIH says there is no treatment unless you are in the hospital and on oxygen. Well, here are the NIH treatment guidelines, and I’ve included their summary table below.
For patients with mild to moderate illness who are not hospitalized, there is some decent evidence of monoclonal antibody therapy and I have referred several patients for this just this past week. This is the same treatment then-President Donald Trump received when he had COVID-19. For patients in the hospital and not receiving oxygen, they recommend remdesivir for those with a high risk of disease progression. And of course, for all patients we are providing counseling on over the counter treatment, supportive care, and anticipatory guidance when they are seen, which any doctor would tell you are the mainstays of treating any illness, whether specific medications are prescribed or not.
So, 1 minute and 50 seconds in we have our first example of Dr. Gold giving a demonstrably false statement. The proof is before your eyes; the NIH treatment guidelines do not say no treatment is available unless you are in the hospital and on oxygen. Will you still give her your absolute trust for another 54 minutes?
2:20“We were promptly de-platformed” This is true; there is no denying that the America’s Frontline Doctors Capitol Hill speeches, and most famously Dr. Stella Immanuel’s hydroxychloroquine speech, were taken down from Facebook and YouTube. Again, as that video was full of dangerous misinformation, it’s hard to feel bad about it; but it certainly lends credence to their claims of censorship (by private companies and not by the government, but still) and in certain peoples’ eyes lends an air or forbidden truth to their comments.
I would much rather have the arguments understood and then analyzed. I wasn’t able to post a video of that talk but you can read the transcript and my analysis here.
2:29 “This is a crime against humanity.” Wait, YouTube taking down their video was a crime against humanity? Hmm…
I’m being facetious; she clarifies that it’s the massive disinformation campaign around COVID-19 that’s the crime against humanity. I happen to agree with her, but we fundamentally disagree about whois a part of that disinformation campaign.
2:52 “The vast majority of deaths in America would never have happened.” Uncanny, we absolutely agree again. When you look at the death rates around the world, every nation, and especially those that took the pandemic very seriously early on, has faired much better than the USA. But the key is prevention of transmission with masking, social distancing, and now vaccines; not ‘give everyone hydroxychloroquine’.
When in your life have you heard a doctor say it’s better to get a deadly disease and then treat it than to avoid getting it in the first place? We are accused of that all the time, but I’ve never actually seen it happen until now. Again, the treatment she is espousing here doesn’t actually work, but that’s beside the point. The very people who will share this video where Dr. Gold promotes unproven treatments and warns against safe vaccines will un-ironically go on to post comics like this one:
Our first day of medical school was actually just a bunch of ice breaker games and a super annoying scavenger hunt that we lost because my friend Jason kept on getting lost, but whatever.
3:09 “You need to understand the magnitude of the lie…” What Dr. Gold is doing here (besides helping fill up her hour, which can be a real challenge sometimes), is repeating to a select audience- both those at this faith healing event and those sharing her video on the internet- misinformation and conspiracy theories they already agree with. This helps solidify her position as a truth-teller and lends additional credibility to the real point of her talk, the concerns she is going to share about the vaccines later. We will go through them as quickly as possible.
3:26 “Its real name should be…” There’s no important information or misinformation here one way or the other. We do not universally name diseases after their location of origin, though it is sometimes a factor, just like the person who discovered it is sometimes a factor in naming. If anything, we are getting further and further away from eponyms in medicine, and where many people would have talked about “Hansen’s Disease” in the early 1900’s, nowadays we just say “leprosy” like they did in the Bible, except for a few test questions during second year of medical school. Naming conventions for diseases in the age of microbiology focus more on either the name of the pathogen or the syndrome that it causes.
For instance, the name of the dangerous Coronavirus disease that was first identified in Foshan China in 2002 was “SARS”; Severe Acute Respiratory Syndrome; it was never called the “Foshan” virus. In contrast, the next dangerous Coronavirus we encountered in 2012 was called “MERS”; Middle Eastern Respiratory Syndrome, based on the region it was discovered in. The name of the novel Coronavirus we are fighting tooth and nail against now is SARS-CoV-2; Severe Acute Respiratory Syndrome Corona Virus 2, because, you know, it’s the second one. The name of the syndrome is COVID-19 for Coronavirus Disease 2019, which I admit is a little bland for something that has devastated the world.
The only times the virus is called the “Wuhan Virus” (or the more overtly racist “Kung Flu”) is by those who wish to make a political statement; calling it the “Wuhan Virus” is politically or ideologically motivated, not the other way around. Here Dr. Gold is simply making a show of solidarity with those who would like to call it what former President Trump often called it; there is no important ground here, only signaling to her audience which team she is on.
3:38 “Before we discovered…” What was discovered was that it is a coronavirus similar to the one that causes SARS, not that the Chinese government didn’t like the name “Wuhan Virus.” Remember, it is called COVID-19 and SARS-CoV-2 around the world; the narrative that the US is in China’s pocket (not my field of expertise) simply does not explain the naming conventions for the pandemic.
3:55 “They called it a coronavirus because it is a coronavirus, but that became very confusing to doctors and scientists…” Nobody was confused. This whole narrative is really weird and insincere.
4:03 “We used to use coronavirus on our charts when we meant a common cold.” Look I realize I am splitting hairs here, but no. If you did a viral respiratory panel and it showed a coronavirus, sure, you would document that; but otherwise we call those colds “viral upper respiratory infection” or just “cold”, or if it is causing a more specific clinical picture, “viral bronchitis” or “viral bronchiolitis”, etc., or if we are really being lazy just “cough, sore throat, and rhinorrhea (runny nose)”.
When I started listening to this last night and Dr. Gold got to this point, my wife (a Registered Nurse) called out from the other room, “Did she just say we use ‘cold’ and ‘coronavirus’ interchangeably?!” Yes, she did. And no, we don’t.
Again, it’s a non-issue, but I was annoyed by it. Sorry, moving on…
4:59 More Hydroxychloroquine I’m really going to limit myself to a few comments on this section because I’ve already linked to my other hydroxychloroquine articles above. The biggest things that stick out here: 5:11 We don’t give any medicine out like candy. 5:18 Treatment and prevention of Malaria is a common use of chloroquine and hydroxychloroquine because they have been proven to be effective against that disease. Comparing this to using it to treat COVID-19 is like saying you don’t understand why a doctor won’t give you penicillin for your high blood pressure when they give it out all the time for strep throat. Carefully deciding which medications to prescribe for specific conditions,and then carefully discussing the risks and benefits of them with our patients, is modern medicine. Is Dr. Gold really saying that if a medicine is helpful and safe for some people and conditions it’s helpful and safe for all people and all conditions? If not, then surely she would admit that we have to follow the evidence here. 5:48 I really shouldn’t have to say this, but the key difference here is that Malaria is common in Sub-Saharan Africa and uncommon in the US. She says it herself, but the issue isn’t consumer demand but rather the ubiquitousness of the disease it treats. That said, if hydroxychloroquine really were the miracle drug for COVID-19 that Dr. Gold and others have claimed, I’d join them in calling for it to be OTC with appropriate pharmacist warnings. Sadly it isn’t. 6:43 We have not been hearing about it being unsafe for 10 months because of an organized misinformation campaign against hydroxychloroquine. Does she ever offer a credible theory as to why such a thing would happen, why doctors wouldn’t want patients to have access to this medicine if it worked? The truth is we heard about it 10 months ago as being something we were hopeful might work, and then were sad when the evidence showed it didn’t. We’ve only continued to hear about it since then because doctors like Dr. Gold continue to build conspiracy theories around it. 6:51 “You’ll be suspicious of everything that follows” And that is the point of it being included in this talk.
7:15“She was so much better” Here the virus is dangerous, which proves hydroxychloroquine is effective because this patient got better.
7:33 “My medical director called me the next day” I absolutely will not try to dissect Dr. Gold’s personal experience here and claim that either she or her medical director was in the right. For one thing, we simply don’t have enough facts, we don’t even know what point in he pandemic she is talking about; I know some very good doctors who were using hydroxychloroquine back before any major studies had been done because there was hope the evidence would show it was effective. Those doctors don’t prescribe it anymore, because they have been convinced by the evidence.
What I do want to say is that her example of the medical director coming to her seems intended as a callback to horror stories we have all heard about a hospital administrator or business consultant telling a doctor or nurse how to practice medicine, usually motivated by profits. That is wrong every time it happens, and those people deserve to get fired, fined, and in some instances, serve jail time. I’ve never had one of those situations, but I’ve been in some that came close.
But this isn’t one of those stories. My medical director is an excellent physician who has been practicing a lot longer than I have; I often go to her for professional and medical advice. If she were to offer feedback or even correction on some treatment I was providing that was not supported by evidence or seemed to be due to political motives rather than evidence-based medicine, that would be part of her job. I might not like it. I could argue my case. I could appeal to any of a number of internal resources. I could lay down the gauntlet, do it anyway, and let the chips fall where they may. But I could notaccuseher of overstepping her bounds. When she says this is against the law or an example of a ‘corporation practicing medicine for her’, she is knowingly wrong.
7:55 “You haven’t read the science the way I have, you’ll change your mind in a couple of months when you get a little wiser.” Yikes. I’d say ‘that didn’t age well’ but she just said this 2 weeks ago.
8:38 “The reason he said I shouldn’t prescribe it was because the insurance company didn’t want us to.” Nope, I don’t believe this for a moment, for 2 reasons. First, Dr. Gold is shamelessly promoting a well worn liethat pharmaceutical companies tell doctors how to practice medicine. It’s commonly believed, it crops up on tv and in movies constantly, and it’s almost an underlying assumption in many peoples’ interactions with healthcare; and it’s 0% true.
I spend countless hours each month helping my patients navigate around their insurance company’s arcane pharmaceutical rules and find the best way to afford their medicines regardless of their insurance status. I often prescribe a medication to one pharmacy, and then print the prescription and a coupon for another pharmacy in case the insurance doesn’t cover it. I pull up GoodRx.com or the Wal-Mart $5 generics list and we tally up the cost of their meds to find the cheapest price and make sure they can afford it. You know what I’ve never seen a class, a lecture, or even a powerpoint slide on and have never given a hoot about since the first day of medical school? Pharmaceutical or insurance company profits. Don’t confuse the broken system with the people who are fighting against it every day.
But the second reason is a lot more straightforward; they are in the Emergency Department, not inpatient in the hospital. The patients are filling their prescriptions at some pharmacy somewhere separate from the hospital, and the medication costs about $15 for a month supply with a coupon; the insurance company doesn’t have to pay for it if they don’t want to, and the ER docs will probably never hear about it. So any intervention or confrontation over this medicine was almost certainly because of the paucity of evidence for it working, not because of financial issues. If Dr. Gold at some point shows documentation that confirms this narrative, I’ll be shocked; I’ll also publicly recant this objection. But it seems to me that she is just retracing a well trodden but false narrative about the toxic control that pharmaceutical and insurance companies have over doctors.
9:17“My days at that particular hospital were numbered.” Listen, I can relate here; I once quit an ED job because of financial issues too. The issue? I found out that ER company was sending their patient’s bills directly instead of going through insurance, and worse, marking up the charge for physician services by about 150 to 300%. I never scheduled another shift. So even if her narrative above isn’t true, if she felt that it was I could empathize with her feeling like her career at that hospital was done.
10:22 “It got 20 million views because human beings recognize truth.” I would be very, very careful about arguing that views=truth. I’m sure there are a lot of youtube videos out there that engaged in less than perfect truth telling but do pretty well. But it’s a nice thought.
13:00 “You have to push back against tyranny.” Dr. Gold is here advocating against wearing a mask and comparing it to tyranny without offering a single scrap of evidence. The evidence that masks help prevent the spread of COVID-19 is absolutely overwhelming (it’s dated, but it was overwhelming when I first wrote about it back in June, and the evidence is only stronger now). This misinformation video and others like it will cost lives; but she is talking to a group of COVID-19 deniers and advocating for masks, or even remaining neutral, isn’t an option for her.
13:24 Not wearing a mask on behalf of others is a very strange argument.
15:00 “Whether you have COVID or you don’t have COVID you can get yourself a prescription…” That’s called a pill mill, folks.
15:38 “People just want to go back to normal lives.” Dr. Simone Gold is absolutely correct here. It’s one of the reasons this medical misinformation is so very seductive, because it speaks directly to our hopes; specifically our hope that we can finally be done with all of this. But the question isn’t whether or not we should be afraid; we shouldn’t. It’s whether our actions are kind and wise, and that in turn is based on whether our information is actually true. Every day, with every patient I test for COVID-19, I tell them not to be afraid; and then we talk about how they can protect themselves and their loved ones from this very dangerous virus.
16:21 “It actually changes nothing.” Again, this simply isn’t true. Vaccines are still our best path out of the pandemic while limiting death and suffering. If you are vaccinated, your risk of both death and long-lasting medical side effects from the virus is significantly lower. If your grandparent is vaccinated, your risk of giving them the virus and them dying from it is incredibly lower. No, a few million people having the vaccine has not yet changed the pandemic substantially for everyone; but thankfully that is the path we are on.
17:03 “According to the CDC which is not known for it’s honesty.” “Everyone is lying to you but me.” There have been multiple examples where the CDC has published confusing, conflicting, or poorly communicated information throughout this pandemic. Sometimes that was because of incompetence, other times because the best information available was just changing so rapidly. And at other times it was because high ranking officials in the Trump administration, with no medical background, were controlling what information was being put out.
If you have any specific examples where the CDC actually lied to the American people during this pandemic, please leave them in the comments. Let’s not just take Dr. Gold’s word that all of the hard working scientists, doctors, and public health workers at the CDC are liars become she’s telling us information that tickles our ears.
And by the way, if you want to see how these numbers Dr. Gold is getting ready to share compare to what the CDC has been saying for months, have a look at this graphic from as far back as October. Don’t let someone tell you’ve been lied to when you haven’t been; check the original source.
17:07 Survival Rate by Age At this point Dr. Gold spends a few minutes talking about the survival rate for COVID-19 for various age groups. Earlier when talking about hydroxychloroquine the virus was very dangerous; it was remarkable that her patient got better after taking the medication. Now the virus will become benign again except for small percentage of the population.
There are some fine points of epidemiology that we are going to have to guess at since Dr. Gold doesn’t give us complete information. For instance, we will assume she means the Infection Fatality Rate, which includes estimates of asymptomatic carriers of the virus, rather than Case Fatality Rate, which is just those who develop the COVID-19 syndrome; it’s the lower number and, for the point she is making, the best one to use. We also don’t know where she is getting her numbers from, as we will see in a minute.
Two more tricks to look out for (again, I don’t mean ‘tricks’ as in intentionally deceptive, just that these are rhetorical tools to make the data better reflect her side of the argument). First, Dr. Gold is going to give you the survival rate, not the mortality rate. This is incredibly important. When Dr. Gold tells you “95% of people over 70 survive,” you are reassured; the way that is phrased, it’s easiest to see yourself or your loved one in that 95%. If you were to say “5% of people die,” you would be sharing exactly the same information, only now it is too easy (for Dr. Gold’s purposes) to see yourself or your loved one in the 5% group that will die; you might want to take some precautions, like wearing a mask and social distancing, which in general Dr. Gold is against. Indeed, when I read survival rates like 99.5% and 95%, I get really worried; those mortality rates are just astronomical compared to any virus we normally face.
Second, Dr. Gold is grouping all ages from birth to >100 into just 4 age groups. This is going to skew the numbers quite a bit. For instance, if you are 49, your ‘survival rate’ is averaged with those who are 22; but you know (just like I do at age 35) that your resistance to illness and ability to recover from infection is not the same as a 22 year old’s. I don’t think Dr. Gold is being deceptive here; she has a one hour talk and has to make the most of it, and a nuanced discussion of these numbers would take more time. Still, I think one reason for choosing such broad age groups is because the numbers fit her narrative better when they are presented that way.
17:07 Under age 20: Survival Rate 99.997% Dr. Gold states that these numbers come from the CDC. You’ll notice she doesn’t say the same for any of the rest of the numbers, so I’m not sure if she is using the same source or different sources. But overall this agrees with the most up-to-date research on Infection Fatality Rate. One word on Infection Fatality Rate: Because you have to know how many asymptomatic cases there are (and we don’t), IFR is incredibly hard to calculate. The numbers will fluctuate some based on what method is used to estimate the asymptomatic cases. Throughout this part of the analysis I’ll present a few different studies that arrive at slightly different numbers; but that’s a good thing.Just like minor differences in the Gospels that complement each other is a proof of their authenticity, so different scientists arriving at slightly different numbers by using different techniques is a good way to know the numbers are, in general, reliable. If you had multiple scientists getting exactly the same numbers with different methods, you’d be suspicious; and you’d be right to be. Small differences are a good thing, and just one more proof that the scientific establishment isn’t pushing some big conspiracy on you.
So the Survival Rate for people under 20 is 99.997%. The US population under 20 is about 80 million, so that’s about 2,300at risk under 20, if our estimates are accurate. So far, we’ve lost about 650 Americans under age 20 to COVID-19 (the CDC uses different age groups from Dr. Gold, so we can’t compare apples to apples here), including two children under 10 years old in Fort Worth, an hour North of here, just a few days ago. Dr. Gold says “There’s nothing to talk about” in this age group, but these are not negligible numbers. Without mitigation, we stand to see four times that number of deaths, even assuming the new variants are only as dangerous as the original COVID-19 strain.
Second, you can’t group 3 year old and 9 year old children together with older teenagers. At age 18, the Survival Rate is closer to 99.992; a mortality rate three higher than that in children.
17:15 Age 20-49: Survival Rate 99.98% Accepting Dr. Gold’s numbers, this means that 25,400 Americans age 20-49 would be at risk; so far we have lost… about that many. So now we need to look closer at these numbers, since something is clearly off, and unlike for the birth-20 age range we don’t know where these numbers came from.
A detailed Meta-Analysis published in Nature in November estimates mortality rate for people age 20-24 at just under 0.01%, and for people age 40-49 at 0.1%; a ten fold difference. Clearly, it doesn’t make much sense to group 20-49 year olds together as one age category. 0.1% is a high mortality rate for a very, very contagious virus like SARS-CoV-2; it means that about 20,000 people are at risk in that age range. If we combine census data with the IFR estimates, we get these estimates of how many Americans would be at risk in this age range:
Age 20-24, IFR 0.008%, population 21.63 million
1,730 at risk
Age 25-29, IFR 0.011%, population 23.5 million
2,585 at risk
Age 30-34, IFR 0.03, population 22.43 million
6,700 at risk
Age 35-39, IFR 0.075%, population 21.73 million
16,300 at risk
Age 40-44, IFR 0.09%, population 19.92 million
17,900 at risk
Age 45-49, IFR 0.11%, population 20.4 million
22,400 at risk
Total Estimate from Dr. Gold’s Survival Rate: 25,400 at risk
Total Estimate from Meta-Analysis Infection Fatality Rate: 67,615 at risk
The mysteriously high survival rate Dr. Gold quotes when clumping together 20-49 year olds give us 25,400 Americans at risk in that age range; comparing the US population with the IFR estimates for much smaller age rangers gives us a total of 67,615 at risk 20-49 year olds. Now, we all hope that herd immunity, whether from infection or from vaccination will mean that we will never see this many deaths among this young demographic; but Dr. Gold’s incredibly low estimates of the danger of COVID-19 in this age group provide a false reassurance and bely how many lives will be saved from mitigation measures, masks, and vaccines.
We won’t get to it, but later on (at 41:40) Dr. Gold says that the only people who are dying of this are your 80 year old nursing home residents with bad hearts and other medical conditions, “It’s not your 45 year old nurse, it’s not your 35 year old police officer.” Except that sometimes it is.
17:20 Age 50-69: Survival Rate 99.5% I won’t go through the numbers for every 5-year age group again, but the further up Dr. Gold gets in these age ranges the further off the survival rates she is quoting seem to be. She quotes an infection fatality rate of 0.5% (Surival Rate 99.5%=Fatality Rate 0.5%) on average for this age range, but this is closer to the fatality rate for 55 year olds. By the time you get to 65 it’s at least 1.1% and as high as 1.4% by some estimates, which is a survival rate of 98.6%. If that sounds like a good number to you, consider the population in that age range; there are over 17 million Americans aged 65-69; that survival rate means that 240,000 of them are at risk of dying without mitigation measures.
We could do the same thing with Dr. Gold’s 95% survival rate for people over 70; that’s the survival rate for 75 year olds, not for everyone above 70. The IFR increases to as high as 15% at age 80, and continues to increase with age; that means millions of Americans are still at risk in this elder population, not to mention the hundreds of thousands who are at risk who are younger.
But even more important than all of these numbers, the fact that Dr. Gold is ignoring, which we’ve talked about over and over again on this blog, is that what makes the pandemic most dangerous for young people is its ability to overwhelm our medical infrastructure. Overwhelmed hospitals, exhausted doctors and nurses, more patients than the staff can possibly provide care for; these factors make COVID-19 extremely dangerous regardless of the Infection Fatality Rate. The COVID-19 survival rate plummets when you can’t get medical care for a severe case of the virus; but so does the survival rate of motorcycle collisions, pneumonia, diabetic ketoacidosis, gangrene, broken hips, closed head injuries, and knife wounds when you can’t get care because there are so many cases of this highly contagious virus. COVID-19 overwhelms healthcare systems and makes everything more dangerous, including itself.
17:55 “The people who die from COVID-19 are the people who are destined to die anyway.” This is simply not true. I dare Dr. Gold or anyone who believes this to look the families of those who have passed from COVID-19 in their 70’s, 60’s… or 30’s, 20’s, or teens in the eye and tell them that person was destined to die anyway.
But I know what the counterargument will be; “those people really died from something else and it just got counted as COVID-19.” We’ve addressed this in detail before when we looked at information from COVID-19 death certificates a few months ago; those deaths really are from COVID-19. But it doesn’t fit Dr. Gold’s narrative of ‘only the old who are already dying will die from COVID’, so regardless of the facts those deaths have to be discounted. I’m not willing to discount them.
Besides the data we’ve examined above that shows the non-negligible death rates in those in their 20’s, 30’s, etc., and the actual data you can go look at for yourself, which shows a steady progression with age and not a steep increase when you reach 80+, there is one more important piece of evidence that disproves Dr. Gold’s “people who die from COVID-19 would have died anyway” narrative, and it’s something called excess mortality. If most patients who died from COVID-19 would have died this year anyway, as the narrative dictates, then we would see little fluctuation from year to year, including 2020.
In fact, there’s a meme with false numbers circulating on social media that claims just that, and in fact claims that the number of deaths in the US was lower in 2020 than recent years. The popular one looks like this, but I’ve been arguing with people about these numbers for a couple of months now.
One of the reasons this is convincing for people is because, in general, we are bad at estimating. Even though the deadliest month of 2020 was December, when 2,000 to 3,000 people were dying from COVID-19 per day, this data from November 22nd seemed to convince a lot of people. That’s with 39 days (10 percent) of the year left, and the deadliest days of the pandemic (at that point) to boot. But it’s actually even worse than that; this is based on data currently reported at the time, not data that had been finalized; and it takes up to 8 weeks to finalize the death count for a particular week in the US. So really, this chart is only reflecting the total deaths from about September 27th. Lest we forget how much things changed between the end of September and the end of the year:
The real numbers are much more dire, but don’t tell us anything we didn’t expect; a lot of people predicted that the US would lose over three million people for the first time ever, as far back as October and November when number of daily cases and deaths began to rise. The real number is 3,200,000, and at least 347,341 of those deaths were from COVID-19. And remember it’s only January 31st; we’ve still got another 3-4 weeks before we’ll know the final death count for 2020.
Part 2: “Experimental Vaccines”
23:10 “You definitely shouldn’t be calling these the COVID-19 vaccines.” Dr. Gold prefers to call them “experimental biologic agents,” which honestly sounds like a term people might use for psychedelic mushrooms when they don’t want anyone to know that they are using psychedelic mushrooms. I think she’s trying to invoke Agent Orange and other biologic weapons here. But the good news is you can go ahead and call them “vaccines,” because they are vaccines.
23:17 “It is currently in it’s investigational stage.” A lot of Dr. Gold’s vaccine information is going to try to hype up fears about the vaccines being experimental, untested, or unproven. We all worry about being ‘guinea pigs’ for modern medicine, and depending on your personal experiences, your race or ethnicity, or other personal characteristics those concerns may be very historically grounded. Thankfully, these vaccines are not experimental; not by a long shot. The vaccines have been through rigorous safety trials that were much, much larger than normal. Most trials for new vaccines have between 3,000 and 6,000 participants; these vaccine trials had 40,000 to 60,000. More to the point, about 30 million people have already been vaccinated in the US alone, including the author of this blog. In a minute when Dr. Gold says “I don’t want to be the first person to take new things…” Well, I’ve got great news for her!
If you get vaccinated against COVID-19 today, you are not in any way a part of an experiment.
23:50 “The first problem is that this brand new technology.” This is an idea that people find particularly appealing because there is such a large kernel of truth in it. These COVID-19 vaccines are the very first vaccines to be made with mRNA (Messenger RNA) technology. That’s actually really, really exciting stuff, but the big question on everyone’s mind is, “how can we trust something so new?” Or to ask it a different way, “how could we trust a vaccine that was developed in just 9 months?
And to that I typically respond that they weren’t developed in 9 months… they were developed in 1 month.
Wait! That’s a good thing! I know that when they make all the pandemic movies about 2020, inevitably there is going to be a scene like this: All of the scientists are laying around their office in the early hours of the morning after another fruitless night of brainstorming and science experiments, surrounded by empty bags of ‘brain food’ like Red Vines and Doritos (or whatever companies pay them for product placement) and inexplicably still wearing their lab coats, when suddenly one of then sits up and says, “Wait, what if we used MESSENGER RNA TO PROGRAM THE CELLS TO BUILD COVID-19 ANTIGENS?!” Everyone sits up and says “That’s it!”, cue the Science Montage. But the truth is that the mRNA technology has been in development since the 1990’s (read this cool article about it from Stat), and was almost ready for use in vaccines when the pandemic hit.
The vaccine companies received the full genetic sequence of the SARS-CoV-2 virus in January; the first vaccine trial participants got their first doses in March, just 63 days later. The whole rest of the time from then until now was spent in clinical trials to make sure the vaccine was safe and effective.
So when Dr. Gold says this is brand new technology she is trying to scare you; but the real story is, this is brand new technology! Yay! This is the culmination of 30 years of research into how to make better, more effective vaccines… And we have access to it!
24:28 “There’s been a tremendous failure of previous Coronavirus vaccines.” Again, this is true. You can read a lengthy but really detailed article about the state of SARS and MERS vaccines here; it even touches on the problem of Antibody-Dependent Enhancement that Dr. Gold will get to in a few moments. But there are two salient points that Dr. Gold is missing.
First, the SARS coronavirus has been around since 2002 and has killed 774 people, total. The MERS coronavirus has been around since 2012 and has killed 858 people, total. COVID-19 has been around since late 2019 and has killed 2,220,000 people. Please tell me, if you were in charge of strategically allocating resources, funds, and manpower toward vaccine research, which coronavirus would you focus on? The new vaccines are possible because for the past year the collective will of the world has been focused on overcoming the challenges in making successful coronavirus vaccines.
But second, notice what Dr. Gold just said.At 23:53 she said “mRNA technology has never ever been used before for vaccines,” and at 24:28, just 35 seconds later, she said “There’s been a tremendous failure of previous Coronavirus vaccines.” Previous failures… New technology… Didn’t Dr. Gold just give us hope that this time things will be different? I would have phrased it this way: “Unfortunately we’ve never been successful at making effective vaccines against Coronaviruses. Luckily, the new vaccine- making technology they’ve been working on for 30 years is finally ready!”
24:53 “You may have heard it called the ‘novel coronavirus’, and I never understood that. This coronavirus is 78% identical SARS-CoV-1.” I mean, it depends on which proteins of the virus you are talking about. The genetic similarity ranges from 76% to 95-100% depending on which proteins we are talking about. I’m just… Not sure why that matters? It’s a coronavirus, so it’s going to be genetically similar to other coronaviruses. What makes it novel is the fact that it causes a novel disease, COVID-19, which has caused the worst pandemic that the world has seen since The Spanish Flu. You are 99.9% similar to the person sitting next to you, but when your friend shows you their new baby you don’t say, “whatever I’ve seen one before.”
25:16 “We’ve never been able to overcome the hurdles to making a vaccine against a Coronavirus.” Until now! Yay! The vaccines are 95% effective.
Me cheering them on, since I definitely don’t know how to make vaccines.
25:25 “There’s no independently published animal studies.” Besides the fact that this technology has been studied on animals for 30 years now, this just isn’t the way we conduct clinical trials. Maybe Dr. Gold is hedging here with the term “independently” and wants a particular standard of non-involvement of the vaccine designers with animal studies, but if so that’s special pleading; it’s common for vaccine manufacturers to co-author academic papers with independent labs, and both contribute different information to the paper; after all, they have to send some of the vaccine before it can be tested on the animals at the lab.
So if Dr. Gold is really just saying there needs to be data from animal studies about the safety of these new mRNA vaccines, well great news:
That was just a search for mRNA COVID-19 vaccine mice, and there’s pages and pages of it.
There is substantial, published data on animal studies both for mRNA vaccines in general and for the COVID-19 vaccines specifically. Here’s an AP Fact Check on the topic if you want to learn more.
Dr. Gold goes on to mischaracterize the status of animal studies further, at 25:45 saying “the animals often die in the end, and unless we know that we don’t know if it’s safe to give to humans.” So in 20 seconds we have gone from not having full access to the results of independently published animal studies, which isn’t true, to not knowing whether the animals died. That’s a pretty big jump. (There’s also a ‘Schrödinger’s Cat’ joke in there somewhere but the internet has too many of those as it is).
25:59 Antibody-Dependent Enhancement (ADE) Immune enhancement is a very real concerned, and one that has been hotly debated within research circles since the beginning of the pandemic, especially in regards to severe COVID-19 cases and the potential role of vaccines. Here’s an article from way back in May 2020 (what is that, like 8 years ago now?) about this exact issue. The specific proteins chosen for the mRNA vaccines were chosen carefully and specifically to avoid this problem, and moreover, this is exactly why we do animal studies and clinical trials.
The Moderna and Pfizer trials were simply huge, with ten times the number of people participating than is typical in a vaccine trial; and no evidence of Antibody-Dependent Enhancement was found. The Nerdy Girls over at Dear Pandemic have a short but great social media update on it from just a couple of weeks ago:
27:21 “Stop Medical Discrimination .Org” I had to do a double take and rewind (I’m old) the youtube video at this point, because I couldn’t believe what Dr. Gold just said. Do we have some common ground? Health equity, medical discrimination, and American medicine’s history of unequal treatment of people of color, ethnic minorities, and women is a huge issue for me, and my clinic is involved in this work every day. If Dr. Gold has a website devoted to stopping medical discrimination, I will absolutely sign-up, even if I disagree with her about pretty much everything else.
I went to the website. It’s an America’s Frontline Doctor’s Petition to stop ‘forced experimental vaccination’, which is a thing that is not happening (so I guess it worked?).
Justin, could you e-mail them about getting that logo centered over the text? Thanks.
This is pretty gross, to be honest. Discrimination in medicine is a real thing and one of the biggest obstacles both in patients receiving equitable care and in physicians building mutual trust. It is experienced every day by Black Americans, Native Americans, Hispanic and Latino Americans, people who are LGTBQ+, those who struggle with obesity, the disabled, the deaf, the blind, women… Really anybody who isn’t like me; an able-bodied, fairly young, straight white English-speaking male, which we have decided is the standard for “normal” to the great detriment of everyone else (not to mention the peril of our souls). It also applies to those who are discriminated against for work, housing, etc. because of their medical conditions. Personally I’m not ok with America’s Frontline Doctors co-opting either.
Looking ahead, we are going to talk about this later in the video as it relates to Dr. Gold’s complete misunderstanding of racial healthcare disparities (but honestly, I’m glad she’s even mentioning it, even if she gets a lot of the concepts completely backwards). My next blog post will focus heavily on the history of American medicine’s research abuse towards African Americans specifically, and the work Black scientists, physicians, and community leaders have done to ensure the vaccines are safe, and the work they are doing to ensure their communities have equal access to vaccine-mediated protection against the virus. That will be later this week, but in the meantime… You should go read Harriet Washington’s Medical Apartheid, and listen to her 6 minute NPR interview about the vaccines and the problem of how Black Americans can trust new medical technology: Race and the Roots of Vaccine Skepticism.
27:33 “Some of the other things you’ve seen in the news.” Here Dr. Gold is using “in the news” to mean “on Facebook”, but that’s fine. Kudos to her for skipping over some of these that have been disproven, though I suppose she felt she needed to mention them for anyone in her audience who had seen this misinformation already. For what it’s worth, here’s my analysis of the COVID-19 Vaccine Bell’s Palsy video that came out a few weeks ago.
28:10 – 30:04 “Has anybody heard of potential fertility problems with this vaccine?” Based on her response I assume that many hands were raised, which isn’t surprising; this has been popular misinformation for months now. I’ve written about it before and since Dr. Gold isn’t actually adding anything new, we’ll move on. The COVID-19 vaccines do not cause female infertility; please feel free to read about it on my Vaccine Q&A post linked above, or any number of fact-checking websites.
30:09 “We simply don’t know.” “Well you can’t possibly know” is the last redoubt of the lazy skeptic. No scientist would ever claim 100% certainty about what might happen, and the lazy skeptic will take that tiny element of doubt, which is really just a protection against hubris, and expand it until there is enough space for any debunked objection or pet theory they want to store there. There are multiple lines of evidence against the possibility of the new vaccines causing infertility, as I examine carefully in the above link, including many examples of women who have become pregnant after completing one or both doses of the vaccine despite being on birth control to prevent pregnancy. Moreover, there is not a plausible theoretical mechanism by which they would cause infertility. Making irrational, unproven claims and then when they are disproven saying “well we can’t know for sure!” isn’t science; it’s fear-mongering.
Part 3: COVID-19 Vaccines and Racial Healthcare Disparities
I don’t always get to watch these videos all the way through before beginning a response, and especially with the minute-by-minute format I tend to write piecemeal as we go through the video (listen, pause, think, read, think, type, repeat). After being so offended that Dr. Gold would call her anti-vaccine petition website “Stop Medical Discrimination,” I was surprised- and not necessarily unpleasantly surprised- to see her spend so much time on the issue of race and COVID-19 vaccines. In fact, with the exception of her group’s recommendations about getting vaccinated (spoiler: they prohibit or strongly discourage it for almost anyone), the rest of the video focuses on this issue. It’s 11:52 PM on Sunday night, so we won’t make it to the recommendations; if you’ve read this far and you still trust Dr. Gold’s analysis,there is nothing I can say at this point to convince you not to follow her advice; I just hope you’ll follow more reliable medical experts instead, and at least talk about it with your doctor.
I am also anxious to get to my next blog post, which coincidentally or not, is 100% about race and the COVID-19 vaccines, and specifically the question of how Black Americans could trust these vaccines in light of America’s long history of medical research abuse. The main point of that upcoming post is to share resources directly from Black scientists, physicians, researchers, and healthcare professionals; but I’m also going to be taking a look at the history of medical research abuse towards African Americans and at the current pandemic’s disproportional impact on Black communities. In that sense, while the post has nothing to do with Dr. Gold, some portions of it could be seen as a response to her comments in during this section of the video.
For now, I want to say three things to introduce that article, which I hope you’ll join me for later this week, and to conclude this minute-by-minute analysis of as much of Dr. Gold’s hour long talk as I could make it through.
First, I am very, very glad that Dr. Gold is talking about this. There are a lot of Dr. Gold’s comments I disagree with, and certain points where her analysis and conclusions are essentially backwards. But the fact that she is talking about it is a good thing. The history of medical abuse and research exploitation of Black Americans is one that is too often waved off as one or two isolated examples (Tuskegee) or ignored completely, especially by white doctors. Meanwhile, this history is part of a common experience and shared cultural narrative among Black Americans, and the disconnect between it being known by the group who has experienced it and unknown or unmentioned by the group that perpetuated it can create a tension that is absolutely deadly to the trust the doctor-patient relationship is built on. Dr. Gold is a great example here, in that she acknowledges some part of that history, and in front of a predominantly white audience.
Now, that doesn’t mean I think Dr. Gold’s talk is useful or good; her information on COVID-19 and the vaccines is all wrong, and so her interpretation of important race equity measures in vaccine distribution is interpreted as a racist attack on people of color instead of an attempt to mitigate already existing injustices. She happens to have it exactly backwards; but if she really believes everything she has said in this video, and I think she believes an awful lot of it, then it’s likely she believes her own analysis here, too. Because it isn’t accurate, the net effect of this part of her talk, were it heeded, would be to worsen the already severely inequitable impact of COVID-19 on communities of color, and obviously using that history to that end is incredibly problematic. But at the very least, talking more about that history is a good thing in itself.
Second, Dr. Gold is absolutely underselling the history of harm done to Black Americans by medical science. Dr. Gold mentions a few specific examples of vaccine reactions that were worse in African Americans, and (I actually can’t remember now if she does or not) mentions a few other examples of racially motivated medical harm. But the true history spans 400 years and is far worse than anything I ever expected, even reading and learning about a few of the most notorious examples in college and medical school. We will look into this in more detail in the upcoming post, but I strongly encourage you to read Harriet Washington’s book, Medical Apartheid.
Third, Dr. Gold is utterly confused on the concept of racial healthcare disparities. Dr. Gold spends a lot of time arguing that Black communities have not really been more severely effected by the pandemic. Of course, the pandemic is having a more severe impact on Black communities, and Hispanic/Latino communities, compared to their white neighbors, so this feels an awful lot like a magic trick; Dr. Gold is going to make the disparities disappear before our eyes. And the two methods she has chosen? First, to explain away the worse impact of COVID-19 not by race but by economic and social circumstances that place people at disadvantages in terms of health outcomes, and then controlling for all of these, to show that race disappears as a factor. And second, to point to Africa and say that ‘if the virus isn’t killing people at a higher rate in Africa, it must not affect Black people worse.’
It’s really hard to tell if Dr. Gold is in earnest here, but if she is then she really believes that whenwe say “Black Americans have been hit harder by COVID-19 than white Americans,” we are saying “COVID-19 makes you sicker if you have more melanin”; a position held by exactly zero doctors, epidemiologists, and public health experts.
When we look at the shocking statistics, like the fact that the death rate in any given age range for Black Americans is equivalent to the death rate in White Americans 10 years older, what we are really looking at is the ongoing legacy of food desserts, inequitable access to wealth, intentional destruction of Black communities, mass incarceration, redlining and planned poverty, barriers to medical access, and every other atrocity that makes up 400 years of systemic oppression.
Brookings: Race gaps in COVID-19 deaths are even bigger than they appear
Sure, let’s say for the sake of argument that if you controlled for every social determinant of health, every area in which Black Americans have experienced discrimination and continue to today, the gap in COVID-19 between Black and white Americans would completely disappear (it leaves out discrimination within healthcare, but again… for the sake of argument). Why would that matter? Does a statistical linear regression that eliminates the results of oppression actually alleviate oppression, or just make it more palatable because we can rationalize away healthcare disparities without the discomfort of actually examining root causes?
The fact that there is no genetic factor that makes COVID-19 more dangerous for Black people is exactly the point; it’s the injustices that Black Americans already experience, especially regarding healthcare access, that make the pandemic more dangerous. That is why efforts have to made to ensure Black Americans have equal access to the COVID-19 vaccines, because they are the best tool we have for mitigating the risk of the virus; and it is exactly why Black leaders like the Black Coalition Against COVID-19 are coming together to provide good, reliable information and to dispel COVID-19 myths, so that Black Americans can choose whether or not to get vaccinated with confidence, and so that they will have increased resilience against medical disinformation like Dr. Gold’s video.
I hope you’ll join me to talk more about this later on this week. In the meantime, please check-out the Black Coalition Against COVID-19 and the other resources I’ve linked to above.
When a friend sends me a video about a vaccine reaction and the next day multiple patients mention the same video to me in clinic, it’s probably time to watch it, and write about it. The video I’ve linked to below is of a registered nurse named Khalilah Mitchell who lives in Nashville Tennessee, who warns about developing Bell’s Palsy, paralysis of one side of her face, after receiving a COVID-19 vaccination. It is impossible to watch the video without empathizing with her, and I encourage you to watch it if you possibly can; I’ve supplied the link below, assuming it’s still up.
Instead of going through it minute-by-minute like we’ve done so often in the past (it is very short, at just one minute and twelve seconds), I want us to dissect a few different aspects of this.
I want to start by stating that I believe this person’s story, for reasons we will get to in a moment. I think that when we develop the disposition to refuse to believe people’s stories about themselves and their experiences we place ourselves in grave peril. This is one of the common and insidious effects of the disinformation campaigns (both medical and not) that we have seen escalated over this past year; whenever someone hear’s something that doesn’t fit into their chosen narrative, they can simply say “but how do we even know if that actually happened?” Certainly, when someone (I won’t name names) consistently proves themselves to be a source of falsehood, their word becomes worthless; but to automatically treat a stranger that way, especially a stranger who is clearly hurting, is to shut ourselves off from compassion and reason in the name of protecting our own biases.
This individual is clearly distraught and deserves our empathy. But there is a balance and a tension here, because the 340,000 people who have died from COVID-19 in the US, and the 1.8 million people who have died from it around the globe, and their families and friends and communities, alsodeserve our empathy; and so do the many more who are still at risk. We can love both, and that may mean accepting someone’s narrative about themselves and their experiences without agreeing with their scientific conclusions. And that’s ok.
And so while I believe this person’s experience, I would be remiss if we did not start with a very brief survey of what we do and don’t know to be true from this video, for the sake of encountering this sort of viral information with our eyes fully open.
We know this woman has Bell’s Palsy, or at least has visible symptoms consistent with that diagnosis.
We know she is an African American woman, a group who among all demographics in the US probably has the most reason to be cautious and skeptical towards the medical field.
She identifies herself as Khalilah Mitchell, a Registered Nurse in Nashville, TN
The Tennessee nursing board does not have any record of a registered nurse by that name.
She reports that she developed Bell’s Palsy shortly after receiving the COVID-19 vaccine.
We do not have evidence that she received the COVID-19 vaccine.
Let’s talk about that 3rd bit, which has been homed in on by multiple fact-checking sites. There are multiple reasons Khalilah Mitchell might not be listed on the Tennessee nursing board’s online records:
She may be a recent graduate or have recently received her license in that state; we don’t know how long it takes for those licenses to be searchable online.
We are in the middle of a pandemic; she may be a nurse licensed in another state who has special permission or an emergency/temporary license to do travel nursing in Nashville.
She only states in the video that she is “in Nashville Tennessee.” She may well be licensed in and work in another state while living in (or even visiting) Nashville. This is not uncommon.
She may go by Khalilah but actually have a different legal first name; Khalilah may be a middle name or a nickname.
She may be Khalilah Mitchell but be registered under a different last name because of a recent marriage, divorce, etc; changing your name on your nursing license is a beast of a process, as my wife can tell you first hand.
She may be using an assumed name or placing herself in a different city and state, or both, to protect herself from reprisals in case this video goes viral (which it has).
She may be lying.
Only one of those reasons, all of which are feasible, negates her story; only one causes us to mistrust the only unprovable/non-falsifiable aspect of her story, that she did indeed receive the COVID-19 vaccine prior to developing her symptoms.
Sadly, hiding among the many people with legitimate fears and uncertainties about healthcare in general and vaccines in particular, there are dishonest people who are not above creating misleading and blatantly false information to deceive others. If this person were a known producer of anti-vaccine propaganda, disbelieving her entire story would be warranted; but I have no reason to believe that’s true, and thus have no reason to disbelieve her story, as some have done, merely because certain aspects of it cannot be verified.
So I believe her story. However, because there have beenand will continue to be elaborate, malicious attempts to deceive the public about these COVID-19 vaccines, I believe we are justified in maintaining a healthy degree of incredulity each and every time we encounter one of these types of videos; the intellectually honest and important work of discerning whether the information presented is true in no way negates or cheapens our compassion for the speaker.
Bell’s Palsy: Medical Facts
I want to talk about the clinical side of medicine, and the human side of medicine. In reality we can never separate them, but we can compartmentalize them for a few moments for the sake of discussion.
Bell’s Palsy is a temporary paralysis of the Facial Nerve, the seventh cranial nerve which controls the muscles of the face. This paralysis occurs without warning, usually gets worse over 2-3 days, and then starts to improve after about 2 weeks. Usually it is entirely improved by 6 months and does not cause long lasting symptoms; but sometimes it does, and the extent of damage to the nerve likely plays a role in the symptoms lasting longer. The cause is unknown. It’s an area researchers have studied for years. A leading theory is that, like shingles, it is caused by a reactivation of a herpesvirus that lies dormant within your nerves. In that case it can be triggered by any compromise of the immune system, but also by physiologic stressors; it has been associated with diabetes, high blood pressure, pregnancy, acute viral infections, and vaccines, all of which tax the immune system (the latter two temporarily). Another theory says it is the immune system itself, in the act of fighting the virus, that causes ‘friendly fire’ damage to the nerve, and this would also explain why it is not just associated with herpesviruses but with other viruses like flu, hand-foot-and-mouth, common colds, and even COVID-19 infection itself. The immune system is also activated by vaccines (that’s how they work; they teach your immune system how to fight new viruses and bacteria it has never seen before), and so also have the theoretical potential to cause Bell’s Palsy, though careful studies have not supported an actual link between vaccines and this condition. But these are still just theories, and we don’t actually know. I treated a patient last week whose Bell’s Palsy, as far as we can tell, occurred seemingly at random.
So, do the COVID-19 vaccines cause Bell’s Palsy? It’s a difficult question to answer. In the vaccine trials, the rate of Bell’s Palsy was incredibly low: 4 in the Pfizer trial and 3 in the Moderna trial; 7 cases out of over 70,000 participants. That’s less than halfthe normal rate of Bell’s Palsy in the general population, which is about 35 cases per 100,000 people. The rate was higher in the vaccine group than in the placebo group, though the numbers are far too small to draw definite conclusions.
If I were to sum up the evidence for my patient or my family member, I would tell them this; getting the COVID-19 vaccine might carry a tiny increased risk of developing Bell’s Palsy compared to not getting the vaccine; but the risk is still about the same overall as it would be just going about your every day life.
Maybe that feels like a paradoxical answer, but truth is often like that. About 40,000 Americans have had Bell’s Palsy this year; very, very few of them have had the COVID-19 vaccine, but those that did may blame it on the vaccine. Those who didn’t may blame it on something else; another illness, their flu shot, stress. They may be right or they may not be, but until we understand the condition better there is simply no way to perfectly avoid it, and it is so rare and typically so benign a condition in the long run that basing our medical decision making on it is unreasonable, both as physicians and as patients (and please remember, I am both, just like every other doctor you know). If you get the COVID-19 vaccine, you are extremely unlikely to develop Bell’s Palsy; no more or less likely than you are to develop it in the coming year anyway. What you are much, much less likely to develop is a severe or fatal case of COVID-19.
Bell’s Palsy: Why I Wish She Were My Patient
Reading that last section, you may think I’m going to say “I wish she were my patient because I could help her understand that her Bell’s Palsy probably wasn’t from the COVID-19 vaccine.” Um, no. My experience has taught me that, for better or for worse, once someone has formed a firm mental association between an event or intervention and deeply distressing symptoms, that association is incredibly difficult to break; even when there is absolutely no plausible link between the two, which is not the case here. Not to digress too far, but I commonly try to break those associations in exactly two situations: first, when my patient has linked their negative experience (or that of a loved one or friend) to a medication or treatment that is actually going to be life-saving for them, or relieve a great deal of their suffering, and there is actually no causal link between them. And second, when the patient has incorrectly linked a negative medical outcome to some perceived failure of theirs. I have at least one or two conversations a month with women who have had miscarriages and have definitely assigned the blame for that tragedy to themselves for some action or omission that couldn’t have caused it; some bump they went over on the road a few days before, a drink of alcohol or a cigarette they smoked before they knew they were pregnant, getting their nails done or taking a dose of an over the counter cold medicine. We spend a long time talking about the causes of miscarriage, because if possible I want to help them let go of that shame and self-blame they’ve have been carrying, and will carry, their entire lives. Those are the circumstances where it is worth it to me to really try to convince my patient that the medical facts really do override their perceived association. With this woman in the video, if she were my patient and we developed a trusting relationship over many years, maybe at some point we would be able to have a frank and honest discussion, looking back, about whether or not that Bell’s Palsy was really caused by the COVID-19 vaccine, and help her loosen that association; but telling someone who is suffering “you are probably wrong about why you are suffering!” is not just an exercise in futility, but a failure in empathy as well.
No, the reasons I wish she were my patient are twofold; first, because I treat Bell’s Palsy all the time and there really are some things you can do to give the patient the best possible chance at recovery. There’s evidence for early steroids and anti-virals, and there are supportive care measures, like synthetic tear eye-drops, to protect from some of the potential long-term complications. We also talk about adjunctive treatments like facial massage, stretching, and facial muscle exercises that have never been proven but are not likely to do any harm either, and will help the patient feel they are an active participant in their treatment (I am always explicit about that last goal; we are not trying to ‘trick’ the patient into thinking they are helping to make them feel better). I print handouts for my patients all the time to help guide their own reading and research at home, and have one I like for Bell’s Palsy because it carefully explains the possible causes, the symptoms, and the prognosis. Medically, Bell’s Palsy is somewhat satisfying to treat because it usually does get better, and in general walking through an illness with someone as it improves is a lot less of an emotional burden for me than sitting with someone in the grief and pain of an illness that isn’t going to improve, which is vital work I wouldn’t give up, but is laden with moral injury.
And second, I wish I were her doctor because in this video she is clearly emotionally distraught. That is the aspect of this illness that the fact checking sources have seemed to ignore; the fact that this illness is incredibly distressing, even though it does have a good prognosis. I have read article after article in the few days since this video came out explaining that 1. the vaccine didn’t necessarily cause the Bell’s Palsy, and 2. it doesn’t matter because it’s a benign condition. But watch the video; it definitely matters to her. The embarrassment of having half of your face paralyzed, but people thinking you’ve had a stroke when you haven’t, of feeling self conscious everywhere you go; a condition can be benign medically but not benign psychologically, socially, or emotionally. When I visit with a patient for a condition like this, our time together is spent as much in counseling as it is in devising a medical plan. We sit in that sorrow, even as we provide hope that it will be short-lived. We offer reassurance but we know that our patients are not thinking about the low rate of long-term complications when they look in the mirror and see a face they don’t recognize. It’s hard. Maybe Khalilah Mitchell would still have been this distraught after our visit for her Bell’s Palsy, and maybe she would have felt some solace and reassurance; I can’t say. But as a physician, when I watch someone who is absolutely grieving over their medical condition, my heart goes out to them and I wish we had the opportunity to just sit down and talk about it.
These vaccines are the best hope we have of ending the pandemic compassionately, with less loss of life. I believe in them. They are safe, and your chances of developing a significant reaction- including Bell’s Palsy- is incredibly low. I absolutely disagree with Nurse Mitchell that these vaccines are “the worst thing ever”. She is very understandably thinking about her own symptoms and not about the millions of lives they will save. Yes, as a medical professional there is a tension between our own distress and the need to think of others before spreading information that can cause harm, as this video certainly will; as a Nurse, she may indeed be failing in her calling to care for the vulnerable by disseminating claims about the vaccine based only on her own negative experience and not on solid scientific facts. But that’s her rightas a patient, and the reality is that most of us will put our own anecdotal experiences above facts when push comes to shove; if this video is sincere, then she sincerely believes she is doing the right thing by trying to protect others from what she has suffered, as ungrounded in the medical realities as that concern is.
As a human being created in the Image of God, Khalilah Mitchell deserves our empathy and compassion for what she is going through first and foremost, even as we work to undo the harm this video is going to cause.
Healthcare as War on Black Bodies
There is one last, vitally important issue that comes up in this video, and if you are privileged to have a long history of the medical field treating people who look like you extremely well, as I am, it may be so subtle that you miss it entirely. Towards the end of this short video, after discussing her personal distress and her opinion that the vaccines are terrible, she closes with this heartfelt appeal,
“Please, America, They do not care about us. Do not take this vaccination.”
I will not claim to speak for her, or to make assumptions about who she includes in “they” (big pharma? medicine? doctors? She states she is a registered nurse herself, so I do not think she can mean the entire medical field), or who she includes in “us.” Certainly she addresses all Americans, but we would be naive to think that her message of “they do not care about us” would resonate equally with everyone. People who have historically experienced and currently experience inequitable medical treatment, poorer access to high quality care and lifesaving treatments, systemic discrimination, and even therapeutic, malicious medical experimentation are going to understand this video in the context of a shared cultural narrative that already teaches that you cannot trust the medical field to have your best interest at heart. This includes women, LGTBQ+ persons, the disabled, those who are obese, non-native English speakers, Hispanics, Native Americans, and at least one group Nurse Mitchell seemingly belongs to herself, African Americans. If you need evidence of this, the instagram tag on this video, @DTR360BOOKS_, is connected to an online bookstore that specializes in works about racial justice, black empowerment, and racial conciliation. If anyone, and particularly any white people, are asking why this one minute video has been shared hundreds of thousands of times on social media, read on.
Before you click over to the ‘About the Author’ page, I’ll let the cat out of the bag; I am a white, able-bodied, English speaking male (I am not neurotypical [ADHD], but I know few doctors who actually are). Healthcare justice, especially in the area of race, is something I was able to casually ignore for a long time because it simply didn’t affect me. But it affects my patients every day (and because of that it certainly makes my life harder too, though obviously to a lesser degree), and in the last few years it’s an area I’ve come to learn more and more about. Suffice to say, I absolutely do not feel adequate to the task of writing about this topic; but I am going to try anyway.
The long history of medical experimentation and abuse of African Americans, of which the notorious Tuskegee Syphilis Study is only a link in the chain, is documented in historian Harriet Washington’s book Medical Apartheid, and elsewhere. If you have time to read this long and rambling blog post you definitely have 7 minutes to listen to her explain the connection between this long history (the word “history” does not here imply that it is over, as the recent COVID-19 death of one of my Black Physician sisters tragically illustrates) and the skepticism, doubt, and fear about the COVID-19 vaccines that exist in communities of color.
Of all the wisdom she shares in this brief interview (you should really read her books), this is the one that I think is closest to our purpose:
“I think this is a good thing to do because I think this vaccine looks as if it’s going to be safe, efficacious – just what we need. So anything that’s done in terms of encouraging African Americans to benefit from it, too, I think is a good step. However, it’s not a substitute for reforming the health care system. If we don’t reform the system, if we don’t make real, large steps toward addressing the inequities that cultivate distrust, then we’re going to have to do this every time we have a new health initiative. That’s a complete waste.”
Because of the systemic healthcare discrimination and poorer access that Black Americans still suffer from today, the COVID-19 pandemic has specifically devastated those communities, causing a disproportional number of deaths and severe illnesses greater than in any racial demographic besides hispanic/latino persons, and far greater than the impact on white communities. It is not hyperbole to say that African American communities are among those that need very high rates of COVID-19 vaccination the mostto stem the tide of this pandemic and prevent further loss of life. And yet, the long history of broken trust on the part of the medical field is now paying dividends, and many in the communities that need the vaccine the most are reasonably mistrustful of a great deal of medical interventions; and especially of anything that seems new or experimental.
There are a great number of reasons to trust the safety and efficacy of the COVID-19 vaccines; they are outside the scope of this post, but I am addressing this piecemeal in my COVID-19 Vaccine Q&A. Just as Nurse Mitchel believes based on her very distressing personal experience that it is good to encourage people to avoid the vaccine, I believe based on the overwhelming scientific data that it is good to encourage my patients, friends, and family to get vaccinated. But Harriet Washington’s work was instrumental in my deciding to get the vaccine myself, which I did last week.
I am low risk, and would much rather have reserved my dose for one of my patients who needs the vaccine more than I do. I’ve written about this tension at length, and the great discomfort I have in receiving any medical treatment not available to all of my patients. But ultimately it was this quote from Medical Apartheid that made me decide to get vaccinated:
“Western physicians have adhered to a long and noble tradition of following animal studies with limited self-experimentation by researchers. This tradition may not always have been prudent, but by testing substances or procedures on themselves before experimenting with appreciable numbers of human subjects, doctors symbolically conveyed their belief that the measures were not inordinately harmful and also signaled a researcher’s willingness to share the risks as well as the glory of discovery.”
I am not a vaccine researcher, and there is no glory at all for me in people getting these vaccines. But they will protect my patients from COVID-19, and I deeply believe that as a medical field our solidarity with our patients, especially those who have been historically and actively marginalized by the medical industry, is an essential component of rebuilding trust. That means not only saying something is safe and encouraging our patients to have it done, but whenever possible taking on the potential risks within our own bodies alongside, and when necessary ahead of, our patients.
Yesterday two patients asked me about the COVID-19 vaccines and about this video specifically, both of them African American. In each case we talked about Bell’s Palsy, the vaccine safety trial data, the way vaccines work, and the history of medical abuse of Black folks in America; a condensed version of the contents of this blog post. We also talked about my experiences getting the vaccine, and my definite conviction that I would never ask my patients to consider a medical intervention I wouldn’t be willing to have done for myself or my family. Both left considering the vaccine, and at least one had definite plans to get it as soon as it was available. I am thankful, because both had risk factors for COVID-19 independent of the risk factor of belonging to a group marginalized by the healthcare sector.
This viral video is going to convince a lot of people not to get vaccinated. It shouldn’t, as we’ve discussed, but it will. My getting vaccinated will convince only a very few to get vaccinated themselves. But if I can show the band-aid on my arm to my patient and look them in the eye and tell them I believe so strongly that these vaccines can help protect our communities that I’ve had it done myself, maybe it will help a few. I can’t look you in the eye through this blog, but I hope you hear my heart, and I hope you decide to get the vaccine yourself to protect those you love and your own community, just as I’ve done.
Intro: Talking about vaccines as a Family Medicine doctor
As a Family Medicine Physician, helping patients navigate uncertainty and doubt around vaccines has been a part of my day-to-day job since long before the COVID-19 pandemic. I have always tried to approach those conversations with patience and understanding (not that I’ve succeeded each and every time), knowing that behind their questions and even suspicion there is, without exception, a deep desire to do what is best and safest for themselves and their families. I get it; vaccines can feel scary. They are pretty mysterious for most people, and there is so much controversy over them that our intuition tells us surely some of it must be true (even though the people who creating it are often intentionally deceitful). I am a father of 4 myself and understand how strange and frightening it can feel to have your child undergo any medical procedure; but unlike an infusion of antibiotics or a dose of tylenol, or the sedated lumbar spine MRI my daughter needed for tethered cord syndrome when she was 1 year old, vaccines are given to children who are healthy to prevent future illness; it makes the decision harder, because the reason for the treatment isn’t readily apparent or at the forefront of our minds.
Vaccines are also one of the single most important innovations of modern medicine, and have saved millions of adults and children from dying of some of the worst and most painful infectious diseases that afflict humanity.
That’s why it’s incredibly important to me that my patients have the time to ask their questions and why I believe they deserve careful, sincere, and thorough explanations. So when I think about all of the medical misinformation that is out there right now around the COVID-19 vaccines and how we can possibly alleviate those fears, I start by imagining a patient sitting across from me in my clinic exam room with doubts, uncertainty, or even trepidation about these new and rapidly developed vaccines, and try to write out how I would try to answer their questions.
𝐇𝐨𝐰 𝐝𝐨 𝐭𝐡𝐞𝐬𝐞 𝐯𝐚𝐜𝐜𝐢𝐧𝐞𝐬 𝐰𝐨𝐫𝐤?
Updated 12/24/2020
When discussing vaccines with my patients, I always, always start with a brief discussion of how they work. It’s not uncommon to hear someone say “I think it’s better to rely on my own immune system” when discussing vaccine preventable illnesses. We’ll talk about this in more detail later on, but my first response is usually to help my patients understand that that is exactly how vaccines work; by relying on your own immune system.
Our immune system is designed with two strategies for fighting infections. The first is non-specific but immediate; in addition to our innate protective barriers like skin, hair, and mucous, we have cells like macrophages, mast cells, and natural killer cells that are able to detect and attack any foreign invader that the body recognizes as not being part of itself. This is a good system and prevents you from getting sick all the time; without it, we would be constantly fighting illness and infection from normal everyday exposures, just as many do who have compromised immune systems.
But even more powerful is our adaptive immunity, which is directed specifically against infections our body recognizes and has dealt with before. This is an incredibly robust system of B and T lymphocytes and antibodies that recognize the invading pathogens and kill them with a higher degree of efficiency and precision. The only problem with it is that it takes time to kick into gear the first time your body is exposed to a new infection; and then it’s a race to see whether it can become active enough, fast enough to prevent an illness from becoming severe. On subsequent exposures, that response is much, much more rapid; so much so that you usually don’t even know you’ve been re-infected with that bacteria or virus because you don’t get sick.
The principle behind vaccines is simple; what if we could safely teach the adaptive (specific) immune system to recognize the deadliest infectious diseases, so when someone is exposed the first time they can mount that powerful, targeted immune response right away and not even get sick?
And that’s exactly what these COVID-19 vaccines are designed to do, just like all of the vaccines before them; they give the body the information it needs to mount a robust immune response with the adaptive immune system as well as the innate immune system, without any possibility of causing an infection in the process. So when someone asks, “wouldn’t it be better to rely on our own immune system?” my answer is, “Yes, absolutely! And vaccines allow us to rely on our entire immune system, not just the weaker half, without even getting sick.”
We will talk about the differences between how traditional vaccines and the mRNA vaccines accomplish this later (and whether or not they re-write your DNA). For now I’ll just say that the new vaccines are even closer to naturally acquired immunity than traditional vaccines, because they trigger our immune system almost exactly like the viruses themselves do.
Will the vaccines have any lasting effect on my body?
Updated 12/26/2020
Hopefully! That’s sort of the idea. While the messenger RNA only survives for a few minutes before degrading, the antibodies that are produced will circulate for months, and some of the other cells of the adaptive immune system, specifically the antibody-producing plasma cells, will hopefully migrate to the bone marrow and lie dormant for decades, which is how vaccines given in childhood continue to provide protection many years later. This is true of the annual flu vaccine too, by the way; the issue isn’t that those vaccines don’t provide lasting immunity, but that influenza is a rapidly mutating virus and different strains are more common every flu season. So your flu shot from 1997 or 2008 is still providing you with protection… But only against the flu strains that were chosen for the vaccine in 1997 and 2008. They’ve even done studies that showed people who survived the Spanish Flu Pandemic of 1918 could still produce an antibody response 100 years later! Coronaviruses mutate much more slowly than the flu, but it is too early to know whether SARS-CoV-2 will mutate enough or in the right way to require additional, regular vaccinations. If we can judge by the SARS and MERS epidemics of 2002 and 2012, it seems unlikely.
As far as other changes to our bodies, thankfully there is no plausible mechanism by which the COVID-19 vaccines could cause other chronic changes than the desired immune response. The mRNA only codes for a few specific proteins and cannot produce an active virus, and the fats, sugar and salts in the vaccines do little else than package the mRNA and help it get into the cell.
What about Infertility?
There has been misinformation circulating online about the vaccines causing female infertility, but these are baseless. The original claim can be traced back to Michael Yeadon, a former Pfizer researcher and COVID-19 denier who has also posted videos claiming that the pandemic really ended in late Spring, at least in the UK, because most of the population was already immune due to having antibodies to other coronaviruses, which cause the common cold (as of today there have been over 70,000 deaths in the UK from COVID-19). This is an extremely ironic idea in light of his claims about the vaccine causing infertility, as we shall see shortly. He has not worked for Pfizer since 2011, and calling him the “Head of Pfizer Research” is just as deceptive as the rest of the headline and article.
The vaccine does not contain a spike protein called Syncytin-1, at all; the article above is simply lying at that point. The actual theory claims that the COVID-19 spike protein the vaccines code for shares similar amino acid sequences with a human protein, Syncytin-1, which is important in placental development. They reason that antibodies trained to attack COVID-19 would also attack Syncytin-1, causing infertility. This is illogical and scientifically invalid for a few reasons.
First, we have already had 80 million cases of COVID-19 worldwide and there has been no evidence of infertility as a side effect; yet the body of any infected person is going to produce antibodies against multiple COVID-19 proteins, including the spike protein in question. If the antibodies we develop against the spike protein from having the virus don’t attack Syncytin-1, there is no logical reason to believe vaccine-induced antibodies would either.
Second, we have evidence from the COVID-19 vaccine trials themselves that pregnancy occurs at similar rates between those vaccinated and those not vaccinated. The vaccine trials did not include pregnant women or women who intended to become pregnant, and all women of child-bearing age that participated had a negative pregnancy test before their first dose and committed to using a method of birth control throughout the study. Thirty-nine women became pregnant anyway; twenty-three in the Pfizer trial and sixteen in the Moderna trial, and the rate of unintended pregnancy in those who received the vaccine was about the same as in the placebo group. Those numbers are too small to draw serious conclusions, but the point is that we already have examples of women who became pregnant after receiving the vaccine, even though they were actively preventing pregnancy; in the coming months as more and more people receive the vaccines, we will have many more examples, and because this misinformation has been popular there are already studies planned to track the pregnancy rate following vaccination.
Third, the number of amino acids in the shared sequence is actually tiny; a segment of 5 amino acids, with only the first two and the last two being shared. Syncytin-1 has a full sequence of 538 amino acids, and the COVID-19 spike protein itself is 1,273 amino acids long. We have an analogy in human disease; one explanation for rheumatic heart disease following streptococcal infection is that certain proteins in the Group A strep bacteria share similar amino acid sequences with myosin, a protein found in heart muscle, allowing antibodies against the bacteria to cross-react with heart tissue. However, in that case there are not only much longer sequences of shared amino acids, but multiple sequences that repeat multiple times each. The section of shared amino acids in the case of Syncytin-1 and COVID-19 antibodies just isn’t significant, and you will find many viruses and bacteria in nature that share such similarities with a great many proteins in humans.
Finally, SARS-CoV-2 is not the only coronavirus in existence; not by a long shot. Coronaviruses are one of the main groups of viruses that cause the common cold, and you and I have both had many coronavirus infections throughout our lives. You still have antibodies to those coronaviruses, as Dr. Yeadon points out in his other videos. Every single coronavirus has spike proteins (that is what gives them their name; they form a halo, or corona, around the virus when you look at it through an electron microscope), and all of those spike proteins share as much or more similarity to Syncytin-1 as the COVID-19 spike protein, because they play similar roles in viral replication to what Syncytin-1 does in placental development (they are fusion proteins). So you have already developed antibodies against coronavirus spike proteins all throughout your life, maybe even every single year, just like everyone around you; and yet this has never been identified as a contributing factor in human infertility.
So yes, the vaccine will have a lasting impact on your body, assuming you respond well like 95% of clinical trial participants. The lasting effects will be the same as the lasting effects of surviving the virus: immunity to COVID-19, and hopefully long-lasting immunity. The difference is that the vaccine doesn’t carry a risk of serious illness or death to you or transmission to those around you. And thankfully, neither immunity from getting the vaccine nor immunity from getting the virus itself will cause infertility.
Aren’t the vaccine ingredients toxic?
Updated 12/29/2020
Those whom I interact with regularly who are undecided or hesitant about vaccines are typically patients and parents with sincere, legitimate questions, who deserve the time it takes to hear their concerns, answer their questions completely, and offer reassurance. But unfortunately, therearealso people out there who are promoting anti-vaccine propaganda and deliberately creating false narratives. One common strategy to increase unease or paranoia about vaccinating our children is to simply list the scientific sounding ingredients and then ask, “do you really want to put that into their bodies?” Usually this approach will ignore benign sounding ingredients like “sucrose” or “gelatin”, and focus in on lengthy or scientific-sounding ingredients like “nicotinamide adenine dinucleotide” or “cetyltrimethylammonium bromide,” which register emotionally as more intimidating, less safe, and less natural. Of course we know that logically a chemical with a long name would not necessarily be any more or less dangerous than one with a short name; “ricin” has a short name, and it’s the 5th most dangerous chemical in the world (that is just an example; there is NO ricin in your vaccines. I do not want to see a bunch of memes next week claiming they put ricin in vaccines). But fear mongering is not always logical.
DANG IT
They might also home in on a naturally occurring and well known chemical that most people think about in conjunction with another of its uses, counting on that association alone to create fear. A good example is formaldehyde, which most of us think of in the context of embalming, but is also used in applications from color photography to deodorants; and of course, as an anti-bacterial and anti-fungal in certain vaccines. Some vaccines contain about .005 to .01 mg per dose; a 2 month old baby produces up to 200 times more than that every single day as a part of their normal metabolism (for adults, it’s more like 3,000 times more). Yet because our culture so strongly associates formaldehyde with death, merely invoking it’s name is enough to create unease.
Most of the ingredients in vaccines are there to keep the attenuated or killed virus pieces from decaying long before they are injected. Others are there to prevent the growth of bacteria or fungi in the vaccine vials themselves. Still others are used to stimulate the body’s immune cells around the injection site to make them more likely to produce an adequate response that leads to long-term immunity. All chemicals we encounter in our lives are toxic under certain circumstances; none of the ingredients in vaccines are toxic at the doses or in the manner given. I think people often forget that the scientists who design the vaccines, and the doctors and nurses that counsel patients about them and inject them, are human beings who also vaccinate ourselves and our children; we want vaccines to be safe for selfish reasons, too, not just altruistic ones.
That all applies to traditional vaccines; the new mRNA vaccines are made differently, and so they don’t need a lot of the same additional chemicals to ensure they work. In fact, what’s shocking about them is just how few ingredients they actually have. In addition to the messenger RNA molecules themselves, the Pfizer vaccine has just 4 synthetic fats (lipid nanoparticles) meant to deliver the mRNA into the cells that will build the COVID-19 spike protein, 4 salts to make sure the vaccine is at the same acidity and osmolality as the tissue it is being injected into so it can get absorbed (and hurt less), and 1 sugar, sucrose, to protect the vaccine during cold storage.
Salt, fat, sugar. And that’s it.
Some of the substances can still cause a reaction; the leading theory right now is that the few anaphylactic reactions to the Pfizer vaccine were likely due to polyethylene glycol, a common chemical we give in huge doses for constipation, but which can cause an extremely rare, but serious, allergic reaction. This chemical is used to create the lipid nanoparticles through some Tony Stark level methods I can’t hope to understand. The lipid nanoparticles (very small fat molecules that can protect the mRNA) themselves are indeed new technology; which in science terms means about 30 years old. Over that time period their safety has been studied extensively and found to be safe, non-toxic, and biocompatible/biodegradable. And because the world is crazy,no, they are not tiny robots(but how cool would that be?!).
By contrast, “Nana Lipid Particles” are just the cookies she keeps sneaking your kids when you aren’t looking.
An article in 2016: “After 25 years of research…” The math checks out.
I can’t claim to be familiar with every anti-vaccine meme and article out there, but I haven’t seen as much about ‘toxic ingredients’ with the COVID-19 vaccine, and I think that’s because even compared to the safe ingredients of traditional vaccines, the ingredients of the COVID-19 mRNA vaccines just sound very unimpressive, and thus feel less intimidating.
If I get the vaccine, can I still transmit/spread the virus?
This is a question I’ve heard frequently, especially from those who themselves work in healthcare or have vulnerable friends and loved ones. It is a question driven by compassion. In this blog we have been trying to address the fears and concerns that arise not only from conspiracy theories and misinformation, but also from the very small but real risk associated with the vaccines; yet I know that many people would brave whatever degree of risk to themselves (again, It’s very small) if it meant protecting their family and community. If they could be guaranteed that their choice to get vaccinated meant they could safely visit an unwell grandparent or have coffee face to face with a friend without any risk of spreading the virus, it would be a no brainer even if there was a considerable risk it might cause significant side effects like Bell’s Palsy (there isn’t).
And I wish I could give that reassurance today, but while I can say that the chances are very good this vaccine will not only protect you but also protect those around you, we still need much more data to be able to quantify the degree of that protection.
The point of the vaccines is to provide your systemic adaptive immune system, the part that acts powerfully and rapidly against specific disease, with the information it needs to produce the antibodies you need to keep you from getting very sick. A common misconception is that after you get say the flu shot, you can’t get the flu. It’s not true. The flu shot doesn’t give you a magical forcefield around your body that blocks flu virus, it just helps you fight it much, much more quickly and efficiently when you do get it; often to the point that you never even know you are infected, or at least only have very minor symptoms. Vaccines drastically reduce the chances of you becoming extremely ill from deadly disease like influenza, measles, or COVID-19; that’s their job.
This is not how you get a cold. He’s the best he is at what he does; but what he does is not immunology and pathophysiology.
This main function of vaccines is what underpins the epidemiology strategy of giving the COVID-19 vaccine to healthcare workers and the most vulnerable first. The medically vulnerable, because they are the most likely to require high levels of care, to suffer long-term problems from infection, or to die from COVID-19; and healthcare workers because as the pandemic worsens it becomes more and more important to preserve our medical workforce, and vaccinated folks are less likely to need sick time (much less become seriously ill and require hospitalization themselves) for COVID-19. The other reasons for vaccinating healthcare workers go back to courage, trust, and solidarity with our patients in the face of any new treatment. We are prioritizing vaccinating the vulnerable instead of say pathologic extroverts because the effectiveness of the vaccines at preventing significant illness is known (90-95%), but their effectiveness at preventing transmission is still unknown.
So how do we find out so that Dustin can get his vaccine? Well, the big question mark is IgA antibodies. Most of the research on antibody production from COVID-19 vaccination focuses on IgM and IgG because they predominate in the blood and represent, respectively, our short-term and long-term antibody protection against systemic (whole body) illness. But IgA is the main antibody in the mucous membranes; your mouth and throat, nasal passages, lung surfaces, and digestive track (it’s also the antibody responsible for passive immunity transmitted through breastmilk), and we know that the IgA response to infection is a big, big part of what neutralizes the virus and decreases transmission in those first 10 days of symptoms. If the vaccines “only” cause a significant IgG and IgM response during that post-vaccine exposure to the COVID-19 virus, it will prevent severe infection; and may still prevent enough viral replication to slow transmission. But if it produces a strong IgA response too (or a strong enough mucosal IgG response), it will almost definitely neutralize any live virus in the upper airway as well, making transmission as unlikely as severe illness. In other words, the degree of IgA response is a strong predictor of whether the vaccine protects those around you as well as it protects you.
Because of this, researchers are already studying the degree of production of mucosal IgA against COVID-19 in vaccine recipients, with some promising results, and at least one intranasal vaccine (which produce a very strong IgA response) is under development. And while the best information we could get would be to see exactly how well someone develops IgA and neutralizes the virus by studying them when they are exposed to COVID-19 after vaccination, it’s sort of hard to catch people in that window. In the end we will probably have to settle for epidemiology data instead; carefully watching to see if clusters of infection occur around exposed, asymptomatic vaccinated people at the same rate that they do around unvaccinated people. That will take time, but if and when it becomes apparent that vaccinated people really aren’t spreading the virus to those around them at all, that will be the point I’ll stop wearing my mask, practicing social distancing, and washing my hands (fine, fine; I’ll keep on washing my hands).
I realize this was a really long-winded way of saying “I have no idea,” but I want to conclude with a few reasons you should get the vaccine even if your main concernis not spreading the virus to others.First, there is already a lot of good data that supports the idea that these vaccines will provide mucosal immunity (and thus decrease transmission), both from studies of the COVID-19 vaccines themselves and from our much more robust knowledge of vaccines in general; it’s hard to say anything with much confidence yet because we’ve had these vaccines for such a short time, but I’m pretty optimist they will. We’ve followed these principles for years; we recommend everyone around a newborn be vaccinated against Pertussis (whooping cough) because the newborn can’t be, and we know that vaccine-derived herd immunity works even for viruses that are primarily spread through respiratory particles. Second, there is no conceivable mechanism by which they would increase transmission. The vaccines cannot make you produce live virus (at all) so they can’t make you contagious, and if you are exposed to COVID-19 later on your body will still respond with a mucosal immune response whether it is augmented by your vaccine or not (and it probably will be); the vaccine won’t stop that. And third, by preventing a severe systemic illness, the vaccine will decrease the amount of time you are shedding virus and prevent transmission in some of the most high-risk settings; aerosol producing procedures like nebulizer treatments or intubation in the hospital. And by preventing symptoms like coughing and sneezing the vaccine will make you less contagious when exposed to the virus, as long as you are still following other transmission control measureslike wearing a mask and quarantining after exposure.
IgA response due to ChAdOx1 nCoV-19 vaccine (the tall red columns are good!)
So no, unfortunately being vaccinated against COVID-19 does not give us carte blanche to schedule giant indoor parties, throw away our masks, and treat the pandemic as if it were over; but they are a huge step in that direction, and in addition to protecting ourselves they do have a fair, if yet unproven, chance of protecting those around us too. And besides, if you don’t get vaccinated, how are you going to get your government tracking microchip?
Bad joke, sorry.
Other Vaccine Posts:
No Vaccine Selfie Yet or “Why I am uncomfortable getting vaccinated”
You all remember what it was like in January and February before the COVID-19 virus had come to the United States, and before we began to treat it like a pandemic. It seemed like everyone was getting the flu, just like any normal year. The flu shot for that flu season only had about a 45% efficacy- not the worst we’ve ever had, but certainly less effective than we’d hoped- and hospitals were busy treating children, adults, and elders for complications of Flu A and Flu B. And then a couple of short months later…. *POOF!* It was like the flu had just disappeared. We didn’t hear about it anymore, nobody was talking about it; everything was COVID-19.
In March and April we began to see memes questioning why the flu had seemingly gone away. And then a few weeks after that… The memes were gone too, like magic! And for 7 whole months nobody mentioned or thought about the flu. Until a couple of weeks ago, when memes like this began to circulate again:
Isn’t is wonderful?
And although it’s only December 15th and the people posting these memes and #whereistheflu conspiracy theories are shooting their shot a bit early, I think now is a great time to answer the question, “Where is the flu?”
Contents: -What does a normal flu season look like? -Why doesn’t the ‘where is the flu’ theory work? -What did happen to all the flu cases? -What would you have to believe for these memes to be true?
What does a normal flu season look like?
The reality is that there’s really no such thing as a “normal” flu season. While different strains of influenza circulate in our communities each year, they are all unique in their own horrible ways, and we can’t predict ahead of time when we will have a mild flu season, like in 2015-2016, or when we will have a terrible flu season that threatens to overwhelm our healthcare systems like in 2017-2018, the worst I’ve experienced as a physician. But we can draw some generalizations about flu season:
It’s going to happen during the Winter.
People are going to die.
It’s going to suck.
I hate the flu, and even if we as a society have mostly relegated it to sitcom B plots and ‘man cold’ jokes, the reality is that it’s a killer, and I have patients with chronic respiratory diseases, compromised immune systems, or just poor overall health that I worry about every single year as flu season begins to ramp up.
We typically expect flu season to begin in early Winter, usually November, peak between December and March, and typically to be ended by April. A late flu season might last until May, but that’s fairly rare. However, the last flu season we’ve seen peak in December was back in 2014, and for the past 6 years it has been in January, February, or even mid-March.
So while I’d never fault anyone for trying to get work done early, those ‘Where are the Flu?” memes really would make more sense in January or February, when we would be expecting flu season to be peaking. Nobody finds misinformation claiming that doctors are padding the COVID-19 numbers with flu cases convincing in June and July, so I’m sure they wanted to take advantage of the cold weather for as long as possible.
And honestly I hope we are still seeing those “where is the flu?” conspiracies in February and March because the flu cases stay ridiculously low. That would be a lot better than internet memes saying “oh man, remember back in 2020 when we only had one deadly respiratory virus epidemic to deal with?”
Why doesn’t the ‘where is the flu’ theory work?
Let’s go back to that first meme at the beginning of the article, which deserves a bit more of our attention. It comes from the WHO FluNet, and anyone in the world can go to that website and look at reported flu cases for any date range going back to 1995. The first thing you’ll notice about the image is that it is on the order of tens of thousands; each major division of the Y axis is 20,000 cases. The image is supposed to convince you that the WHO just forgot to record flu cases at all as a part of this big hoax, but still published their flu numbers with empty charts for the whole world to see. Pretty incompetent conspiratoring if you ask me. But the truth is, that seemingly empty section of the graph is not empty; the 2nd image below is that same ’empty’ time frame, just with a smaller scale.
This is still an incredibly small number of cases, but it demonstrates the same week-to-week and seasonal variability flu cases normally follow; that part of the graph isn’t empty, and the data checks out.
In this context, the original image is suppose to convey two ideas; either that doctors have stopped checking for the flu altogether, or that they are ‘stealing’ flu cases and filing them under COVID-19.
The first is easy enough to answer; we haven’t stopped checking for the flu. I’ve just logged onto our electronic health record and I have a message from a colleague about a positive Flu case. We are ordering the tests, and some of them are positive. How reliable flu testing is at baseline is a topic for another day; at the very least it can be compared from year to year to help us understand how relatively bad the flu season is. As a physician I rarely order flu tests, but I’m not the one driving this data; and in fact, with COVID-19 causing similar but not identical symptoms to influenza, I’ve personally been testing for flu more in 2020 than in any year before, because differentiating between flu and COVID-19 is now an additional utility of the flu test; I know several clinicians who are doing the same. We can look at the CDC numbers to see if we are outliers here in Waco, or if doctors are in fact still testing for the flu.
So far, labs that participate in CDC influenza monitoring have tested 232,452 Americans for the flu. At the same point last year, the number of tests reported was 265,670, but instead of having only 496 positive results and a 0.2% positivity rate, we had 15,027 positive results and a 5.7% positivity rate. And while this clearly does not include all flu tests that have been ordered since September, it is a representative sample. So we know that doctors at ordering the tests; the tests are just negative.
That leaves us with the flu cases being stolen somehow. One way for this to happen is for the flu analyzers to be calibrated to call flu tests negative so we can count them as COVID-19 instead (and by logical extension, the COVID-19 machines calibrated to detect flu and call it COVID). The problem with that is that every lab has a different strategy for testing these two viruses. Many labs use completely different machines to test for COVID-19 and flu, and their flu machines have been utterly uninvolved with their COVID testing strategy; untouched, with no updates or software downloads that would cause them to stop detecting flu. There are even lots ofclinics that don’t test for COVID-19 at all; have they had their rapid flu tests updated to stop detecting flu, and are now just going through the motions of collecting flu swabs to make some other lab’s COVID-19 results more believable? It’s not just far fetched because of the unbelievable extent of involvement such a conspiracy would require, but because so many people would have to be a part of it even when they are far removed from the COVID-19 testing process and apparently have nothing to gain.
A more parsimonious theory is that the tests are being run as normal, but the CDC is changing the numbers. We track flu tests in the US to determine the positivity rate and understand when flu season begins, when it peaks, and when it ends. We use other metrics like excess mortality to really understand the full impact of a flu season and estimate the number of cases. Right now, the laboratory result tracking is telling us that there just isn’t appreciable community transmission; but what if the CDC has moved all of the positives over to COVID-19? By this point last year there had been 15,027 positive flu tests reported to the CDC. In that same time period this year, we’ve had 9,755,813 new COVID-19 cases (including me!). So those flu cases would represent approximately 0.15% of all of the new laboratory confirmed cases of COVID-19 reported in the US since monitoring for the new flu season began at the end of September. Shifting the flu tests we track to COVID-19 wouldn’t just be a dishonest and transparent strategy for inflating the pandemic numbers, it would also be entirely ineffective and unnecessary. If they just reported flu cases like normal, the COVID-19 numbers would be almost exactly the same, and they’d be far less likely to get caught. If you are trying to embezzle millions of dollars from the bank, you don’t cook up a fake set of books and then turn around and stiff your customers a couple of bucks when they come in to cash their checks, too (I am currently in the market for a much better financial analogy. Please send suggestions to tjwebb@tjwebbmd.com).
Claiming that the COVID-19 numbers are being inflated with influenza cases also does absolutely nothing to explain two important facts about the pandemic; the pattern of cases over time, and the number of deaths. If we were ever to see even a fraction of the number of deaths due to seasonal influenza that we are right now from COVID-19, especially this early in flu season, we would be dealing with the worst flu since the Spanish Flu of 1918. If that were the case, the flu itself would be a pandemic exactly as bad as COVID-19… So why all the pretending? The numbers also don’t fit the pattern of seasonal flu at all. Look on the graph below and tell me when ‘they’ would have switched to using the flu to generate COVID-19 numbers. October 10th? That’s when cases really began to climb, and that’s too early for flu season. What about the cases in April, or the nationwide surge in July?
The “What Happened to the Flu?” conspiracy is extremely weak because not only does it have no explanatory power, it also has to be combined with multiple other conspiracy theories (like “the doctors are lying on the death certificates“) to work at all.
I think a lot of people find the apparent absence of the flu convincing, and I think I understand where they are coming from. Most of us aren’t used to thinking like epidemiologists. I’m not. We know people who had COVID and were fine, just like we know people every year who get the flu and are fine. If we know someone who died of COVID, as I do, it’s a tragedy; just like it’s a tragedy if we know someone who died of influenza. But we aren’t actually very good at looking at the world around us and intuitively understanding the scale of a normal flu season versus the scale of a global pandemic. So noticing a decrease in one is enough to allow us- if we really want to be convinced- to dismiss or explain away the other; until we actually look at the real numbers.
What did happen to all the flu cases?
The reality is that the CDC and the WHO are reporting such a small number of positive flu tests because… there are a lot fewer cases of the flu. And although experts have told us to expect a particularly light flu season for months, it begs the question; is it really possible for it to be this light?
The answer is yes, thankfully, and for some very good reasons. First, as we’ve been saying, it’s still very early in flu season; we just don’t know how bad the peak will end up being yet, though these early numbers are a very good sign. Second, flu vaccination rates are actually higher this year than last. With the flu vaccine typically being between 40 and 60 percent effective, even a modest increase in flu shots will result in millions of fewer cases. But more importantly, we can expect a light flu season because every single measure we use to decrease COVID-19 transmission decreases transmission of the flu too. Decreased indoor gatherings, wearing masks that block respiratory particles, a significant portion of the population working from home, doing remote learning, and sheltering in place; all of these are going to decrease transmission of influenza even better than transmission of COVID-19. Why better? Because the flu is less contagious, for one thing; it is less efficient at spreading from person to person and therefore it is easier to mitigate with masks and distancing. But even more important is the fact that some of our strategies thatare only modestly effective for COVID-19 are actually veryeffective for influenza.
Take symptom monitoring for instance. Right now every school, daycare and university, and most businesses, are carefully monitoring their students and employees for infectious symptoms like cough, nausea, and fever, and insisting they miss school or work and see a doctor if they are ill. Because COVID-19 is spread even by people who are asymptomatic or who have not yet developed symptoms, this strategy is only effective for symptomatic COVID-19. There is also a long lead time for COVID-19 during which a pre-symptomatic patient can spread the virus before they are sick enough to screen positive and be told to stay home; the incubation period of the virus is up to 14 days or longer, with most people developing symptoms around day 6-7 on average. Prior to this, they are at work and school and don’t realize they can infect others. That’s why this strategy absolutely has to be paired with excellent contact tracing and quarantine for close contacts. But our contact tracing system in the US failed early on, and between American individualist culture and misinformation and conspiracy theories about the virus, quarantine of close contacts has been the single hardest measure to generate buy-in for.
Contrast this with influenza, which has a 1-4 day (average 2 days) incubation window and is far less transmissible in asymptomatic or pre-symptomatic patients. By the time a person is able to spread the flu, they have symptoms of the flu. In normal years a fever or vomiting might cause them to stay home, but they can continue to work or go to school with mild to moderate flu symptoms like cough and sore throat; but not in 2020, when even the social condemnation attached to coughing in public is enough to keep a lot of us at home when our allergies are acting up. Keeping people who feel well in quarantine because of exposure to the virus was always going to be a hard sale, even when that advice is based on solid epidemiology principles. Fortunately, slowing the flu doesn’t depend on that particular strategy.
Is that enough memes? That feels like more than enough. You get the idea.
It also bears pointing out that the mitigation measures for COVID-19 actually have worked, and are working. Those who want to minimize or deny the realities of this horrible pandemic are fond of pointing to the early models that predicted greater than 1 million deaths in the US and asking, “what happened to all the deaths?” But those were predictions about what would happen without mitigation, and having already reached 307,000 deaths with extensive mitigation efforts, those early numbers now feel like low estimates instead of end-of-the-world scenarios. Because strategies to reduce COVID transmission are being followed or ignored to more or less of a degree not in different states or cities but in different houses on your street (and even by different people in your own house), we will never really know which mitigation measures were most effective or how effective they might have been with higher engagement; but it is clear that even with actual levels of adherence, they are even more effective for the flu than for COVID-19, which makes perfect sense when you compare the characteristics of the two viruses.
What would you have to believe for these memes to be true?
Finally, I want us to really stop and ask ourselves, if these memes and commentaries were true, what would we have to believe? First, let’s reiterate that the people creating these mean one of 3 things:
Where are the flu cases? The flu cases are there, but doctors and the CDC have decided to ignore them altogether.
Where are the flu cases? A lot of the tests for COVID-19 are actually positive tests for the flu, but they aren’t being reported that way.
Where are the flu cases? Oh wow! It’s so wonderful that we aren’t seeing much flu activity right now.
Since we can rule out the 3rd one (even thought it is, actually, the one supported by the facts), it has to be some combination of the first two. And in order to find those ideas convincing, here’s what you have to believe.
Warning: Most of what follows is sarcasm. (so please don’t quote me on any of this out of context)
– Your local clinic doctors (including me), who hate the flu and COVID-19 and have lost patients to both, are waking up every morning, going into work in full PPE, and seeing patients for cough and fever. – They are spending 10-15 minutes talking face to face with patients about COVID-19, about the safety precautions and how to do isolation and quarantine, what red-flags to watch out for, and offering heartfelt reassurance and telling their patients not to be afraid, but to stay vigilant in monitoring their symptoms. Sometimes they are even praying with them at the end of those visits. – This is all a waste of breath and they know it. It’s a big sham, and they are play-acting their part. They know full well that whether their patient has a cold, or seasonal allergies, or the flu, they are going to call it COVID-19 anyway (and go ahead and ignore the fact that we aretelling people ‘hey I think this is actually just your allergies’ all the time. If we wanted to inflate COVID-19 numbers we could do it all day long. But we don’t and we aren’t). They’ve spent all these years trying to help peoplefightdisease, and now they are going to spend their time lying to people, leaving them less prepared for and knowledgable about the disease they actually have. And because they don’t give you a new patient panel when you sign up for a global conspiracy, they are actually lying to thesame people they’ve spent all of those years trying to help as their primary care doctor.
I realize this is the worst possible gif and the opposite of my point. I just really like this movie.
– They order a COVID-19 test and the nurse collects a sample and brings it to the lab tech, who places it in a machine to test for COVID-19; maybe they are also running a flu test for that patient. But the fluanalyzer has been programmed to call the flu test negative and the COVID-19 analyzer has been programmed to call the flu COVID instead. Why test for anything at all; why not just call a certain percentage positive and have done? – The clinic doc gets the fake COVID-19 test back and tells you it’s positive, and advises you to isolate for 10 days. This is because they… Hate your job, I guess, and want to make you stay home so you won’t get paid? I mean, I write letters for patients to help them get work accommodations for their medical conditions all week long, and I even call managers, bosses, and HR reps to make sure my patient isn’t at risk of losing their job because of a medical issue. I’ve helped people with their depression and anxiety every day for years, a lot of it because of financial difficulties. I’ve even connected people with legal resources so they could fight to keep working when they were wrongfully terminated because of their health. But sure, I guess it makes sense that I want my patients to face more financial hardships and want their lives to be worse. That’s what really lights the fire under us to make all those sacrifices in medical school and residency. – The doctor knows you have the flu, but instead of seeing if you are one of the people that might benefit from Tamiflu (it’s not as good of a medicine as you might think), they withhold that medicine because offering it to you would give away the game, and of course their commitment to this fake pandemic is greater than their commitment to helping their patients or their Oath. – You ask the doctor about your young children; are they going to be ok? Even though they know that children under 5 (including two of my own), and especially under 2 are at high risk for complications from the flu, they go ahead and offer fake reassurances. “I don’t want you to be afraid,” they say, “thankfully, your children are at much lower risk from this virus than even a healthy young adult.” That probably eats at them a bit, lying to you about whether or not your kids are in danger; but they are just really committed to this conspiracy.
– Meanwhile, by the way, their colleagues in the hospital are spending even more hours and making even more personal sacrifices to treat incredibly sick hospitalized patients. Instead of treating them like normal pneumonia, flu, and heart attack patients, they are calling them all ‘COVID-19’ and treating them with steroids, prone positioning, anti-virals, and convalescent plasma; all to maintain the ruse. It wouldn’t look good for the numbers to only be bad in clinic. – Finally it’s time for the doctor and the nurse and the lab tech to send their fake lab results to the county health department, and then on to the CDC. Here the CDC, rather than reporting fake numbers that perfectly match their false narrative, will carefully tabulate the fake lab results they’ve received from all over the country, throwing in a few positive Flu cases and different flu strains (including some their experts didn’t recommend we vaccinate against) just for good measure. Seems like an awful lot of trouble.
Also, by having an incredibly mild flu season and diverting all of those flu numbers to COVID-19 (even though, again, they aren’t really needed), they allow graphs like the one in this article that make it really obvious to any conspiracy theorist on the internet what’s going on. Such an intricate conspiracy, but so poorly executed.
And why do we do all of this? Well, because fear of the pandemic helps shutdown the economy and hurts your political candidate, according to one theory (I still don’t know how they convinced all of my conservative, Republican doctors to go along with it). You would think there’d be an argument that two contagious killer viruses might convince people to stay home even better than one… Or, according to another theory, to sell COVID-19 vaccines for big pharma. Because everyoneknows I get daily instructions from my pharmacy sales rep masters, instead of, you know, barely tolerating being forced to occasionally interact with them so I can get some free insulin samples for my patients. I suppose flu shots just aren’t as profitable.
Not you Gus! I didn’t mean it.
Which brings up another good point. Besides the doctors and nurses and lab techs and of course the CDC, who else would need to be complicit in this scheme? Well, Hoffmann-La Roche Inc. and Gilead Sciences, for one, the manufacturers of Tamiflu. I don’t prescribe it much myself, but during flu season it’s one of the most commonly prescribed medications. That company also makes Remdesivir, one of the medicines used for certain COVID-19 patients; but only in the hospital. Bad work on their accounting department, sacrificing most of their sales from a widely prescribed outpatient medication to focus exclusively on an inpatient medication prescribed only for some patients.
I’m not willing to put anything past drug companies, but it does seem like allowing for a ‘normal’ flu season would at least help them hedge their bets a bit. Then again, Tamiflu is available as a generic now too, so maybe this is a corporate high risk, high reward gamble. Let’s move on.
Who else would have to be complicit in it? These guys: Sanofi Pasteur, Inc Seqirus, Inc. GlaxoSmithKline Biologicals Protein Sciences Corporation MedImmune, LLC Recognize them? Those are the top manufacturers of seasonal flu vaccines, and none of them has a COVID-19 vaccine (at least not one close to being approved). The companies that make the two vaccines currently approved or about to be approved for COVID-19, Moderna and Pfizer, do not have seasonal flu vaccines.
You write the script. Powerful, multi-billion dollar pharmaceutical companies that have lost the race to create a vaccine against a hoax virus (or didn’t even try), and now are missing out on all of that sweet, sweet COVID money. They know it’s a hoax and more than likely have some proof. So what do they do? They expose it for what it is, involving their competitors in scandal and allowing them to grab a greater market share and keep their flu vaccine as the most important vaccine of 2020. Except that’s not what they’ve done; if you go to any of their websites, you are going to see messages saying, basically, “good job on developing those COVID-19 vaccines you guys, we are rooting for you.” Sincere? Who knows. But definitely not the type of corporate warfare you would expect if they knew the virus wasn’t really that dangerous and were missing out on all the fear-monger profits.
Now, I know what you are going to say. ‘Fine, maybe it isn’t the doctors and nurses, maybe it’s just the CDC and the WHO. And hey, thanks for not including me in your global conspiracy. Let’s say that this is a regular flu season, or even a particularly bad flu season. That means that say hundreds of people a day are dying (or 3,000, if you are saying all COVID-19 cases are really the flu), and hundreds of thousands are getting the flu, and the doctors are… What? Too dumb to know the difference? Too lethargic to figure out what’s flu and what’s COVID-19? If we aren’t in on it, then we are either too dumb or too complacent to notice it; you know, the two primary things doctors are known for, being stupid and lazy. Every day at our COVID-19 outdoor clinic I hear the same conversation between doctors that are floating there to help; “have you guys seen much flu yet?” And every day I hear the same answers; “not really” and “I’ve had a couple.” If we were in the midst of a bad flu season right now and it were being covered up, you’d have hundreds of thousands of doctors, nurse practitioners, physician assistants, nurses, and all sorts of healthcare workers blowing the whistle, not just a couple of drug reps posting their text messages on Parler. Instead what those clinicians are saying is, “COVID is really bad right now. Please wear a mask. Our hospitals are overwhelmed; thank God the flu isn’t bad right now too.”
After weeks of COVID-19 misinformation being a secondary or minor issue- to me because we have been so busy actually diagnosing and treating the virus, and to the country in general because election misinformation was much more interesting- I suddenly find myself with more pieces of misinformation to write about than I could possibly make time for. There is this meme that probably needs some attention as people who haven’t complied with mitigation measures since March threaten non-compliance with any future mitigation measures because the mitigation measures they already didn’t comply with didn’t work(because they didn’t comply with them). If I get time I’d love to explore that a little further (and, I should hope, a bit more graciously than I did in that last snarky sentence).
This reminds me of the great Chesterton quote; “Christianity has not been tried and found wanting. It has been found difficult; and left untried.” Could we say the same thing about self-quarantine, shelter in place measures, and especially lockdown efforts? And what then shall we say about wearing masks? “It has been found slightly inconvenient and inexplicably controversial, and tried only begrudgingly and inconsistently?”
There’s also a discussion that we need to have, as a nation, about how this pandemic didn’t go away on November 4th and isn’t going to go away when we have a new president in the White House. This virus is pitilessly apolitical. It doesn’t care about Republicans and Democrats, the electoral college, lawsuits in Pennsylvania, or any of the other big problems facing our democracy (did I just include Republicans and Democrats in the list of problems facing our country? Yes, yes I did). In an election year, and particularly one this contentious, there was never any chance that information and understanding about the pandemic would fail to fall out along party lines. Now that the election is over, is it possible for us to drop our politicized misinformation and as a countrymen find some common ground on which to fight this deadly virus together? Probably not. But it doesn’t mean I can’t rant about it for five or six thousand words.
But I think the most pressing is the video I’ll share a little way below, which was sent to me by a Facebook friend. It’s a short misinformation video about the COVID-19 vaccines that are being developed and, like most misinformation, is an amalgam of half-truths, deliberate misrepresentations, and outright lies. It’s very short and I’ve posted it here in it’s entirety with the hope that you will read the accompanying discussion and not just watch the video.
Will I get the COVID-19 Vaccine?
Let me start with a statement that might be a bit controversial; while I’m obviously strongly leaning that way, and hope I have the decision put before me as soon as possible, I haven’t absolutely decided whether or not I will get the COVID-19 vaccine once it is available. That might sound like heresy coming from a doctor, particularly when we are currently in midst of the worst wave of the deadliest pandemic of our lifetimes.
But let me explain what I mean. While it’s encouraging to hear that the new vaccine from Pfizer is 95% effective against this very, very deadly virus, and while a safe and effective and widely accepted vaccine is the best and quickest route we have to beating the COVID-19 pandemic without even more massive loss of life, I remain at heart and by training a scientist, not a science fan; I default to skepticism of any new discoveries or developments until I have reviewed the evidence for myself. With regards to the COVID-19 vaccines that have been in development over the past year, I am like most physicians cautiously optimistic. Before deciding to have the vaccine administered to myself and my four children, however, I plan to review all the data that I can in order to ensure my choice is as informed and sound as possible, just like I would for any medication, surgery, or any other intervention my doctor recommends (or, for that matter, any treatment or medication that I recommend to my patients).
“But Dr. Webb, this is exactly what anti-vax parents are doing when they refuse vaccines.”
Yeah, except that it isn’t. At least, not generally. You see, when I say I plan to review the data I mean the actual data from the clinical trials and independent studies, not misinformation and propaganda. If you are like me and have the privilege of scientific training that allows you to independently parse the information contained in published clinical trials, you probably have no desire whatsoever to outsource this type of academic work to people who do not have that training and who are approaching the information with blatant and unabashed bias. But if you do not have the background to do that work yourself, you still deserve the same degree of reassurance and comfort before choosing to accept a vaccine or have it given to your children; it is just less likely that you have access to the resources you need. The anti-vaccine movement knows this and it is in this gap- the gap between the confidence you need for such an important decision and the degree of explanation, information, and reassurance that you are generally given– that they do their best (or most effective) work.
Who is to blame? Well, obviously, I am. Your local doctor, your pediatrician, your PCP; we carry the burden not of fighting propaganda, the blame for which rightly rests on those creating and spreading it, but of helping you become resilient against propaganda and misinformation through patient-centered health education.
So I am begging you, if you are at all wary of or uncertain about a COVID-19 vaccine, and if you do not have the technical background or family/community resources you need to review the source data independently, ask your primary care doctor. Maybe even give them a heads up when you schedule an appointment so they can look into it beforehand (they probably already will have). If they are active on social media, ask them if they would be willing to write about it and share it openly. Some primary care physicians, like Dr. Ben Brashear here in Texas, believe so strongly in this type of work that they have devoted a large amount of their time and energy to helping their patients and other readers navigate these issues through their clinic websites and social media pages. I think this is the single most effective way to combat Social Media Misinformation; with a hundred or a thousand or ten thousand doctors and scientists in small towns like mine or Dr. Brashear’s helping patients whom they have already built a trusting doctor-patient relationship with navigate what information is reliable and what isn’t.
And of course, on the off-chance that over the past 6 months of my writing these blog posts you have somehow decided you actually trust me, I’ll plan to write a short post about my decision on the vaccine as soon as I’ve decided, for certain, what to do for myself and my family.
I should also point out, while we are dispensing with preliminaries, that this post is not designed to be an overview of the research and development of the various COVID-19 vaccines. For that I will point you to my hero, Baylor Friendly Neighbor Epidemiologist Dr. Emily Smith.
“The ChAd Vaccine” Video Minute-By-Minute Discussion
0:12 Share this everywhere!
I’ve been doing this sort of misinformation debunking work as a hobby for about 8 months now and I’ve come to recognize some of the language or verbiage that ought to make us extremely suspicious that the information we are about to be given is not necessarily reliable. The speaker hits several right out of the gate:
“This is a fact.”
In my experience, things that are facts don’t need the disclaimer “this is a fact.” Both for people spreading misinformation and those of us fighting it, the goal has to be to lay out such a clear and compelling case for the facts that the rhetorical sledgehammer of “I’m telling you the truth, I wouldn’t lie to you” is as unnecessary as it is hollow. If someone finds this verbiage convincing, it is likely because they are anxious to be convinced; and it should put you on your guard. “Let your ‘Yes’ be ‘Yes,’ and your ‘No,’ ‘No.’ For whatever is more than these is from the evil one.” -Matthew 5:37
“Share this everywhere.”
Similar to the last point, I believe that most people giving reliable, expert advice or guidance will never ask you to “share” something they have written. Why? Because the burden of demonstrating that an issue is so important and pressing that it should be shared broadly lies again with the author, and lies in the substance and veracity of the arguments, not with the mere desire of seeing their assertions disseminated broadly. Nevertheless, I do recognize that “share this now” is a part of our vernacular now and used by almost everyone of a certain generation on back; but I think it is most suspicious as a herald of misinformation when it is accompanied by….
“They will take this down.”
I sure that at some point something I write, either here or just on just on social media, will be taken down or marked as inaccurate; and when that happens I will probably throw a fit like I’ve seen others do. Until then, I will hold onto the sanctimonious belief that only those intending to spread misinformation feel that it is necessary to preface each video, meme, and essay with “this will be removed” or “they don’t want you to know this.” Who, exactly? The expansiveness, complexity, absolute loyalty, and conflicting goals and values of all of these conspiracies you believe are striving to prevent you from seeing some silly video are really beyond belief. The reality is that most scientists don’t mind at all if you watch the Plandemic documentary or Dr. Stella Immanuel’s speech on capitol hill; what matters is that you know going into it that this misinformation has already been disproven, and that you are armed with the understanding and data you need to work through and decode it. This presents an easy enough decision for me; my goal of helping you sort through this misinformation is best served when it is accompanied by the source material, and posting the video alongside the discussion is a no-brainer. But I think it’s a much more difficult decision for Facebook, Youtube, and Twitter, because they have to worry about the viral nature of this misinformation and the real potential for harm, and can’t accompany every repost or upload with a detailed analysis. Allowing lies to circulate without any disclaimer or precautions to protect those that are easily deceived is irresponsible and cruel; it submits to the whims of anyone with any lie to tell or anything to sell. But the very act of censoring or cautioning about misinformation also serves to reinforce the narrative of oppression; the last redoubt for conspiracy theorists is to use the very censure called down onto themselves for the unreliability of their assertions as proof of their veracity. It is a poor sort of fortress to be sure; yet there are far, far too many who see it as the last citadel of truth.
And, saddest of all, “Share to all of your Bible groups.”
We will talk about the specifics of what misinformation or misrepresentations in this video specifically might appeal to certain streams or factions within Christianity, but for the time being all I can do is grieve, as a follower of Christ, that a video or meme about the pandemic being spread primarily or at a higher velocity within Christian circles is so often a sure sign that it contains little truth and much that is meant to deceive and disrupt efforts of self-sacrifice and self-denial on behalf of our neighbors and community. I have written about how I believe the Church ought to respond to misinformation and why, but it really does feel as though we are behind the World in this area, both in our discernment and in our charity. Lord Jesus, please teach us to be as wise as serpents so that we might be as harmless as doves!
0:26 “Share with… Anybody that doesn’t want aborted fetal tissue fragments put into them.”
This is actually a major claim of the video and the most compelling topic of discussion of the three the speaker introduces, and we will cover it more extensively in just a couple of minutes. For now, let me just say that it is a fact that the COVID-19 vaccine, or any vaccine for that matter, does not contain any aborted fetal tissue fragments! Share with your Bible group, they will take this down!
It also won’t change your DNA, but we’ll get to that too.
0:40 This is the packaging of the AstraZeneca COVID-19 vaccine.
I have not seen the packaging of the AstraZeneca vaccine or any others for COVID-19 and have no reason to believe this individual photoshopped this package (and compelling reasons to believe they are not capable of doing so, as we shall see).
0:59 “It’s called Chad”
ChAdOx1 stands for Chimpanzee derived Adenovirus-vectored vaccine developed by Oxford University. The 1 means it’s the first of multiple Chimpanzee derived Adenovirus-vectored vaccines for COVID-19 that Oxford is working on.
It does not stand for “Chad- whatever that is, zero, or whatever it is- times one.”
1:19 Go to ResearchSquare.com
Research Square is a fine website, just be aware anything you read there is in pre-print; it hasn’t been finalized or peer reviewed yet. That’s the whole point of the website, for people to get feedback before they publish.
1:21 “I want you to learn to do your own research.”
The speaker claims that she wants her viewers to “do their own research” and begins well enough by directing them to Research Square, a reputable website where you can find original sources. But within about 10 seconds she has transformed “doing your own research” into something about as academic and reliable as a Wikipedia binge (or exactly as academic and reliable, since a Wikipedia binge is exactly what it is); googling random words you don’t understand and reading about them, then deciding whatyou thinkthey mean without any background or context. It’s hard to tell whether she is being intentionally deceptive here, or if she really believes that she has attained a solid grasp of these concepts through the methods she is espousing.
That’s not what research is. In the context she is using it, ‘doing your own research’ at minimum means using the amazing, abundant resources of the internet to learn more about the concepts being discussed, and then using that new knowledge to get yourself over that first hump in the Dunning-Kruger effect and figure out 1. what you need to learn next and 2. what the limits are on how much you can actually learn about this on your own. The good news is, as long as you are humble in your assessment of your own understanding, you can also use that knowledge to 3. verify the reliability of whomever you go to to learn more.
We’ve all done this before, haven’t we? When I wanted to talk to an HVAC specialist about a problem with the air supply plenum in my crawlspace, I studied the anatomy of different HVAC systems, read some discussions on HVAC forums, and watched several videos that addressed similar problems. When this didn’t fully solve my issue, I called the specialist; and I used that research, mixed with a healthy appreciation of my own general ignorance on the topic, to both improve my understanding of his recommendations and to inform my gut decision on whether to trust his expert advice or get a second opinion (for anybody who is curious, he said the squirrels shouldn’t be living in there and he’s coming out to take a look on Monday. Based on my independent research, I’ve decided I believe him… though the squirrels have been waging a fierce misinformation campaign).
I’ve written (though not yet published) about this before; I want my patients to use Google. Really. And then I want them to come and talk with me about what they’ve read so I can help them get further beyond the point they could by themselves. Like I said in the article I’ve written that nobody else has access to:
“Most of all we went to school to become very, very good at parsing information about the human body and its diseases, and when it comes to the research you’ve brought in that is the primary way I can help; by helping you sort out which information is actually going to affect you and which isn’t, which you should worry about and which you shouldn’t, and what the underlying motivations might be for the people that published it. I’ve spent countless hours looking at research and studies and clinical trials and have become very good at determining when a study design is too flawed or data is too skewed to be reliable, when there is a strong bias that makes the data suspect, or when a conclusion is not supported by the evidence as it claims. If you are a scientist or a researcher or have training in those areas you may be able to do the same, maybe just as well or better; but for most people that isn’t the case, and it would be a little silly to trust your doctor when they offer one of the services they are highly trained for, such as looking at your child’s ear and determining if there is a bacterial infection requiring antibiotics, and not trust them when they offer another service they have been highly trained for, such as telling whether the research you’ve brought in about the human body is reliable or not.”
1:28 “Don’t rely on us or anyone else, do it yourself!”
This is so subtle and clever that I just wanted to point it out briefly. “Don’t rely on us or anyone else” when doing your research is an attempt to level the playing field between the different sources you might listen to, and it seems so reasonable on the surface.. Don’t listen to me, or your doctor, or a scientist, or an epidemiologist or researcher, only listen to yourself. The problem is that, at least in the viral version of this video, we have no idea who this lady even is. Telling you not to take her word for itor your doctor’simplies those two sources of information are equally educated, informed, and reliable; this from a lady who just called it the “CHAD Zero Times One Vaccine.”
1:49 “Google every single word on here.”
Again, that’s not “research.” If you need to google some of these words to know what they mean then by all means do so; but that is the pre-research prep work, not the research itself. Thinking you understand a concept because you looked up the definition of a word is unmitigated folly, as she demonstrates in a few moments.
1:58 Recombinant DNA doesn’t mean they are reprogramming your DNA. At all.
The speaker and her assistant begin their “research” by looking up the term “Recombinant DNA” on Wikipedia. Wikipedia is great, and one of my favorite things about it is that most articles are written at a level that most lay people can understand (except the math ones. Yikes). So I think if you want to follow the speaker’s advice here and read that wikipedia article, you should. I’ll wait.
But the thing is, she doesn’t actually read it in this video, does she? She only reads the first sentence and then, despite her prior warnings, asks you to take her word on what that sentence means. But listen to the way she says it! The emphasis, the alarm, the righteous anger as she enunciates “molecular cloning” and “genome”! She spits the words out as though it were self-apparent how evil they are, without seeking (or asking you to seek) any additional understanding of what they actually mean. Just one googled word in, and she has entirely abandoned her ‘method’ of research; don’t google every single word in this article that you don’t understand, just take it on her authority that this is bad, bad stuff. She tells you earlier not to be intimidated by scientific terms; but here she actually wants you to be frightenedby them.
If you actually read that article, you will quickly realize that the idea she implies here (and stated explicitly earlier on), that recombinant DNA reprogramsyour genetic code, is actually complete nonsense. In fact, it’s exactly the type of nonsense you would expect if someone’s entire understanding of the science involved was gained through googling random words and reading the first sentence only of wikipedia articles.
The Recombinant DNA got him!
Recombinant DNA describes how the vaccines or medications were developed, not what they do once they are inside of you. Just look at the ‘applications’ section of that same wikipedia article; rDNA technology has been used to develop insulin, accurate testing for HIV, and safe growth hormone for patients with pituitary failure, not to mention interferon therapy for cancer, treatments for cystic fibrosis, and TPA, a life saving treatment for strokes and heart attacks. None of these therapies change your DNA. Saying recombinant DNA therapies change your DNA is like saying that Mashed Potatoes mash you if you eat them. No, the potatoes were mashed during the preparation phase so that they would be delicious for you later on; you don’t get mashed, they do. DNA of fungal or bacterial or animal cells waschanged in order to develop these treatments, so that they would be safe and effective for the people who need them.
Since I’m waxing eloquent here, I’ll give one more analogy. It’s like my first and only experience in debate club back during Freshman year of college. The topic was “is preemptive war justified.” The first team to debate, the “for” team, got to define the terms of the debate and chose to argue that preemptive war was justified because nations have the right to defend themselves if they are the victims of a preemptive attack; so preemptive war, “war initiated by a preemptive attack,” was 100% justified… on the part of the nation that was attacked first.
They changed the very definition of the term to suit the argument that was easiest to defend; they were arguing for retaliatoryor defensive action instead of preemptive, because it was a much simpler position to defend. And the only problem with that is that words have meanings, Keith!
Sorry, I may still have some baggage to work through there. But that’s exactly what this speaker is doing too; changing the meaning of the term ‘recombinant DNA’ and just hoping you won’t notice or indeed read the very article she has pointed you to herself.
There is one more part of this discussion, and it doesn’t have anything to do with what she’s mentioned here, but intersects with this idea of “reprogramming DNA,” even if I don’t think she has the science background to realize it. Here she’s focused on rDNA, but you’ll also hear discussion about mRNA; messenger RNA, the genetic sequences that organisms use to instruct cellular machinery to build proteins. The two vaccines that have recently shown such promise, from Pfizer and Moderna, both use mRNA technology. Traditional vaccines provoke an immune response, teaching your body to produce it’s own antibodies to fight the infection, by presenting your immune cells with non-dangerous particles of the virus that it can recognize and then build antibodies against. Each of these viral particles has to be produced in a lab and enough of them have to be preserved and injected to ensure some are picked up by your macrophages or dendritic cells and then presented to your lymphocytes (T and B cells) to make sure that you really do develop the ability to mount a robust immune response when you exposed to the virus for real later on.
The mRNA vaccines do the exact same thing, only instead of injecting the deactivated viral proteins directly into your body, they only inject a code for them; a code that teaches the machinery in a few of your own cells to build and release the proteins needed to produce the desired immunity. This outside mRNA hijacks the cellular machinery to produce the proteins needed for immunity without any of the proteins that cause illness; and the rest functions just like a normal vaccine. This is the same naturally occurring ‘technology’ that mRNA viruses use themselves. This is great news for people who want to acquire natural immunity; by mimicking the action that the viruses themselves use, which in turn produces our immune response to them, these vaccines have become the closest you can possibly get to acquiring immunity naturally without actually running the risk of getting sick and infecting others. Instead of getting a deadly mRNA virus from a cough or sneeze, you get a safe mRNA ‘virus’ from a vaccine, and from it your body’s own immune system learns how to kill the deadly virus.
This video below explains these concepts really well, starting at the 1:53 mark.
Again, this mRNA technology doesn’t change your DNA. It just sends a message to some of your cells with a set of instructions, just like any common cold would. Your chromosomes, your genetic code, are unaffected; the vaccine doesn’t even interact with them. If an analogy would help, imagine someone ‘hacked’ your network printer at the office. Normally you are the only person who prints to this printer; you write the document on Word or Notepad (judging you) on your computer and then hit “print,” and the signal goes to the printer, which prints the document. But one day you walk in to find that someone else has been printing things to your network printer. That doesn’t mean that they’ve hacked your computer, it just means they have used your paper and ink (and toner! those monsters).
And what did they choose to print? A detailed set of instructions on how to protect your networked printer from hackers. Big Cybersecurity, at it again.
3:00 “We used direct RNA sequencing to analyse transcript expression from the ChAdOx1 nCoV-19 genome in human MRC-5 and A549 cell lines.”
Here is where we enter what is, I think, the heart of what has drawn most people to this video. I think we can quickly dispense with one piece of false information before entering a more important discussion. The ChAdOx1 nCoV-19 vaccine does not use the MRC-5 cell line. This is an inherent problem with both the ignorance of the speaker (and here I do not mean to be insulting, but merely mean the lack of actual education and experience in the field in which she puts herself forward as an expert) and the deep flaw in her ‘method’ of research. This article is not from the vaccine manufacturer at all; it’s from an independent lab that used these human cell lines to study the vaccine after it was produced. You can find the full text here and read it for yourself. The manufacturers did not use those cell lines. In telling you all about the MRC-5 cell line and warning you that;
“One thing [the ChAdOx1 vaccine] definitely has is the lung tissue of a 14-week-old aborted caucasian male fetus.”
Narrator: “It doesn’t.”
the author is stating an absolute untruth based in her own haphazard and unreliable method of trying to find scientific information and uncover medical conspiracies. If her “research” methodology has left her unable to even grasp the basics of who is doing the study and why they are doing the study, or the difference between making a vaccine and studying a vaccine that has already been made, why would you possibly trust her method of research? For that matter, why trust her at all, when she has proven herself so unreliable? Even her assistant, the enigmatic Claire, tries to offer some clarification that the cell line used in the study has been replicated over and over again since the 60’s; that the researchers did not actually abort a child and then collect its cells to study the vaccine (or make the vaccine, as she mistakenly believes); but that attempt is ignored by the main speaker.
What about fetal cell lines in medical research?
Despite the speaker’s severe misunderstanding, and regardless of the tired horror tactic of trying to get you to visualize fetal parts being injected into your children in order to illicit a visceral reaction (there are no aborted fetal parts or fetal cells in vaccines, even the vaccines developed using human cell lines), this is an important question and I think we should spend some time on an actual discussion of it, instead of the sensationalized and inaccurate rage that characterizes its treatment in the video.
I am a pro-life doctor. Like most physicians my views on abortion are nuanced, deeply felt, and strongly based in the lived experiences of my patients. Since this video was designed to spark a visceral reaction among pro-life people in order to make them more susceptible to vaccine misinformation, I think the issue of abortion and fetal cell lines in research warrants discussion on this blog post. I have helped prevent countless abortions, both through providing high quality women’s health services, often to women who otherwise would not have good healthcare access, and by providing compassionate listening, patient-centered care, and judgement free counsel during the most tumultuous times of an unintended pregnancy. There are those that will argue that doctors shouldn’t be pro-life, that my moral opposition to abortion means I can never truly provide unbiased guidance and information to a woman facing this most difficult and painful decision of her life, or that I am somehow unable to respect my patients’ autonomous decision making in this area and help them leave my office more empowered than when they came in. I don’t believe that matches the experience of my patients. I might argue that informed consent, a core principle of medical ethics, is impossible without a robust patient-focused discussion of the medical realities and practical alternatives surrounding the decision to terminate a pregnancy, and that there is reason to believe that these conversations are too often sacrificed or short-circuited once the specter of abortion first arises. It is a debate for another day, to be sure, and with many of the physicians who hold the opposite view I nonetheless share a strong mutual respect, born of proven care for and dedication to our patients, that overrides even our deeply held reservations on this issue. Even on the question of abortion and consent itself, we both believe, based on all of our medical training and the high degree of altruistic concern we bring to our jobs, that we are striving to do what is best for our patients; to help them in the way that is best for them and most consistent with their own stated goals and deepest felt wishes.
Many medications and vaccines use fetal cell lines. The reason is simple; human cells typically work best for studying and developing treatment for human diseases, and fetal cells have unique characteristics that allow cells to achieve, or nearly achieve, cellular immortality; allowing the same cells to be replicated over and over again without any need for additional cell lines to be collected. There is no question that this is a challenging ethical and moral area for pro-life scientists like myself, and strongly pro-life physician and multidisciplinary healthcare organizations, like the Christian Medical and Dental Alliance (CMDA), have discussed and written extensively about it. Here are a few articles CMDA has published, written by conscientious physicians of deep, theologically sound Christian conviction. I hope you will weigh their words and reflections with at least as much gravity as a random person on the internet telling you to “pray big” and share her video with as many “christian-loving” people as possible.
There are a few salient facts you should know about this area of medicine.
No children are aborted or have been aborted for the purpose of developing medicines or vaccines. The sensationalism that some forces in the anti-vaccine movement are willing to engage in knows no bounds, and it is not uncommon to hear the propaganda that these unborn babies were actually aborted for the purpose of being used in medical research. This is simply wrong. The few unborn children whose cells (or accurately, copies of copies of their cells) are regularly used in medical research and development were likely aborted for the same reasons that most abortions occur; the unbelievably difficult balance of perceived goods and anticipated challenges faced by a woman who had not intended to become pregnant. These mostly occurred in the 60’s and 70’s, and cell lines (copies of cells) derived from those same aborted fetuses have continued to be used ever since without the ‘need’ to derive new cell lines from abortions occurring today. For instance, HEK 293, the actual cell line used in the development of the ChAdOx1 vaccine, was derived from an abortion in The Netherlands in 1973; we simply do not know the story of the woman who chose to have this abortion, or the reasons behind her choice.
There are no fetal cells in vaccines; not even in vaccines developed using fetal cell lines. Vaccines are not a ‘mix’ of fetal cells and viral particles, not by any stretch of the imagination. When fetal cell lines are used to grow viruses that infect humans in the vaccine development process, it is distant to the final product of the vaccine, which has also been through multiple rounds of purification. The human cell lines are used to grow the virus and deactivate it; they are not included in the actual material injected through a syringe to produce an immune response in our bodies.
Not all vaccines use human cell lines. There are vaccines for almost every vaccine preventable illness that are designed using methods that even the most rigorous pro-life groups consider ethical. When the anti-vaccine movement tries to convince you that all vaccines are suspect from a pro-life perspective, they are rather co-opting a pro-life position for their own aims rather than being a legitimate part of the pro-life movement.
Like the CMDA doctors above and most pro-life physicians and scientists, and even the Vatican, I believe that using vaccines and medications not developed using fetal cell lines from aborted human beings is strongly preferable whenever possible, and that this is an area where continued economic and moral pressure can encourage pharmaceutical companies and research institutes to pursue alternative means of developing novel treatments to human disease. However, the principles of whole-life pro-life ethics also dictate that a treatment or preventative measure developed in part through material derived from a past harm through abortion, with no potential to cause further harm in this same way but massive potential to prevent loss of life (including unborn human life) is still, clearly, a moral good; a position even Popes have affirmed. In saving the lives of a great many people from a single death that would not have been prevented regardless, we derive the greatest possible moral good from what was an undeniably tragic situation for all involved.
For pro-life persons, accepting a vaccine that was developed from fetal cells collected 50 or 60 years ago makes them neither complicit with nor promoting of a depreciation of human life. But seeking treatments developed using alternative means may send a message to pharmaceutical companies that these issues are indeed dear to their hearts and that their collective will is that these methods in research would become a thing of the past.
4:23 “This is what they want… They KNOW this vaccine is going to hurt people or kill people so badly.”
A few things here.
If there is a way to kill people not so badly, please let me know. We could be on the brink of a medical breakthrough here.
Who is “they” anyway?
She jumps around so much in this video that the viewer is left to assume, just like with the MRC-5 discussion, that this last bit is screenshot from the original papers from the vaccine manufacturer; that the people making the vaccine have, in their published study, asked the universe at large to supply them with some sort of computer program or something to help them sort through all the people they intend to maim or kill. We’ve talked before how conspiracy theories rely on this weird paradox where shadowy conspirators are both incredibly clever, subtle, and nigh-invulnerable but alsoso clumsy as to announce their real plans in such a way that some random person on the internet can piece it all together with a 5 minute video. Pfizer or Moderna publishing “please help us, our excel spreadsheets aren’t robust enough to keep track of all the victims we are after” at the bottom of their research would certainly fall under this phenomenon.
But this isn’t from the vaccine manufacturers. It’s from the Medicines and Healthcare products Regulatory Agency (MHRA), the British counterpart of the FDA. And it isn’t from a research paper, it’s from their contracts division, announcing the technology services they are hoping to contract with as they anticipate the release of these vaccines.
Why would the MHRA or FDA want to track possible adverse reactions to a new vaccine? Because it’s literally their job.
And why would they anticipate a “high volume” of reported adverse reactions? Because we are in the middle of a highly politicized, deeply contentious global pandemic; billions of people are going to get these vaccines, and some of them are going to have very mixed feelings about it. Adverse reactions to vaccines range from the common but mild to the serious and extremely rare, but reported or perceived reactions are all over the place. I saw a patient yesterday who believed that his flu shot had caused him to feel fatigued and sore the next day (it had), and also to have six days of diarrhea and loss of taste and smell two weeks later (it hadn’t). He tested positive for COVID-19, the true source of his symptoms. I’ve also had patients who believed their flu shot gave them COVID-19, which is utterly impossible.
Vaccines feel scary; they are sciency and mysterious and they are going into your body, and you are taking someone’s word for it that they are safe and a wise decision. I get that. A new vaccine is even scarier, and a new vaccine for a virus that is deadly, has changed our entire lives over the past year, and is surrounded by a thick haze of misinformation and conspiracy theories is even scarier. Some of the folks getting that vaccine are going to do so, probably to keep those around them safe, only after warring within themselves over it (even I told you I’ve still got some research to do before I’m fully satisfied with the decision). For some of those folks, anything medical that happens to them in the next few months might potentially feel like the negative fallout of that one difficult decision. The point of the MHRA using an AI tool to augment their ability to analyze that data is so that they don’t miss any real adverse reactions hidden in all of that noise; to make sure that if the vaccine is dangerous after all, despite the safety demonstrated in clinical trials, they discover it as quickly as possible. Again, because that’s their job. This is evidence that the people tasked with making sure the vaccines are safe really do take that role seriously; not evidence that someone is planning to hurt you and wasn’t sneaky enough in hiding their intentions.
5:01 “I don’t know how you do it, I’m not technical.”
After watching the same 5 minutes of these folks pointing a shaky phone camera at their computer screen and pulling up various image preview programs and web browsers over and over again while writing this blog post, I can now verify that this is the single most true and reliable statement in the entire video.
It looks like I’m just being cheeky at this point, so I guess it’s time to stop there.
The following is a short repost from social media.
Well, call me triggered.
I’m a Family Medicine Physician, and every day for the past 3 months I’ve seen patients for COVID-19. Every day for 3 months, I’ve told every patient I’ve diagnosed with COVID-19, with the exception of the few I’ve sent directly to the hospital because of the severity of their symptoms, the same three things:
1. Don’t be afraid of COVID-19.
I say this to my patients for a few reasons. First, because I am mostly seeing patients in the outpatient setting, my patients and I have the privilege of emphasizing this point. Second, for many patients who have a mild to moderate severity course of COVID-19, anxiety is a very real issue, and I want to make sure that while they are recovering they are not sitting at home wondering when the virus is going to get them. Most people who get COVID-19 don’t end up in the hospital (as we have been saying since the beginning of the pandemic), even fewer end up in the ICU or die from the virus (as we have been saying since the beginning of the pandemic). The virus is very, very dangerous, but our brains are bad at statistics; just because this is the most dangerous viral pandemic since the Spanish Flu of 1918 doesn’t me that your individual chances of dying are high or that getting deathly ill is a foregone conclusion. If I were mainly seeing very sick patients in the hospital or ICU I wouldn’t be saying this as much; we would be talking more about treatment and response than about the patient’s anxiety about getting sicker, though the latter certainly deserves our time and attention in any clinical setting. When a patient is struggling to breathe, “don’t be afraid” is a theological statement rather than a clinically valid reassurance, and it typically gives way to “I am with you; I am here and I am going to do my absolute best for you.” But in the outpatient setting, talking with patients who are worried about how COVID-19 will affect them and their children and their friends, “don’t be afraid” is an extremely important part of the conversation.
2. If you have the following symptoms, go to the hospital.
As important as “don’t be afraid” is, it is equally as important to talk about what we call emergency and return precautions. Yes, for most people COVID-19 is not deadly; but it is for some, for many in fact, and we do not have any perfect way of predicting who will have a more severe course. For my healthy patients in their 20’s and 30’s, the chances of ending up severely ill are extremely low; yet people who are medically just like them- same age, same paucity of risk factors- have died from the virus. The same for parents who are worried about their children; children are at extremely low risk from COVID-19, yet some children have died from the virus. I can look my young, healthy patient in the eye and honestly tell them I expect them to be fine; but I cannot promise them that they will be, and that’s a vital distinction. So with each and every patient, in addition to reassurance, we talk about what to look out for. Shortness of breath. Chest pain. Severe malaise and fatigue, even syncope; passing out or almost passing out from the toll the virus is taking on your body. We talk about oxygen levels if they happen to have a pulse oximeter at home, and signs of hypoxia if they don’t. We discuss both the reasons they would come back to see me in clinic and the reasons they would skip my clinic and go directly to the Emergency Department instead. With my older patients or patients who have known risk factors (most Americans, in fact, including myself, considering that risk factors for a more severe course of COVID-19 include hypertension, diabetes, obesity, chronic lung disease and other very common ailments), this discussion is even more important, because even though the odds are still in their favor, their ending up in the hospital or dying from COVID-19 is not nearly as unlikely. I want my patients to be free from fear; but I also want them to be equipped with the knowledge they need to make sound choices if their symptoms do worsen.
3. Please keep the virus from spreading to others.
This piece of guidance is no less important than the previous two. If you are healthy and young and your chances of dying from COVID-19 are very low, that’s really wonderful; but self-isolation during your illness is still the responsible, kind, and charitable decision because not everyone is as lucky as you. The case fatality rate of COVID-19 is much higher than even very deadly illnesses like the flu, and it is very, very contagious. With each and every patient I discuss the precautions they can take to keep the virus from spreading to their own family, and of course the responsible social decisions like sheltering at home during their contagious window and alerting their close contacts so they can self quarantine. It’s one thing to tell yourself that you’ve only exposed other people at similarly low risk to yourself, but once you have spread the virus to someone else you have no control of whose grandmother, whose father in poor health, or whose immunocompromised child it spreads to from there. I said before that we are bad at intuitively comprehending statistics; the COVID-19 virus, like most illnesses, is unlikely to cause death to any given individual regardless of risk factors, but is extremely deadly in aggregate; containment is still our best strategy for keeping the 210,000 deaths in our country from doubling or tripling by the end of this pandemic. The reality is that most people get this; most people I talk to understand the need and are concerned about keeping their families and communities safe. But there is a counter-narrative being promoted by some that rejoices in defying all calls for caution, sober mindedness, or charity when it comes to COVID-19, and so the reminder from me, the doctor actually seeing the patient face to face in clinic, becomes that much more important in case my patient has been lured by these cruel and irresponsible ideas.
These are the three pieces of advice, the three categories of discussion that I have with each and every patient. It is time consuming; it appropriately turns what might be a 5-8 minute visit into a 10 or 15 minute visit. It requires careful explanation of statistical and clinical concepts that might be challenging. It is worth it, because the proper way to approach a diagnosis of COVID-19 is with caution on behalf of others and preparedness rather than fear for yourself and your family, and it’s my job as a Physician to equip my patients with the knowledge and tools they need to approach the virus this way, even in the face of anxiety and rampant misinformation.
So when I see someone with a platform like President Trump’s endorse the firstpoint of not being afraid of the virus, follow the secondpoint of going to the hospital when his symptoms escalated and he experienced hypoxia and shortness of breath, and finally utterly disregard and contradict the third point of taking precautions on behalf of others, I am, I think very understandably, upset. Because when a doctor or a nurse survives COVID-19 (and many haven’t), contracted by putting themselves in harm’s way every day and despite taking maximum precautions to keep themselves and those around them safe, they rejoice that they are now able to dive back into the fray, fighting the virus with no less caution but somewhat less stress and anxiety for their own health, knowing that reinfection is very likely a rare occurrence. But when the president contracts COVID-19 by ignoring all precautions and survives it with the help of state of the art high-level hospital care, expensive and experimental treatments, and a private team of doctors and nurses, his first statement after leaving the hospital is one that builds upon his long-standing guidance and example of not taking precautions or acting to protect those around you, despite neither you nor your family and community having anything like the medical access that helped him.
Please keep yourself and others safe. Don’t be afraid of the virus, but please act in charity to those around you by taking reasonable and proven precautions like wearing a mask, maintaining physical distancing, and engaging in sound epidemiological principles like getting tested if you are ill, self-quarantining if you are exposed, and honestly and proactively participating in contact tracing if you are diagnosed.
Edit #1: I will go ahead and anticipate a couple of objections to this post. First, some people are going to claim that the facts I’ve shared here are inaccurate; that the ‘CDC admitted’ that only 6% of the deaths were actually from COVID-19, or that the fatality rate is actually lower than the flu, or some such nonsense. For people who still believe these pieces of COVID-19 misinformation, there is no shortage of good explanations and rebuttals available on the internet and I suggest finding and reading one. For people who don’t mind a long and mediocre rebuttal over a good one, I’ve written a few myself over at tjwebbmd.com.
Second, some people are going to look at this tweet from the president and say, “but TJ, he isn’t discouraging caution or telling people to take COVID-19 less seriously! He just said don’t let it dominate your life, that could mean lots of things!” To those people I will say, along with Doctor Archibald from Veggie Tales, “Stop being so silly!”
When I tell my patient “don’t be afraid” after reviewing their vital signs, asking about their symptoms, carefully examining them and listening to their heart and lungs, and carefully talking through emergency precautions and transmission control measures, they are absolutely not confused about what I mean. And nobody in America is confused about what the president means when, after months of promoting misinformation, minimizing the pandemic, shirking transmission control guidelines even to the point of endangering his secret service and staff during his own illness, refusing to wear a mask (and then only wearing one intermittently and with a wink at mask truthers when he does), he then says to ‘not let it dominate your life’. And nobody will be surprised when the ongoing unwillingness of our national leadership to take the pandemic seriously, and encouraging others to do likewise, results in more cases, more severe illnesses (and associated suffering and medical debt), and more deaths.
Edit #2: On the same day that I posted a short essay titled “Don’t Be Afraid of COVID-19”, Dr. Emily Smith, Your Friendly Neighborhood Epidemiologist, posted a short essay saying that Yes, We Should Be Afraid of It. Now, Dr. Smith is so much smarter than me that this would normally be enough to make me immediately delete my post; but thankfully, it turns out we are saying essentially the same thing, despite the seemingly contradictory essay titles. To understand what Dr. Smith and I mean when we say you should/shouldn’t be afraid of COVID-19, go and read her essay where she discusses the difference between unhealthy fear and wisdom, the latter being something our national response to this very deadly and dangerous virus has been sorely lacking.