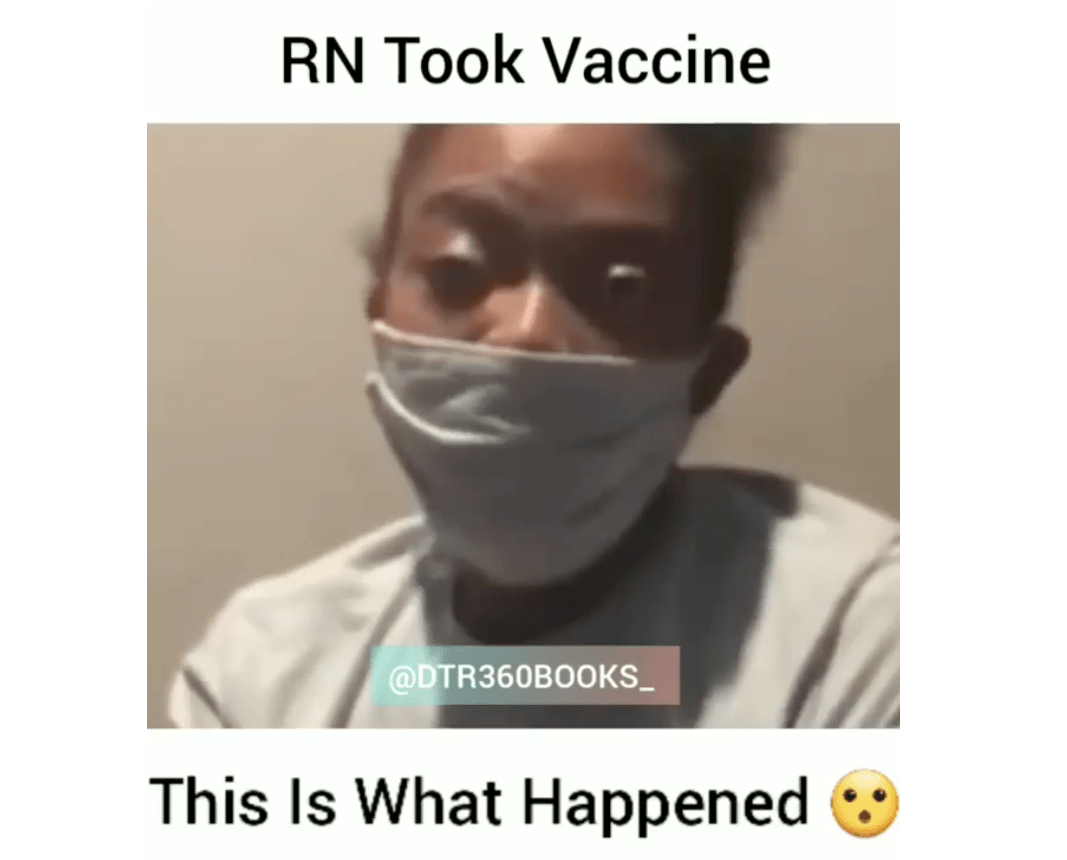
When a friend sends me a video about a vaccine reaction and the next day multiple patients mention the same video to me in clinic, it’s probably time to watch it, and write about it. The video I’ve linked to below is of a registered nurse named Khalilah Mitchell who lives in Nashville Tennessee, who warns about developing Bell’s Palsy, paralysis of one side of her face, after receiving a COVID-19 vaccination. It is impossible to watch the video without empathizing with her, and I encourage you to watch it if you possibly can; I’ve supplied the link below, assuming it’s still up.
Video: RN Took Vaccine: This is What Happened
Instead of going through it minute-by-minute like we’ve done so often in the past (it is very short, at just one minute and twelve seconds), I want us to dissect a few different aspects of this.
Contents:
Healthy Incredulity
Bell’s Palsy: Medical Facts
Bell’s Palsy: Why I Wish She Were My Patient
Healthcare as War on Black Bodies
Healthy Incredulity
I want to start by stating that I believe this person’s story, for reasons we will get to in a moment. I think that when we develop the disposition to refuse to believe people’s stories about themselves and their experiences we place ourselves in grave peril. This is one of the common and insidious effects of the disinformation campaigns (both medical and not) that we have seen escalated over this past year; whenever someone hear’s something that doesn’t fit into their chosen narrative, they can simply say “but how do we even know if that actually happened?” Certainly, when someone (I won’t name names) consistently proves themselves to be a source of falsehood, their word becomes worthless; but to automatically treat a stranger that way, especially a stranger who is clearly hurting, is to shut ourselves off from compassion and reason in the name of protecting our own biases.
This individual is clearly distraught and deserves our empathy. But there is a balance and a tension here, because the 340,000 people who have died from COVID-19 in the US, and the 1.8 million people who have died from it around the globe, and their families and friends and communities, also deserve our empathy; and so do the many more who are still at risk. We can love both, and that may mean accepting someone’s narrative about themselves and their experiences without agreeing with their scientific conclusions. And that’s ok.
And so while I believe this person’s experience, I would be remiss if we did not start with a very brief survey of what we do and don’t know to be true from this video, for the sake of encountering this sort of viral information with our eyes fully open.
- We know this woman has Bell’s Palsy, or at least has visible symptoms consistent with that diagnosis.
- We know she is an African American woman, a group who among all demographics in the US probably has the most reason to be cautious and skeptical towards the medical field.
- She identifies herself as Khalilah Mitchell, a Registered Nurse in Nashville, TN
- The Tennessee nursing board does not have any record of a registered nurse by that name.
- She reports that she developed Bell’s Palsy shortly after receiving the COVID-19 vaccine.
- We do not have evidence that she received the COVID-19 vaccine.
Let’s talk about that 3rd bit, which has been homed in on by multiple fact-checking sites. There are multiple reasons Khalilah Mitchell might not be listed on the Tennessee nursing board’s online records:
- She may be a recent graduate or have recently received her license in that state; we don’t know how long it takes for those licenses to be searchable online.
- We are in the middle of a pandemic; she may be a nurse licensed in another state who has special permission or an emergency/temporary license to do travel nursing in Nashville.
- She only states in the video that she is “in Nashville Tennessee.” She may well be licensed in and work in another state while living in (or even visiting) Nashville. This is not uncommon.
- She may go by Khalilah but actually have a different legal first name; Khalilah may be a middle name or a nickname.
- She may be Khalilah Mitchell but be registered under a different last name because of a recent marriage, divorce, etc; changing your name on your nursing license is a beast of a process, as my wife can tell you first hand.
- She may be using an assumed name or placing herself in a different city and state, or both, to protect herself from reprisals in case this video goes viral (which it has).
- She may be lying.
Only one of those reasons, all of which are feasible, negates her story; only one causes us to mistrust the only unprovable/non-falsifiable aspect of her story, that she did indeed receive the COVID-19 vaccine prior to developing her symptoms.
Sadly, hiding among the many people with legitimate fears and uncertainties about healthcare in general and vaccines in particular, there are dishonest people who are not above creating misleading and blatantly false information to deceive others. If this person were a known producer of anti-vaccine propaganda, disbelieving her entire story would be warranted; but I have no reason to believe that’s true, and thus have no reason to disbelieve her story, as some have done, merely because certain aspects of it cannot be verified.
So I believe her story. However, because there have been and will continue to be elaborate, malicious attempts to deceive the public about these COVID-19 vaccines, I believe we are justified in maintaining a healthy degree of incredulity each and every time we encounter one of these types of videos; the intellectually honest and important work of discerning whether the information presented is true in no way negates or cheapens our compassion for the speaker.
Bell’s Palsy: Medical Facts
I want to talk about the clinical side of medicine, and the human side of medicine. In reality we can never separate them, but we can compartmentalize them for a few moments for the sake of discussion.
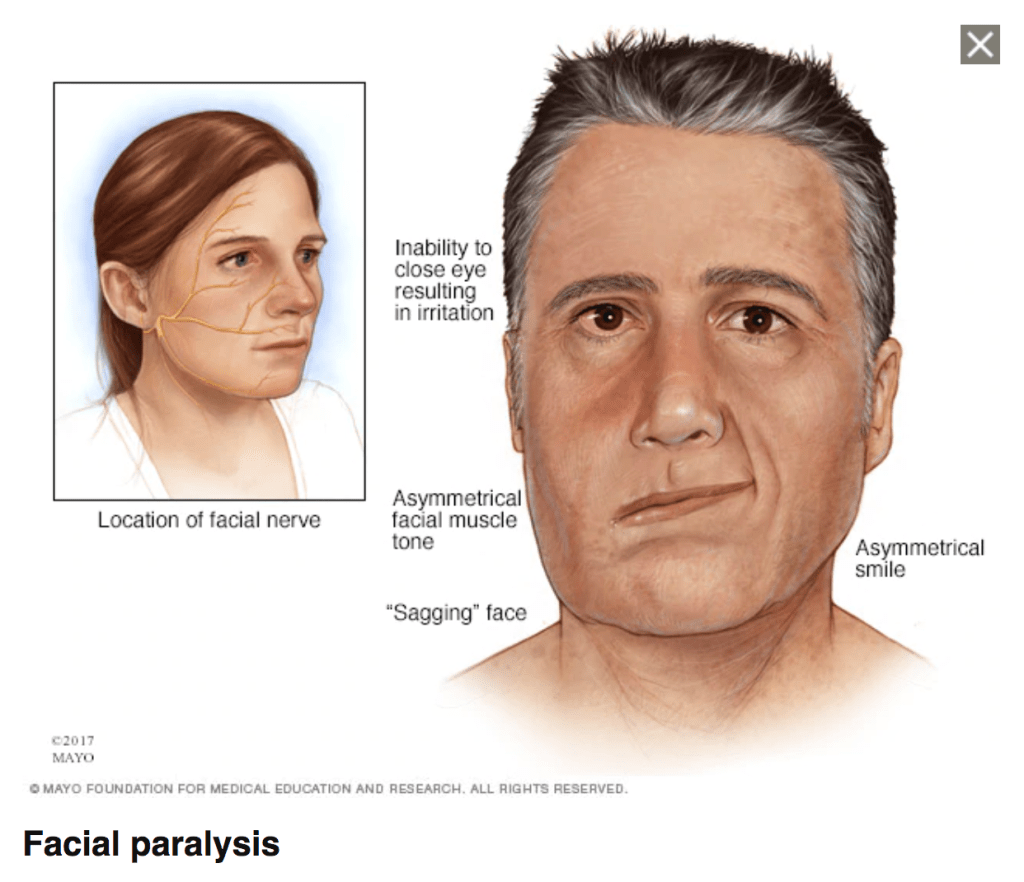
Bell’s Palsy is a temporary paralysis of the Facial Nerve, the seventh cranial nerve which controls the muscles of the face. This paralysis occurs without warning, usually gets worse over 2-3 days, and then starts to improve after about 2 weeks. Usually it is entirely improved by 6 months and does not cause long lasting symptoms; but sometimes it does, and the extent of damage to the nerve likely plays a role in the symptoms lasting longer. The cause is unknown. It’s an area researchers have studied for years. A leading theory is that, like shingles, it is caused by a reactivation of a herpesvirus that lies dormant within your nerves. In that case it can be triggered by any compromise of the immune system, but also by physiologic stressors; it has been associated with diabetes, high blood pressure, pregnancy, acute viral infections, and vaccines, all of which tax the immune system (the latter two temporarily). Another theory says it is the immune system itself, in the act of fighting the virus, that causes ‘friendly fire’ damage to the nerve, and this would also explain why it is not just associated with herpesviruses but with other viruses like flu, hand-foot-and-mouth, common colds, and even COVID-19 infection itself. The immune system is also activated by vaccines (that’s how they work; they teach your immune system how to fight new viruses and bacteria it has never seen before), and so also have the theoretical potential to cause Bell’s Palsy, though careful studies have not supported an actual link between vaccines and this condition. But these are still just theories, and we don’t actually know. I treated a patient last week whose Bell’s Palsy, as far as we can tell, occurred seemingly at random.
So, do the COVID-19 vaccines cause Bell’s Palsy? It’s a difficult question to answer. In the vaccine trials, the rate of Bell’s Palsy was incredibly low: 4 in the Pfizer trial and 3 in the Moderna trial; 7 cases out of over 70,000 participants. That’s less than half the normal rate of Bell’s Palsy in the general population, which is about 35 cases per 100,000 people. The rate was higher in the vaccine group than in the placebo group, though the numbers are far too small to draw definite conclusions.
If I were to sum up the evidence for my patient or my family member, I would tell them this; getting the COVID-19 vaccine might carry a tiny increased risk of developing Bell’s Palsy compared to not getting the vaccine; but the risk is still about the same overall as it would be just going about your every day life.
Maybe that feels like a paradoxical answer, but truth is often like that. About 40,000 Americans have had Bell’s Palsy this year; very, very few of them have had the COVID-19 vaccine, but those that did may blame it on the vaccine. Those who didn’t may blame it on something else; another illness, their flu shot, stress. They may be right or they may not be, but until we understand the condition better there is simply no way to perfectly avoid it, and it is so rare and typically so benign a condition in the long run that basing our medical decision making on it is unreasonable, both as physicians and as patients (and please remember, I am both, just like every other doctor you know). If you get the COVID-19 vaccine, you are extremely unlikely to develop Bell’s Palsy; no more or less likely than you are to develop it in the coming year anyway. What you are much, much less likely to develop is a severe or fatal case of COVID-19.
Bell’s Palsy: Why I Wish She Were My Patient
Reading that last section, you may think I’m going to say “I wish she were my patient because I could help her understand that her Bell’s Palsy probably wasn’t from the COVID-19 vaccine.” Um, no. My experience has taught me that, for better or for worse, once someone has formed a firm mental association between an event or intervention and deeply distressing symptoms, that association is incredibly difficult to break; even when there is absolutely no plausible link between the two, which is not the case here. Not to digress too far, but I commonly try to break those associations in exactly two situations: first, when my patient has linked their negative experience (or that of a loved one or friend) to a medication or treatment that is actually going to be life-saving for them, or relieve a great deal of their suffering, and there is actually no causal link between them. And second, when the patient has incorrectly linked a negative medical outcome to some perceived failure of theirs. I have at least one or two conversations a month with women who have had miscarriages and have definitely assigned the blame for that tragedy to themselves for some action or omission that couldn’t have caused it; some bump they went over on the road a few days before, a drink of alcohol or a cigarette they smoked before they knew they were pregnant, getting their nails done or taking a dose of an over the counter cold medicine. We spend a long time talking about the causes of miscarriage, because if possible I want to help them let go of that shame and self-blame they’ve have been carrying, and will carry, their entire lives. Those are the circumstances where it is worth it to me to really try to convince my patient that the medical facts really do override their perceived association. With this woman in the video, if she were my patient and we developed a trusting relationship over many years, maybe at some point we would be able to have a frank and honest discussion, looking back, about whether or not that Bell’s Palsy was really caused by the COVID-19 vaccine, and help her loosen that association; but telling someone who is suffering “you are probably wrong about why you are suffering!” is not just an exercise in futility, but a failure in empathy as well.
No, the reasons I wish she were my patient are twofold; first, because I treat Bell’s Palsy all the time and there really are some things you can do to give the patient the best possible chance at recovery. There’s evidence for early steroids and anti-virals, and there are supportive care measures, like synthetic tear eye-drops, to protect from some of the potential long-term complications. We also talk about adjunctive treatments like facial massage, stretching, and facial muscle exercises that have never been proven but are not likely to do any harm either, and will help the patient feel they are an active participant in their treatment (I am always explicit about that last goal; we are not trying to ‘trick’ the patient into thinking they are helping to make them feel better). I print handouts for my patients all the time to help guide their own reading and research at home, and have one I like for Bell’s Palsy because it carefully explains the possible causes, the symptoms, and the prognosis. Medically, Bell’s Palsy is somewhat satisfying to treat because it usually does get better, and in general walking through an illness with someone as it improves is a lot less of an emotional burden for me than sitting with someone in the grief and pain of an illness that isn’t going to improve, which is vital work I wouldn’t give up, but is laden with moral injury.
And second, I wish I were her doctor because in this video she is clearly emotionally distraught. That is the aspect of this illness that the fact checking sources have seemed to ignore; the fact that this illness is incredibly distressing, even though it does have a good prognosis. I have read article after article in the few days since this video came out explaining that 1. the vaccine didn’t necessarily cause the Bell’s Palsy, and 2. it doesn’t matter because it’s a benign condition. But watch the video; it definitely matters to her. The embarrassment of having half of your face paralyzed, but people thinking you’ve had a stroke when you haven’t, of feeling self conscious everywhere you go; a condition can be benign medically but not benign psychologically, socially, or emotionally. When I visit with a patient for a condition like this, our time together is spent as much in counseling as it is in devising a medical plan. We sit in that sorrow, even as we provide hope that it will be short-lived. We offer reassurance but we know that our patients are not thinking about the low rate of long-term complications when they look in the mirror and see a face they don’t recognize. It’s hard. Maybe Khalilah Mitchell would still have been this distraught after our visit for her Bell’s Palsy, and maybe she would have felt some solace and reassurance; I can’t say. But as a physician, when I watch someone who is absolutely grieving over their medical condition, my heart goes out to them and I wish we had the opportunity to just sit down and talk about it.
These vaccines are the best hope we have of ending the pandemic compassionately, with less loss of life. I believe in them. They are safe, and your chances of developing a significant reaction- including Bell’s Palsy- is incredibly low. I absolutely disagree with Nurse Mitchell that these vaccines are “the worst thing ever”. She is very understandably thinking about her own symptoms and not about the millions of lives they will save. Yes, as a medical professional there is a tension between our own distress and the need to think of others before spreading information that can cause harm, as this video certainly will; as a Nurse, she may indeed be failing in her calling to care for the vulnerable by disseminating claims about the vaccine based only on her own negative experience and not on solid scientific facts. But that’s her right as a patient, and the reality is that most of us will put our own anecdotal experiences above facts when push comes to shove; if this video is sincere, then she sincerely believes she is doing the right thing by trying to protect others from what she has suffered, as ungrounded in the medical realities as that concern is.
As a human being created in the Image of God, Khalilah Mitchell deserves our empathy and compassion for what she is going through first and foremost, even as we work to undo the harm this video is going to cause.
Healthcare as War on Black Bodies
There is one last, vitally important issue that comes up in this video, and if you are privileged to have a long history of the medical field treating people who look like you extremely well, as I am, it may be so subtle that you miss it entirely. Towards the end of this short video, after discussing her personal distress and her opinion that the vaccines are terrible, she closes with this heartfelt appeal,
“Please, America, They do not care about us. Do not take this vaccination.”
I will not claim to speak for her, or to make assumptions about who she includes in “they” (big pharma? medicine? doctors? She states she is a registered nurse herself, so I do not think she can mean the entire medical field), or who she includes in “us.” Certainly she addresses all Americans, but we would be naive to think that her message of “they do not care about us” would resonate equally with everyone. People who have historically experienced and currently experience inequitable medical treatment, poorer access to high quality care and lifesaving treatments, systemic discrimination, and even therapeutic, malicious medical experimentation are going to understand this video in the context of a shared cultural narrative that already teaches that you cannot trust the medical field to have your best interest at heart. This includes women, LGTBQ+ persons, the disabled, those who are obese, non-native English speakers, Hispanics, Native Americans, and at least one group Nurse Mitchell seemingly belongs to herself, African Americans. If you need evidence of this, the instagram tag on this video, @DTR360BOOKS_, is connected to an online bookstore that specializes in works about racial justice, black empowerment, and racial conciliation. If anyone, and particularly any white people, are asking why this one minute video has been shared hundreds of thousands of times on social media, read on.
Before you click over to the ‘About the Author’ page, I’ll let the cat out of the bag; I am a white, able-bodied, English speaking male (I am not neurotypical [ADHD], but I know few doctors who actually are). Healthcare justice, especially in the area of race, is something I was able to casually ignore for a long time because it simply didn’t affect me. But it affects my patients every day (and because of that it certainly makes my life harder too, though obviously to a lesser degree), and in the last few years it’s an area I’ve come to learn more and more about. Suffice to say, I absolutely do not feel adequate to the task of writing about this topic; but I am going to try anyway.
The long history of medical experimentation and abuse of African Americans, of which the notorious Tuskegee Syphilis Study is only a link in the chain, is documented in historian Harriet Washington’s book Medical Apartheid, and elsewhere. If you have time to read this long and rambling blog post you definitely have 7 minutes to listen to her explain the connection between this long history (the word “history” does not here imply that it is over, as the recent COVID-19 death of one of my Black Physician sisters tragically illustrates) and the skepticism, doubt, and fear about the COVID-19 vaccines that exist in communities of color.
Race And The Roots Of Vaccine Skepticism
Of all the wisdom she shares in this brief interview (you should really read her books), this is the one that I think is closest to our purpose:
“I think this is a good thing to do because I think this vaccine looks as if it’s going to be safe, efficacious – just what we need. So anything that’s done in terms of encouraging African Americans to benefit from it, too, I think is a good step. However, it’s not a substitute for reforming the health care system. If we don’t reform the system, if we don’t make real, large steps toward addressing the inequities that cultivate distrust, then we’re going to have to do this every time we have a new health initiative. That’s a complete waste.”

Because of the systemic healthcare discrimination and poorer access that Black Americans still suffer from today, the COVID-19 pandemic has specifically devastated those communities, causing a disproportional number of deaths and severe illnesses greater than in any racial demographic besides hispanic/latino persons, and far greater than the impact on white communities. It is not hyperbole to say that African American communities are among those that need very high rates of COVID-19 vaccination the most to stem the tide of this pandemic and prevent further loss of life. And yet, the long history of broken trust on the part of the medical field is now paying dividends, and many in the communities that need the vaccine the most are reasonably mistrustful of a great deal of medical interventions; and especially of anything that seems new or experimental.
There are a great number of reasons to trust the safety and efficacy of the COVID-19 vaccines; they are outside the scope of this post, but I am addressing this piecemeal in my COVID-19 Vaccine Q&A. Just as Nurse Mitchel believes based on her very distressing personal experience that it is good to encourage people to avoid the vaccine, I believe based on the overwhelming scientific data that it is good to encourage my patients, friends, and family to get vaccinated. But Harriet Washington’s work was instrumental in my deciding to get the vaccine myself, which I did last week.
I am low risk, and would much rather have reserved my dose for one of my patients who needs the vaccine more than I do. I’ve written about this tension at length, and the great discomfort I have in receiving any medical treatment not available to all of my patients. But ultimately it was this quote from Medical Apartheid that made me decide to get vaccinated:
“Western physicians have adhered to a long and noble tradition of following animal studies with limited self-experimentation by researchers. This tradition may not always have been prudent, but by testing substances or procedures on themselves before experimenting with appreciable numbers of human subjects, doctors symbolically conveyed their belief that the measures were not inordinately harmful and also signaled a researcher’s willingness to share the risks as well as the glory of discovery.”
I am not a vaccine researcher, and there is no glory at all for me in people getting these vaccines. But they will protect my patients from COVID-19, and I deeply believe that as a medical field our solidarity with our patients, especially those who have been historically and actively marginalized by the medical industry, is an essential component of rebuilding trust. That means not only saying something is safe and encouraging our patients to have it done, but whenever possible taking on the potential risks within our own bodies alongside, and when necessary ahead of, our patients.
Yesterday two patients asked me about the COVID-19 vaccines and about this video specifically, both of them African American. In each case we talked about Bell’s Palsy, the vaccine safety trial data, the way vaccines work, and the history of medical abuse of Black folks in America; a condensed version of the contents of this blog post. We also talked about my experiences getting the vaccine, and my definite conviction that I would never ask my patients to consider a medical intervention I wouldn’t be willing to have done for myself or my family. Both left considering the vaccine, and at least one had definite plans to get it as soon as it was available. I am thankful, because both had risk factors for COVID-19 independent of the risk factor of belonging to a group marginalized by the healthcare sector.
This viral video is going to convince a lot of people not to get vaccinated. It shouldn’t, as we’ve discussed, but it will. My getting vaccinated will convince only a very few to get vaccinated themselves. But if I can show the band-aid on my arm to my patient and look them in the eye and tell them I believe so strongly that these vaccines can help protect our communities that I’ve had it done myself, maybe it will help a few. I can’t look you in the eye through this blog, but I hope you hear my heart, and I hope you decide to get the vaccine yourself to protect those you love and your own community, just as I’ve done.
