It’s rare for me to be able to muster the time to write two misinformation blog posts in the same month, let alone in two days. Between moving across the country, fighting a global pandemic (still), and the unbelievable amount of take-home work created by practicing Family Medicine five days a week, it’s unfortunately a lower priority than I’d like for it to be. But when friends all over the country send me the same video and a friend in Louisiana, which is utterly overwhelmed by COVID-19 right now, posts it as proof that vaccines are ineffective and dangerous, watching and dissecting the video becomes a higher priority.
For those of you who would prefer a quick 8 minute video in response to this quick 6 minute video, I’ll refer you over to ZDoggMD. We cover some of the same ground and he is much, much more fun to listen to compared to reading however many thousand words I can manage to write this evening.
A few preliminaries. Dr. Dan Stock practices Family Medicine (the same specialty I practice) in Hancock County, Indiana, just east of Indianapolis. Unlike many early medical misinformation sources, he appears to be fully licensed. His website is currently down (no doubt flooded with new patients in the wake of this viral video) so there is no way to know if his practice is evidence based in its approach to science and medicine. His speech here is to the Mt. Vernon school board… Sorry, “Community Education Corporation.” It’s essentially a rapid-fire review of misinformation we have seen shared throughout the pandemic, up to and including the recent misinformation regarding the Massachusetts “Outbreak.”
Many people still see the removal or censorship of any misinformation, no matter how dangerous or how full of lies and half-truths, as proof of it’s absolute validity. I have mixed feelings on taking down these misinformation videos, but since my (self-appointed, unpaid) job is to debunk the videos and my preferred method of doing so is going through them minute-by-minute, I tend to include a direct link to them on my blog posts. It’s the method I personally find most convincing, and that I believe best arms others with the information and insight they need to engage in conversations about viral misinformation like this with their friends and relatives.
The Video: Dr. Dan Stock at the Mt. Vernon Community School Corporation
Contents
Introduction
Video
Minute-By-Minute Breakdown
Minute-by-Minute Analysis
0:25 “We’re getting our information from the Indiana State Board of Health and the CDC, who don’t read any science.”
In my opinion Dr. Stock has severely harmed his credibility here within the first 30 seconds. By stating that the Center for Disease Control, a federal agency comprised of researchers, epidemiologists, laboratory based scientists, virologists, statisticians, experts in every field of biomedical science and physicians of every specialty, and his own state-level department of the same composition “don’t bother to read science,” he is making a statement that is obviously ridiculous. I would submit to you that Dr. Dan Stock does not believe this. He knows that both the CDC and the ISDH read scientific literature, closely follow and analyze epidemiological studies, conduct extensive studies of their own, and in fact maintain rigorous standards of evidence on which they base their recommendations. He knows it, and he could have chosen here to say, as ZDoggMD says about his ambivalence about children wearing masks (an ambivalence I do not share; my kids are definitely wearing masks if we have to take them anywhere right now), that he earnestly disagrees with some of the CDC’s recommendations or conclusions. That is a credible and understandable stance, and many doctors I know have taken issue with some one or another of the CDC recommendations for various reasons. But Dr. Stock chose instead to make a statement he can’t possibly believe because he knew it would be appealing to certain people; the people in the room speaking out against vaccination, for instance, and whether he knew it or not many people across the country who would like to believe that any scientific finding or recommendation they disagree with is simply fake. Saying the CDC “does not bother to read science” is a signal of what team you are on, and nothing more; and it’s an unfortunate harbinger of what is to come in the rest of his speech.
0:39 “Everything being recommend by the CDC and the State Board of Health is actually contrary to all the rules of science.”
Again, these blanket statements should begin to make your misinformation Spider-Sense tingle pretty early on. Everything the CDC has recommended throughout the pandemic has contradicted the “rules of science”? Social distancing and staying home when sick don’t decrease transmission? Quarantining when exposed to a deadly and contagious pathogen doesn’t save lives? Dr. Stock would be on a much stronger footing if he said that he opposed specific recommendations- for instance masking and vaccinations- and then told us why he opposes them on scientific grounds. This “CDC is BAD” signaling is sure to get applause and video shares, but it’s hardly a good start for reasonable, precise debate.
0:43 “Things you should know about Coronavirus and every other respiratory virus…”
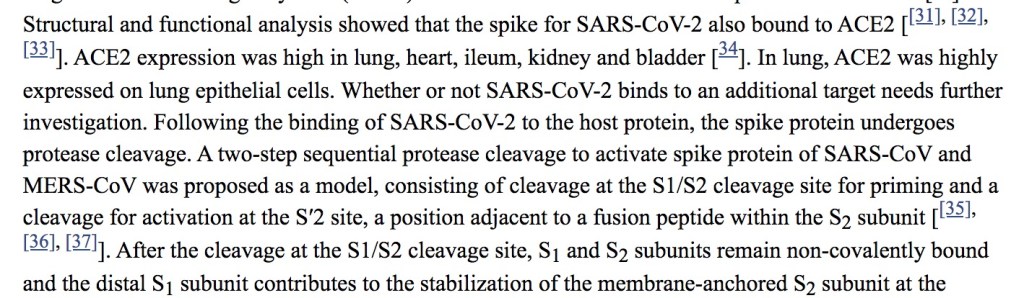
I would be incredibly suspicious of anyone lumping SARS-CoV-2 in with “all other respiratory viruses”… or lumping ‘all respiratory viruses’ together at all, for that matter. The virus that causes COVID-19 has behaved unpredictably throughout the course of this pandemic in more ways than we could count. It is a strange and unpredictable virus, which is why we had an even harder time treating it effectively in the hospital early on and why our transmission control measures, which have worked astoundingly well for Flu, have only ever managed to take the edge off of it’s transmission.
Dr. Stock would like to lull you into thinking that there is a set of regularities that viruses called “upper respiratory viruses” all follow, and that COVID-19 follows all of these as well. He may be lulled into believing it himself; he says later that he has seen only 15 COVID-19 patients. Last March many of us, myself included, believed that the ‘new coronavirus’ in China and parts of Europe was just media medical sensationalism. “Coronaviruses aren’t that dangerous,” we said (forgetting all about SARS since many of us had never actually seen a case of it), “they cause the common cold; there’s nothing to be worried about.”
Then we started treating it. I still remember the night I sat in bed watching videos from ICU’s in Italy, completely overwhelmed and without the medical equipment, supplies, rooms, or staff to care for all of the patients dying in respiratory distress, and I realized for the first time, “this is real.”
When Dr. Stock tells you throughout this video, “we shouldn’t do x, y, or z for COVID-19 because we’ve never done it for respiratory syncytial virus (RSV),” you need to remember that we have never seen RSV kill 600,000 Americans of all ages in 18 months. It’s the grossest kind of false-equivalence.
0:45 “Coronaviruses are spread by aerosol particles that are small enough to go through every mask.”
It’s been 18 months and it’s really hard to believe we are still talking about whether or not masks work, considering the abundance of data from epidemiology, physics, microbiology, and virology. I wrote about this extensively in June of 2020, and the evidence was already robust then. Yes, while masks like N95’s do a reasonably good job of stopping even small aerosolized particles that contain live viruses, surgical masks, simple cloth masks, and other options have a much lower filter efficacy at the 50-140 nanometer range, the size of the Sars-CoV-2 virions. A surgical mask will not stop every viral particle; but the mask that you are wearing will filter out a percentage of them depending on the type of mask; more for an N95, less for a surgical mask, and even less for a bandana or scarf. And the mask the infected person is wearing both block respiratory droplets from normal talking and will greatly decrease the velocity and spread of respiratory droplets, including the smaller aerosolized particles, and ensure that they hang around in the air for a shorter period of time.

I have never heard a scientist or physician claim that if 100% of people wore masks it would completely halt COVID-19 transmission; I’ve certainly never made that claim. But it does help, a lot, and the evidence for it is supported by far more than the three studies referenced by Dr. Stock (to be fair, he mentions these are the 3 that were funded by the CDC; he surely has more). This article on masks and COVID-19 transmission from Sri Lanka from last June cites 139 articles on upper respiratory viral transmission, particle size and dynamics, and prevention; a pretty good benchmark for that sort of paper. Saying “the masks don’t work” at this point in the pandemic is a call-back to the COVID-19 anti-mask skepticism of last Summer.
1:03 “Even though the CDC and the NIH have decided to ignore the very science they paid to have done.”
The CDC and the NIH fund literally tens of thousands of research studies each year; many of them are looking at the exact same or very closely related issues, and many times different studies that they fund produce differing conclusions; data that requires analysis, synthesis, and careful parsing. We would be extremely worried if they didn‘t. The fact that the CDC and NIH sponsor many studies and then carefully analyze the results, as well as the results of studies they didn’t pay for, before giving recommendations is a very good thing. If the CDC were to either ‘not read the science’, or cherry-pick the information they believe based on what agrees with their presuppositions- as Dr. Stock is doing with these studies he references- they would not be a reliable source of medical and epidemiological guidance. Thankfully, they don’t do that.
1:15 “The history of all respiratory viruses is that they circulate all year long waiting for the immune system to get sick through the Winter or become deranged as has happened recently with these vaccines.”
Dr. Stock practices something called “functional medicine”; basically the idea of addressing the root causes of disease and using the body’s own systems, as much as possible, to fight illness. It isn’t different than the practice of medicine in general, but it is a neat field that certainly has a more intentional focus on underlying causes. Because the emphasis so often lies on the patient’s own immune system fighting any infectious illnesses, the functional medicine doctors I know are very pro-vaccine; vaccination is as much in-line with the concept of letting the immune system do what it was designed to do as any medical practice. Unfortunately, functional medicine also attracts some doctors who are embracing certain anti-medicine or anti-science narratives, either because they have come to believe them themselves or because they see what a lucrative market there is for someone willing to offer all the benefits of modern medicine from an anti-modern medicine perspective and without the restrictions of having to follow the scientific evidence when it’s inconvenient. Good functional medicine doctors don’t do that, and I have heard recently from those practicing functional medicine who feel that doctors like Ben Edwards and now Dan Stock who spread misinformation give their discipline a bad name.
Because Dr. Stock has embraced a perspective that emphasizes the immune system above all else (yet somehow he doesn’t embrace the vaccines that give the immune system the data it needs to fight COVID?), his perspective on the seasonal pattern of respiratory viruses here is extremely incomplete. I thought about skipping this section, but it’s such subtle misinformation that it might get past people and lay the groundwork for more direct misinformation he shares in a few minutes.
Dr. Stock claims that respiratory viruses are worse in the Winter because the immune system is weaker, or because we get seasonal vaccines (like the flu shot or COVID-19 vaccines) that ‘derange’ the immune system. The latter part is nonsense; we’ll talk about it more later but it’s like saying that a construction crew becomes deranged when given a set of blueprints, or a sniper becomes deranged when given a photograph of her target. There is some truth to the first part; the immune system does work better during the Summer for a number of reasons, including sunlight exposure and increased exercise. But of the three major reasons for respiratory illnesses being worse during the Winter (or during the rainy season in temperate climates), it is probably the least influential in the seasonal pattern of these types of viruses.
First, viruses spread more during the Winter because of our behavior. How often have you heard the cultural myth that someone became ill with flu or pneumonia because they went out in the cold or got wet out of doors? It’s the opposite; they got ill with an infectious illness when they came back in to warm-up or dry-off, and were around someone with the virus. We spread respiratory viruses person to person through contact, sneezing, coughing, and touching surfaces while contagious. That transmission happens more easily indoors because of the close proximity and decreased air-flow compared to outside, and we spend most of our time indoors during the Winter. Think of your last Summer event; say spending the day at the lake. Yes, there were many people there, but you could spread out, the wind was blowing, and your conversations tended to happen with some space between you. Now think of your last Winter event- say a Christmas party. The same number of people, but this time inside, talking less than a couple of feet away, sharing the same air. Both events are wonderful (and I missed the latter this past year more than I can tell you), but there is no denying that one is a better opportunity for respiratory viruses to be transmitted than the other.
But the second reason is because of the behavior of the viruses themselves. Viruses are living organisms and like all living organisms they respond to their environment. Viruses like RSV and influenza are more stable in colder temperatures, meaning they can survive longer outside of the body when it is cold; both on surfaces and in the air. They also are more effective as aerosolized droplets when the humidity is low, because the droplets tend to be smaller. There are also effects of sunlight exposure on the viruses themselves, with the UV radiation damaging the genetic information of the viruses (just like it does ours; please wear sunscreen!), inactivating them to a certain degree. If anyone remembers last April, we all hoped that COVID-19 would disappear during the Summer because of these environmental factors. SARS-CoV-2 is an incredibly contagious, previously unknown virus; we hoped that it would display strong seasonal patterns like the flu and we would have a reprieve during the Summer. And maybe we did; but it wasn’t enough of a reprieve to prevent outbreaks, including here in Texas. In a little while Dr. Stock will tell you that the COVID-19 vaccines are the cause for the virus causing outbreaks this Summer. This is a myth, plain and simple. These outbreaks happened last year too, before anyone outside of clinical trials had access to the vaccine. The outbreaks this Summer are simply due to the fact that, unfortunately, COVID-19 does not display as strong seasonality as many of the other respiratory viruses we liken it to, and even more importantly, because the Delta variant is probably the most contagious dangerous respiratory in human history.
1:25 “The CDC has managed to convince everybody that we can handle this like we did smallpox.” The CDC and public health experts, and those of us fighting COVID-19 every day, have not felt a sense of extreme urgency to promote effective vaccinations against COVID-19 in order to eradicate it, but to prevent people from dying from it. Vaccination was invented by Dr. Edward Jenner, and was taken directly from the practice of inoculation- deliberately exposing the person to a small amount of the disease or a similar disease and hoping they would survive if they were exposed later. The practice of inoculation- or variolation when we are referring specifically to smallpox- was dangerous; since it was a live, active infection, it was possible to become sick with the disease when inoculated, and possibly to die from it. Nevertheless it was effective, and when American doctors were first given the idea to use inoculation to combat smallpox by an enslaved African man in 1721, his knowledge of traditional African healing practices saved hundreds of people during a smallpox epidemic in Boston.

Vaccination was different; it exposed the person to enough of the virus to trigger an immune response without the risk of the person contracting the virus. Traditionally this has been done by weakening or killing the virus, or by giving very closely related viruses that cannot cause disease (cowpox, in the case of smallpox vaccination). We now have the technology to teach cells to build specific, non-dangerous viral proteins so the immune system can learn to recognize them and build antibodies against them without exposing the body to any virus at all. This is a natural progression of the principal of inoculation that humans have used for thousands of years; live virus to weakened virus, weakened virus to dead virus, and now dead virus to no virus at all. The mRNA vaccine technology feels unknown or unnatural to many people, because it came about in their lifetime (I was 6 years old the first time scientists successfully used mRNA technology to teach cells to express viral proteins); but it is really the logical next step along the path set for us by traditional African, Indian, and Asian healing practices; the path of using the body’s own immune system to fight disease.
Dr. Edward Jenner’s personal goal, oft stated, was to eradicated Smallpox. But that was not the only or even the primary goal. The goal of inoculation, variolation, and vaccination has always been to prime a person’s immune system to fight an illness so that they have a less severe course of illness and a lower risk of dying from it. That was the goal of variolation in Western African and later in Boston, it is the goal of the childhood vaccinations we give against measles, whooping cough, and tetanus, it is the goal of the annual flu shot, which has saved millions of lives, and it is the goal of the COVID-19 vaccines; a goal they have seen incredible success at achieving, for those who have received them. We may not be able to eradicate COVID-19; but we can very effectively protect people from it.
2:04: “I would hope this board would start asking itself, before it considers taking the advice of the CDC, the NIH, and the State board of health, why we are doing things about this that we don’t do for the common cold, influenza, or respiratory syncytial virus?”

2:16 “Why is a vaccine that is supposedly so effective having a breakout in the middle of the Summer when viral respiratory syndromes don’t do that?
It’s a little tricky to understand what he is talking about right here. First of all, the vaccine isn’t having an outbreak. That would actually be awesome, if just suddenly there was this uncontrollable surge of people getting vaccinated. What he means is, ‘the virus is having an outbreak because of the vaccines.’ He is subtly shifting responsibility for the outbreaks away from the virus itself, the incredibly contagious delta variant, the general lack of caution and transmission control measures being exercised, abysmally low vaccination rates, and widespread conspiracy theories and disinformation, and onto the vaccines, which is a tactic from the “it’s so crazy it just might work” school of misinformation. He is asking you to shorten your memory and ignore the fact that we already knew pre-vaccine that this is how COVID-19 behaves, since this is what it did last Summer. He wants you to think something like this; “COVID-19 is really bad this Summer. Dr. Stock says that shouldn’t happen during the Summer. A lot of people I know have been getting those vaccines… I bet that’s why.” It’s a logically bankrupt argument with no foundation in reality… But it just might convince some people.
In a moment Dr. Stock is going to offer a seemingly plausible explanation for his false narrative in the form of “antibody-mediated viral enhancement.” Dr. Simone Gold shared this same misinformation a few months ago, so below I will copy my discussion of the phenomenon from that time. But the best cure I have for Dr. Stock planting this sort of deliberate misunderstanding is just data. The vaccines are working well, and anywhere that you see high vaccination rates you see fewer and less severe cases, not higher numbers and more severe cases. All of the evidence says the vaccines are working against COVID-19. If we had higher vaccination rates in Texas and Louisiana, we would have smaller and less severe outbreaks this Summer, plain and simple.

2:28 “You need to know the condition called “antibody-mediated viral enhancement. That is a condition done when vaccines work wrong…”
There’s a lot of misinformation here. For instance, he implies that COVID-19 has low pathogenicity- a low rate of causing illness- which is totally disconnected from reality. He also implies that the current COVID-19 vaccines caused antibody mediated enhancement in previous studies, which they absolutely did not. In fact, even though Dr. Stock presents this as though he were blowing the lid off of this hitherto-unheard-of fatal flaw in COVID-19 vaccines, avoiding the risk of this phenomenon was foremost in researchers minds when designing these vaccines; he would have you believe that the scientists designing the vaccines had never heard of it before, simply because you might not have heard about it before.
Immune enhancement is a very real concerned, and one that has been hotly debated within research circles since the beginning of the pandemic, especially in regards to severe COVID-19 cases and the potential role of vaccines. Here’s an article from way back in May 2020 (what is that, like 8 years ago now?) about this exact issue. The specific proteins chosen for the mRNA vaccines were chosen carefully and specifically to avoid this problem, and moreover, this is exactly why we do animal studies and clinical trials.
The Moderna and Pfizer trials were simply huge, with ten times the number of people participating than is typical in a vaccine trial; and no evidence of Antibody-Dependent Enhancement was found. The Nerdy Girls over at Dear Pandemic have a short but great social media update on it from just a few months ago:

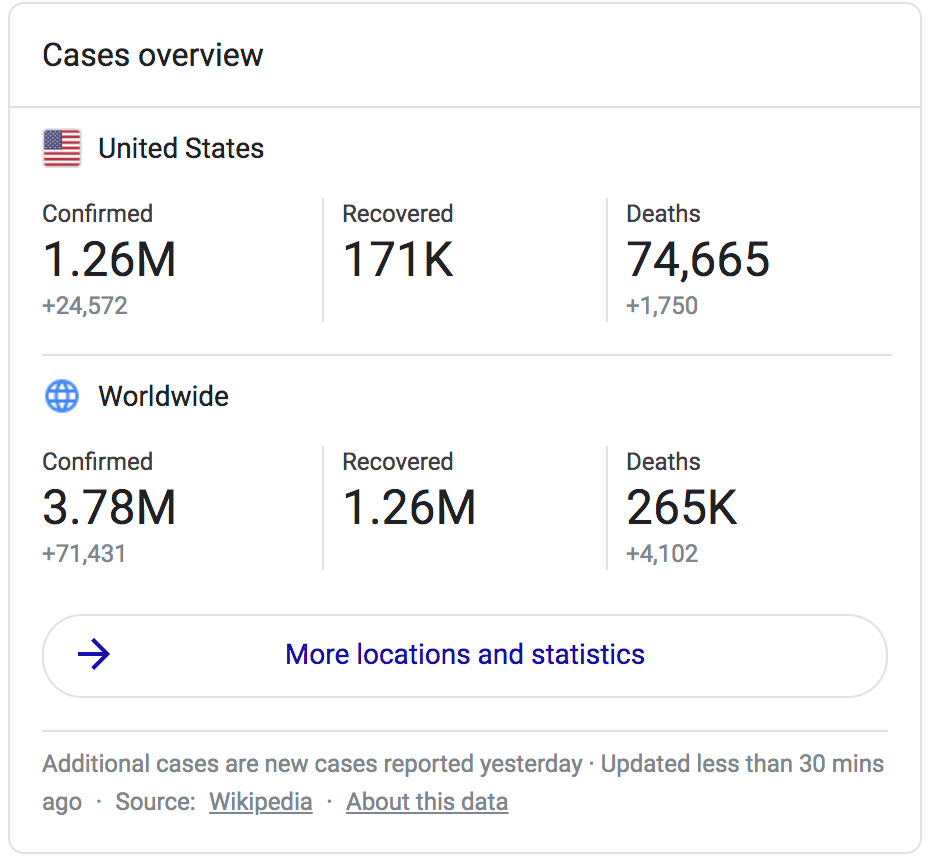
Moreover, we have now given 352 million COVID-19 vaccine doses in the US alone and over 4 billion doses worldwide, and there is still no evidence that the COVID-19 vaccines cause antibody-dependent or antibody-mediated enhancement. The entire course of the pandemic shows exactly the opposite; those who have the vaccine get less sick, less often, and have drastically lower rates of severe illness, hospital and ICU admission, or death from COVID-19.
3:10 “75% of people who had COVID-19 positive symptomatic cases in the Barnstable Massachusetts outbreak were fully vaccinated.”
And 4 of them were hospitalized, and none of them died. I wrote about this just yesterday so I won’t rehash it; it’s a very short post and the link is just below. The long and short of it is, the Barnstable “outbreak” is proof of how well the vaccines work, not of the contrary. What we saw in Barnstable is the opposite of antibody-dependent enhancement; it’s a clear demonstration of the effective protection against severe illness and death for those with the vaccine, and an example of what might have been if we had such high vaccination rates in Texas, Louisiana, and Florida before the Delta variant hit.
The Massachusetts Outbreak is More Proof that the COVID-19 Vaccines Work.
3:23 “Therefore there is no reason for treating any person fully vaccinated any differently than any person unvaccinated.”
In a sense, he’s correct; morally we absolutely should be aiming to treat all people the same regardless of their personal health choices. I am reminded of the quote by C.S. Lewis:
“There are no ordinary people. You have never talked to a mere mortal. Nations, cultures, arts, civilizations – these are mortal, and their life is to ours as the life of a gnat. But it is immortals whom we joke with, work with, marry, snub and exploit – immortal horrors or everlasting splendors.”
― C.S. Lewis, The Weight of Glory
Your unvaccinated neighbor, your vaccinated friend… They are equal in dignity and honor; they are equal bearers of the Imago Dei. Yet our very respect for that Image of God in each person does require us to weigh many factors in the balance as we consider our approach to this complex pandemic. I believe that profound respect for the dignity of all people requires us to “treat” vaccinated and unvaccinated people differently in two ways.
First, we need to recognize that, regardless of Dr. Stock’s subsequent comments, the COVID-19 vaccines do prevent transmission of the virus. The jury is still out on how well they do this; most of our data just establishes how good they are at preventing symptomatic infection and especially severe infection and death, and there are studies happening right now to see to what degree vaccinated folks can still pass the virus along when symptomatic and when exposed but asymptomatic. The Barnstable MA outbreak is warning enough for all of us who are vaccinated to continue to take precautions like wearing masks and staying home and getting tested when we are ill, if anyone had any doubts. But it was also a contained, small outbreak and we don’t actually know how much of it was transmitted by vaccinated residents of Barnstable county vs. out-of-state visitors; and there’s no way to go back and find out. Nationwide we are seeing Delta surging, and surging most in the states with the lowest vaccination rates. All of the physiology of how our immune systems fight viruses when primed with vaccines suggests that vaccinated people will transmit the virus at a lower rate, and for a shorter duration, than those who are unvaccinated. Vaccines don’t teach your immune system how to ignore the virus, while it multiplies and gets passed along to others; it teaches your body how to kill it. And this, married to the epidemiology evidence of how the surge is progressing in highly vaccinated vs. poorly vaccinated areas constitutes strong evidence that the vaccines do confer protection not only against getting sick from the virus, but against passing it along to others as well.

Does this mean that I treat my unvaccinated friends and family like second-class-citizens, barring them from my home and preventing them from ever spending time with my children? While I understand and sympathize with those who feel forced to do so, my answer is a definite “no.” But it does mean that the complex balance of goods and risks that determine in what way I and my family interact with others- which always existed even prior to COVID- has one more important factor. My children are unvaccinated (though I am trying to enroll them in clinical trials so they can get a COVID-19 vaccine as soon as possible), and there is already anecdotal evidence that the Delta variant effects children more than the original strain. I have a basic moral responsibility to protect my children, and the reality is that factors like community transmission rates and the personal health choices of others do have to be factored into our decisions. For us it’s not a question of, “who do we cut out of our lives because they won’t get vaccinated?”, but a question of, “how can we best build and maintain relationships while limiting risk?” That answer is going to vary to some degree with the current prevalence of COVID-19, with the level of caution those in our lives are themselves following, and with their vaccination status.
But I think the second way we treat unvaccinated people differently is arguably much more important. The reality is that, whether they believe it or not, they are more vulnerable to the virus. As a physician, the rapidly branching mental decision tree I follow when helping a patient decide what level of caution to exercise, what treatments to pursue, what symptoms to watch out for, how aggressive to be in seeking further care, and how closely to follow-up is determined by many factors. For COVID-19 care, vaccination status is a big one. My vaccinated patient’s chances of dying from COVID-19 are far, far lower than my unvaccinated patient’s chances, all other things being equal. As a society, our decisions about protecting people from the virus need to be centered on those who can’t be vaccinated, like children or those with true vaccine allergies, on those like the immunocompromised for whom the vaccines might not be as effective, and on those who decide not to be vaccinated. They are still at risk, and nowhere in my medical training can I recall an ethical precedent that says we don’t take excellent care of people if their personal health choices led to their illness (though I do realize that, far too often in modern medicine, we treat patients poorly if they are perceived as contributing to their own health problems or ‘not caring enough’. It’s a huge problem, and trying to address it is one of the reasons I’ve taken a new job teaching at a medical school).
In general I don’t agree with measures that say, “if you are vaccinated you can do this, if not you have to do this.” I understand that from an epidemiology standpoint some of these distinctions are logistically impossible to get around; but the tenets of my faith call for humility and self-sacrifice on behalf of others. If their decision to not get vaccinated means that I have to endure some ongoing inconveniences- like wearing a mask while buying groceries or sitting outside and socially distanced at my favorite coffee shop in the middle of August, when it would be more pleasant inside- I’m here for it. If I knew for a fact that everyone at that store or everyone inside the coffee shop were vaccinated, I might loosen those measures, as I do in small gatherings where I do know that everyone is vaccinated (just ask my Dungeons and Dragons group; we had this exact conversation last week!). I wouldn’t advocate for stricter transmission control measures imposed only on the unvaccinated, but I would advocate for us all following those strict measures, and then dropping some of them that are no longer needed when we know the unvaccinated aren’t going to be potentially hurt by doing so. If that still means I’m “treating them differently,” I guess guilty as charged; I’m treating them like their lives are in danger, because they are, and well, that’s something I really do care about.
3:27 “No vaccine ever stops infection.”
By “infection” Dr. Stock does not mean the virus multiplying significantly in your body for any specific period of time, or the onset of any specific symptoms; only the state of having the virus enter your body and begin to reproduce itself. This is what I’ve been trying to help patients understand for the past 9 months as we have talked about the COVID-19 vaccines: vaccines don’t place a forcefield around you that prevents the virus from entering your system; they prime your immune system to defeat it.
But saying that infection still occurs whenever you are exposed to the virus is not the same as saying that transmission occurs, or occurs at anywhere near the same rate, if you are vaccinated. We’ve just talked about how the evidence on this is still evolving for COVID-19, but that it’s very clear that those areas with higher vaccination rates have lower transmission rates. Yes, some people who are vaccinated still get COVID-19, but tend to have shorter illness, lower viral loads, and less severe symptoms. It’s unclear exactly how well they spread the virus, just as it’s still unclear whether the vaccinated are sometimes asymptomatic carriers. But we do know that both of those types of transmissions occur, and occur at extremely high rates, in the unvaccinated who become infected with COVID-19. The current surge of the Delta variant is being driven by transmission from and to unvaccinated individuals.
I won’t keep rehashing the same points, but I will add this; Dr. Stock is wrong about vaccination ‘never stopping infection’ (the virus getting into your system in the first place); it stops infection for the next person, by decreasing the chances that you’ll get sick and pass it along. Please catch the contradiction he has created for himself; Dr. Stock is painting a picture of viral infections moving from person to person uninhibited by their immune systems, with those who get the vaccine (or at least, the vaccines he agrees with) not getting sick but still invisibly passing it around as much as anybody as it lives rent-free in our systems forever.
But a couple of minutes ago he admitted that vaccines eradicated smallpox.
I’ve never been vaccinated against smallpox. Hardly anyone in the US has since 1972. So where is it? High vaccination rates literally stopped it from infecting anyone. If it only suppressed disease and not infection and transmission, we should have seen a smallpox resurgence decades ago, once we stopped vaccinated for it; thankfully, there is still no evidence of smallpox transmission anywhere in the world. No, I don’t think we’ll eradicate COVID-19 the same way, even with high vaccination rates; it’s a very different sort of virus, and the best we can probably hope for is to remove its teeth. But since he brought up smallpox in the first place, I think it’s fair to point out how the history of smallpox vaccination and eradication blows his picture of how vaccines work right out of the water.
3:38 Mumps Outbreak in the National Hockey League.
In 2014 there was an outbreak of mumps in the NHL that affected 24 players. The mumps vaccine is not 100% effective, but it is very, very effective as Dr. Stock admits. Prior to the mumps vaccine, almost all children got mumps at some point during childhood. After vaccination against mumps became common, the rate of mumps infection dropped by 99 percent. Yes, it is still possible to get or spread a virus if you are vaccinated, no one has ever said otherwise; but it is far less likely. Why is Dr. Dan Stock currently citing contract tracing for a so-called outbreak that affected 24 people, when just 50 years ago most people got mumps during childhood? Because vaccination against mumps is so effective.
How effective? Well, two doses of the mumps vaccine is about 88% effective at preventing this previously ubiquitous illness. 88% is also how effective the mRNA vaccines seem to be against the Delta variant of COVID-19. Ask yourself, when was the last time you worried about mumps? Wouldn’t it be great to get to that point with COVID-19 too?
4:12 “You get infected, you shed pathogen; you just don’t get symptomatic from it.”
We’ve talked this false idea that vaccinated people spread the virus just as well as unvaccinated people to death in the last few paragraphs, so I’ll just add this; when “getting symptomatic” from COVID-19 has resulted in 617,000 deaths in the US in just 18 months, doesn’t “not getting symptomatic” sound like a really, really good thing?
4:14 “You cannot stop spread, you cannot make these numbers that you’ve planned on get better by doing any of the things you’re doing, because that is the nature of viral respiratory pathogens.”
All of the epidemiological evidence, from all over the country, says he’s wrong. The vaccines are slowing the spread and making the numbers better. He’s also wrong that the nature of viral respiratory pathogens means that you can’t slow them with basic transmission control efforts like wearing masks and strict sick policies in schools; those very efforts helped us kick influenza’s butt last year. COVID-19 is trickier to beat since it is so much more contagious and has so much asymptomatic transmission, but there’s no doubt that when these measures are followed, they do help. There’s ample evidence of that all over the world, both pre- and post-vaccine.
I’ve said it before and I’ll say it again; there is something deeply disingenuous about people who refuse to wear masks or follow transmission control measures, and have refused to do so since the beginning of the pandemic, pointing to increasing case counts and saying, “see! these masks (I won’t wear) and transmission control measures (I won’t follow) don’t work!”
4:26 “You will be chasing this the rest of your life until you recognize that the Center for Disease Control and the Indiana State Board of Health are giving you very bad scientific guidance.”
And what does Dr. Stock place in opposition to this scientific guidance? Other expert organizations with teams of researchers and epidemiologists devoted to finding the very best ways to slow the pandemic and combat COVID-19? A specific, innovative plan of attack that none of the experts have thought of yet (hey, it could definitely happen!)? No; his e-mail, and the other people in the room who have presumably come to the board meeting to protest mask mandates or vaccines or whatever specific measure was originally on the table for discussion that night.
4:47 “That’s why you’re still fighting this with this vaccine that was supposedly going to make all of this go away...“
“The vaccine I won’t get and am telling all of my patients not to get. Why hasn’t it worked yet?”
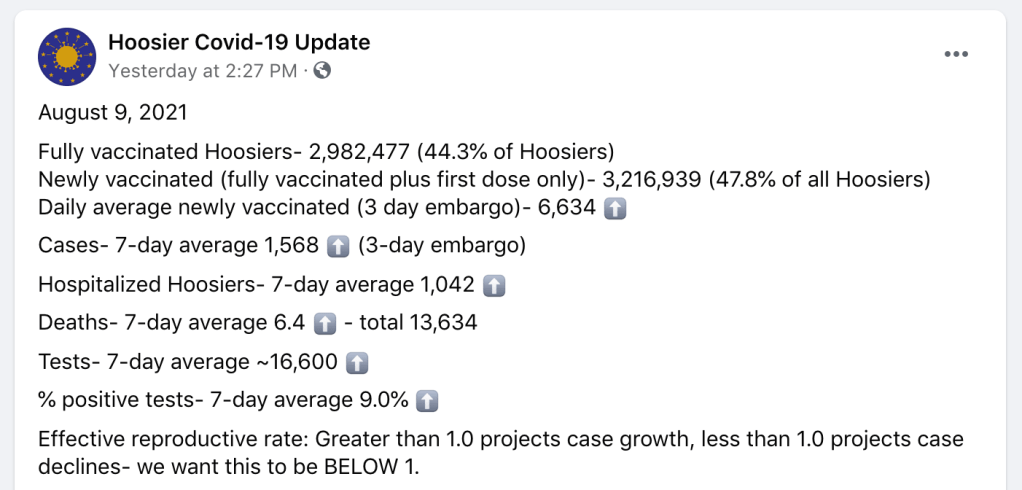
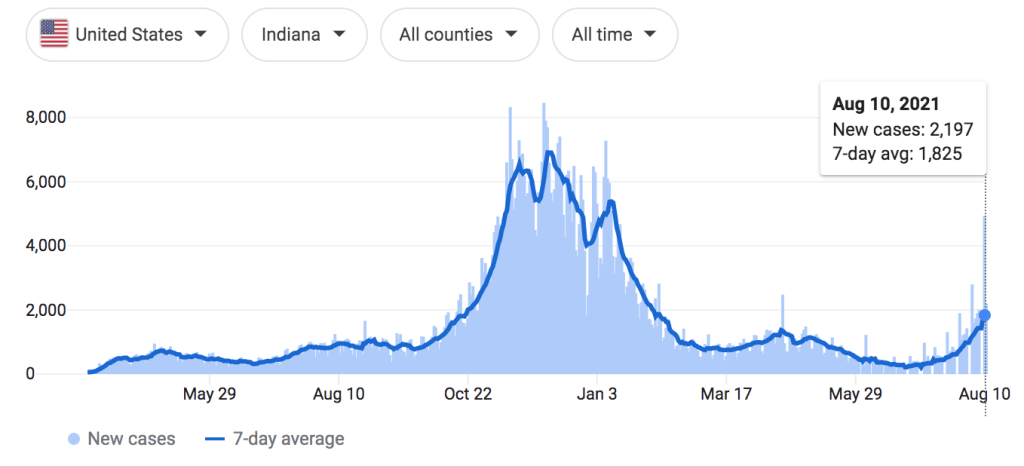
Indiana has only a 44.3% vaccination rate. They are in the middle of a COVID-19 outbreak; not as bad Texas or Louisiana, but still on the rise.
Again Dr. Stock blames the vaccines, instead of the virus and our low vaccination rates, for the outbreak, reinforcing his false narrative that vaccines have caused the outbreak through antibody mediated viral enhancement instead of reduced or prevented outbreaks wherever vaccination rates are high. If his “outbreak in the middle of the Summer” reference is to his own state of Indiana, I would paraphrase G.K. Chesterton; ‘the vaccines have not been tried and found wanting; they have been found shrouded in disinformation, and left untried.’
On the other hand, if he is again referencing the contained “outbreak” in Barnstable Massachusetts, one would ask why he feels compelled to rely on epidemiology data about the pandemic from a county a thousand miles away, when the evidence from his home state shows how effective the vaccines are? I submit that it is because the outbreak in Massachusetts is the data that best seems to support his claims (again, we’ve seen already that it doesn’t), and he would go to the ends of the earth to find it. When you are committed to misinformation, the experiences of people affected by the virus all around you simply aren’t important unless they fit into your narrative.
5:05 “I can tell you having treated over fifteen COVID-19 patients…”
Listen, I know no misinformation video would be complete without touting the latest en-vogue, unproven therapies. But 15 patients? Fifteen?!
I’ve treated hundreds. Nobody wishes that we had a safe and effective prophylactic or early symptomatic treatment regimen more than I do. I spend so much time kneeling on pavement next to cars in the Texas heat, counseling my patients on what to look out for with COVID, helping them establish a posture of vigilance and discernment but without fear or anxiety, helping them navigate the different options for considering monoclonal antibody therapy, and helping them make decisions about work, school, and how to prevent transmission to loved ones. This narrative that we are refusing to give effective treatment to our patients is deeply frustrating and not at all based in truth; I have never withheld a medicine I believed my patient needed, not once in my life; and I spent a lot of my time trying to help them figure out how to get those medicines regardless of expense or other barriers. We are giving them the best that we have to offer; we have been since the beginning of the pandemic and long before.
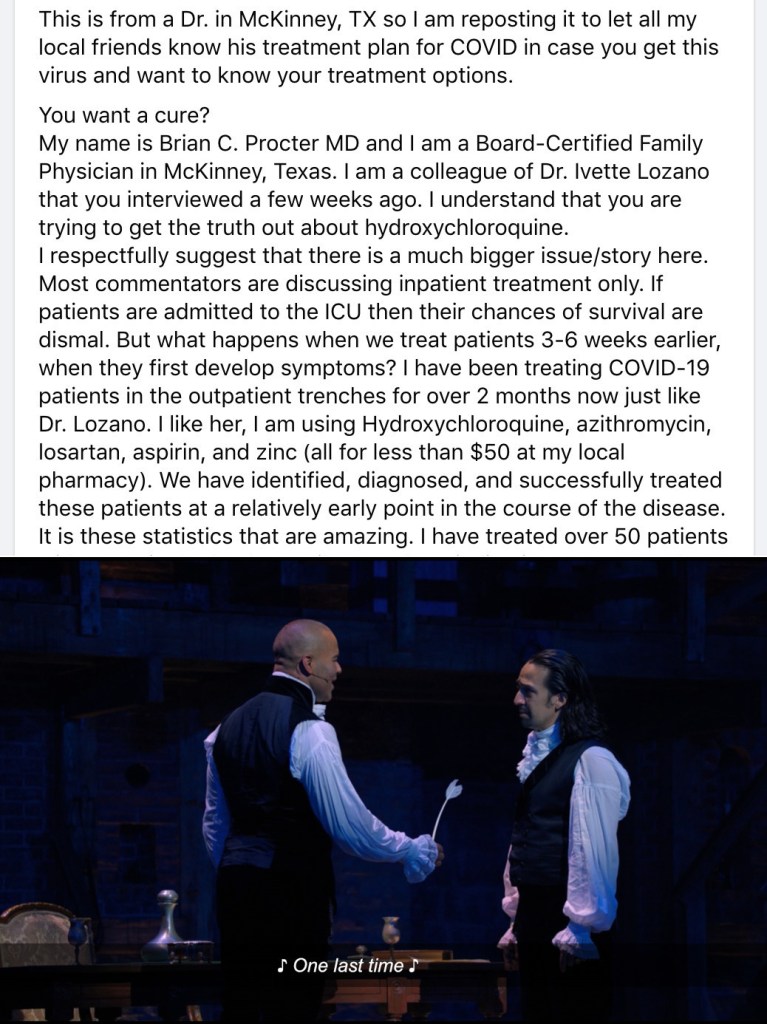
This “clinical experience” that these doctors like Simone Gold or Ivette Lozano who have treated a small handful of COVID-19 patients (or in their own words, people who thought they might have COVID-19; many times these doctors don’t even bother to test because they don’t believe the tests work) share about how they’ve found a universally effective treatment against COVID aren’t even anecdotal evidence; they are just sampling bias. They see a couple of patients, some of them have COVID and some of them don’t. They put them all on a cocktail of drugs, none of which have been shown to be effective in clinical trials. Those patients recover, as most patients with COVID-19 do without these unproven treatments; but then these doctors tell themselves “without my treatment, that patient would have died.” Except there is no evidence they would have; for some of these docs, there isn’t any evidence those patients who “would have died without my treatment” even had COVID-19 to begin with. They were doing this same nonsense last March and April in areas that hadn’t even seen their first surge of COVID-19 yet, drawing customers (they aren’t your patients when you are just selling them something) from all over the state and saying things like, “yeah, you probably have it, take all of these medicines”, then adding that person’s “survival” to their “evidence.”
I don’t know if this is what Dr. Stock is doing or not. Maybe his patients all had laboratory confirmed COVID-19, or a convincing combination of symptoms and exposure history. Maybe they had really significant risk factors for severe illness, and their recovery turned him from a skeptic to a believer; I don’t know. He certainly seems sincere in his beliefs. but the fact of the matter is, 15 patients with COVID-19 is not enough to base your case on. That’s one of the principals of evidence-based medicine, having the humility to give our own personal experiences only the weight they are due, and respecting our colleagues, our patients, and people from around the country and world enough to recognize when our experiences are atypical or, as in this case, just way, way too small to actually draw conclusions from. I’ve had many days in clinic when I took care of more than 15 patients with COVID-19. Sometimes I’ve been surprised by how sick a young, previously healthy person got with the virus, and sometimes I’ve been surprised by how light a course of illness someone with many risk factors experienced. I can’t draw conclusions from those experiences any more than Dr. Stock can; even my vastly more extensive experience with COVID-19 pales in comparison to our collective experiences as a medical field, compiled as evidence and then analyzed carefully.
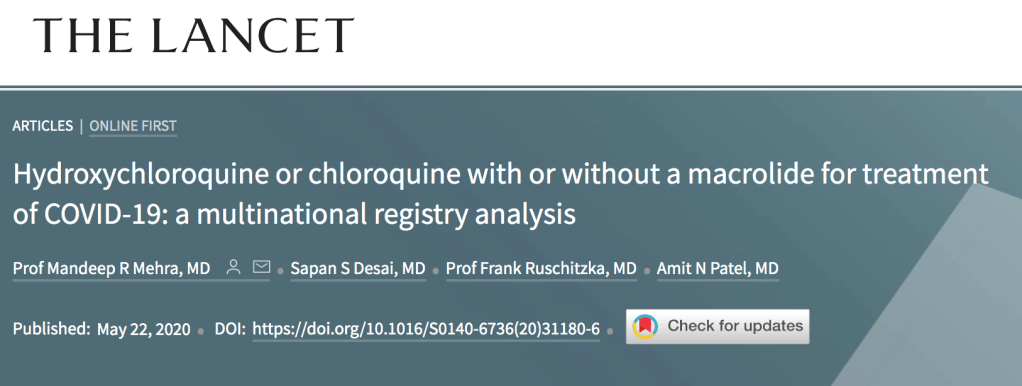
And look, I get it. If I were seeing less than 1 patient a month for COVID-19, I might be tempted to abandon evidence and just throw whatever the current theoretical treatment was at them too. These medicines like hydroxychloroquine, zinc, Azithromycin (remember when that was a thing?), and Ivermectin are generally safe, and I’ve prescribed them all for different illnesses in the past. If I gave out one prescription a month because I though there was a chance they would help, I wouldn’t be doing something morally wrong. But it’s not evidence based medicine, and it only feels excusable to practice on gut instinct or social media hearsay like that when you are talking about incredibly small numbers of patients. But because there is no evidence that they do work against COVID-19, prescribing them routinely, prescribing them for thousands of patients with COVID-19, COVID-19 exposure, or COVID-19 like symptoms like I would have to do as someone who fights this virus every single day, would be no different than throwing antibiotics at viral infections because it’s quicker than explaining the difference being a viral and a bacterial infection, doing unnecessary surgeries because it “might help the pain,” or adding more and more medications because you are too busy or too lazy to help your patient find a diagnosis and understand their illness. It isn’t the practice of medicine.
If I’m going to prescribe a medication to a thousand patients, I have to have evidence that it works. And if I’m going to hold a certain high standard of care for a thousand patients, my one patient deserves that same standard of care; they don’t deserve to be the guinea pig for the ‘Ivermectin study I’m doing in my head.’ Right now there is no evidence Ivermectin prevents severe COVID-19. I hope that changes. It didn’t change for azithromycin or hydroxychloroquine, but I hope it does for ivermectin so I can start prescribing just tons of it. And if it doesn’t, I hope the next hot-button medicine really does work, so that I’ll finally have the silver bullet many patients are looking for when I give them the anxiety provoking news that they have COVID-19, instead of ‘just’ careful counseling, reassurance, guidance, and symptomatic treatment.
You know what is safe and does work extremely well at preventing severe COVID-19? Vaccination. As a functional medicine doctor, Dr. Stock’s entire ethos should revolve around identifying root causes, relying on our own body to produce a state of health (a privilege not everyone has), and prevention rather than treatment whenever possible. In stating that we should abandon training our immune systems to fight COVID-19 with the vaccines for all of the erroneous reasons he has offered because unproven treatment is available, he has abandoned functional medicine altogether.
5:45 “People who have recovered from COVID-19 infection get no benefit from vaccination.”
Dr. Stock’s very last point is that people who have already had COVID-19 get no benefit from vaccination. This is a question I am asked frequently, and the epidemiology data about who is getting COVID-19 and who is not, and who is getting the most sick from it, does show that those who have already recovered from COVID benefit from the vaccine. The truth is that, if you have already had COVID-19 (just as I did back in December) and then are subsequently vaccinated (just as I was, also back in December, about 2 weeks later), you probably have the best immunity out of just about anybody. Seriously, I wouldn’t encourage anyone to go out and get COVID, but if you’ve already had it and decide to vaccinate, you are getting protection against COVID-19 that money can’t buy. Studies of antibody titers have shown that the immune response elicited by vaccination is equal or greater than that from natural immunity from previous infection. These vaccines are very, very good at what they do, and they work incredibly similarly to how our body’s learn how to defeat viruses from natural infection, only without the risk of illness since the vaccines contain no actual SARS-CoV-2 virus.
When you have an infection, your body responds with a host of inflammatory and immune cells. It’s a very good system, and if we are lucky enough to have a healthy immune system, it prevents us from becoming seriously ill from the various pathogens in our environment most of the time. But just like Sherlock Holmes, it needs a lot of information before it can produce its most incredible work.

During that initial infection, the body is building antibodies, memory B and T cells, and other other specific immune cells targeted at that virus specifically. The next time you are exposed to that virus, the secondary immune response leaves the first one standing. With repeated exposures, the body learns that a threat is real and something you need to be prepared for; cells created after the first exposure, whether it’s from an infection or a vaccine, respond to the immune cells reacting to the 2nd exposure to create and even more robust response; cells that produce massive amounts of antibodies, cells that are incredibly active against the virus, and cells that move to the bone marrow and live for decades; maybe even your entire life.
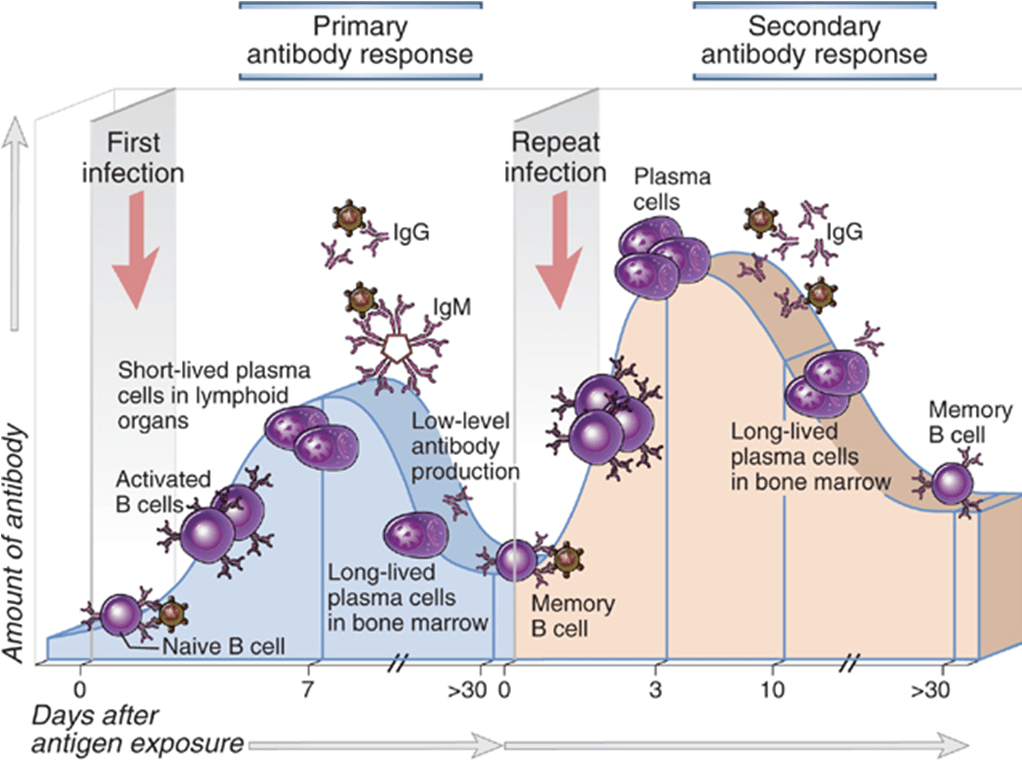
If you’ve been lucky enough to avoid COVID-19 so far, the vaccines give you the opportunity to teach your body how to effectively produce this robust immune response without having to actually suffer through or take on the risk of getting the virus that has killed over 617,000 Americans in the past 18 months. If you’ve been unlucky enough to have COVID-19, but have recovered from it, the vaccines give you the opportunity to take that immune response you have already started building and ensure that you don’t just have some immunity, but that you actually have robust, probably very-long-lasting immunity. Your body doesn’t check Facebook or watch the news; the vaccines are your best and safest way of telling your body, “Remember COVID-19? Yeah, so that’s still a thing… Might want to be really prepared for it.”