
Introductory Comments
(skip ahead if you just want the minute-by-minute analysis)
Dr. Simone Gold and America’s Frontline Doctors
The video below is going viral right now, spread mostly by private text and social media messages. I’ve had it sent to me by several people in the last week, both doctors who were frustrated with the obvious untruths but too busy (with the pandemic) to formulate a response, and bdiy people with less scientific training who knew the information didn’t sound right but didn’t quite know why.
The talk is from The Stand, a mass faith healing and miracle event put on by known religious hucksters in Florida. False Teachers and theological misinformation are another passion of mine and have been for much longer, ever since I attended a Benny Hinn crusade for a Sociology course. But even though there’s also a pandemic of heresy in the United States right now, it’s the medical aspects of Dr. Gold’s talk at The Stand on January 3rd that we are focused on today.
For an introduction to Dr. Gold and her organization I would encourage you to glance at the response I wrote to their most popular video, a press conference they gave at Capitol Hill back in July. This was the video where Dr. Stella Immanuel from Houston spoke about hydroxychloroquine.
America’s Frontline Doctors (I guess I don’t count?)

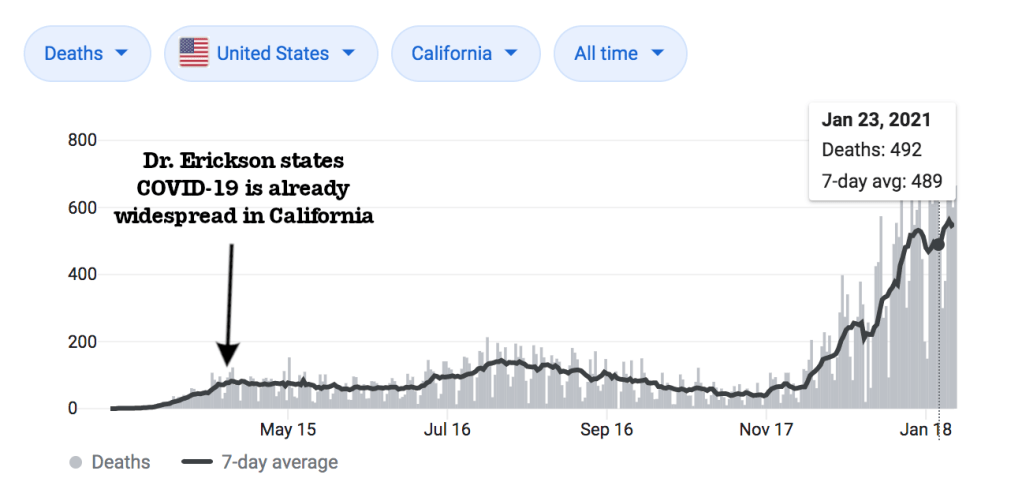
This group has been speaking and writing about COVID-19 since at least May, when they wrote a letter comparing the COVID-19 pandemic to a Mass Casualty Event, where presumably the 437,000 Americans who have died from the pandemic so far would be in the “black” category of mass casualty triage; not worth trying to save. The group also includes Dr. Dan Erickson, the California urgent care doctor who spoke out about how the virus is not-dangerous and how most of California had already had it… Back in April. To Dr. Erickson’s credit, his later statements have been much more measured, and based on his sincerity in the original press conference I actually wouldn’t be surprised if he at some point quietly recants his analysis, which was founded on extremely flawed epidemiological assumptions. To date, there have been 40,192 COVID-19 deaths in California.

Finally, you may have read about Dr. Gold’s recent arrest for her involvement in the attack on the US Capitol, which occurred just 3 days after her appearance at The Stand, during which she gave a brief speech again condemning the vaccines and encouraging people to get ahold of hydroxychloroquine. Dr. Gold has since stated that she regrets being involved in that event. My sincere hope for Dr. Gold is that this series of events will force her to consider not just that particular action, but also her stance on the pandemic over the past year as a whole, and to reexamine the evidence, reflect on the harm that has been done by medical misinformation and the people who have died as the result of attending to it, and maybe even become a leading voice for reform from within the COVID-19-denial movement. Dr. Gold is sincere, funny, and winsome as a public speaker; it would be the greatest thing in the world if after this she chose to use her platform to help people take the pandemic seriously and love their neighbors by following common sense, effective transmission control measures.
Layout of this post
This is a very long post and I don’t expect everyone to read it all the way through. I’ve divided it up into a minute-by-minute breakdown with time stamps for easy reference. If there’s a section of the video you want to read a counterargument or clarification for, just look at the time on the video and scroll to that part of the post.
I’ve also separated it into large sections which I’ve hyperlinked below in the “contents” section. Though Dr. Gold jumps around a bit (that’s not a criticism, I jump around way more when I speak in public), it is possible to separate her talk into some big chunks, so that if you are really only interested in particular topics from her video you don’t have to watch the whole video or read the whole post.
Finally, I’ve included the video itself in my blog post. Just as we have to fight the COVID-19 pandemic on an individual level by providing excellent patient care to those affected and on a population level by encouraging transmission control measures like masking and social distancing, misinformation can be fought in two ways; containing the spread by taking down harmful and misleading content, and by engaging with that content and providing thorough analysis. I have mixed feelings about the first method, and as a primary care engaging directly has been the focus of all of my training and my life’s work. So if Dr. Simones Gold’s video gets taken down on other platforms, it will be up here; and all I ask is that if you are going to watch the video on my blog you’ll also read the blog. Not doing so is tantamount to admitting you are only willing to consider one side of these arguments, and I’m betting that’s not consistent with how you see yourself; all of us want to be fair and reasonable in our judgements.
Contents
Introduction
Dr. Simone Gold and America’s Frontline Doctors
Post Layout (you are here)
1 thing I’m going to do and 1 thing I’m not going to do
3 things Dr. Gold is going to do
Video
Minute-By-Minute Analysis
Part 1: Preliminaries, Hydroxychloroquine, and Masks
Part 2: “Experimental Vaccines”
Part 3: COVID-19 Vaccines and Racial Healthcare Disparities
1 Thing I’m going to do and 1 Thing I’m not going to do
First, I am going to try to be very fair to Dr. Gold in this analysis.
I know that Dr. Gold has a lot to gain from her minority position on COVID-19 issues (becoming the niche go-to medical expert for millions of people who want to believe what you are telling them can be very profitable), but also a lot to lose, which she touches on in the video. Yes, it’s almost a certainty that we will see a book or another political bid from Dr. Gold in the future, and someone whose videos have been shared tens of millions of times and who has successfully sold medication from her website before being forced to stop might sound a bit hollow when complaining about what a risk she is taking by “speaking out”. But the truth is that there is risk. She has been arrested, albeit for her involvement in an attack on the US Capitol and not for anything she has said about COVID-19, and considering everything she has said and written over the past year I’ll honestly be surprised if she keeps her medical license, and I could honestly argue either way as to whether or not that’s actually fair. A doctor friend and I have often morbidly joked that if we didn’t care about morality or medical ethics, we could make lots of money as MD’s; we’ve all seen people do it, endorsing some expensive supplement or offering unproven treatments at exorbitant prices. But I do not believe that Dr. Gold has simply conducted a market analysis and decided there is more money in spreading COVID-19 misinformation than in quietly working as an ED doc, treating disease and alleviating suffering. She must earnestly believe at least some portion of what she has said in this video and has been saying since early in the pandemic, or she would not take the risks; and that is a sympathetic position. I disagree with her on many points, I think it’s pretty clear that she is wrong and why, and that as a physician I think she ought to know better; but I believe she is sincere in a certain way, and wish rather that she could see the truth than that she would simply stop spreading falsehood.
So I’m going to try to be fair. When I perceive that Dr. Gold is speaking from a sincerely held belief I’m going to say so, and when I can’t tell I’m going to assume that she is. We will look at why, in her personal experience and clinical practice, she might be justified in believing some of those things (though as a doctor she has as much access as any of the rest of us to high quality information to put her limited personal observations into a broader context). But there are also times in this video that it is clear she is either lying, engaging in shameless hyperbole, or spreading misinformation she doesn’t believe because she thinks her audience will. Indeed, her conviction in this video seems to be that no COVID-19 myth, no matter how far out, is too ridiculous to include. She basically admits this at several points and I want to be fair and give her credit when we get there; but I’m also not going to shy away from stating that she is almost certainly lying at the times when that is clearly the case. People will die because they attend to this video, and I think being fair to her context and intentions has to cut both ways.
Second, I am not going to rehash arguments that have been made thoroughly and extensively elsewhere.
I’ve written on the evidence of hydroxychloroquine’s ineffectiveness for COVID-19 (Budesonide too) more times than I can count and won’t do it again. Instead I will shamelessly link to my old posts, or better external sources, which you can read if you wish. I’m also not going to argue with every point Dr. Gold makes because she throws out almost every COVID-19 conspiracy theory and myth at some point in the course of the video, even those that have been systematically disproven over and over again. I may touch on masking and other issues very lightly and provide links, and other sections I may skip over almost entirely. This video is 1 hour long and the focus needs to be on the vaccine misinformation, which she begins sharing at about 23 minutes in; so I’m going to pass some things by. Silence does not imply agreement or ceding the point, but I’ve got a full time job and a family I really like, and don’t have 10 hours to spend debunking this video. If there’s a point she makes that you find particularly salient but that I don’t get to, please say so in the comments and I’ll see what I can do.
3 Things Dr. Gold is going to do
I usually like to only debunk/analyze as we go, but this video is so long that we will save a lot of time by touching on the 3 most common “tricks” Dr. Gold uses in her talk. I don’t mean “tricks” as in deception, though some are that; I mean these are debate tactics or rhetorical maneuvers that make her arguments more convincing to the unwary listener without really adding to the actual content of her presentation. I think if you’ll watch the video with these 3 things in mind and can see when she is doing them, you’ll find a lot of this content far less convincing than if we merely reacted to each particular instance.
1. The COVID-19 virus is dangerous or not dangerous when it suits my point.
This is one we’ve seen consistently with misinformation throughout the pandemic, especially from doctors and especially when talking about unproven treatments. The very same doctors who will tell you that the virus isn’t really dangerous and you shouldn’t wear a mask or social distance will then turn around and rely on extremely small numbers of patients to prove that their intervention is the cure, assuming those patients would have had a bad outcome without it.
But you can’t have it both ways. You can’t use a high recovery rate among certain demographics as proof that preventing the virus simply isn’t necessary, and then use a patient in that demographic recovering as proof that your treatment works. You can’t say that the death rate for a 25 year old patient is “0.02%” so you shouldn’t even worry about it, as Dr. Gold states later in the video (will look at the context and impact of these numbers at that time), and then turn around and say that the 25 year old you treated not dying proves your treatment saved their life.
This is a true contradiction, but it’s explicable when you realize that the doctors who hold these contradictory views derive them from two separate thought processes. When talking about the pandemic being blown out of proportion, they are speaking from a political and economic standpoint that wishes, as we all wish, to get life back to normal as soon as possible; the evidence of the danger of the pandemic, which has now killed over 430 thousand Americans, simply cannot change that philosophical belief, no matter how overwhelming the evidence becomes. But when they are talking about their favorite treatment being ‘the cure’ for COVID-19, they are consulting extremely small samples of patients that constitute nothing like substantial anecdotal evidence, much less reliable data. Besides the fact that most of America’s Frontline Doctors are nowhere near the front line (no pay wall but you have to register for that article. Sorry), the way they have admitted to selecting their patients and “diagnosing” COVID-19 make their clinical experiences entirely unreliable. We talked about that more with Dr. Stella Immanuel’s and Dr. Ivette Lozano’s viral videos.
Watch for this as you go through Dr. Gold’s talk. In each section, is she working from the assumption that the virus isn’t really dangerous and therefore you don’t need masks or vaccines, or that the virus is universally deadly and therefore it’s vital that you have access to unproven treatments for it? Most importantly, is she working from a consistent assumption or does it fluctuate based on the point she is trying to make?
2. Everyone is lying to you but me.
I know it feels really calloused to even point this out, but I’d argue it’s more calloused to actually engage in this type of argument. But Dr. Gold does this over and over again. Each time she tells you that historically truthful sources of information like the WHO or the CDC are known for dishonesty or unreliability, each time she tells you that all the doctors and scientists are ‘in on it’ or ‘have fallen for it’ or ‘have drunk the Kool-Aid’, she is saying the traditional sources you would get your health information from can’t be trusted anymore because they are either lying or have been deceived themselves. This is a transparent, mean-spirited, and petty rhetorical trick; it’s also devastatingly effective when you are the one telling people what they want to hear. “Trust me, not them” is not a good standard of evidence, but it works when someone already wants to trust you, as the people she is speaking to almost certainly do. They are comforted because it alleviates the cognitive dissonance of going against the medical experts and what you are being told by people in your own community. If you don’t know them or don’t like them they are lying; if you like them and know them, they have been duped. It gives you a position of both moral and intellectual superiority to believe that you alone are in a position of being both knowledgeable and truthful, and that is the gift Dr. Gold is giving to her audience. It is seductive.
There is also no counterargument that works against it, because if you don’t know me then you can just think that my whole rebuttal is simply lies (ouch), and if you do know me and like me you can think that I’ve been duped myself; that’s the whole point of the ‘you can’t trust anyone but me’ trap. The only way to avoid being deceived by this is to consistently think of this video in the context of your own life and not in a vacuum. You know people who have been harmed by COVID-19, even though Dr. Gold would tell you those were anomalies or they were really harmed by something else altogether. You probably knew people who died from it who weren’t going to die this year otherwise, even though she claims that’s the only people this hurts, people who would have died anyway.
And you know medical professionals. Dr. Gold and a handful of doctors are taking an extreme minority position and telling you that over a million other doctors are wrong or lying; that we are part of the medical establishment and being told what to do by the government, big pharma, and whoever else (by the way, I’ve literally never been told what to do by either the government or a pharmaceutical company when it comes to practicing medicine. Not once). But you know some of those people and you don’t know Dr. Simone Gold. Those other doctors aren’t nameless, faceless, nefarious intellectuals. They are your local Family Medicine doc or Pediatrician you go to and bring your kids to and ask for advice on medical issues ranging from the deeply concerning to the fairly mundane to the kind of embarrassing. They are the nice young resident who took care of you in the ER that time, or the grumpy specialist that nevertheless got to the bottom of your problem. And yes, they are the doctor you didn’t trust or had a bad experience with; but so Dr. Simone Gold’s allies might be. For hundreds of people in Minden, Louisiana, they are that goofy but good natured kid you taught in Sunday School and Youth Group or bought Boy Scout popcorn from for all those years. For some church members in East Texas, they are that son-in-law of the church secretary who visits with his beautiful family whenever they are in town. And for lots of random people across the country, they are that young man who stopped to help you change a tire or gave you a lift when you were hitching, or helped you pick out an over-the-counter medication when you were confused at the local pharmacy even though he absolutely shouldn’t be giving out medical advice in the middle of Wal-Mart. Maybe you don’t know TJ Webb, MD, but you probably knew people as children or as teenagers or young adults who went on to careers in science, epidemiology, and medicine. Those are the people Dr. Simone Gold says are lying to you, and you only have her word to prove it.
That is the context in which you have to think about this claim that ‘everyone is lying’; the context of the real world, where each of those ‘lying or duped’ medical professionals and scientists come from somewhere and have real-life relationships, souls, and histories. We are not a nameless, faceless, monolithic establishment; and disagreeing with Dr. Gold doesn’t make us one.
3. Calling misinformation “truth” and truth “misinformation.”
This is the simplest one but also the most insidious. Dr. Gold spreads misinformation throughout this video, but she is going to claim that her talk is specifically intended to correct or debunk misinformation. This is a false equivalence; she wants to put the information she is sharing, which is believed by a tiny handful of doctors and scientists, on equal footing with the research and clinical experience of millions of scientists, physicians, nurses, epidemiologists, and researchers. Speaking from a widely debunked and extreme minority position, she wants to turn all things COVID-19 related into a ‘he said / she said’ situation and ask you to choose between the two as equally valid and scientifically supported views.
And in a way that’s ok; when presented with false information like that which Dr. Gold shares in this video, you really should decide for yourself based on the evidence. But please keep in mind what the implications are of accepting one or the other. If you decide that Dr. Gold is truthful then you are in effect saying that you agree that there is a wide-ranging conspiracy to deceive the public and cause mass suffering, which involves almost every single doctor, nurse, and scientist you know. And if you believe that, that’s fine; some people do prefer conspiracy theories, or even just want that to be true because it would mean that life could get back to normal sooner. But let’s not pretend that the real life experiences of millions of generally altruistic doctors and nurses is equivalent to the fringe view of a few overtly political physicians. At the very least, the burden of proof rests with the latter.
*WARNING*
The Below Video Contains oh just tons of incorrect and misleading information.
If you are going to watch the video, please also read a counter-argument; either mine or someone else’s.
Minute By Minute Analysis
Part 1: Preliminaries, Hydroxychloroquine, and Masks
0:39 “Experimental Vaccines”
Well that didn’t take long. Dr. Gold will consistently call these vaccines “experimental” because all of us are afraid of being guinea pigs in some science experiment. She is mischaracterizing them and we look at that in detail later on, but she wants you to adopt her terminology now because even the idea of the vaccines being experimental will convince some people not to get them. People will die because of this video.
1:03 America’s Frontline Doctors
Dr. Gold’s organization has been spreading misinformation about the pandemic for going on a year now; here is the first instance of her claiming that they are trying to combat it. Truth is lies, lies are truth.
1:25 “Groups of physicians, scientists, and government agencies lying to the American people”
This is the first instance of “everyone is lying but me”, but certainly not the last.
1:50 ‘The NIH is lying when it says that unless you are in the hospital requiring oxygen there is no treatment available‘
Dr. Gold is going to spend the next few minutes talking about hydroxychloroquine, and you can read my analysis of these claims in any of the many posts where they’ve already been addressed.
But this claim specifically is that the NIH says there is no treatment unless you are in the hospital and on oxygen. Well, here are the NIH treatment guidelines, and I’ve included their summary table below.
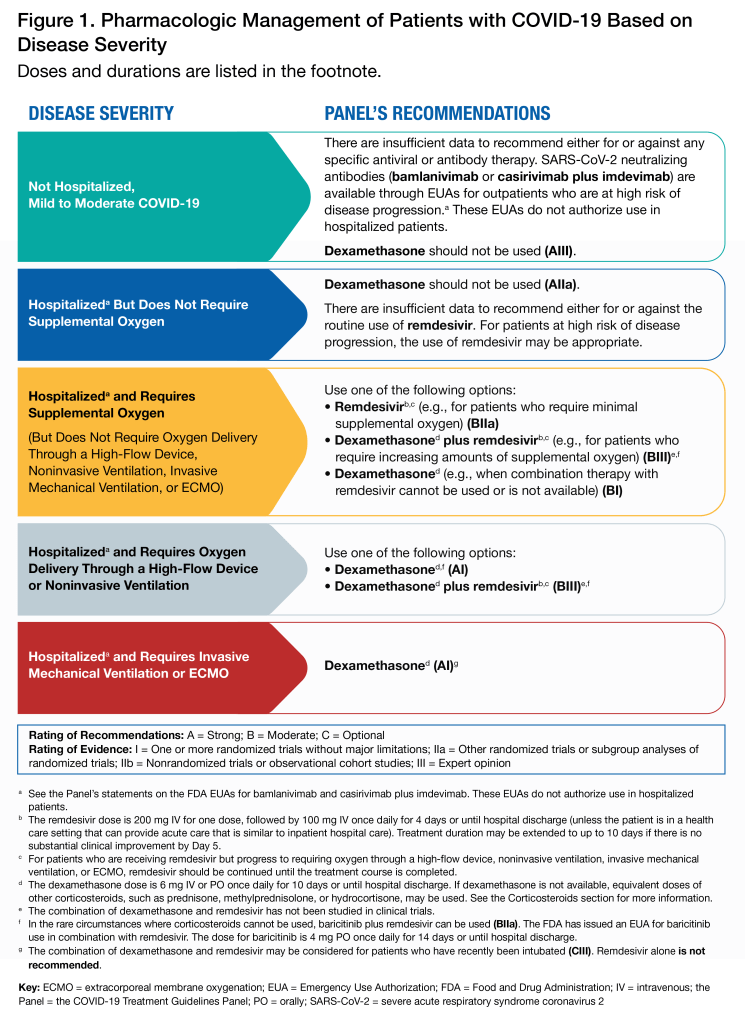
For patients with mild to moderate illness who are not hospitalized, there is some decent evidence of monoclonal antibody therapy and I have referred several patients for this just this past week. This is the same treatment then-President Donald Trump received when he had COVID-19. For patients in the hospital and not receiving oxygen, they recommend remdesivir for those with a high risk of disease progression. And of course, for all patients we are providing counseling on over the counter treatment, supportive care, and anticipatory guidance when they are seen, which any doctor would tell you are the mainstays of treating any illness, whether specific medications are prescribed or not.
So, 1 minute and 50 seconds in we have our first example of Dr. Gold giving a demonstrably false statement. The proof is before your eyes; the NIH treatment guidelines do not say no treatment is available unless you are in the hospital and on oxygen. Will you still give her your absolute trust for another 54 minutes?
2:20 “We were promptly de-platformed”
This is true; there is no denying that the America’s Frontline Doctors Capitol Hill speeches, and most famously Dr. Stella Immanuel’s hydroxychloroquine speech, were taken down from Facebook and YouTube. Again, as that video was full of dangerous misinformation, it’s hard to feel bad about it; but it certainly lends credence to their claims of censorship (by private companies and not by the government, but still) and in certain peoples’ eyes lends an air or forbidden truth to their comments.
I would much rather have the arguments understood and then analyzed. I wasn’t able to post a video of that talk but you can read the transcript and my analysis here.
2:29 “This is a crime against humanity.”
Wait, YouTube taking down their video was a crime against humanity? Hmm…
I’m being facetious; she clarifies that it’s the massive disinformation campaign around COVID-19 that’s the crime against humanity. I happen to agree with her, but we fundamentally disagree about who is a part of that disinformation campaign.
2:52 “The vast majority of deaths in America would never have happened.”
Uncanny, we absolutely agree again. When you look at the death rates around the world, every nation, and especially those that took the pandemic very seriously early on, has faired much better than the USA. But the key is prevention of transmission with masking, social distancing, and now vaccines; not ‘give everyone hydroxychloroquine’.
When in your life have you heard a doctor say it’s better to get a deadly disease and then treat it than to avoid getting it in the first place? We are accused of that all the time, but I’ve never actually seen it happen until now. Again, the treatment she is espousing here doesn’t actually work, but that’s beside the point. The very people who will share this video where Dr. Gold promotes unproven treatments and warns against safe vaccines will un-ironically go on to post comics like this one:

3:09 “You need to understand the magnitude of the lie…”
What Dr. Gold is doing here (besides helping fill up her hour, which can be a real challenge sometimes), is repeating to a select audience- both those at this faith healing event and those sharing her video on the internet- misinformation and conspiracy theories they already agree with. This helps solidify her position as a truth-teller and lends additional credibility to the real point of her talk, the concerns she is going to share about the vaccines later. We will go through them as quickly as possible.
3:26 “Its real name should be…”
There’s no important information or misinformation here one way or the other. We do not universally name diseases after their location of origin, though it is sometimes a factor, just like the person who discovered it is sometimes a factor in naming. If anything, we are getting further and further away from eponyms in medicine, and where many people would have talked about “Hansen’s Disease” in the early 1900’s, nowadays we just say “leprosy” like they did in the Bible, except for a few test questions during second year of medical school. Naming conventions for diseases in the age of microbiology focus more on either the name of the pathogen or the syndrome that it causes.
For instance, the name of the dangerous Coronavirus disease that was first identified in Foshan China in 2002 was “SARS”; Severe Acute Respiratory Syndrome; it was never called the “Foshan” virus. In contrast, the next dangerous Coronavirus we encountered in 2012 was called “MERS”; Middle Eastern Respiratory Syndrome, based on the region it was discovered in. The name of the novel Coronavirus we are fighting tooth and nail against now is SARS-CoV-2; Severe Acute Respiratory Syndrome Corona Virus 2, because, you know, it’s the second one. The name of the syndrome is COVID-19 for Coronavirus Disease 2019, which I admit is a little bland for something that has devastated the world.

The only times the virus is called the “Wuhan Virus” (or the more overtly racist “Kung Flu”) is by those who wish to make a political statement; calling it the “Wuhan Virus” is politically or ideologically motivated, not the other way around. Here Dr. Gold is simply making a show of solidarity with those who would like to call it what former President Trump often called it; there is no important ground here, only signaling to her audience which team she is on.
3:38 “Before we discovered…”
What was discovered was that it is a coronavirus similar to the one that causes SARS, not that the Chinese government didn’t like the name “Wuhan Virus.” Remember, it is called COVID-19 and SARS-CoV-2 around the world; the narrative that the US is in China’s pocket (not my field of expertise) simply does not explain the naming conventions for the pandemic.
3:55 “They called it a coronavirus because it is a coronavirus, but that became very confusing to doctors and scientists…”
Nobody was confused. This whole narrative is really weird and insincere.
4:03 “We used to use coronavirus on our charts when we meant a common cold.”
Look I realize I am splitting hairs here, but no. If you did a viral respiratory panel and it showed a coronavirus, sure, you would document that; but otherwise we call those colds “viral upper respiratory infection” or just “cold”, or if it is causing a more specific clinical picture, “viral bronchitis” or “viral bronchiolitis”, etc., or if we are really being lazy just “cough, sore throat, and rhinorrhea (runny nose)”.
When I started listening to this last night and Dr. Gold got to this point, my wife (a Registered Nurse) called out from the other room, “Did she just say we use ‘cold’ and ‘coronavirus’ interchangeably?!” Yes, she did. And no, we don’t.
Again, it’s a non-issue, but I was annoyed by it. Sorry, moving on…
4:59 More Hydroxychloroquine
I’m really going to limit myself to a few comments on this section because I’ve already linked to my other hydroxychloroquine articles above. The biggest things that stick out here:
5:11 We don’t give any medicine out like candy.
5:18 Treatment and prevention of Malaria is a common use of chloroquine and hydroxychloroquine because they have been proven to be effective against that disease. Comparing this to using it to treat COVID-19 is like saying you don’t understand why a doctor won’t give you penicillin for your high blood pressure when they give it out all the time for strep throat. Carefully deciding which medications to prescribe for specific conditions, and then carefully discussing the risks and benefits of them with our patients, is modern medicine. Is Dr. Gold really saying that if a medicine is helpful and safe for some people and conditions it’s helpful and safe for all people and all conditions? If not, then surely she would admit that we have to follow the evidence here.
5:48 I really shouldn’t have to say this, but the key difference here is that Malaria is common in Sub-Saharan Africa and uncommon in the US. She says it herself, but the issue isn’t consumer demand but rather the ubiquitousness of the disease it treats. That said, if hydroxychloroquine really were the miracle drug for COVID-19 that Dr. Gold and others have claimed, I’d join them in calling for it to be OTC with appropriate pharmacist warnings. Sadly it isn’t.
6:43 We have not been hearing about it being unsafe for 10 months because of an organized misinformation campaign against hydroxychloroquine. Does she ever offer a credible theory as to why such a thing would happen, why doctors wouldn’t want patients to have access to this medicine if it worked? The truth is we heard about it 10 months ago as being something we were hopeful might work, and then were sad when the evidence showed it didn’t. We’ve only continued to hear about it since then because doctors like Dr. Gold continue to build conspiracy theories around it.
6:51 “You’ll be suspicious of everything that follows” And that is the point of it being included in this talk.
7:15 “She was so much better”
Here the virus is dangerous, which proves hydroxychloroquine is effective because this patient got better.
7:33 “My medical director called me the next day”
I absolutely will not try to dissect Dr. Gold’s personal experience here and claim that either she or her medical director was in the right. For one thing, we simply don’t have enough facts, we don’t even know what point in he pandemic she is talking about; I know some very good doctors who were using hydroxychloroquine back before any major studies had been done because there was hope the evidence would show it was effective. Those doctors don’t prescribe it anymore, because they have been convinced by the evidence.
What I do want to say is that her example of the medical director coming to her seems intended as a callback to horror stories we have all heard about a hospital administrator or business consultant telling a doctor or nurse how to practice medicine, usually motivated by profits. That is wrong every time it happens, and those people deserve to get fired, fined, and in some instances, serve jail time. I’ve never had one of those situations, but I’ve been in some that came close.
But this isn’t one of those stories. My medical director is an excellent physician who has been practicing a lot longer than I have; I often go to her for professional and medical advice. If she were to offer feedback or even correction on some treatment I was providing that was not supported by evidence or seemed to be due to political motives rather than evidence-based medicine, that would be part of her job. I might not like it. I could argue my case. I could appeal to any of a number of internal resources. I could lay down the gauntlet, do it anyway, and let the chips fall where they may. But I could not accuse her of overstepping her bounds. When she says this is against the law or an example of a ‘corporation practicing medicine for her’, she is knowingly wrong.
7:55 “You haven’t read the science the way I have, you’ll change your mind in a couple of months when you get a little wiser.”
Yikes. I’d say ‘that didn’t age well’ but she just said this 2 weeks ago.
8:38 “The reason he said I shouldn’t prescribe it was because the insurance company didn’t want us to.”
Nope, I don’t believe this for a moment, for 2 reasons. First, Dr. Gold is shamelessly promoting a well worn lie that pharmaceutical companies tell doctors how to practice medicine. It’s commonly believed, it crops up on tv and in movies constantly, and it’s almost an underlying assumption in many peoples’ interactions with healthcare; and it’s 0% true.
I spend countless hours each month helping my patients navigate around their insurance company’s arcane pharmaceutical rules and find the best way to afford their medicines regardless of their insurance status. I often prescribe a medication to one pharmacy, and then print the prescription and a coupon for another pharmacy in case the insurance doesn’t cover it. I pull up GoodRx.com or the Wal-Mart $5 generics list and we tally up the cost of their meds to find the cheapest price and make sure they can afford it. You know what I’ve never seen a class, a lecture, or even a powerpoint slide on and have never given a hoot about since the first day of medical school? Pharmaceutical or insurance company profits. Don’t confuse the broken system with the people who are fighting against it every day.
But the second reason is a lot more straightforward; they are in the Emergency Department, not inpatient in the hospital. The patients are filling their prescriptions at some pharmacy somewhere separate from the hospital, and the medication costs about $15 for a month supply with a coupon; the insurance company doesn’t have to pay for it if they don’t want to, and the ER docs will probably never hear about it. So any intervention or confrontation over this medicine was almost certainly because of the paucity of evidence for it working, not because of financial issues. If Dr. Gold at some point shows documentation that confirms this narrative, I’ll be shocked; I’ll also publicly recant this objection. But it seems to me that she is just retracing a well trodden but false narrative about the toxic control that pharmaceutical and insurance companies have over doctors.
9:17 “My days at that particular hospital were numbered.”
Listen, I can relate here; I once quit an ED job because of financial issues too. The issue? I found out that ER company was sending their patient’s bills directly instead of going through insurance, and worse, marking up the charge for physician services by about 150 to 300%. I never scheduled another shift. So even if her narrative above isn’t true, if she felt that it was I could empathize with her feeling like her career at that hospital was done.
10:22 “It got 20 million views because human beings recognize truth.”
I would be very, very careful about arguing that views=truth. I’m sure there are a lot of youtube videos out there that engaged in less than perfect truth telling but do pretty well. But it’s a nice thought.
13:00 “You have to push back against tyranny.”
Dr. Gold is here advocating against wearing a mask and comparing it to tyranny without offering a single scrap of evidence. The evidence that masks help prevent the spread of COVID-19 is absolutely overwhelming (it’s dated, but it was overwhelming when I first wrote about it back in June, and the evidence is only stronger now). This misinformation video and others like it will cost lives; but she is talking to a group of COVID-19 deniers and advocating for masks, or even remaining neutral, isn’t an option for her.
13:24 Not wearing a mask on behalf of others is a very strange argument.
15:00 “Whether you have COVID or you don’t have COVID you can get yourself a prescription…”
That’s called a pill mill, folks.
15:38 “People just want to go back to normal lives.”
Dr. Simone Gold is absolutely correct here. It’s one of the reasons this medical misinformation is so very seductive, because it speaks directly to our hopes; specifically our hope that we can finally be done with all of this. But the question isn’t whether or not we should be afraid; we shouldn’t. It’s whether our actions are kind and wise, and that in turn is based on whether our information is actually true. Every day, with every patient I test for COVID-19, I tell them not to be afraid; and then we talk about how they can protect themselves and their loved ones from this very dangerous virus.
16:17 “The vaccine doesn’t stop transmission.”
If I get the vaccine, can I still transmit/spread the virus?
16:21 “It actually changes nothing.”
Again, this simply isn’t true. Vaccines are still our best path out of the pandemic while limiting death and suffering. If you are vaccinated, your risk of both death and long-lasting medical side effects from the virus is significantly lower. If your grandparent is vaccinated, your risk of giving them the virus and them dying from it is incredibly lower. No, a few million people having the vaccine has not yet changed the pandemic substantially for everyone; but thankfully that is the path we are on.
17:03 “According to the CDC which is not known for it’s honesty.”
“Everyone is lying to you but me.” There have been multiple examples where the CDC has published confusing, conflicting, or poorly communicated information throughout this pandemic. Sometimes that was because of incompetence, other times because the best information available was just changing so rapidly. And at other times it was because high ranking officials in the Trump administration, with no medical background, were controlling what information was being put out.
If you have any specific examples where the CDC actually lied to the American people during this pandemic, please leave them in the comments. Let’s not just take Dr. Gold’s word that all of the hard working scientists, doctors, and public health workers at the CDC are liars become she’s telling us information that tickles our ears.
And by the way, if you want to see how these numbers Dr. Gold is getting ready to share compare to what the CDC has been saying for months, have a look at this graphic from as far back as October. Don’t let someone tell you’ve been lied to when you haven’t been; check the original source.

17:07 Survival Rate by Age
At this point Dr. Gold spends a few minutes talking about the survival rate for COVID-19 for various age groups. Earlier when talking about hydroxychloroquine the virus was very dangerous; it was remarkable that her patient got better after taking the medication. Now the virus will become benign again except for small percentage of the population.
There are some fine points of epidemiology that we are going to have to guess at since Dr. Gold doesn’t give us complete information. For instance, we will assume she means the Infection Fatality Rate, which includes estimates of asymptomatic carriers of the virus, rather than Case Fatality Rate, which is just those who develop the COVID-19 syndrome; it’s the lower number and, for the point she is making, the best one to use. We also don’t know where she is getting her numbers from, as we will see in a minute.
Two more tricks to look out for (again, I don’t mean ‘tricks’ as in intentionally deceptive, just that these are rhetorical tools to make the data better reflect her side of the argument). First, Dr. Gold is going to give you the survival rate, not the mortality rate. This is incredibly important. When Dr. Gold tells you “95% of people over 70 survive,” you are reassured; the way that is phrased, it’s easiest to see yourself or your loved one in that 95%. If you were to say “5% of people die,” you would be sharing exactly the same information, only now it is too easy (for Dr. Gold’s purposes) to see yourself or your loved one in the 5% group that will die; you might want to take some precautions, like wearing a mask and social distancing, which in general Dr. Gold is against. Indeed, when I read survival rates like 99.5% and 95%, I get really worried; those mortality rates are just astronomical compared to any virus we normally face.
Second, Dr. Gold is grouping all ages from birth to >100 into just 4 age groups. This is going to skew the numbers quite a bit. For instance, if you are 49, your ‘survival rate’ is averaged with those who are 22; but you know (just like I do at age 35) that your resistance to illness and ability to recover from infection is not the same as a 22 year old’s. I don’t think Dr. Gold is being deceptive here; she has a one hour talk and has to make the most of it, and a nuanced discussion of these numbers would take more time. Still, I think one reason for choosing such broad age groups is because the numbers fit her narrative better when they are presented that way.
17:07 Under age 20: Survival Rate 99.997%
Dr. Gold states that these numbers come from the CDC. You’ll notice she doesn’t say the same for any of the rest of the numbers, so I’m not sure if she is using the same source or different sources. But overall this agrees with the most up-to-date research on Infection Fatality Rate. One word on Infection Fatality Rate: Because you have to know how many asymptomatic cases there are (and we don’t), IFR is incredibly hard to calculate. The numbers will fluctuate some based on what method is used to estimate the asymptomatic cases. Throughout this part of the analysis I’ll present a few different studies that arrive at slightly different numbers; but that’s a good thing. Just like minor differences in the Gospels that complement each other is a proof of their authenticity, so different scientists arriving at slightly different numbers by using different techniques is a good way to know the numbers are, in general, reliable. If you had multiple scientists getting exactly the same numbers with different methods, you’d be suspicious; and you’d be right to be. Small differences are a good thing, and just one more proof that the scientific establishment isn’t pushing some big conspiracy on you.
So the Survival Rate for people under 20 is 99.997%. The US population under 20 is about 80 million, so that’s about 2,300 at risk under 20, if our estimates are accurate. So far, we’ve lost about 650 Americans under age 20 to COVID-19 (the CDC uses different age groups from Dr. Gold, so we can’t compare apples to apples here), including two children under 10 years old in Fort Worth, an hour North of here, just a few days ago. Dr. Gold says “There’s nothing to talk about” in this age group, but these are not negligible numbers. Without mitigation, we stand to see four times that number of deaths, even assuming the new variants are only as dangerous as the original COVID-19 strain.
Second, you can’t group 3 year old and 9 year old children together with older teenagers. At age 18, the Survival Rate is closer to 99.992; a mortality rate three higher than that in children.
17:15 Age 20-49: Survival Rate 99.98%
Accepting Dr. Gold’s numbers, this means that 25,400 Americans age 20-49 would be at risk; so far we have lost… about that many. So now we need to look closer at these numbers, since something is clearly off, and unlike for the birth-20 age range we don’t know where these numbers came from.
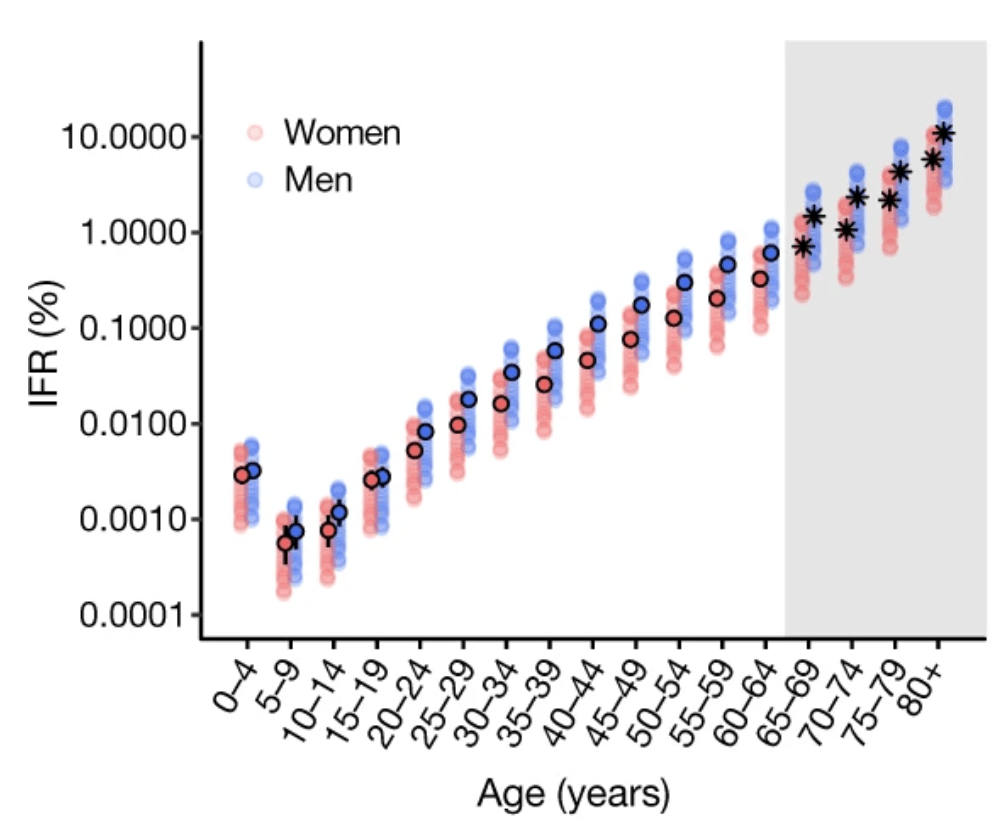
A detailed Meta-Analysis published in Nature in November estimates mortality rate for people age 20-24 at just under 0.01%, and for people age 40-49 at 0.1%; a ten fold difference. Clearly, it doesn’t make much sense to group 20-49 year olds together as one age category. 0.1% is a high mortality rate for a very, very contagious virus like SARS-CoV-2; it means that about 20,000 people are at risk in that age range. If we combine census data with the IFR estimates, we get these estimates of how many Americans would be at risk in this age range:
- Age 20-24, IFR 0.008%, population 21.63 million
- 1,730 at risk
- Age 25-29, IFR 0.011%, population 23.5 million
- 2,585 at risk
- Age 30-34, IFR 0.03, population 22.43 million
- 6,700 at risk
- Age 35-39, IFR 0.075%, population 21.73 million
- 16,300 at risk
- Age 40-44, IFR 0.09%, population 19.92 million
- 17,900 at risk
- Age 45-49, IFR 0.11%, population 20.4 million
- 22,400 at risk
- 22,400 at risk
- Total Estimate from Dr. Gold’s Survival Rate: 25,400 at risk
- Total Estimate from Meta-Analysis Infection Fatality Rate: 67,615 at risk
The mysteriously high survival rate Dr. Gold quotes when clumping together 20-49 year olds give us 25,400 Americans at risk in that age range; comparing the US population with the IFR estimates for much smaller age rangers gives us a total of 67,615 at risk 20-49 year olds. Now, we all hope that herd immunity, whether from infection or from vaccination will mean that we will never see this many deaths among this young demographic; but Dr. Gold’s incredibly low estimates of the danger of COVID-19 in this age group provide a false reassurance and bely how many lives will be saved from mitigation measures, masks, and vaccines.
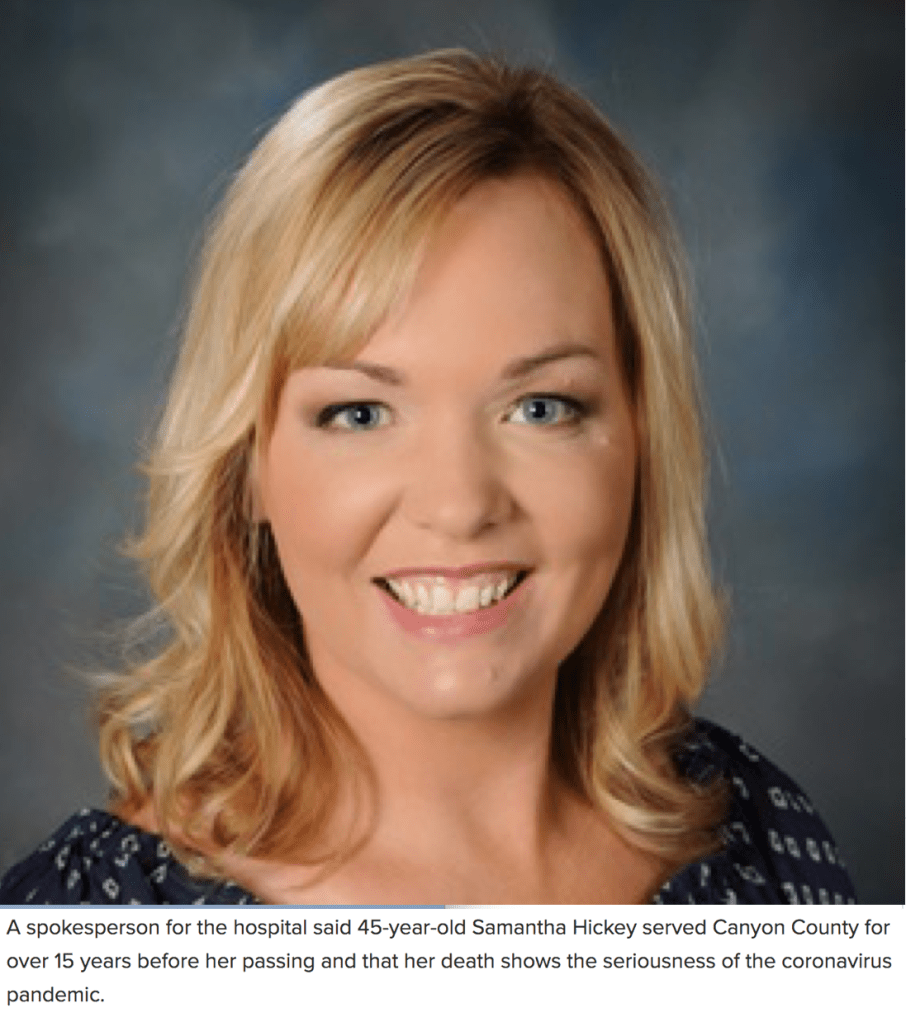
We won’t get to it, but later on (at 41:40) Dr. Gold says that the only people who are dying of this are your 80 year old nursing home residents with bad hearts and other medical conditions, “It’s not your 45 year old nurse, it’s not your 35 year old police officer.” Except that sometimes it is.

17:20 Age 50-69: Survival Rate 99.5%
I won’t go through the numbers for every 5-year age group again, but the further up Dr. Gold gets in these age ranges the further off the survival rates she is quoting seem to be. She quotes an infection fatality rate of 0.5% (Surival Rate 99.5%=Fatality Rate 0.5%) on average for this age range, but this is closer to the fatality rate for 55 year olds. By the time you get to 65 it’s at least 1.1% and as high as 1.4% by some estimates, which is a survival rate of 98.6%. If that sounds like a good number to you, consider the population in that age range; there are over 17 million Americans aged 65-69; that survival rate means that 240,000 of them are at risk of dying without mitigation measures.
We could do the same thing with Dr. Gold’s 95% survival rate for people over 70; that’s the survival rate for 75 year olds, not for everyone above 70. The IFR increases to as high as 15% at age 80, and continues to increase with age; that means millions of Americans are still at risk in this elder population, not to mention the hundreds of thousands who are at risk who are younger.
But even more important than all of these numbers, the fact that Dr. Gold is ignoring, which we’ve talked about over and over again on this blog, is that what makes the pandemic most dangerous for young people is its ability to overwhelm our medical infrastructure. Overwhelmed hospitals, exhausted doctors and nurses, more patients than the staff can possibly provide care for; these factors make COVID-19 extremely dangerous regardless of the Infection Fatality Rate. The COVID-19 survival rate plummets when you can’t get medical care for a severe case of the virus; but so does the survival rate of motorcycle collisions, pneumonia, diabetic ketoacidosis, gangrene, broken hips, closed head injuries, and knife wounds when you can’t get care because there are so many cases of this highly contagious virus. COVID-19 overwhelms healthcare systems and makes everything more dangerous, including itself.
17:55 “The people who die from COVID-19 are the people who are destined to die anyway.”
This is simply not true. I dare Dr. Gold or anyone who believes this to look the families of those who have passed from COVID-19 in their 70’s, 60’s… or 30’s, 20’s, or teens in the eye and tell them that person was destined to die anyway.
But I know what the counterargument will be; “those people really died from something else and it just got counted as COVID-19.” We’ve addressed this in detail before when we looked at information from COVID-19 death certificates a few months ago; those deaths really are from COVID-19. But it doesn’t fit Dr. Gold’s narrative of ‘only the old who are already dying will die from COVID’, so regardless of the facts those deaths have to be discounted. I’m not willing to discount them.
Besides the data we’ve examined above that shows the non-negligible death rates in those in their 20’s, 30’s, etc., and the actual data you can go look at for yourself, which shows a steady progression with age and not a steep increase when you reach 80+, there is one more important piece of evidence that disproves Dr. Gold’s “people who die from COVID-19 would have died anyway” narrative, and it’s something called excess mortality. If most patients who died from COVID-19 would have died this year anyway, as the narrative dictates, then we would see little fluctuation from year to year, including 2020.
In fact, there’s a meme with false numbers circulating on social media that claims just that, and in fact claims that the number of deaths in the US was lower in 2020 than recent years. The popular one looks like this, but I’ve been arguing with people about these numbers for a couple of months now.

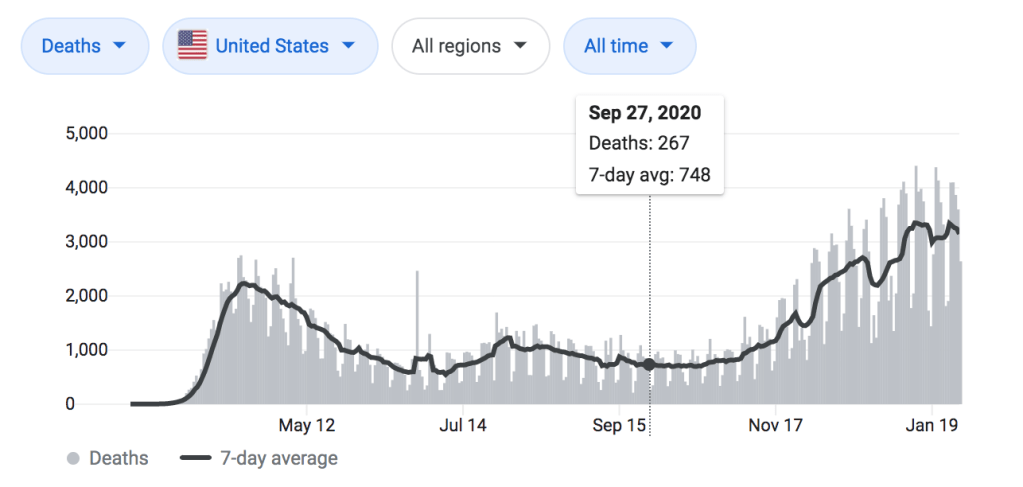
One of the reasons this is convincing for people is because, in general, we are bad at estimating. Even though the deadliest month of 2020 was December, when 2,000 to 3,000 people were dying from COVID-19 per day, this data from November 22nd seemed to convince a lot of people. That’s with 39 days (10 percent) of the year left, and the deadliest days of the pandemic (at that point) to boot. But it’s actually even worse than that; this is based on data currently reported at the time, not data that had been finalized; and it takes up to 8 weeks to finalize the death count for a particular week in the US. So really, this chart is only reflecting the total deaths from about September 27th. Lest we forget how much things changed between the end of September and the end of the year:
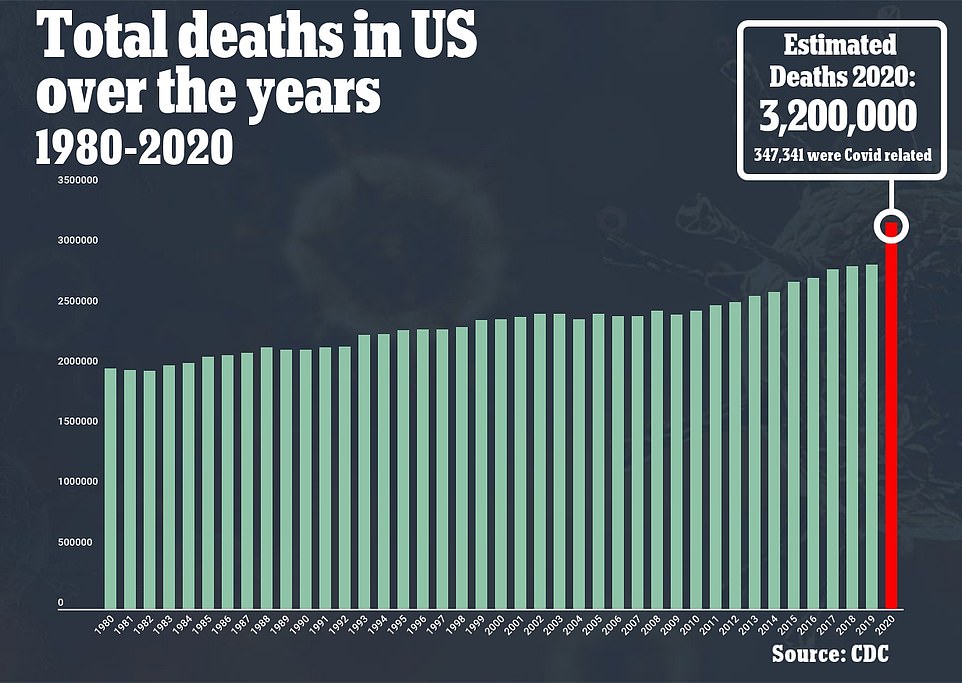
The real numbers are much more dire, but don’t tell us anything we didn’t expect; a lot of people predicted that the US would lose over three million people for the first time ever, as far back as October and November when number of daily cases and deaths began to rise. The real number is 3,200,000, and at least 347,341 of those deaths were from COVID-19. And remember it’s only January 31st; we’ve still got another 3-4 weeks before we’ll know the final death count for 2020.
Part 2: “Experimental Vaccines”
23:10 “You definitely shouldn’t be calling these the COVID-19 vaccines.”
Dr. Gold prefers to call them “experimental biologic agents,” which honestly sounds like a term people might use for psychedelic mushrooms when they don’t want anyone to know that they are using psychedelic mushrooms. I think she’s trying to invoke Agent Orange and other biologic weapons here. But the good news is you can go ahead and call them “vaccines,” because they are vaccines.
23:17 “It is currently in it’s investigational stage.”
A lot of Dr. Gold’s vaccine information is going to try to hype up fears about the vaccines being experimental, untested, or unproven. We all worry about being ‘guinea pigs’ for modern medicine, and depending on your personal experiences, your race or ethnicity, or other personal characteristics those concerns may be very historically grounded. Thankfully, these vaccines are not experimental; not by a long shot. The vaccines have been through rigorous safety trials that were much, much larger than normal. Most trials for new vaccines have between 3,000 and 6,000 participants; these vaccine trials had 40,000 to 60,000. More to the point, about 30 million people have already been vaccinated in the US alone, including the author of this blog. In a minute when Dr. Gold says “I don’t want to be the first person to take new things…” Well, I’ve got great news for her!
If you get vaccinated against COVID-19 today, you are not in any way a part of an experiment.
23:50 “The first problem is that this brand new technology.”
This is an idea that people find particularly appealing because there is such a large kernel of truth in it. These COVID-19 vaccines are the very first vaccines to be made with mRNA (Messenger RNA) technology. That’s actually really, really exciting stuff, but the big question on everyone’s mind is, “how can we trust something so new?” Or to ask it a different way, “how could we trust a vaccine that was developed in just 9 months?
And to that I typically respond that they weren’t developed in 9 months… they were developed in 1 month.

Wait! That’s a good thing! I know that when they make all the pandemic movies about 2020, inevitably there is going to be a scene like this: All of the scientists are laying around their office in the early hours of the morning after another fruitless night of brainstorming and science experiments, surrounded by empty bags of ‘brain food’ like Red Vines and Doritos (or whatever companies pay them for product placement) and inexplicably still wearing their lab coats, when suddenly one of then sits up and says, “Wait, what if we used MESSENGER RNA TO PROGRAM THE CELLS TO BUILD COVID-19 ANTIGENS?!” Everyone sits up and says “That’s it!”, cue the Science Montage. But the truth is that the mRNA technology has been in development since the 1990’s (read this cool article about it from Stat), and was almost ready for use in vaccines when the pandemic hit.
The vaccine companies received the full genetic sequence of the SARS-CoV-2 virus in January; the first vaccine trial participants got their first doses in March, just 63 days later. The whole rest of the time from then until now was spent in clinical trials to make sure the vaccine was safe and effective.
So when Dr. Gold says this is brand new technology she is trying to scare you; but the real story is, this is brand new technology! Yay! This is the culmination of 30 years of research into how to make better, more effective vaccines… And we have access to it!
24:28 “There’s been a tremendous failure of previous Coronavirus vaccines.”
Again, this is true. You can read a lengthy but really detailed article about the state of SARS and MERS vaccines here; it even touches on the problem of Antibody-Dependent Enhancement that Dr. Gold will get to in a few moments. But there are two salient points that Dr. Gold is missing.
First, the SARS coronavirus has been around since 2002 and has killed 774 people, total. The MERS coronavirus has been around since 2012 and has killed 858 people, total. COVID-19 has been around since late 2019 and has killed 2,220,000 people. Please tell me, if you were in charge of strategically allocating resources, funds, and manpower toward vaccine research, which coronavirus would you focus on? The new vaccines are possible because for the past year the collective will of the world has been focused on overcoming the challenges in making successful coronavirus vaccines.
But second, notice what Dr. Gold just said. At 23:53 she said “mRNA technology has never ever been used before for vaccines,” and at 24:28, just 35 seconds later, she said “There’s been a tremendous failure of previous Coronavirus vaccines.” Previous failures… New technology… Didn’t Dr. Gold just give us hope that this time things will be different? I would have phrased it this way: “Unfortunately we’ve never been successful at making effective vaccines against Coronaviruses. Luckily, the new vaccine- making technology they’ve been working on for 30 years is finally ready!”
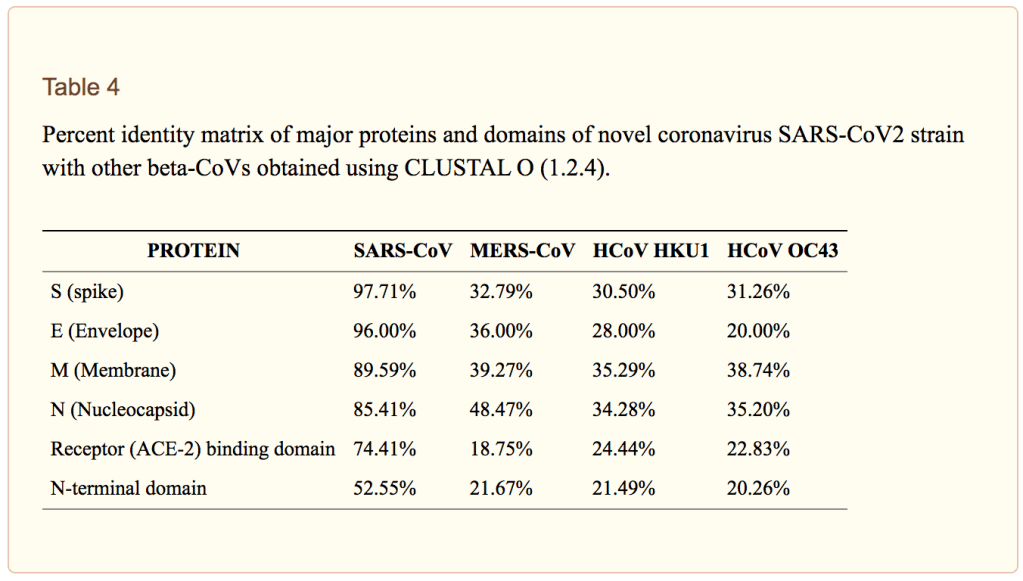
24:53 “You may have heard it called the ‘novel coronavirus’, and I never understood that. This coronavirus is 78% identical SARS-CoV-1.”
I mean, it depends on which proteins of the virus you are talking about. The genetic similarity ranges from 76% to 95-100% depending on which proteins we are talking about. I’m just… Not sure why that matters? It’s a coronavirus, so it’s going to be genetically similar to other coronaviruses. What makes it novel is the fact that it causes a novel disease, COVID-19, which has caused the worst pandemic that the world has seen since The Spanish Flu. You are 99.9% similar to the person sitting next to you, but when your friend shows you their new baby you don’t say, “whatever I’ve seen one before.”

25:16 “We’ve never been able to overcome the hurdles to making a vaccine against a Coronavirus.”
Until now! Yay! The vaccines are 95% effective.

25:25 “There’s no independently published animal studies.”
Besides the fact that this technology has been studied on animals for 30 years now, this just isn’t the way we conduct clinical trials. Maybe Dr. Gold is hedging here with the term “independently” and wants a particular standard of non-involvement of the vaccine designers with animal studies, but if so that’s special pleading; it’s common for vaccine manufacturers to co-author academic papers with independent labs, and both contribute different information to the paper; after all, they have to send some of the vaccine before it can be tested on the animals at the lab.
So if Dr. Gold is really just saying there needs to be data from animal studies about the safety of these new mRNA vaccines, well great news:
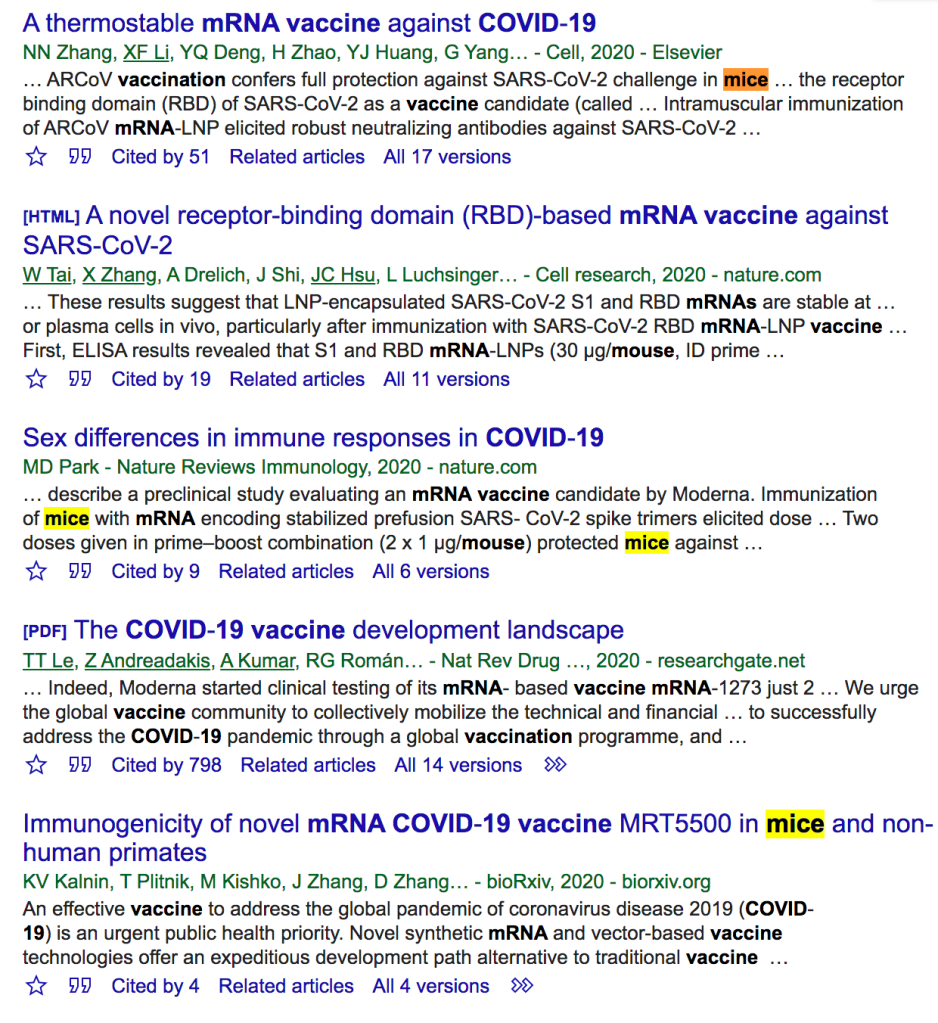
There is substantial, published data on animal studies both for mRNA vaccines in general and for the COVID-19 vaccines specifically. Here’s an AP Fact Check on the topic if you want to learn more.
Dr. Gold goes on to mischaracterize the status of animal studies further, at 25:45 saying “the animals often die in the end, and unless we know that we don’t know if it’s safe to give to humans.” So in 20 seconds we have gone from not having full access to the results of independently published animal studies, which isn’t true, to not knowing whether the animals died. That’s a pretty big jump. (There’s also a ‘Schrödinger’s Cat’ joke in there somewhere but the internet has too many of those as it is).
25:59 Antibody-Dependent Enhancement (ADE)
Immune enhancement is a very real concerned, and one that has been hotly debated within research circles since the beginning of the pandemic, especially in regards to severe COVID-19 cases and the potential role of vaccines. Here’s an article from way back in May 2020 (what is that, like 8 years ago now?) about this exact issue. The specific proteins chosen for the mRNA vaccines were chosen carefully and specifically to avoid this problem, and moreover, this is exactly why we do animal studies and clinical trials.
The Moderna and Pfizer trials were simply huge, with ten times the number of people participating than is typical in a vaccine trial; and no evidence of Antibody-Dependent Enhancement was found. The Nerdy Girls over at Dear Pandemic have a short but great social media update on it from just a couple of weeks ago:
27:21 “Stop Medical Discrimination .Org”
I had to do a double take and rewind (I’m old) the youtube video at this point, because I couldn’t believe what Dr. Gold just said. Do we have some common ground? Health equity, medical discrimination, and American medicine’s history of unequal treatment of people of color, ethnic minorities, and women is a huge issue for me, and my clinic is involved in this work every day. If Dr. Gold has a website devoted to stopping medical discrimination, I will absolutely sign-up, even if I disagree with her about pretty much everything else.
I went to the website. It’s an America’s Frontline Doctor’s Petition to stop ‘forced experimental vaccination’, which is a thing that is not happening (so I guess it worked?).
This is pretty gross, to be honest. Discrimination in medicine is a real thing and one of the biggest obstacles both in patients receiving equitable care and in physicians building mutual trust. It is experienced every day by Black Americans, Native Americans, Hispanic and Latino Americans, people who are LGTBQ+, those who struggle with obesity, the disabled, the deaf, the blind, women… Really anybody who isn’t like me; an able-bodied, fairly young, straight white English-speaking male, which we have decided is the standard for “normal” to the great detriment of everyone else (not to mention the peril of our souls). It also applies to those who are discriminated against for work, housing, etc. because of their medical conditions. Personally I’m not ok with America’s Frontline Doctors co-opting either.
Looking ahead, we are going to talk about this later in the video as it relates to Dr. Gold’s complete misunderstanding of racial healthcare disparities (but honestly, I’m glad she’s even mentioning it, even if she gets a lot of the concepts completely backwards). My next blog post will focus heavily on the history of American medicine’s research abuse towards African Americans specifically, and the work Black scientists, physicians, and community leaders have done to ensure the vaccines are safe, and the work they are doing to ensure their communities have equal access to vaccine-mediated protection against the virus. That will be later this week, but in the meantime… You should go read Harriet Washington’s Medical Apartheid, and listen to her 6 minute NPR interview about the vaccines and the problem of how Black Americans can trust new medical technology: Race and the Roots of Vaccine Skepticism.

27:33 “Some of the other things you’ve seen in the news.”
Here Dr. Gold is using “in the news” to mean “on Facebook”, but that’s fine. Kudos to her for skipping over some of these that have been disproven, though I suppose she felt she needed to mention them for anyone in her audience who had seen this misinformation already. For what it’s worth, here’s my analysis of the COVID-19 Vaccine Bell’s Palsy video that came out a few weeks ago.
28:10 – 30:04 “Has anybody heard of potential fertility problems with this vaccine?”
Based on her response I assume that many hands were raised, which isn’t surprising; this has been popular misinformation for months now. I’ve written about it before and since Dr. Gold isn’t actually adding anything new, we’ll move on. The COVID-19 vaccines do not cause female infertility; please feel free to read about it on my Vaccine Q&A post linked above, or any number of fact-checking websites.

30:09 “We simply don’t know.”
“Well you can’t possibly know” is the last redoubt of the lazy skeptic. No scientist would ever claim 100% certainty about what might happen, and the lazy skeptic will take that tiny element of doubt, which is really just a protection against hubris, and expand it until there is enough space for any debunked objection or pet theory they want to store there. There are multiple lines of evidence against the possibility of the new vaccines causing infertility, as I examine carefully in the above link, including many examples of women who have become pregnant after completing one or both doses of the vaccine despite being on birth control to prevent pregnancy. Moreover, there is not a plausible theoretical mechanism by which they would cause infertility. Making irrational, unproven claims and then when they are disproven saying “well we can’t know for sure!” isn’t science; it’s fear-mongering.
Part 3: COVID-19 Vaccines and Racial Healthcare Disparities
I don’t always get to watch these videos all the way through before beginning a response, and especially with the minute-by-minute format I tend to write piecemeal as we go through the video (listen, pause, think, read, think, type, repeat). After being so offended that Dr. Gold would call her anti-vaccine petition website “Stop Medical Discrimination,” I was surprised- and not necessarily unpleasantly surprised- to see her spend so much time on the issue of race and COVID-19 vaccines. In fact, with the exception of her group’s recommendations about getting vaccinated (spoiler: they prohibit or strongly discourage it for almost anyone), the rest of the video focuses on this issue. It’s 11:52 PM on Sunday night, so we won’t make it to the recommendations; if you’ve read this far and you still trust Dr. Gold’s analysis, there is nothing I can say at this point to convince you not to follow her advice; I just hope you’ll follow more reliable medical experts instead, and at least talk about it with your doctor.
I am also anxious to get to my next blog post, which coincidentally or not, is 100% about race and the COVID-19 vaccines, and specifically the question of how Black Americans could trust these vaccines in light of America’s long history of medical research abuse. The main point of that upcoming post is to share resources directly from Black scientists, physicians, researchers, and healthcare professionals; but I’m also going to be taking a look at the history of medical research abuse towards African Americans and at the current pandemic’s disproportional impact on Black communities. In that sense, while the post has nothing to do with Dr. Gold, some portions of it could be seen as a response to her comments in during this section of the video.
For now, I want to say three things to introduce that article, which I hope you’ll join me for later this week, and to conclude this minute-by-minute analysis of as much of Dr. Gold’s hour long talk as I could make it through.
First, I am very, very glad that Dr. Gold is talking about this.
There are a lot of Dr. Gold’s comments I disagree with, and certain points where her analysis and conclusions are essentially backwards. But the fact that she is talking about it is a good thing. The history of medical abuse and research exploitation of Black Americans is one that is too often waved off as one or two isolated examples (Tuskegee) or ignored completely, especially by white doctors. Meanwhile, this history is part of a common experience and shared cultural narrative among Black Americans, and the disconnect between it being known by the group who has experienced it and unknown or unmentioned by the group that perpetuated it can create a tension that is absolutely deadly to the trust the doctor-patient relationship is built on. Dr. Gold is a great example here, in that she acknowledges some part of that history, and in front of a predominantly white audience.
Now, that doesn’t mean I think Dr. Gold’s talk is useful or good; her information on COVID-19 and the vaccines is all wrong, and so her interpretation of important race equity measures in vaccine distribution is interpreted as a racist attack on people of color instead of an attempt to mitigate already existing injustices. She happens to have it exactly backwards; but if she really believes everything she has said in this video, and I think she believes an awful lot of it, then it’s likely she believes her own analysis here, too. Because it isn’t accurate, the net effect of this part of her talk, were it heeded, would be to worsen the already severely inequitable impact of COVID-19 on communities of color, and obviously using that history to that end is incredibly problematic. But at the very least, talking more about that history is a good thing in itself.
Second, Dr. Gold is absolutely underselling the history of harm done to Black Americans by medical science.
Dr. Gold mentions a few specific examples of vaccine reactions that were worse in African Americans, and (I actually can’t remember now if she does or not) mentions a few other examples of racially motivated medical harm. But the true history spans 400 years and is far worse than anything I ever expected, even reading and learning about a few of the most notorious examples in college and medical school. We will look into this in more detail in the upcoming post, but I strongly encourage you to read Harriet Washington’s book, Medical Apartheid.
Third, Dr. Gold is utterly confused on the concept of racial healthcare disparities.
Dr. Gold spends a lot of time arguing that Black communities have not really been more severely effected by the pandemic. Of course, the pandemic is having a more severe impact on Black communities, and Hispanic/Latino communities, compared to their white neighbors, so this feels an awful lot like a magic trick; Dr. Gold is going to make the disparities disappear before our eyes. And the two methods she has chosen? First, to explain away the worse impact of COVID-19 not by race but by economic and social circumstances that place people at disadvantages in terms of health outcomes, and then controlling for all of these, to show that race disappears as a factor. And second, to point to Africa and say that ‘if the virus isn’t killing people at a higher rate in Africa, it must not affect Black people worse.’
It’s really hard to tell if Dr. Gold is in earnest here, but if she is then she really believes that when we say “Black Americans have been hit harder by COVID-19 than white Americans,” we are saying “COVID-19 makes you sicker if you have more melanin”; a position held by exactly zero doctors, epidemiologists, and public health experts.
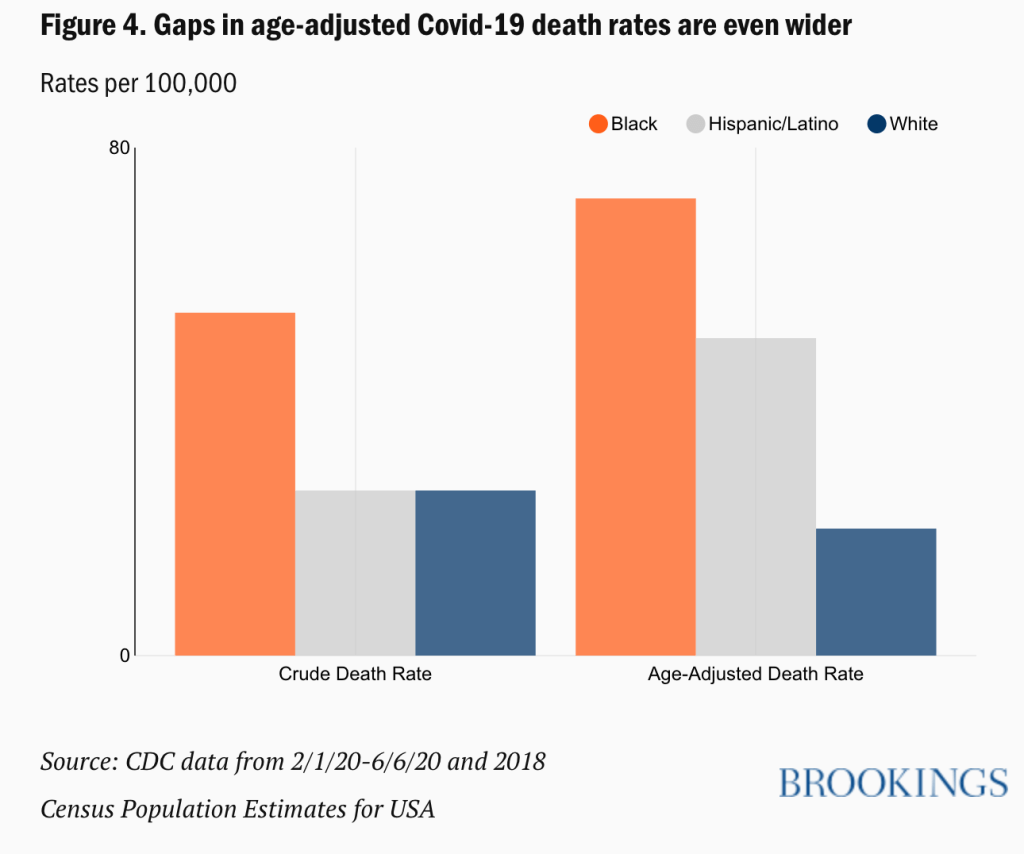
When we look at the shocking statistics, like the fact that the death rate in any given age range for Black Americans is equivalent to the death rate in White Americans 10 years older, what we are really looking at is the ongoing legacy of food desserts, inequitable access to wealth, intentional destruction of Black communities, mass incarceration, redlining and planned poverty, barriers to medical access, and every other atrocity that makes up 400 years of systemic oppression.
Sure, let’s say for the sake of argument that if you controlled for every social determinant of health, every area in which Black Americans have experienced discrimination and continue to today, the gap in COVID-19 between Black and white Americans would completely disappear (it leaves out discrimination within healthcare, but again… for the sake of argument). Why would that matter? Does a statistical linear regression that eliminates the results of oppression actually alleviate oppression, or just make it more palatable because we can rationalize away healthcare disparities without the discomfort of actually examining root causes?
The fact that there is no genetic factor that makes COVID-19 more dangerous for Black people is exactly the point; it’s the injustices that Black Americans already experience, especially regarding healthcare access, that make the pandemic more dangerous. That is why efforts have to made to ensure Black Americans have equal access to the COVID-19 vaccines, because they are the best tool we have for mitigating the risk of the virus; and it is exactly why Black leaders like the Black Coalition Against COVID-19 are coming together to provide good, reliable information and to dispel COVID-19 myths, so that Black Americans can choose whether or not to get vaccinated with confidence, and so that they will have increased resilience against medical disinformation like Dr. Gold’s video.
I hope you’ll join me to talk more about this later on this week. In the meantime, please check-out the Black Coalition Against COVID-19 and the other resources I’ve linked to above.
Black Coalition Against COVID-19

