The full, ironic title of this blog post is actually “Why would any Black American trust these new vaccines? A white doctor’s perspective (because, you know, that’s exactly what we need more of),” but it was too long to fit in the title heading.
As a white, male doctor, I am not the best person to write this blog post. Thankfully I am not the only person writing and talking about this, and am in fact a late comer both to the issue of higher rates of vaccine skepticism within medically marginalized communities and to the larger issues of racial health equity and healthcare justice in general. Much of the work that has already been done in this area comes directly from Black physicians, scientists, healthcare workers, and community leaders who are concerned about the disproportional impact the COVID-19 pandemic has had on people of color, and have been working hard on behalf of their communities to verify that the vaccines are trustworthy and effective, and to ensure equal access to this lifesaving intervention.
I believe those voices are far worthier of your time than this post, whether you yourself are a member of a medically marginalized group trying to decide about the new vaccines or, like me, someone who just wants to gain a deeper understanding of the ways that American medicine’s history of racial discrimination and research exploitation have contributed to ongoing healthcare disparities and earned mistrust. That’s why I’ve flipped the usual structure for this post and have placed additional resources and reading as the first proper section, instead of tacking them on at the end or dispersing them throughout the essay. Many of the resources I’ve included come directly from my Black peers in medicine, or our colleagues in research or community health.
So I write about this topic today not because I believe my perspective is the most important one or because I believe I have something particularly unique to add to the conversation, but rather because I believe this issue is so important that we should all be talking about it. Further, I am writing because a certain number of African American men and women have already entrusted me, as their primary care doctor, with the the sacred responsibility of helping them navigate these issues as they make decisions about whether or not to trust the vaccines, and because a good portion of my time over the past few weeks has been spent doing that work. And finally, I am writing because the vast majority of those medical research atrocities that laid the groundwork for the dilemma many Black Americans face today were committed by people within a group I belong to: white, male, American doctors. And even though I claim no kinship with their ilk, and believe that in breaking their sacred oath and committing grievous harm against their fellow man they have forfeited the title of “Physician,” nevertheless I have benefited in various ways from those crimes, and believe that a responsibility rests specifically with white doctors to do whatever we can to bring that history to light and mitigate its consequences. We should not strive to dominate the conversation, as we have so often done; but neither can we stay silent and remain complicit in that exploitation.
Contents:
COVID-19 Vaccine Resources from Black Medical Experts
The Problem: A History of Racist Medical Research Abuse
The Other Problem: The Unequal Burden of COVID-19
My Conversations with Black Patients
COVID-19 Vaccine Resources from Black Medical Experts
If like me you find that you only have a limited amount of time to read today, I would recommend the following resources; you can always come back to my blog post later.
In other words, start here.
Black Coalition Against COVID-19

BCAC19 is a DC area coalition of Black doctors, scientists, healthcare workers, community leaders, academics, and political voices working together to stop COVID-19 misinformation and rebuilt trust in medicine, in order to help Black communities fight the pandemic.
On their website they host public health resources, a COVID-19 FAQ, and town hall videos with medical and community leaders discussing issues around the COVID-19 vaccines.
“Love Letter to Black America”
The Black Coalition Against COVID-19 has also produced this short but important video touching on the importance of trust and accountability in every step of the vaccine creation and rollout process.
“Why distrust for COVID-19 vaccines may be higher in African American Communities”
This video and article focus on Jeff Fard, founder of the Brother Jeff Cultural Center in Denver, and his work on combatting the health consequences of COVID-19 on his community. It then branches out to look at what Black-led medical institutions and organizations are doing to support communities of color across the country during the pandemic.
“The Black scientist who helped develop Moderna’s COVID-19 vaccine just got her first shot“

One of the many excellent articles about Dr. Kizzmekia Corbett, PhD, Virologist and one of the team leads who helped develope Moderna’s mRNA vaccine (the one I and so many of my colleagues and patients have already received).
Personal Essay by Dr. Lisa Fitzpatrick, MD, MPH

A featured essay in Business Insider magazine, written by Infectious Disease expert Dr. Lisa Fitzpatrick. “I’m a doctor who volunteered to get one of the first coronavirus shots. Here’s why I got involved, and what the side effects have been like.”
Waco COVID-19 Vaccine Townhall, 1-21-2021
Local Resource: This is a Waco COVID-19 Vaccine town hall led by African American community leaders, from just a couple of weeks ago. It features Dr. Terri Woods-Campbell, a former teacher from my days in medical residency, and one of several Black, female Physicians who trained me in surgical skills over the years.
Race and the Roots of Vaccine Skepticism
This is a short NPR interview with one of my favorite historians, Harriet Washington, author of Medical Apartheid: The Dark History of Medical Experimentation on Black Americans from Colonial Times to the Present. She discusses the Tuskegee Syphilis Study, but also the much broader history of medical research abuse and exploitation of Black Americans of which the Tuskegee study was only the most widely known and notorious example.
The Slave Who Helped Boston Battle Smallpox
This one is more academic but offers such an important perspective on the vaccines. It shares an account I first discovered in the pages of Medical Apartheid; the story of an African man known only by his slave name, Onesimus, and how his knowledge of traditional African healing practices and the techniques of variolation saved hundreds of lives from Smallpox and pointed the way toward the future of vaccination science.
The Problem: A History of Racist Medical Research Abuse
I’ll start with a personal story (so bear with me). During my first clinical rotation during 3rd year of medical school, I worked with an upper level resident who despised me. And she had good reasons. I was really struggling academically at the time and my medical knowledge was far behind my peers. Just as importantly, I was a rotation behind them in 3rd year clinicals; it was my 1st rotation, but their 2nd, a lifetime in terms of clinical experience and ability to contribute to a medical team. All of this together meant I was a weak medical student (in medical education we inexplicably still use words like “weak” and “strong” to describe people who struggle with different aspects of the incredible burden of practicing medicine) and, in all honesty, a big drain on her teaching time and resources.
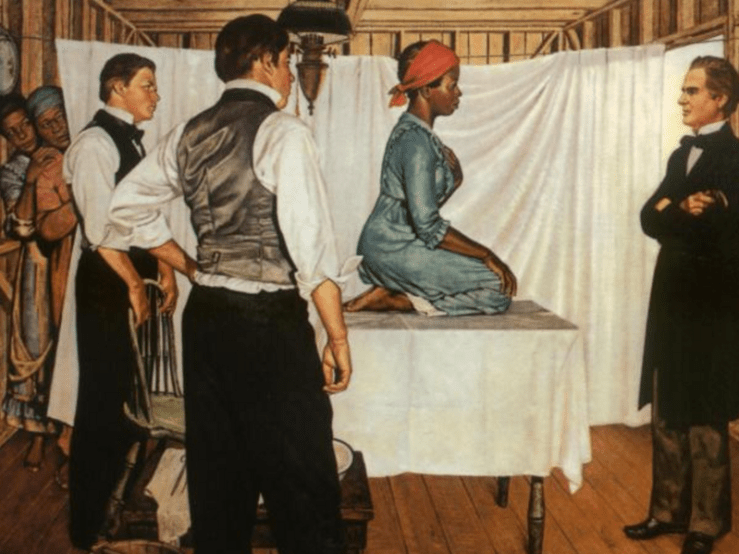
One day during lunch, the program director was lecturing on the history of Gynecology and the techniques and instruments invented by Dr. J. Marion Sims, the “Father of Modern Gynecology,” in Montgomery Alabama in the early 1800’s. The program director posed this question, seemingly rhetorical: “Historically, medical researchers have not always had access to enough volunteers for new techniques and medicines, so who have they used when volunteers weren’t available?” I was a weak med student but I at least had a liberal arts education and knew a little about history, sociology, and moral philosophy, so I answered; “minorities and the poor.” My upper level resident clearly interpreting this as either an off-color joke or even an endorsement of such practices, and generously wanting to save me from immediate expulsion from medical school, shot out her hands in a gesture meant to quell the coming storm and exclaimed to the whole table, “He’s joking. You’re joking, right? Tell them you’re just joking”
But I wasn’t joking, and said so; those groups were exactly who had been used for medical research when the experiments were too dangerous or degrading to recruit volunteers, and it was pretty clear that that was exactly where the program director was headed in that talk. We spent the rest of the lecture learning about the abuse and violent exploitation of poor, Black slave women that had enabled Dr. Sims to perfect his techniques before using them on the patients actually meant to benefit from his research; wealthy whites. These techniques, practiced on slaves without anesthesia and often resulting in infection or other severe complications, eventually made his name famous and led to his becoming the president of the American Medical Association. Only recently has Dr. Sims lost some of the celebration he attained in life because of this history. (The brief slideshow below shows his statue being removed from New York’s Central Park in 2018; you can read about it on NPR from the link provided)




‘Father Of Gynecology,’ Who Experimented On Slaves, No Longer On Pedestal In NYC
But before I run the risk of anyone thinking the above is a story of my wokeness as a medical student (exploitation of allyship, anyone?), I was anything but. I had got the answer right that day (probably for the first and last time during that 2 month rotation) more because I was good at guessing what a lecture was about from the intro than any actual insight into issues of race and justice. I had learned about the Tuskegee Syphilis Study in college, I learned about J. Marion Sims that day in med school; and later during residency I was confronted constantly with the realities of racial healthcare disparities today. And that was it. I was aware of three ‘situations’ out of a 400 year history of abuse, violence, neglect, and exploitation. And for several years, though I grew slowly in this area and fought for healthcare justice 80+ hours a week, I remained essentially ignorant to the actual scope of American Medicine’s racist history (and, you know, racist present).
And if I’m being perfectly transparent and honest, I was at times really frustrated by how my African American patients sometimes seemed to be slower to trust me as their doctor, or to be more suspicious of treatments I recommended, than a lot of white patients. Like many people, I no doubt would have responded to the recent revelation that only 25% of Black Americans planned to get vaccinated against COVID-19 with knowing sagacity; ‘for some reason, Black patients are just more suspicious of modern Medicine. Hmm, oh well… I guess it will always be a mystery.‘
Then in 2020 a chance recommendation led me to download an audiobook (and then later purchase a hardcopy and an E-Edition) of Harriet Washington’s Medical Apartheid. A keen historian and a lover of science and medicine, Ms. Washington started with J. Marion Sims like we did that day in medical school; but then instead of jumping ahead a hundred years to Tuskegee or Henrietta Lacks, carefully traces a thorough but not exhaustive (as she herself states, that undertaking would take a lifetime and would fill volumes) history of clinical and especially research abuse towards Black Americans, beginning with the medical abuses towards slaves that were so common on the plantation and continuing through emancipation and reconstruction, Jim Crow, the Civil Rights movement, into the modern era and the exportation of medical research abuse to Africa where researchers can more easily get around ethics regulations, and finally concludes in the 1990’s and early 2000’s (it was published in 2006) with exploitative research in topics from drug dependence to human reproduction to criminality, all of which continue to pick and choose data to portray ethnic minorities, and especially those of African descent, as less developed, more aggressive, and in many ways less human (though less overtly than the “research” of the 1700’s and 1800’s) than the “normal;” that is to say, white people.
I’ve been thinking of the best way to distill this incredible, earth shattering, 512 page work into a single section of a blog post, and I’m at a loss. We could choose any of the hundreds of examples she gives in the book as reasons why Black Americans might be slower to trust American medicine than their white neighbors.
One that stood out to me was the section “Racism by Numbers” in Chapter 6 when she discusses the US Census of 1840 which showed significantly higher rates of mental illness and disease in free Blacks compared to those still in Slavery; proof, according to Southern plantation owners and their political allies, that freedom was unhealthy for Blacks, that they were too mentally feeble to handle making their own daily life choices. That scientific data was a huge blow to the abolitionist movement against slavery… Until it was utterly debunked as false and based on horrible methodology and underlying racism, by an African American Physician, Dr. James McCune Smith (the first Black American to earn a medical degree, though he had to go to medical school in Scotland to be allowed to do it) and a white Physician and statistician, Dr. Edward Jarvis. I mentioned listening to Medical Apartheid on audiobook; I was listening to this section during a run, and as someone who spends a considerable amount of my time fighting misinformation, was literally whooping and fist pumping throughout the story of how Dr. McCune Smith and Dr. Jarvis systematically dismantled the failed assumptions and overt racist methods of census takers, who had relied on the reports of plantation owners and slavers to collect data on the health of their slaves, and in many Northern cities reported several times more free “negro lunatics and idiots” (medical vernacular of the time) than the actual total free Black population of those towns. If someone had seen me on my run, they would think I was listening to my favorite team winning a big match; and in a way I was, though in this case even the thorough work of these two brilliant scientists was not enough to erase the damage done by the 1840 census, and chattel slavery continued for another 25 years and only ended with the conclusion of the Civil War.
Or we could look at the display of Black bodies- both living and dead- for popular curiosity and scientific study throughout the 1700’s and 1800’s that she outlines in Chapter 3: Circus Africanus and Chapter 5: The Restless Dead. Or radiation experiments conducted without informed consent on Black Americans throughout the early to mid 1900’s, which she outlines in Chapter 9: Nuclear Winter. Or at Chapter 11: The Children’s Crusade, where she reviews the research conducted throughout the 1990’s attempting to link criminality to genetics and hence to Blackness; research conducted on children and under extremely questionable scientific methodology that strived to prove Black Americans were genetically predisposed towards all manner of violence and anti-social behavior.
But instead of a doomed effort to recreate the progression of Ms. Washington’s meticulously researched review of medical research abuse of Black Americans from the dedication to the epilogue, I want to strongly encourage you to buy a copy and read it or listen to it. Below I share the section and chapter titles, but you have to read it for yourself to discover how richly and clearly she explains the long, relentless violence of medical research towards our Black neighbors, friends, and loved ones.

Contents
Introduction: The American Janus of Medicine and Race
Part 1: A Troubling Tradition
Chapter 1 Southern Discomfort: Medical Exploitation on the Plantation
Chapter 2 Profitable Wonders: Antebellum Medical Experimentation with Slaves and Freedmen
Chapter 3 Circus Africanus: the Popular Display of Black Bodies
Chapter 4 The Surgical Theater: Black bodies in the Antebellum Clinic
Chapter 5 The Restless Dead: Anatomical Dissection and Display
Chapter 6 Diagnosis: Freedom: The Civil War, Emancipation, and Fin de Siècle Medical Research
Chapter 7 “A Notoriously Syphilis-Soaked Race”: What Really Happened at Tuskegee?
Part 2: The Usual Subjects
Chapter 8 The Black Stork: The Eugenic Control of African American Reproduction
Chapter 9 Nuclear Winter: Radiation Experiments on African Americans
Chapter 10 Caged Subjects: Research on Black Prisoners
Chapter 11 The Children’s Crusade: Research Targets Young African Americans
Part 3: Race, Technology, and Medicine
Chapter 12 Genetic Perdition: the Rise of Molecular Bias
Chapter 13 Infection and Inequity: Illness as Crime
Chapter 14 The Machine Age: African American Martyrs to Surgical Technology
Chapter 15 Aberrant Wars: American Bioterrorism Targets Blacks
Epilogue: Medical Research with Blacks Today.
Though full agreement might be impossible until you have read the book for yourself, it is at least clear to me that the history of medicine in the United States, and particularly of medical research, is sufficient reason for Black Americans to have increased wariness of anything in medicine that is seen as experimental or unproven. But a natural objection presents itself; “But TJ, most Black Americans haven’t read Harriet Washington’s Medical Apartheid, so that history can’t possibly be the cause of their unease or suspicion.“
Reasonable enough on the surface, this objection fails to recognize the fact that Black Americans, generation after generation, have experienced medical apartheid, whether they have read Ms. Washington’s seminal work or not. Most American’s have at least heard of the Tuskegee Syphilis Study*, and in a hundred news articles talking about African American hesitancy towards the COVID-19 vaccines you will read phrases like “the legacy of Tuskegee” or “almost 50 years since the Tuskegee study.”

But for Black Americans that notorious series of events is not a one-off episode or anomaly in an otherwise untarnished history of medical altruism and benevolence, but part of a shared cultural narrative of the potential dangers of trusting too readily in scientists, researchers, and lamentably, doctors. Harriet Washington says it better than I can:
It is a mistake to attribute African Americans’ medical reluctance to simple fear generated by the Tuskegee Syphilis Study, because this study is not an aberration that single-handedly transformed African American perceptions of the health-care system. The study is part of a pattern of experimental abuse, and many African Americans understand it as such, because a rich oral tradition has sustained remembrances of pain, abuse, and humiliation at the hands of physicians. We should remember that, as Vanessa Northington Gamble, M.D., director of Tuskegee University’s National Center for Bioethics in Research and Health Care, averred, “many African Americans fear and distrust Western medicine who have never heard of Tuskegee.”

So yes, that ‘25%’ statistic is incredibly disheartening, but it’s also understandable once we know something of the historical context of the relationship between modern medicine and people of color. And while these new vaccines are not experimental and fears of being a “guinea pig” by taking the vaccine really are unwarranted for anyone, those concerns are common among many people of all racial and ethnic backgrounds in our current climate of mistrust and disinformation; and it is not a mystery that those fears might be stronger among Black Americans, with the weight of 400 years of medical and research abuse behind them.
*A note on Tuskegee
I would be remiss if I didn’t at least touch on a the basics of the Tuskegee Syphilis study, though Medical Apartheid does a much better job than I can. This was a study that was run by the US Public Health Service in Macon County, Alabama from 1932 to 1972. The full title of the study was “The Tuskegee Study of Untreated Syphilis in the Negro Male“, and as awful as that sounds it’s probably even worse than what you’ve heard. The public health service initially recruited 600 Black men from among poor sharecroppers in an impoverished county in Alabama; they chose 400 with evidence of latent syphilis and 200 without syphilis as a control group. There were some treatments for syphilis available in 1932 when the study began, but none of them were particularly effective; nevertheless, not even these were offered to the men in the study at any point, even though they were given dummy pills and told they were being cured. The intention was never to cure them, but to carefully observe and document the progression of the disease from its early stages all the way until death, and then conduct post-mortem examinations to see which organs and body systems had been deranged or destroyed by the unchecked bacteria. Of course, this was not only done without consent, but through active and ongoing deception of those involved in the study.
It gets worse. Alexander Fleming discovered Penicillin in 1928, just 4 years before the Tuskegee experiment began; but it wasn’t used clinically until the 1930’s and early 1940’s. It became standard of care for all manner of bacterial infections by the mid 1940’s, and by 1947- 15 years into the 40 year Tuskegee study- was both widely available and a known cure for syphilis. Not a treatment; a cure. The researchers and even the administrators over the Public Health Service met to discuss whether the research project should end and all of the participants be offered Penicillin. Appallingly, they decided that, no, the study would continue. Their reasoning? Now that a cure for the disease had been discovered, this was the only chance to find out what the long-term affects would be if it was left untreated. Please… Stop and process that reasoning for a moment.
The study continued for another 25 years. Participants became wise to the fact that syphilis was now being treated elsewhere with a simple injection instead of countless check-up visits, seemingly ineffective medications, and steady progression of the disease. Many of the men sought treatment elsewhere at other Public Health Service clinics, one of the few places they could receive affordable care; only to find that their names and information had been sent ahead of them. Those in charge of the study had sent a list throughout the Public Health Service network: these men were part of a PHS study; they should not receive treatment for syphilis outside of the study. I hope I do not have to pause here and explain how antithetical this study was to every ethical principle in medicine, every moral imperative towards our fellow human beings. Participants were tricked and lied to, denied effective, curative medication, and then when they discovered the grift and sought care elsewhere they found that steps had already been taken to block their treatment there as well. Some did manage to get treated, by seeking care in other clinics or providing assumed names in order to get the penicillin; but most had already suffered the devastating neurologic effects of late syphilis… Just as the study designers had intended. The study finally ended in 1972 when news of it was leaked by the media (you know, that mainstream media you just can’t trust…); it was popular outrage that finally shut it down, not any moral or ethical consideration by the Public Health Service or the individual researchers, scientists, or doctors that were involved.
That, in a nutshell, is the history of the Tuskegee Syphilis Study. Medical Apartheid’s seventh chapter, “A Notoriously Syphilis-Soaked Race”: What really happened at Tuskegee does it more justice, and by itself is worth the price of the book. That history is more or less known, especially among Black Americans; and even were it just that, wouldn’t it be enough?
The Other Problem: The Unequal Burden of COVID-19
A recent viral video of Dr. Simone Gold, one of the founders of the COVID-19 disinformation group “America’s Frontline Doctors,” featured a long segment where she accuses the CDC of overt racism for stating explicitly that they both aim to make COVID-19 vaccines widely available in communities of color, and for listing strategies to increase acceptance rates and combat vaccine hesitancy in those communities, including recruiting celebrities and other influential people to encourage vaccination.
On the surface, her claims actually sound fairly reasonable; given the history above, any efforts for medical treatments to target specific racial demographics, and especially a historically (and concurrently) oppressed group, has to be carefully scrutinized. Erroneously believing that vaccines are poison, and that these COVID-19 vaccines are “experimental”, Dr. Gold (had she read Medical Apartheid) would make the claim that the CDC’s efforts today are just the latest in the long sequence of medical research efforts that, intentionally or not, resulted in the exploitation, humiliation, and harm of Black Americans.
And she would be wrong.
The key difference, as Harriet Washington herself points out over and over again throughout her work, is that these efforts by the CDC are therapeutic, not experimental. Dr. Gold’s claims about the experimental nature of the vaccines is demonstrably incorrect (see my most recent blog post), as she herself is well aware. Calling them “experimental” or unproven, or referring to vaccine recipients as ‘guinea pigs’, is merely a scare tactic; and one that could be particularly effective when targeted at groups who already have legitimate grievances against American medical research. It goes without saying, but Dr. Gold is also wrong about the vaccines being dangerous; the safety trials were extensive and rigorous, and the protection offered by the vaccines against a horribly deadly virus is excellent. Rather than being a malevolent attempt to test the vaccines on Black people to make sure they are safe for whites, as was the case with Dr. J. Marion Sims’ surgical procedures in the 1800’s and the radiation trials in the 1990’s, this is an altruistic attempt to ensure that Black Americans have equal access to a treatment that has already been proven safe and effective. Finally, in contrast to those experiments, the efforts to address vaccine hesitancy and combat misinformation within Black communities are being done with not only buy-in, but active leadership by Black physicians, scientists, researchers, and public health experts. This is certainly the case on the national level, where organizations like BCAC19 are working with government and healthcare organizations across the country. But it is also being done on the local level in many places. My own clinic has a list of resources similar to the one in this blog that I often provide to Black patients in the context of a conversation about the COVID-19 vaccines and America’s history of racist medical research abuse. It was created specifically at the behest and encouragement of one of our African American physicians, and vetted by a work group dedicated to race health equity.
Treatment, not experimentation.
Beneficence, not malevolence.
Black leadership, not subjugation.
The effort to help Black Americans get vaccinated against COVID-19 is the polar opposite of the very real history of medical research exploitation Dr. Gold wishes to link it to.
But why is it necessary at all? Because despite what Dr. Gold implies in her video by factoring out the health outcomes associated with our long history of racial discrimination, healthcare inequality is a very real factor in America today. And if you need proof, look no further than the data around COVID-19.

Black and Hispanic Americans are far more likely to die of COVID-19 than their white counterparts, and the gap only widens when you factor for age. This is because non-white Americans have consistently faced discrimination and unequal access in healthcare, both individually but especially systemically, and this has resulted in a greater burden of disease for many illnesses and conditions that are independent risk factors for a bad outcome from COVID-19 infection.
Compared to whites, Black Americans are twice as likely to be uninsured. They are more likely to die from cancer despite many of those cancers occurring at higher rates in other groups. The rate of infant mortality is 11 for every 1,000 live births, compared to the national average of 5.8 for every 1,000 live births, and Black mothers are 2-3 times more likely to die from pregnancy-related complications than white mothers. Black men have the lowest rates of survival 5-years after receiving a diagnosis of heart failure. Black men and women are less likely to receive cancer screening and preventative health services. And Black Americans are less likely to have a primary care doctor or clinical home and get their care piecemeal in the emergency room setting, and not surprisingly, consistently report higher levels of distrust in doctors and healthcare.
Dr. Gold and others wish to ignore these factors, to make it seem that there is no need for efforts to ensure the vaccine gets to Black communities. After all, if such efforts are not desperately necessary, they must just be inherently racist. It’s a clever enough ploy, but look at all the history that has to be white-washed in order to eliminate the unequal burden of COVID-19 on Black Americans.
Dr. Gold and others say the difference in death rates between races decreases if you adjust for socioeconomic status and poverty. Manipulating the statistics in this way erases 246 years of chattel slavery, 89 years of Jim Crow, and 67 years of unequal wages, discriminatory hiring practices, and unequal higher education access.
Dr. Gold and others say the difference in death rates between races decreases if you adjust for conditions that increase transmission; crowded neighborhoods, multi-family buildings, use of public transportation, and cramped living conditions. Manipulating the statistics in this way erases 247 years of Black American not being allowed to own property, 67 years of over legal housing discrimination, 35 years of redlining, and 53 years of ongoing housing discrimination even after the Fair Housing Act.
Dr. Gold and others say the difference in death rates between races decreases if you adjust for chronic medical conditions. Manipulating the statistics in this way erases the over 400 years of medical exploitation and ongoing healthcare disparities we’ve already discussed.
We could go on. It’s well and good to say that, all things being equal, the COVID-19 virus doesn’t seem to have any race-based predisposition to harm people of color more than whites. But all things are not equal. Our longterm investment in the destruction of Black Americans’ health is now paying compound dividends, as our seemingly impenetrable barriers to access and long neglect of Black healthcare needs places Black communities in a position of heightened vulnerability to devastation by the COVID-19 pandemic, and our sinister history of medical research abuse rightfully increases the wariness many already feel about the new vaccines, our best protection against it. Those who deliberately spread COVID-19 vaccine disinformation are banking on this dynamic increasing acceptance of their false and fantastic claims, and there is something particularly evil about using the lasting wounds of centuries of medical victimization, neglect, and exploitation of Black Americans to further victimize them by damaging their access (medical misinformation is a healthcare access issue) to the best life-saving interventions we currently have available.
My Conversations with Black Patients
So this is the double-edged sword facing our Black friends, neighbors, and loved ones, and my Black patients; on the one side, ongoing disparities that put them at greater risk from the virus, and on the other a history that legitimately causes mistrust in the best tools we have to fight it. Each and every day in my clinic I am talking with Black patients who are aware of Tuskegee, who are aware of Henrietta Lacks, who are aware that these cases are not isolated incidents, and who are seeing all of the same anti-vaccine propaganda and fear-mongering that you and I are on social media.
Many are not at all fooled. They have been navigating this dynamic their entire lives and are used to making these sorts of difficult decisions. They are well aware of the threat COVID-19 poses to themselves and their loved ones. Many of my Black patients at highest risk- healthcare workers, those who are older or have medical complications- have already been vaccinated through our clinic. We are working daily (a physician friend of mine is working literally day and night) to create vaccine access for still more. Often my patients bring it up without me even asking; “Dr. Webb, when do you think the clinic will have the vaccine available?” Others, when I ask, are excited to be scheduled, or added to our call list for when more doses do come in.
For others (and certainly not just among my Black patients), hesitancy about the vaccines is indeed a factor, and I have been intentional about carving out time in the midst of busy clinic days to have these conversations.
For me, the first step in any conversation about vaccine or treatment hesitancy is acknowledgment, and this is particularly true when speaking with my Black patients. Though I was becoming aware of this area of our medical history for a long time, I was hesitant to discuss it openly, fearing it would come off as insincere or virtue signaling; until one day it just burst out.
I was in the COVID-19 outdoor clinic and discussing a patient’s cough and cold symptoms. My patient, an African American woman, was hesitant to get a nasal swab to test for COVID-19 despite having very classic symptoms (though thankfully her test ended up being negative). When asked about her concerns, she said something I had heard from hundreds of patients of every race, age, gender, and background; “I just have a hard time trusting doctors” (I should mention here that the fact I, a doctor, had heard it hundreds of times points to how widespread this problem is; how many thousands of patients felt that exact way but didn’t feel like they could say it to me?). Normally I would respond by saying “I understand” or “I think a lot of people feel that way, let’s talk about it”; measured and time-honored responses that preempt any defensiveness I might feel and allow the conversation to keep moving forward. But that morning I had gone for a run before clinic and listened to Medical Apartheid for about a half hour, and without thinking whether it was wise, instead I burst out with, “Well how could you as a Black woman, when there’s been so much research abuse by the medical field?!” Before I even had time to consider whether I had just stuck my foot directly in my mouth, she grabbed my arm and said “Yes! Exactly!”
Without adopting it as a stratagem, since then I’ve felt much more free to discuss that history with my Black patients (and not just in the context of the COVID-19 vaccines), who of course already know it but might not think I know it- or am willing to admit it- as a white doctor. And I’ve been disappointed, thought not surprised, at how many times my Black patients have told me it’s the first time they’ve heard a doctor even acknowledge Tuskegee, much less all the rest; historical groundwork that has shaped a huge part of their paradigm for interacting with modern medicine, and their doctors, including me, have never even mentioned it or recognized that it exists. When we confess that history we are working to rebuild trust, and we sincerely signal our intent to do the difficult work, individually and as a field, to correct the abuses of the past and present and ensure they never happen again.
Next, I will often share my personal experience of being vaccinated (and that of my wife, a nurse) with my patients. I received my first dose of the Moderna vaccine on Christmas Eve, and my second just last week. As a healthy, 35 year old man with no major risk factors, even my privileged access to the vaccine is understandably controversial, and there is a strong argument to be made for my doses going to someone who needed them more. I wrestled with this for days before getting vaccinated. Ultimately, I decided I needed the vaccine because as a primary care doctor it is vital that I can look my patients in the eye and tell them I would never recommend that you accept a medical intervention, vaccine, or medicine I wouldn’t take myself or advise for my own family.
This is absolutely true, though it isn’t always possible; so far I haven’t needed my appendix removed or required anti-seizure medications or chemotherapy, yet of course I would recommend those for patients who need them. But it is true about the vaccines, and vitally important in the context of our climate of medical disinformation. But with my Black patients in particular there is an additional layer of significance; to the extent that these vaccines are seen as “unproven” (they are not unproven, just commonly understood as such: safety trials involved 10 times the number of participants than normal vaccine safety trials!), it was important for me as a white doctor to show my patients that I am willing to go first on their behalf, when historically it has been Black Americans that have been tricked or forced into going first in order to protect people who look like me. As Harriet Washington says, it is only since Western Physicians and researchers have abandoned the tradition of subjecting themselves to potential harms before they were willing to subject others that research abuse has become so common.
Then I will spend some time, if the patient has specific concerns, answering questions about the COVID-19 vaccines and helping them see through the misinformation around them. The same legitimate misunderstandings and unanswered questions, wild speculations, deliberate lies and mischaracterizations, and outlandish conspiracy theories that I see every day and try to combat on my blog (see my slowly expanding COVID-19 Vaccine Questions & Answers and more importantly the list of resources there) are being sent to my patients, regardless of their skin color or background. We talk about those myths and I try to use this area of semi-expertise to benefit their decision making as well as I can. I often share a two page handout on the most common COVID vaccine myths, that goes into far less excruciating detail than I do on the blog, knowing my patients can ask me for clarification if they want more information. We also talk about the efficacy of the COVID-19 vaccines, the dangers of the virus, and my firm belief that this is our best path forward out of this pandemic.
Finally, I point my patients towards exactly the same types of resources I shared at the beginning of this article; but here is where my relationship with the patient is a key factor. I have been practicing for 5 years now since completing my residency and have many patients, including many Black patients, who trust me as their primary care physician more than they trust any other individual who could speak into their medical decisions or their healthcare fears or anxieties. Though I will still point them towards the incredible resources that come from my Black colleagues, it is to support the work of trust-building that we have already been doing within our patient-doctor relationship for years. Those resources are influential and reassuring, but my word is also valuable to them specifically because they have seen me work diligently on their behalf and engage with them in a partnership to further their healthcare goals and protect their dignity and autonomy.
Other patients I don’t have that kind of relationship with yet. Either we’ve only had a few visits together or I am seeing them in a context outside of their usual clinic; our COVID-19 outdoor clinic or covering for their normal doctor. In those settings we still work to build trust, but I have to be humble and realistic about how much this can be accomplished in 15 minutes (though you’d be surprised). When I and a Black patient I barely know talk about the COVID-19 vaccines, I explicitly state the fact that we are probably both thinking: that I can’t as a white doctor tell them ‘you should get vaccinated’ and expect to be believed by default, or feel entitled to be believed, by virtue of my title or position, my medical education, or my presumed expertise. And though I hope that through our conversation about the history above and just as importantly through sincerely listening to their concerns and working hard to care for their medical needs I will have built some degree of confidence and trust in my recommendations, nevertheless it is in those situations that I have to lean most heavily on the outstanding work that my Black physician and scientist brothers and sisters have already done in dispelling the COVID-19 vaccine myths and empowering fellow Black Americans to make the best and most informed, empowered choices about getting vaccinated. At the end of those conversations, like the beginning of this blog post, my most important role is getting the resources that have already been created by those Black leaders, without any input from me whatsoever, into the hands of people who share with them a history of medical abuse and subjugation but are striving to claim ownership of their health narratives and use every good tool and resource available to defeat this pandemic and end its inequitable impact on Black Americans.
