
A Brief Apology
It’s been a difficult pandemic. And while our COVID-19 cases and the severity of illness we faced as a community was undoubtedly worse over the Winter, the hardest time period for me professionally has been the past 3 or 4 months, as we have dealt with the emotional, psychological, spiritual, and physical fallout of the pandemic’s worst season, trying to help people rebuild while still managing chronic medical problems and, of course, trying to keep everyone safe from the possible threat of another surge.
Healing is hard. Anyone who has done Primary Care Medicine, and especially those who have served a community that faces a great deal of healthcare injustice, knows that those 10 or 15 minutes the doctor gets with the patient in the exam room are not nearly enough to address their mental and physical health needs. The extra time has to come from somewhere, and since there’s another patient already waiting in the next room, for me it tends to come out of evenings, weekends, and early mornings. The number of hours your Family Doctor (or PA, or NP) works on your behalf behind the scenes is hard to calculate. Just check out Dr. Glaucomflecken’s take on Family Medicine:

Or maybe ZDoggMD puts it best when he simply says, “We love our patients, hate the system.”
I last published on medical misinformation back in February. Since that time I have had to choose between writing and carving out some amount of time with my family, and even with such an important topic as COVID-19 and vaccine misinformation, it was a pretty easy choice. So consider this my apology to anyone who has sent me conspiracy theory videos and disinformation memes that I haven’t had time to write about over the past few months; I hope you found the answers you needed.
But when a doctor in your clinic texts you at 7 AM, and it’s a video of a former Chief Resident from your own residency program sharing outrageous disinformation about the COVID-19 vaccines in front of the Texas state senate, it’s probably time to pick up the pen (or keyboard) again and do your part to debunk it.

Dr. Ben Edwards Testifies in front of the Texas Senate Committee on State Affairs
I first saw this video this morning; it’s from earlier in the week and was sent to me by a Physician that actually trained with Dr. Edwards. It’s short, barely over 8 minutes long, and in keeping with my longstanding policy I have shared it below. If it does get taken down by YouTube, which seems unlikely since it was a testimony before a government body and part of the public record, I will make efforts to find another active link to it. Even though it is short there is a lot of misinformation to unpack here, so I’ll be following a time-stamp format below as we dive in.
Contents:
Video
Evidence Based Medicine
Vaccine Safety
Vaccine Immunity vs. Acquired Immunity
0:09 “The Chair calls Dr. Ben Edwards”
For context, this was part of a Texas Senate Committee on State Affairs hearing to consider a proposal by State Senator Bob Hall regarding what measures or policies public and private entities can and cannot implement based on COVID-19 vaccination status. It is part of a broader misinformation campaign trying to portray those who choose not to get the COVID-19 vaccine as experiencing widespread prejudice and portray basic epidemiology measures based on vaccination status as a form of discrimination.
Of course there’s a balance here; while the evidence that the vaccines are very safe is overwhelming, I don’t know any doctor that would be comfortable with people being vaccinated against their will (something that has never been on the table despite the alarmist misinformation to the contrary) or becoming second-class citizens based on a personal health choice. There’s a discussion to be had about which measures are reasonable for government and private entities to take based on vaccination status and which are not; absolutely there is. But as I’ve been saying since the beginning of the pandemic, any such balance has to be struck on the basis of truth; that is, on firm evidence and an honest understanding of how dangerous the COVID-19 virus really is. State Senator Bob Hall, a consistent promoter of myths and misinformation throughout the pandemic, is not a man I would trust to strike such a balance. The balance we need to find is not a middle-ground between truth and lies.
Evidence Based Medicine
0:29 “Ben Edwards, trained as a Family Physician”
Family Medicine is a noble and challenging field of medicine. We take care of patients of all ages, we are trained in obstetrics and pediatrics, we perform many outpatient surgical procedures, and have experience in every field of medicine. Working in underserved care, we help carry some small fragment of our patients’ burdens and fight for healthcare justice on their behalf on a daily basis. It’s a struggle sometimes, but I am incredibly proud to be a Family Medicine Physician.
From what I can tell, Dr. Ben Edwards no longer practices Family Medicine. Or least, he doesn’t just practice Family Medicine. While the point of this post is to address Dr. Edward’s arguments in the video and not his philosophy of medicine, it is important to understand that despite the credentials and training background he shares at the beginning of his testimony, he now practices fringe, non-evidence-based medicine.
Take a look at the price sheet from his clinic’s website. Yes, there are some evidence-based services here; I am very thankful that his clinic is providing cervical cancer screening, and I certainly do cryotherapy for appropriate skin lesions in my own clinic. But they also provide a variety of unproven services like ozone infusions and ultraviolet blood irradiation.
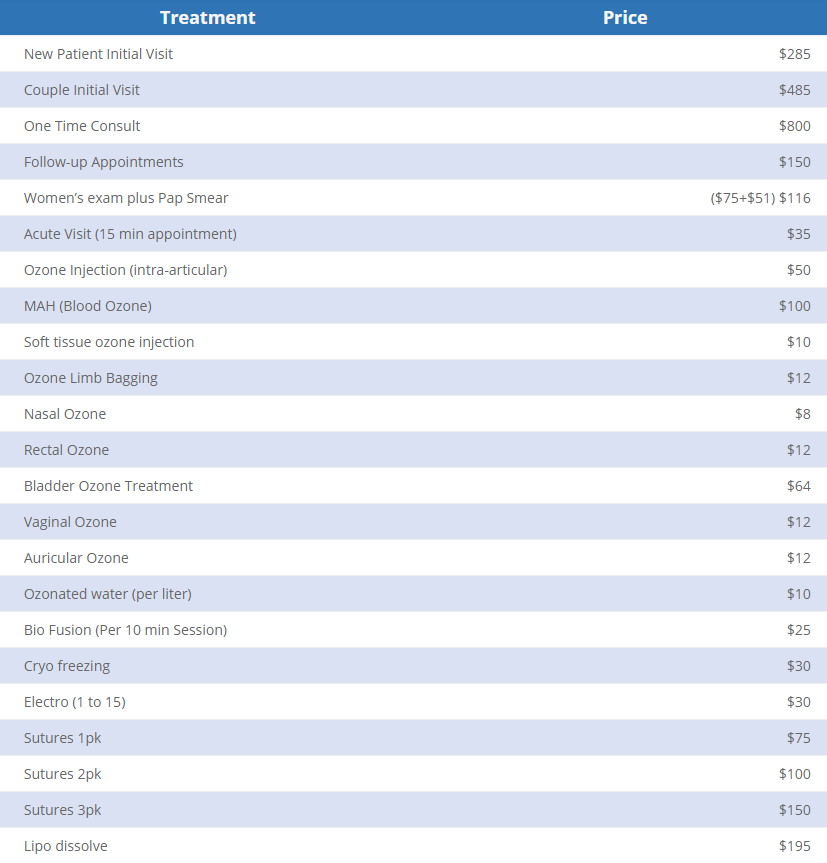
As Dr. Edwards essentially states in the video, he does not believe in limiting his practice to only what is supported by scientific evidence. Maybe you believe in some of these treatments and maybe you don’t. Maybe you are curious about UV blood irradiation therapy or you believe that in vitro studies on the effects of ozone against cancer cells means it will really cure cancer (fire also kills cancer cells in a petri dish, but you wouldn’t inject it into your body). Maybe you are like me and believe this is essentially modern day snake oil. At the very least, I hope we can all give Dr. Edwards the benefit of the doubt and assume that he, at least, believes in his own medicine. Honestly it doesn’t really matter, because the main point is this; when a doctor tells you that he doesn’t believe in scientific evidence, why would you give credence to his testimony about scientific evidence?
0:30 “Did my undergrad at Baylor”
I love Baylor University, despite its flaws. I have great friends that work there, men and women I greatly respect and admire who are working tirelessly to help it become the best university it can be. I’ll even be teaching a class there in the Fall. Still, I never studied there and am only a Baylor Bear by proxy, so this doesn’t hit too close to home.
0:31 “UT Houston Medical School”
Great, fine. I went to UC Denver.
0:33 “And then Waco for Family Practice Residency where I was Chief Resident.”
Uh-Oh.

Now, Dr. Edwards and I trained more than a decade apart and we’ve never actually met; but I know doctors who trained with him, and I feel like a doctor who trained in my clinic, who probably even saw some of the same patients I’ve cared for, sharing false information before the state legislature definitely puts me in a position of “come get your people.”
0:57 “I’d like to begin with a reminder to everyone on the definition of Evidence Based Medicine“
When I first watched this video I did not know about Dr. Edwards’ alternative practices, so I was expecting something pretty standard and uncontroversial here. Most of the doctors I’ve argued with on this blog (I should say “argued against“, not with, since none of them know I exist) have portrayed themselves in the position of sharing scientific evidence, even when such evidence was anecdotal or when their analyses were utterly incorrect. None that I know of have actually come right out and said that evidence doesn’t matter to them, which is why I was so surprised by what came next.
1:09 “The elements of Evidence Based Practice are the integration of best research evidence with clinical expertise and patient values.”
Here’s the full quote if you want it. The landmark article was published in 1996; I’m assuming he found a later quote of the same article, which is where the 2002 in his citation comes from. So far, we are all on the same page.
“Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research.”
-David L. Sackett, OC FRSC, et al. Evidence Based Medicine: What it is and what it isn’t. British Medical Journal, 1996
1:19 “Patient values trump clinical expertise, and clinic expertise trumps scientific evidence.”
Whoa, whoa, whoa. Hold up a second. Is that what Dr. Sackett meant? Is that what “integrating” means in the original quote, that one always trumps the other? Of course not. Yes, patient values always overrule anything else we do in medicine; but that’s the ethics principle of patient autonomy, not the best practice for harmonious, evidence-based patient care, where the physician and the patient work together to find an evidence-based treatment that corresponds to the patient’s goals and values. In order to understand Dr. Edwards’ subsequent comments better, let’s look at what that quote actually means, and how his interpretation of it completely turns it on its head.
Example 1: Insulin for Diabetes. Integrating patient values, evidence, and clinical expertise.
I will use this illustration becomes it’s a conversation I have multiple times a month. Let’s say you have a diabetic patient whose blood sugar is still not well controlled despite taking multiple oral diabetes medications. The best evidence on helping that patient prevent the terrible long-term effects of uncontrolled diabetes says it is time to talk about starting insulin. And for most patients, that’s what ends up happening. But the principle of integrating evidence with clinical expertise and patient values means that decision is a discussion, not something you can arrive at with a flow-chart or a “Idiocracy” style medical computer interface.
That discussion is focused on your patient’s values. How do they feel about insulin? What is their personal or family history with insulin? For many people who have a family history of diabetes, insulin carries an emotional weight; it represents the point where their loved one’s diabetes began to take a more severe toll on them. Of course there’s good reason for that, we give it for more serious cases of diabetes; but I’ve often spoken with patients who genuinely believed that insulin would make you lose your leg or your eyesight based on associations they have had since childhood. Even when we carefully discussed that this was actually due to the uncontrolled blood sugar levels the insulin was prescribed to treat (and my patients typically see that distinction right away once I really explain it), the emotional impact of starting insulin remains. For others, the inconvenience of daily or multiple-times-per-day injections or the barriers involved in administering the medication may represent an insurmountable barrier.
And this is where clinical expertise comes in, to help bridge the gap. The doctor, who has (hopefully) earned the patient’s trust and proven themselves a reliable source of health information and wise counsel, now has to figure out how this evidence relates to this specific patient. The person is a person and people always fit imperfectly into diagrams and algorithms. Maybe the evidence says insulin is indicated at this point, but you also know this patient was recently on a long taper of steroids for resistant poison ivy; steroids that drove up the blood sugar and gave the impression of worsening diabetic control. Maybe your patient has such a negative association with insulin that this discussion itself was the wake-up call they needed to take greater ownership of their health, and you truly believe they are going to be able to get their blood sugar down through dietary changes, exercise, and better adherence to their other medications even without the insulin. Or maybe you are seeing not just the high blood sugar numbers, but also the early signs that the diabetes is taking a toll on their body; the early signs of neuropathy in the feet, the subtly worsening renal function, the minor scrapes and wounds that just aren’t healing like they used to. In that case, integration of evidence, expertise, and patient values may mean helping your patient find a way to be ok with starting insulin, and walking alongside them knowing it’s a really difficult decision for them; or helping them fully grasp the medical realities they are facing so they can make the most informed choice possible, even if it’s not the one you were hoping for. Your medical expertise doesn’t mean practicing against the evidence or ignoring the evidence any more than it means trying to overrule your patient; it means combining your understanding of the evidence with your relationship with the patient to help the patient thrive. It’s why we have doctors in the first place.
Contrast this to Dr. Edwards’ misrepresentation of these concepts.
“Patient values trump clinical expertise, and clinical expertise trumps the scientific evidence.”
Dr. Ben Edwards, Just Now
Example 2: Antibiotics for Viruses. Patient values trump clinical expertise; clinical expertise trumps evidence.
There are a million examples we could use to illustrate the model Dr. Edwards seems to espouse, but this one is prototypical. Let’s say you have a patient come in for upper respiratory symptoms; cough, runny nose, slight fever, etc. (for the sake of argument let’s say it isn’t in the middle of a global respiratory viral pandemic). You have diagnosed the patient with an upper respiratory virus, and they tell you they would like a prescription for antibiotics. Since they have no indication for needing an antibiotic, prescribing one would be a medical error; probably not a dangerous error, but it’s possible; antibiotics are not benign medications. Normally, this would be an opportunity to educate your patient. This is one of the most important roles physicians have; we have the privilege of years of high level medical training that almost none of our patients had access to; it is a true joy to see your patients more empowered and more knowledgeable because of their relationship with you. Under Dr. Sackett’s model, this would be part of integrating patient values and medical evidence.
Or you could take a different approach. If you believe that “patient values trump clinical expertise, and clinical expertise trumps scientific evidence,” you could do some pretty modest mental gymnastics to convince yourself that your patient wanting an antibiotic is part of their “values,” and therefore the right medical decision despite there being no evidence that it will actually help them, and plenty of possibility that it will harm them. By treating preference or assumption as though they were values and autonomy, you have moved from evidence based, patient-centered care to retail medicine; just give the people what they want. A doctor who has fully embraced this philosophy of medicine won’t help you reach a diagnosis, won’t help you get treatment supported by the full weight of thousands of years of learning about the human body that humans have acquired, and won’t help you face harsh realities about your health and learn to cope with them. Such physicians, whoever they may be, have apparently decided that their hard-won medical degrees and board certifications were really just a means to gain the power to prescribe treatments; not to take on the responsibility to use that knowledge and experience in the best interest of their patients.

But the second part of Dr. Edwards’ quote is even more disturbing, if only because it is seemingly so much more common. “Clinical Expertise trumps Scientific Evidence.” In the best light, this mindset seeks to portray the Physician as the Lone Ranger, a maverick that plays by their own rules and uses common sense instead of all that med school learning. They don’t need fancy books and studies to tell them how to care for their patients, they just know. The went to the Med School of Hard Knocks, etc. And the scary part is that we are all really at risk to fall into that mindset and paint ourselves in this light.
But every single time, it’s because we as Physicians have fallen into one of three professional sins; hubris, avarice, or laziness. The former abandons evidence, holding their own clinical experiences higher than the accumulated experiences and careful analysis of their peers around the world, because they think that they alone are capable of intuitively navigating the minefield of confirmation bias and tunnel vision that constantly threatens those who seek to heal. The second abandons evidence because it simply isn’t profitable; a lot of evidence based treatment involves sitting with the patient in the midst of pain and difficulty, helping them find internal resilience and make healthy choices, or prescribing simple, affordable (with the right advocacy) medications that you will never see a dime from (your doctor doesn’t get a cut of your prescription medications!). Instead choosing to push designer, unproven and unregulated treatments can be incredibly lucrative; all doctors know that our medical degrees could be incredibly profitable if we abandoned medical ethics; it’s a temptation we all see coming a mile away, but some still fall into it. The third; well, it’s the easiest of all to understand. I would love to tell myself that my clinical expertise trumps scientific evidence because it’s comforting; it means it’s ok if I can’t keep up. Medicine is hard, and there’s a lot of it; human health and disease is a vast and complex field. If arrogance and greed aren’t my bugbears, this one definitely is; I know I have the tendency, like Dick Van Dyke’s character in Scrubs, to rest on my laurels and lean on my own understanding because I just don’t have the energy. I have to fight that temptation every day.
Saying my clinical expertise trumps the evidence is really just a self-assuring way of me saying that my clinical expertise trumps everyone else’s.
Vaccine Safety
1:29 “I am also concerned that the forced and coerced COVID-19 vaccinations would be a violation of the Nuremberg Code, etc.”
I completely agree, and as a Physician I would never support any forced or coerced medical treatment of any kind; patient autonomy is sacred.
I also don’t know what he’s talking about; I’ve heard exactly zero evidence that anyone is being forced or coerced into being vaccinated against COVID-19. When patients come to see me and we discuss the vaccines, we look at the evidence together and I help them integrate their values with the best available evidence. We don’t shoot needles in their arms as they walk in; we don’t deny them services if they don’t want the vaccine. Right now, I don’t know of any businesses that deny service if you aren’t vaccinated, and I certainly don’t know of any government services vital to health and human thriving that do so either. I’ve heard of some sporting events- huge gatherings that are entirely voluntary to attend and have the potential to become super-spreader events- having separate entrances or seating sections for unvaccinated and vaccinated attendees. Surely we do not consider this to be tantamount to forcing or coercing vaccines? I always want to look at the strongest argument from the other side; if you know of a situation that comes closer to truly forcing COVID-19 vaccinations on people, please send it my way.
2:00 “According to the CDC’s vaccine adverse event reporting system (VAERS), 4,178 deaths are now being reported.“
I think this is the most important point in the entire video, and it’s worth spending some time on. This is a similar claim to one that’s been circulating on social media, and even repeated earlier this month by Tucker Carlson. And the thing is, it’s a fascinating bit of misinformation. Let’s dive into it.
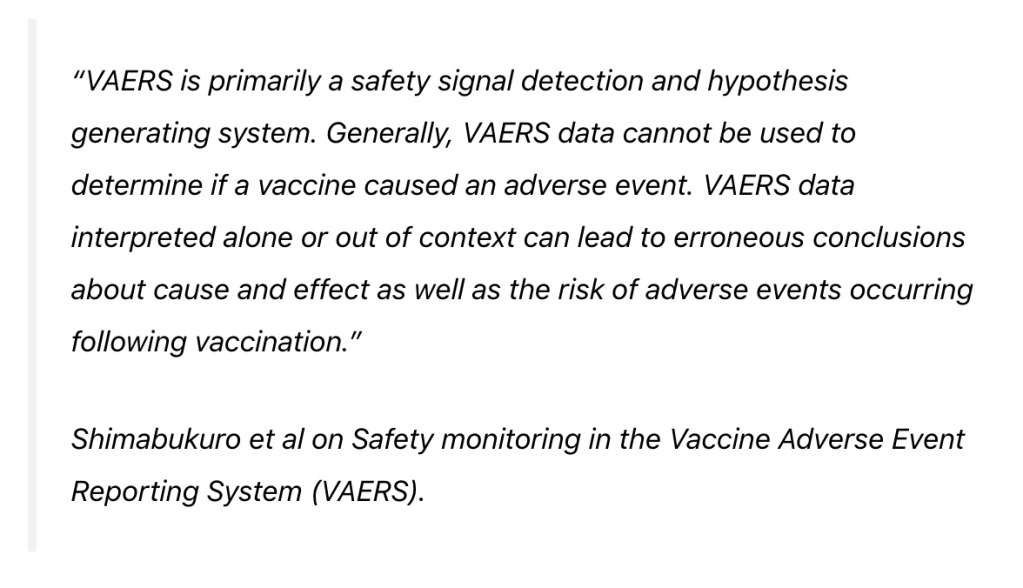
Dr. Edwards shares a number that is incredibly easy to find; the number of deaths reported in VAERS for all people who have received a dose of the COVID-19 vaccine. You can find the numbers for yourself; start by going to https://vaers.hhs.gov/data.html and clicking through until you find an option to search the VAERS data, then select the COVID-19 vaccines and run a report on ‘deaths’. It took me less than 5 minutes to figure out how to run the report, and I’ve never used the system before. Nobody is trying to hide this data. I will note, however, that you have to indicate that you agree that you have read and understood a disclaimer that you can’t use this data the way Dr. Ben Edwards is using it in this video because that’s not what it means at all. At the very least, Dr. Edwards is guilty of breaking the website’s end-user agreement.
Running the report right this second gives me a figure of 3,919 deaths of persons who have received at least one dose of the COVID-19 vaccine; close enough to Dr. Edward’s 4,178 that we won’t split hairs about it. So we agree on the numbers, which are publicly available. The more important question is what the numbers mean.
Remember last year when we repeatedly saw the claim that deaths from COVID-19 were being inflated to make the pandemic look more dangerous, and that all deaths at any point following COVID-19 infection were being called “COVID Deaths,” even if someone got shot or hit by a car or died of cancer. I debunked this one over and over again, but the key to understanding that misinformation hinged on understanding death certificates. Those numbers of COVID-19 deaths were not raw data of ‘everyone who had died’ around the time they had COVID-19; there were based on the detailed reports of physicians, coroners, and other medical experts who had to analyze the cause of death and file a report, with their name attached, in a specialized system that not everyone has access to. If a death is reported as being from COVID-19, it is because a medical expert believed that COVID-19 contributed to or caused the death.
But the VAERS system is the exact opposite. As the disclaimer on the VAERS website says outright, this is raw data without any analysis attached. It can be submitted anonymously and by absolutely anyone. And it absolutely includes people who happened to die from car accidents and gun shot wounds at some point after receiving the COVID-19 vaccines.


And I find this really fascinating because it really seems like after a year of saying the CDC and WHO and your Family doctor down the street were just attributing every death to COVID-19 to inflate the apparent danger, which wasn’t true at all, the medical misinformation spreaders decided that was actually a great idea and decided to do that exact thing with the COVID-19 vaccines! “If you can’t beat ’em, join ’em!”
So now that we understand a little better why the VAERS data can’t be used the way Dr. Edwards is trying to use it, to say that those 4,178 deaths are due to the COVID-19 vaccine, let’s look at what that data does mean.
The first question we have to ask ourselves is, is this more deaths than we would expect in this population even if people didn’t get the vaccine? This is a concept called attributable mortality, and it’s been one of the major proofs of the real danger of the COVID-19 virus against all of the misinformation claims over the past year. We can’t get perfect data from the VAERS system (because, again, that’s not what it’s for), but what we basically need to ask ourselves is whether the death rate in those who received the COVID-19 vaccine is any higher than the rate we would have expected from all causes anyway. Let’s do that math.

To date, 158.4 million Americans have received at least one dose of the COVID-19 vaccine, which became available to the public just over 5 months ago on December 14th, 2020. That’s just below half of the US population. Half the US population with at least one vaccine dose; 4,178 deaths reported on VAERS since we started vaccinating. In that same time period, there have been over 1.4 million deaths in the US. Or to put it another way, in a population of 158.4 million people we would expect about 517,924 deaths in the amount of time since we started vaccinating people. And that’s based on pre-COVID mortality rates.
So among the people who received a dose of the COVID-19 vaccine, VAERS reports far fewer deaths than would be expected in the normal population in that time period. Does that mean that the doctors and nurses are lying about vaccine safety? Does it mean that the CDC is changing the numbers? Does it mean the COVID-19 vaccines are protecting people against more than just COVID? Does it mean they are bestowing some degree of immortality or vitality on people, protecting them from heart disease and diabetes and gunshot wounds?
No. It just means you can’t use the data that way because it doesn’t represent what Dr. Edwards is telling the senate it represents. That’s it.
2:00: “Over the past 20 years, all vaccinations combined there were a reported 4,182 deaths.”
The second question we have to ask is why the deaths reported on VAERS (I won’t say ‘the deaths associated with the COVID-19 vaccine’ the way he does, since we just saw why that is not accurate) in the past 4 months rival the deaths reported from all vaccines in the past 20 years. Surely that, regardless of the small number of deaths compared to the general population, indicates that these vaccines are far more dangerous than ‘traditional’ vaccines we’ve been using for years, right?
No. Again, it entirely depends on what those numbers mean, and the fact that we are reporting adverse events differently for the COVID-19 vaccines than we have for vaccines in the past. This is not clandestine or hidden information; it’s right there on the VAERS website under the reporting instructions. Look at the instructions for medical professionals for reporting adverse events following vaccines, from the VAERS reporting FAQ:

For most vaccines, we report adverse events that have a credible link to the vaccine itself, such as an allergic reaction, and any serious events that occurred within a specific, limited time period following the vaccine. Here’s a preview of the table they mention and link to above:
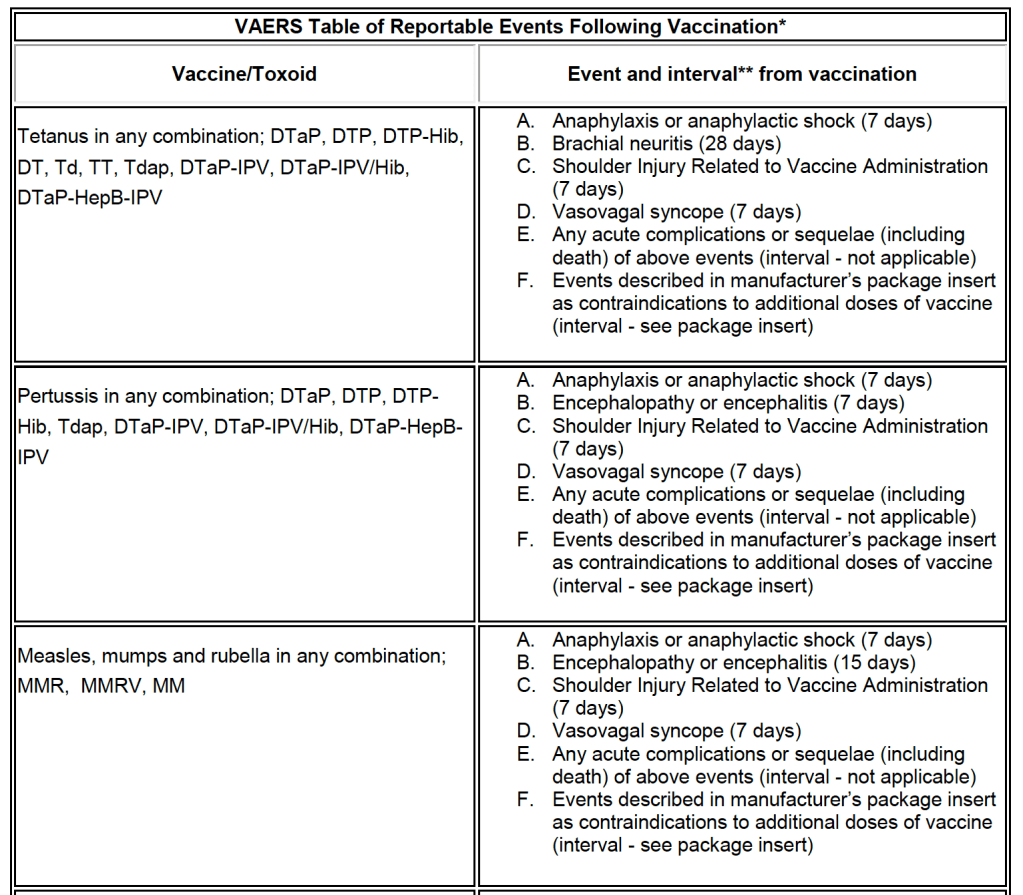
So for the DTaP vaccine, for instance, I would obviously report a severe reaction like anaphylactic shock, if it occurred within 7 days of the vaccine. Anaphylactic shock doesn’t occur a week after a vaccine, and yes this would mean that I would still report it if the patient got a vaccine on Monday and had an anaphylactic reaction to a bee sting on Sunday… But that’s really unlikely, and they have to set a reasonable, liberal time-period. If the patient dies from that anaphylaxis or complications of the reaction, that gets reported too. If the patient is shot, or they develop sepsis from a pneumonia, or their heart failure claims their life, those events don’t get reported because there is no theoretical link between those events and the vaccine; that data is being filtered through clinical reasoning. Which makes sense, because in the past 20 years about 60 million Americans have died; some of those folks happened to receive a vaccine of some sort around the time of their death, but with no plausible causal link there would be no reason to report those deaths on VAERS; it would be entirely unreasonable and misleading to do so.
Now look at the instructions for COVID-19 vaccine adverse event reporting, from the same FAQ:

If a patient dies at some point after receiving the COVID-19 vaccine, healthcare professionals are required to report it. Even if there is no theoretical link; even if there is no possible causal link, such as the reports in VAERS involving traffic accidents and end-stage cancers. If a patient dies and the clinician knows they have been vaccinated against COVID-19, they are required to report it in VAERS, full stop. That’s not the case with other vaccines, so it makes sense that many, many more of the deaths that occur every day as a part of normal human life will be reported on VAERS than ever before. And that’s a good thing; it’s better to have that data than not have that data. But using that data in a way it was never intended, to scare people away from safe and life-saving vaccines, is either ignorant, unethical, or both; you are told before you even pull of the data what it represents, and my hope for Dr. Edwards is that he simply didn’t understand this when he testified in front of the state senate; to knowingly misrepresent this data is simply lying.
The other thing you’ll notice from the above instructions is that, unlike with the TDaP or MMR vaccines, there is no time limit on COVID-19 vaccine adverse event reporting. That means that, while deaths within a week or two of the vaccines are more likely to be reported because the professional treating the patient is more likely to be aware of their recent vaccine, it is still technically required to report deaths on VAERS even 4 or 5 months after vaccination. The same goes for all adverse events. And lest you think it’s far fetched that any of the data on VAERS is coming from that long after people got vaccinated, just remember that if you signed up for V-SAFE to report adverse events to the CDC on your smartphone, you were still getting these texts months later:
So to summarize, those 4,178 deaths that Dr. Edwards mentions are an incredibly small percentage of the people who have actually died in the US in the past 5 months, those deaths reported on VAERS are explicitly stated by the reporting system itself to not represent a causal link with the vaccines, and out of 1.6 million people who have been vaccinated it is a statically insignificant figure. And the rules for reporting adverse events to VAERS are different for the COVID-19 vaccines than for other vaccines, both in the types of events reported and in the length of time since vaccination that a report is required; comparing the “deaths associated with the COVID-19 vaccines” on VAERS to the “deaths from all vaccine over the past 20 years” isn’t just comparing apples to oranges; it’s a total misrepresentation of the data. It’s a scare tactic, plain and simple.
2:29 “This includes a 15 year old boy in Colorado, two 16 year old girls in Wisconsin, a 17 year old girl in Wisconsin, and a 17 year old boy, all healthy, in New Hampshire.”
If these 5 teenagers have died it is absolutely a tragedy. At this point we do not know anything about them; their names, their medical conditions, their history, or what led to their deaths. We don’t have that information because it isn’t in VAERS, and because there are no independent, verified reports of these deaths available. You can search for local news stories or articles about these individuals and so far there don’t seem to be any details of these situations; no information other than that they died at a tragically young age, and that they had receive the COVID-19 vaccine at some point; and all of that only from VAERS itself. Remember that the VAERS reporting system is anonymous, open to anyone, and that none of the reports are verified. In fact, though we know that the COVID-19 vaccines have never been given to children younger than age 2, even in clinical trials, when you run the numbers on VAERS there are well over 200 reports of adverse events to the vaccines in that age group. This is raw, unverified data from the public and it has to be understood as such.
The CDC really does investigate these cases; far from the conspiracy theories about the CDC trying to cover up vaccine injuries, the whole goal of V-Safe and VAERS is to help us make sure the vaccines are safe, and a lot of resources are devoted to following-up on these reports. When there are reports of deaths in teenagers who have received the COVID-19 vaccine, that deserves attention and an assumption of authenticity; but there is no reason to believe that the COVID-19 vaccine they received contributed to the death; VAERS can’t tell us that. What we actually have is basically, “someone went online and reported a death in a teenager who had been vaccinated against COVID-19. We need to look into this.” By transforming this into “the COVID-19 vaccine killed this teenager,” Dr. Edwards is not advocating for the teenager and their family. He is not bringing light to their situation. He is simply using the report of that death in VAERS to create fear, with no understanding of the circumstances around that death and no knowledge of the people affected by that tragedy. We cannot use other people’s tragedies, which we know nothing about, to promote our own political agendas.
2:42 “The evidence is pretty clear that VAERS grossly underestimates the adverse events that are reported... Only 1% of adverse events are ever reported to VAERS.”
This is absolutely true, but before you let Dr. Edwards guide you into inaccurate assumptions, you need to realize the subtle switch he’s just made.
Up until now Dr. Edwards has been talking about deaths reported in VAERS. He’s given numbers, he’s given tragic examples. He’s been trying to convince you that the number of deaths “from” the COVID-19 vaccines has been astronomical. Without any clarification or verbal signal, he has now switched from deaths to adverse events. All adverse events, including mild reactions. So when he tells you that ‘4,178 people have died from the COVID-19 vaccines’ (which isn’t true), and then immediately tells that “less than 1% of adverse events are reported to VAERS,” he wants you to do some quick head math and say to yourself, “Wait, that means that over 400,000 people have died from the vaccines!” If that number sounds crazy to you, it’s because it is. We passed 400,000 deaths from COVID-19 in January of this year (we are now pushing 600,000). It took 11 months from the first American COVID-19 death in February 2020 to get to that point, and at various times in the pandemic our hospital systems were utterly overwhelmed. If we were now seeing 400,000 deaths from the COVID-19 vaccines in 5 months, you wouldn’t have to watch Dr. Ben Edward’s testimony on Facebook or YouTube to hear about it; you would be seeing it in your hometown, you’d be hearing about it from your friends and family who were affected by it personally. Your local hospitals would be on divert and over-capacity like they were because of COVID-19 back in December. No, the COVID-19 vaccines are not causing massive numbers of deaths. In fact, they are very, very safe.
So where does that 1% statistic come from? Well let me ask you; when you had a sore arm from the Flu shot last year, or your child spiked a mild fever due to their MMR shot and you had to give them tylenol, did you report it on VAERS? No; I didn’t either. We could have, it would have been totally reasonable to do so; but since those were expected, mild, self-limited reactions to the vaccines it never occurred to us to report them. The more serious reactions are reported at much higher rates, which is exactly the way VAERS is designed. There’s a great discussion of this phenomenon on Vaxopedia, and since they’ve done the literature review already I’m going to steal some of the studies they cite.

Serious reactions, and especially deaths that clinicians believe might be linked to a vaccine, are going to be reported at high rates, while mild, expected reactions will be reported far less than 1% of the time. Dr. Edwards uses “deaths” and “adverse events” almost as synonyms in this section by not clarifying what that 1% statistic really means. At the end of the day, the Vaccine Adverse Event Reporting System is doing exactly what it is supposed to do; providing huge amounts of raw data that we can search for unexpected patterns and then form hypothesis. Unfortunately, any time raw data is publicly available, there is the risk that people, including physician scientists who trained in Waco, will latch onto the data and use it to weave false narratives, stoking unfounded fear and panic.
3:44 “Personally I have received numerous reports from family members of my patients, close friends of my patients, that within hours to days of receiving the vaccine they have suffered from stroke, heart attack, pulmonary embolism, blood clots, and death.”
I also see patients every day, and many of my patients have received their COVID-19 vaccines. I couldn’t give you an estimate of how many. My patients are typically excited to show me their vaccine card and we celebrate together that they now have better protection against the virus. I always ask if they had any side effects, and I often hear about body aches, chills, nausea, fevers, malaise, and fatigue; “All the things you told me to expect, Dr. Webb.” I also talk to plenty of patients who had a sore arm, or no side effects at all. I have had no patients tell me about a dangerous side effect or death they believed was related to the COVID-19 vaccine.
How do we reconcile this? One of two ways. Either one of us, me or Dr. Edwards, is lying; or at least exaggerating. Or else, we are receiving the types of narratives from our patients that they expect we will resonate with and appreciate. My patients know I am a vaccine advocate and I want to see them protected against COVID-19. Some of them know I write about COVID-19 misinformation. Many decided to get vaccinated after we talked about the vaccines and I answered their questions. It’s entirely possible that my patients are more apt to tell me about their minor symptoms. But isn’t the opposite at least as true for Dr. Edwards? My population of patients are from all walks of life, all backgrounds; his are self selected; they have specifically chosen his clinic because they are strong believers in homeopathic and alternative medicine and want those services. Their doctor is against vaccines and they likely know it just as much as my patients know I am for them. Wouldn’t his patients be apt, even anxious to share vaccine horror stories they had heard with him? And of course, referencing these stories later while trying to make a point, how much verbal precision can we expected someone to exercise in distinguishing between “my patients have told me they’ve heard stories about serious adverse events from the vaccines” and “my patients’ friends and family members have experienced serious adverse events from the vaccines.” It’s the most important distinction in the world; it’s also exactly the kind of distinction most of us wouldn’t scruple to make if we really believed our point was valid and wanted to emphasize it as strongly as possible. Adverse events, like jokes, are best when told in the 1st person.
Vaccine Immunity vs. Acquired Immunity
4:19 “Studies have shown a 2-3 fold increase risk of adverse reactions to this vaccine if you’ve already had COVID.”
I am not familiar with the studies he is referencing here, but I don’t doubt this for a moment. We already expected this because of the more robust set of side effects we’ve seen with the second shot in the Moderna and Pfizer vaccine series; in fact, I’ve been counseling my patients to expect more robust side effects if they’ve already had COVID-19 for months. It certainly matches my experience; I had COVID-19 in December and got the vaccine a few weeks later; I had body aches, chills, and nausea after both doses, not just the 2nd, and I’m sure it was because I had already had COVID-19.
Remember, he is not saying there is a 2-3 fold increase in injury or death from the COVID-19 vaccines if you’ve already had the virus; just in adverse reactions. Most of the adverse reactions we experience are related to our body’s immune response to the vaccines; they are part and parcel of that robust immunity we are hoping for. We get fevers after vaccines because of Interleukin-1, which the macrophages that pick up the viral proteins release to stimulate B and T cells. We get body aches and headaches because of the Interleukin-6 those cells produce to turn the B cells into antibody producing plasma cells. We feel tired because… Well, nobody really knows; but all of that immune response does take up a lot of energy. Yes, you are more likely to have adverse events after the COVID-19 vaccine if you’ve already had COVID-19, because your immune response is more robust; those “adverse events” are the symptoms of your immune system working.
4:26 “Natural immunity confers a more robust immunity than vaccine immunity could.”
Dr. Edwards repeats this idea multiple times in the next minute, and there was a time I would have agreed with him; intuitively it seems like that would always be the case. But it isn’t true. This is an area where I was skeptical at first, but the data has forced me to change my mind; the COVID-19 vaccines really do create a stronger immune response than our own natural response to COVID-19 once we’ve recovered from it. My friend and medical misinformation hero Dr. Emily Smith has written bout this before, and she’s better at explaining things than I am:
So Dr. Edwards is simply incorrect on this point. But it’s not a competition between your body’s response to COVID-19 and your body’s response to the vaccine, because his assertion that it is dangerous or unwise to vaccinate someone who has already survived COVID-19 is inaccurate; it’s actually the best immunity you can get, if you were unfortunate enough to already get sick from COVID-19 like I was.

5:03 “God gave us an amazing, robust immune system, and I don’t think you can improve on God.”
Absolutely! I complete agree. I was writing about how awesome our immune system is, and how we ought to treat it, back at the beginning of the pandemic. I’m a big, big fan of my immune system.
You know who else was a fan of the immune system? The folks who invented vaccines. Vaccination came to the United States from, among other sources, an enslaved African man in Boston whose knowledge of the African traditional medicine practice of inoculation helped save hundreds, maybe thousands from Smallpox in the 1720’s. We don’t know his true name, but his slave name was Onesimus, and it’s only in recent years that his insight and knowledge is bringing him the credit that was previously received only by the man he shared these with, the Boston doctor who owned him.

Onesimus, like the traditional healers before him and the vaccine pioneers since, understood that the immune system is an incredibly powerful defense against disease, but that it works best when it knows what it is fighting. By giving the immune system a template- previously by injecting a small amount of live pathogen into the body through inoculation, but now by presenting it with just a few key proteins (that cannot cause disease) through vaccination- we unlock the immune system’s full, robust, God-given disease-fighting potential. Vaccines are not an improvement on God’s design; that’s just anti-vax propaganda. They are the best way we have to arm the immune system with the information it needs without having to actually get sick in the process.
Imagine you want to assassinate someone (for the sake of argument), and you hire the world’s best assassin. You pay her exorbitant asking price, all up front and in unmarked bills, and receive her guarantee that the job will be done. Finally, you try to tell her the name of the target, maybe even hand her a picture and dossier; she plugs her ears and won’t look at the picture. “I’m the world’s greatest assassin,” she says, “I don’t need to know who the target is.”
That’s what it sounds like, saying we shouldn’t try to “improve on God’s design” of the immune system with vaccines.

God bless you, and thank you.
LikeLiked by 1 person
Thanks for taking the time to write this stuff! Weirdly enough there was another graduate of our program that was publicizing similar incorrect content but he didn’t have quite as big of a platform (just his Facebook followers). What class are you teaching?
LikeLike
It’s demoralizing that there is more than one Waco Family Medicine residency graduate who is spreading misinformation online. On the bright side, there are also several doing myth-busting work and of course many who are sharing excellent, reliable information. Dr. Ben Brashear is a graduate of our program and has been fighting misinformation online since early in the pandemic: https://www.facebook.com/BrashearFamilyMedical
LikeLike