I had intended to write this weekend on a variety of topics, including herd immunity, the recent RECOVERY trial using low-dose dexamethasone in critically ill COVID-19 patients, antibody testing, and the question of whether the increase in cases is really just due to increased testing (answer: unfortunately, no). But when I woke up this morning the world seemed suddenly, vehemently, and inexplicably divided on just one subject: wearing masks.
Part of this can be accounted for, at least locally; yesterday the City of Waco issued an order requiring businesses to create and post mask policies for employees and customers. As with anything that has been unnecessarily politicized and sensationalized, I recommend you read for yourself what the order actually does and does not require. This morning I had half a dozen messages asking for my thoughts on whether or not masks are an effective strategy, and several people shared pieces of misinformation they wanted to bring to my attention.
So while I would still like to write about all of the above issues, I think this one will have to take priority today.
Are masks safe and effective?
G.K. Chesterton said that he was most convinced by evidence that is ‘miscellaneous and even scrappy.’
“A man may well be less convinced of a philosophy from four books, than from one book, one battle, one landscape, and one old friend. The very fact that the things are of different kinds increases the importance of the fact that they all point to one conclusion.”
G.K. Chesterton, Orthodoxy
So while we will look at scientific studies, journal articles, and other medical evidence, I want to include data from various kinds of research, including both laboratory conditions and real-world epidemiology, and from both prior to and during the COVID-19 pandemic. I also want us to apply some common sense and a good bit of our own past experiences. This can be dangerous in a field like medicine, where realities are often counter-intuitive, but if undertaken cautiously this common sense approach can serve as an anchor for the more academic information.
With that in mind, I think we can start by thinking about the advice we give to children when they are sick or have seasonal allergies (if your children are like mine, these efforts are ultimately futile, but struggling against that futility is a time honored parenting tradition). We tell children to place their hands over their mouths when they sneeze or cough. If we are particularly savvy (and can get past the occult theme; looking at you anti-Harry Potter friends), we teach them the Vampire Sneeze/Cough, where we cough into the antecubital fossa (the bend of the elbow) instead of our hands.
Why? Because respiratory viruses are spread through respiratory droplets; mucous and saliva from the respiratory track that contains the virus. In this article we will look at the filtering ability of various types of masks and whether they are actually able to catch the microscopic particles that cause illness, but you don’t need a microscope to measure the number of microns between a toddler’s fingers when she almost but not quite entirely fails to cover her mouth for a cough; it’s a lot.
Now it’s true that these etiquette maneuvers do not actually stop or absorb all of the particles; they catch some and merely redirect others into the surrounding environment. But you knew that. If you live with a sick child, the odds of yourself or another family member getting sick is high regardless of how good they are at vampire coughing. The goal isn’t to stop 100% of the droplets, but to modify the spatial distribution; to make it less likely that you will get sick from someone coughing or sneezing a few feet away or across the room. Even in science some things are intuitive; if you can feel the spray of respiratory droplets on your face when someone coughs near you, you know your chances of getting sick are higher.

This is the same principal we are talking about when it comes to masks. Nobody is saying that if someone has COVID-19 they can just wear a mask, N95 or otherwise, and cough and sneeze without getting anyone sick; studies have show that the particles still escape. But if someone coughs across the room from you, their mask or their elbow, or even better both, interrupts the momentum of the droplets (50 mph for a cough, 100 for a sneeze according to a study in the Journal of Fluid Mechanics) and decreases the chances of the droplets reaching you, giving you time to move away or at least cover your own face, blocking a few more particles. These are components of an overall risk mitigation strategy that involves things like social and physical distancing, frequent hand washing, sitting outside instead of inside, contact tracing of COVID-19 patients, and staying home if you are sick.

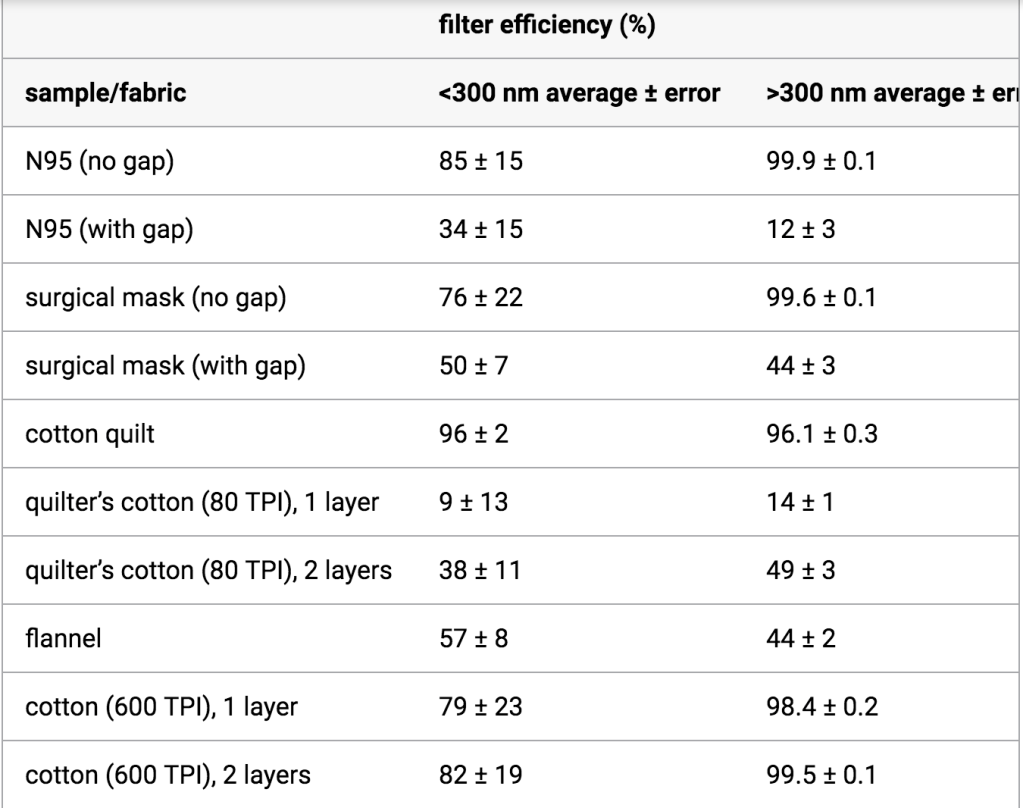
It’s also important to note that the studies that have shown only very modest benefits of masks, such as the study that produced the graph above, have focused on the spread of droplets through coughing and sneezing; high pressure, high velocity events that force droplets through and around barriers such as masks and sleeves. However, the City of Waco is not asking 100,000 people to wear a mask in case one of those people happens to cough in HEB. We now know that both asymptomatic and presymptomatic COVID-19 transmission do indeed occur, and the mechanism of transmission still seems to be from saliva and respiratory mucous, including respiratory droplets and aerosols, even in the absence of coughing and sneezing. Talking, forcefully exhaling, singing, yawning, spit talking; all of these are lower pressure events where a mask may actually block, rather than redirect, a higher percentage of these small, lower velocity particles. Again, you already believe this intuitively, because you cover your mouth when your breath stinks.
I also think that revisiting our actual real life experience and common sense is particularly important when dealing with medical misinformation, which is often found to be self-contradictory and manifestly illogical within only a few moments consideration and comparison to facts we already know. It rarely takes being a physician or another scientist to figure out that these wild claims on social media aren’t accurate, though I’m sure it helps.
Unmasking Mask Misinformation (sorry)

A friend sent this to me this morning; it was posted on a public forum (“public forum” sounds so much more legitimate than “Facebook comments”) as a response to our city’s new masking policy. I’ve also been sent a longer paragraph format piece that starts “I am OSHA 10&30 certified.” Since they overlap quite a bit, I won’t re-post that one in its entirety, but it’s just full of contradictions (‘surgical masks only filter on the exhale’ yet ‘become useless’ for protecting you if your breath clogs them), false claims (‘N95 masks can’t filter COVID-19’, ‘asymptomatic spread doesn’t occur’), and nonsensical statements (if you wear a mask and get exposed to COVID-19 you become a walking virus dispenser, cloth masks are worse than no barrier at all). It does make one really excellent point though; if you are relying on wearing a mask to fully protect you from getting or spreading COVID-19, that is indeed a false sense of security. We can’t say that often enough; but it just doesn’t follow that masks are worthless or make the problem worse, which is what they repeatedly claim. I’d like to go through the claims above in order, before concluding with some final arguments for masking.
Claims #1 and #2: Masks decrease oxygen intake and increase carbon dioxide retention.
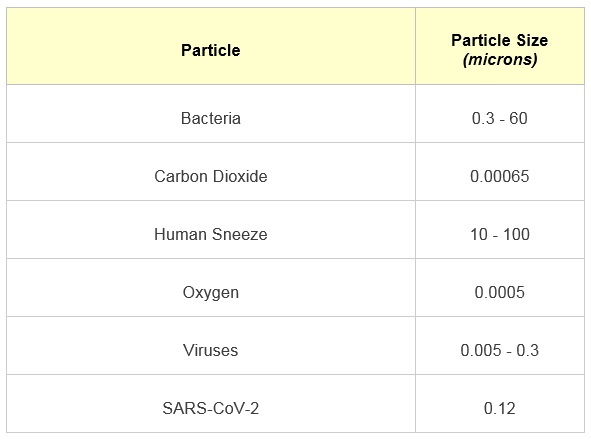
This is something that has been studied extensively, and there is no evidence that simple surgical or cloth face masks will cause hypoxia or any significant decline in oxygen levels. Oxygen molecules are very small and diffuse easily both around and through these types of masks; they are nowhere near the size of viruses, or the much larger respiratory droplets that carry most of the virus that is exhaled. The same is true about Carbon Dioxide, which is only slightly larger.
But you can also consult your own experience here. Many types of people already wear masks for many hours of the day, from surgeons to certain industrial workers, and women in many cultures wear face coverings as a part of their public clothing. Yet we do not consider these persons to be at high risk for either hypoxic (low oxygen) or hypercapnic (high CO2) injury. A big part of the problem is that we have sensationalized the wearing of masks during COVID-19 and have started to treat it like it isn’t a normal part of our experience already, which it absolutely is. Whether it is the above examples, or Halloween or Comic-Con, or my 5 year old spending three weeks straight in his Spider-Man costume and refusing to wear anything else, the wearing of masks is something we all have some degree of experience with and have never really been concerned about until now, when we are suddenly being told they are extremely dangerous, generally by the same people who have been spreading various types of COVID-19 misinformation since mid-March.
But more to the point, you can study this on your own. A battery powered pulse oximeter is very accurate and costs about $12, and you can use one to do a simple experiment that will reassure you, at the very least, that your face mask is not causing your oxygen levels to drop. Check your oxygen level with your mask off, and then wear it for however long you expect to need it when you are out running errands or whatever scenario you are worried about. Then check it again. In general in a healthy adult, readings above 95% are normal and below 90% are concerning. As an example, I’ve been wearing my properly fitting N95 for the last half-hour and my O2 saturation has fallen exactly one percentage point.

There is one group of people we should mention here, and that’s people with chronic lung disease such as COPD or Asthma. For people with these conditions, the increased heat and moisture of the air within the mask, and the decreased air flow directly to the nose and mouth, really can create both real and perceived difficulty breathing (and in these conditions, these trigger each other so easily that drawing a distinction between the physiologic respiratory distress and the anxiety-provoked sensation of respiratory distress is almost a false dichotomy; not being able to breath is scary). These are also conditions that predict a higher likelihood of severe illness in COVID-19, which complicates matters. For these individuals who should already be taking every precaution possible for their own safety in the midst of this pandemic, the decision of whether and what kind of mask they should wear when they do have to go out should be a discussion between them and their doctor. For the rest of us, especially those of us who personally care about someone with Asthma or COPD, it’s important that we take every precaution we can; it should go without saying that our “what about someone with a chronic respiratory illness” should only ever be a legitimate question on their behalf, not a rhetorical ‘gotcha’ to turn off our intellectual honesty on this issue and dismiss the benefits of everyone else wearing a mask.
Claims #3 and #4: Masks shut down the immune system and reactive your own viruses.
The third claim, that masks shut down your immune system, is just a reiteration of the above two, and there is absolutely no evidence for it. As we’ve already said, doctors, nurses, and other medical professionals, and especially those involved in surgery, wear masks all the time without any fear of their immune systems being shut down or weakened. And while these types of people are often fearless when confronting deadly situations or illnesses in order to care for their patients, as we have seen throughout this pandemic, they tend to otherwise be fairly health conscious. I still remember being shocked during a group discussion in medical school when we were asked what it was we valued most highly. I was trying to honestly wrestle with whether I valued my faith, my wife, or my daughter most, and how it was even possible to separate those things from one another, when my friend answered “my health,” and several others nodded in agreement. I have no judgement for that person, but the whole idea was very alien to me (and maybe that shows something of my privilege in having lived overall a very healthy life, often despite my personal choices). Maybe this friend would risk the thing he valued highest on behalf of a patient (in fact I think he would); but if there was any evidence that his health was imperiled by wearing a mask, he would be leading the charge against masking (just checked facebook; he isn’t), and probably would have been doing so since medical school.
The fourth claim is one that I first came across in the Plandemic “documentary” last month, and based on the wording it seems to be taken directly from there (or they are both taken from a 3rd, unknown source, which I’ll call “Q”)(I’m now being told that “Q” is already taken). The actual claim is that wearing a mask will activate dormant retroviruses that live in your body. Retroviruses are a family of viruses that replicate by inserting viral DNA into host cells and hijacking cellular machinery, and only a few known species causes disease in humans, including HIV and Human T-Lymphotropic Virus, which can cause certain cancers. This claim is very specific and very conspiracy-theory oriented, but I suspect that this distinction between retroviruses and common viral illnesses like cold and flu is not being made by the people spreading this meme.
The long and short of it is that this just isn’t the way the immune system works. You don’t have a host of dormant viruses sitting in your lungs that, if breathed into a cloth or small space and then breathed in again, will suddenly become active and cause an infection. Do you get sick when you sit in a car? What about when you hold your breath? What if you sleep with your face too close to a pillow? Is there evidence that we see more respiratory infections in people that wear masks regularly? Of course not. In someone who has a functioning immune system, once your immune system has seen and defeated a virus, you cannot give that virus to you; you already have an effective immune response to it. There are a small number of exceptions, like getting shingles through varicella zoster reactivation, but coronaviruses aren’t one of them and there is no evidence that wearing a mask or breathing out and then breathing in the ‘same air’ has anything to do with viral reactivation; there isn’t even a physiologic mechanism that would make this possible.
Claim #5: The virus is too small to be trapped by the masks!
This is where both the misinformation and the answer get a bit more technical, and if you want all of the scientific details, the blog First10em has an amazing article on masking, viral transmission, the 6 feet apart rule (which they call the “2 meter” rule, whatever that means), and the transmission patterns and particle sizes of both droplets and aerosols. The question of whether various types of face masks besides N95’s actually do filter the COVID-19 virus itself is still an unanswered question, but the answer seems to be, to some degree, yes. Studies have shown different types of masks to have varying filtering efficacy even down to to very, very small particles in the range of 300 nanometers or less, in fact right in the range of the virus itself (the SARS-CoV-2 virus is roughly 120 nanometers; an earlier version of this article incorrectly reported the size of the measured particles in this study as 40 times smaller than the virus, which was just due to me getting my conversions wrong. Sorry; pay attention in 8th grade algebra, kids), but other studies have shown that the virus is still able to transmit through (or around) masks, at least to a few inches away and if propelled by a cough. Taken together these studies seem to reiterate what we have been saying all along; masks aren’t perfect, but they do decrease the risk, especially in short-term contact with non-cough, non-sneeze related transmissions like we would see in asymptomatic and presymptomatic cases. Indeed, this is confirmed by a Hong Kong study in 2011 that found that the protection offered against respiratory pathogens by all types of face masks decreased with higher velocities and prolonged exposure.
Regarding this piece of misinformation though, we can summarize the two main errors pretty succinctly; the virus isn’t floating through the air by itself, it’s suspended in respiratory droplets and aerosols; and the masks aren’t supposed to block 100% of the particles on the microscopic level (though that would great), just trap most of them and slow the others down. The mosquito through a chain link fence analogy is silly because mosquitos can fly around barriers volitionally, and because it uses the size of the virus instead of the size of the respiratory particles, which are much larger (1-100 microns, mostly, instead of 0.12 microns). But if you want to use the analogy, it’s more like hitting golf balls through a chain link fence; yes, the gaps are bigger than the golfballs, and some will go through if they are hit really hard; but many will be blocked outright and many others will be slowed down and redirected.

Claim #6: There is no evidence to support masks.
We have already looked at some of the various types of evidence that I believe we all find somewhat convincing. We believe as a culture that masks are least helpful in preventing infections in some situations, such as surgery, and believe they are safe when we wear them for cultural or religious reasons, as part of our jobs, or as part of costumes. We engage in barrier maneuvers (some better than others) to block large respiratory droplets when we cough and sneeze. We know the masks redirect and lessen such droplets even in these high-velocity conditions, and we’ve seen the evidence from physics and fluid dynamics studies that they can filter the smaller aerosols under low-velocity conditions. For me, the last remaining piece of the puzzle is, “does it actually work, really?”
I want to look at two more types of evidence; epidemiology evidence from before the COVID-19 pandemic, and emerging epidemiological data from right now. An Australian study in 2009, well before the COVID-19 Pandemic (but you knew that), found that the wearing of face masks did diminish the transmission of upper respiratory illnesses even among household contacts, but that there were fairly low rates of compliance with masking. If masks were worn more, they could help significantly.
“Adherence to mask use was associated with a significantly reduced risk of ILI-associated (Influenza Like Illness) infection. We concluded that household use of masks is associated with low adherence and is ineffective in controlling seasonal ILI. If adherence were greater, mask use might reduce transmission during a severe influenza pandemic.”
This study and others like it, 10 years prior to the COVID-19 pandemic, should at least put to rest any ideas that wearing masks is a novel recommendation or a government ploy to control yet another aspect of our lives. Masks have been recommended, and shown to work, for preventing respiratory virus transmission for decades; any suspicion of them now likely comes more from the current hyper-politicized, conspiracy saturated climate than from anything else. But the COVID-19 virus is new and acts very differently from other respiratory viruses in so many ways, so what’s to say that masks will be effective for COVID-19?
It is too early in this pandemic to have robust and definite conclusions about which measures helped most and which showed modest or negligible benefits. We know that social distancing helps from evidence in places like Sweden and Norway, and we now seem to be living the results of relaxing our own social distancing measures without other robust mitigation strategies in place. When it comes to masks, we could compare the United States, which is (apparently) very resistant to masks becoming a social norm to places like South Korea where wearing a mask has been the norm since early in the pandemic; but this comparison is complicated by vastly different healthcare systems and populations and by a strong difference in adherence to other mitigation efforts as well, which we Americans have also been consistently defiant of.

I do agree in principal with the approach by one writer to the CDC’s journal, Emerging Infectious Diseases, in comparing Taiwan to Singapore; but again this is not a perfect comparison by any means.

- Update: It has been pointed out to me that there are now several recently published studies, conducted during the COVID-19 pandemic itself, that have looked at the issue of mask wearing to determine if the benefit is significant. You can find two of them here and here (with thanks to Baylor Epidemiologist Dr. Emily Smith, PhD, who has written an excellent summary of the current evidence for masks). I’m sure many more studies are ongoing. Of course none of these are going to be able to perfectly measure the effectiveness of masking under real life pandemic conditions; if you can imagine a scientific experiment that could, it would probably be unethical and immoral (and logistically impossible), such as taking members of a population and randomizing them to wearing or not wearing masks and then measuring how many become sick from each group. Those types of study designs are entirely off the table, so we analyze epidemiological data; looking at what happened in countries, regions, and cities where masks were adopted early, and what happened in other places after they were adopted later on. It isn’t possible to know how well the mask policies were followed from such data, or to perfectly tease out confounding factors like social distancing measures, the success of contact tracing, and the robustness of testing programs; it wouldn’t be possible to say masks are the most important thing if they are always or nearly always used in conjunction with other mitigation strategies, which is exactly how they should be used. But these studies do conclude that implementing mask policies (and following them!) makes a significant difference in the trajectory of this pandemic, and taken as just one important kind of the multiple kinds of evidence we have looked at, I do think they contribute to a convincing case for wearing masks.
Ultimately, once this turns the corner, we will never be able to say with certainty what the real answer was; whether it was wearing masks that helped the most or the heightened caution in other areas when cases began to climb, whether reopening resulted in a surge here in Texas or if it was our bucking of social distancing all along, whether each of our mitigation measures individually made a difference or not. What we can say for certain is that the American method so far has not been working. By denying the disease’s existence and danger, producing conspiracy theory after conspiracy theory, claiming we beat it prematurely, and fighting tooth and nail against every reasonable recommendation and rule meant to protect ourselves and our neighbors, we have taken a global pandemic and made it largely into an American pandemic, with the highest number of cases and deaths in the world.
There is plenty of evidence that masks are safe, and that they stand a fair chance of helping, especially against asymptomatic and presymptomatic spread. If you are sick, get tested, stay home, and isolate; make sure you get the medical care you need. If you are well and can physically distance yourself from others, then distance yourself from others while finding ways to still care for your community and your own mental and physical health. If you cannot distance because of strong religious or moral convictions or the realities of your job, or due to strong personal preferences, then please wear a mask and wash your hands frequently.
This is just one of the ways we can do better during the rest of this pandemic; myself included.
