Trigger warning for human trafficking, rape and sexual assault, sexual abuse of children, and exploitation.
The big question we didn’t address yesterday (well, two days ago now) is whether the people making these comparisons between COVID-19 and cancer or diabetes are doing so because they truly care about those medical problems, like the nurses and doctors who treat them and the patients and their family members who are affected by them every day do, or just because they happen to find them convenient comparisons for minimizing or dismissing concerns about the pandemic. And while using a lifelong illness that causes real suffering like stroke or cancer for rhetorical purposes is a bit calloused, I can’t say I find it truly morally repugnant the way I do when the same thing is done, if indeed it has been done, with human trafficking and modern day slavery. Recently, I have started seeing a few different memes/images shared on social media making just such a comparison; but I believe they have very different degrees of merit and, I’m afraid, might be coming from very different places in terms of degree of actual sincere concern about the very real problem of modern day slavery.
Human trafficking is a truly evil industry. Some of the people who have shared these memes have quoted conservative estimates of 25 million slaves worldwide today; I believe the ILO estimates that are closer to 40.3 million, though even that was back in 2016 and the number is likely to be even higher now. This includes 5 million people, 99% of whom are women and girls, who are victims of sex trafficking and forced sexual exploitation. In addition to being robbed of their freedom and dignity, the men and women affected by modern day slavery suffer extensive medical and psychological problems that can last a lifetime, and many are subjected to nearly constant physical, sexual, and psychological violence, torture, and dehumanization. It is one of the worst offenses against human beings occurring today, and its cost in human lives and suffering is incalculable. In one sense, there can be no comparison between human trafficking and COVID-19, because even the suffering from a respiratory virus that claims your life would be preferable to most of us compared to what is endured by victims of modern day slavery.

I first heard about modern day slavery from my friend Michelle Palmer, co-founder of the blog Tuesday Justice, back in 2008, my first year of medical school. That next year we became involved in grassroots organizations in Denver involved in raising awareness about human trafficking and modern slavery both in the United States and internationally. In medical school I hosted film screenings, attended academic conferences on human trafficking and training with the FBI and GEMS on commercial sexual exploitation of children (CSEC), and once even sat next to the author of The Vagina Monologues on a committee focused on professional collaboration to fight human trafficking in the city and state. When we moved to Waco I got involved with Unbound and eventually became one of their medical professional trainers. Over the last few years myself and one of my clinic partners have trained hundreds of physicians, nurses, other healthcare professionals, and Texas medical students to use their calling in medicine to recognize the signs of human trafficking and help address the unique medical and support needs of survivors, in addition to treating survivors of human trafficking and modern day slavery in our own clinic.
Last week, that partner and I both spent a significant number of hours in full PPE, in the 90-100 degree heat, evaluating, testing, and counseling patients for COVID-19. In 2 weeks, I’m going to lead a group of family medicine residents in a discussion of human trafficking cases; I will be working in the COVID-19 clinic that morning and that afternoon. I recognize that all of this sounds dangerously akin to self promotion, but the reality is that given my privileged position as a doctor and the scope of the problem, I feel that I’ve personally done very little towards combating either COVID-19 over the past 7 months or human trafficking over the past decade. That’s not my point. My point is that there is not a competition of awareness, focus, advocacy, or effort between the fights against these two assaults on our fellow Image-Bearers of God. The people who are fighting human trafficking are often the very same people fighting COVID-19.
And I humbly submit that memes which suggest otherwise may, in fact, be made by people who care about neither.
The Bad

I wanted to start with this one because I believe it’s somewhere in the middle in terms of both dismissiveness about COVID-19 and creating a false opposition between COVID-19 and Human Trafficking advocacy. The meme makes two claims; first a statistics claim about the relative risk of human trafficking and COVID-19, and the second a claim about the increased danger to children posed by masks because it perpetuates trafficking. Let’s look at both.
Though the numbers don’t usually matter much in posts like this one, I always like to know where they come from if possible. I went to the original source, an Instagram user who, apparently, works to promote “vaccine education, toxin free living, and government corruption.” I love it when people have eclectic interests.
Unfortunately, she doesn’t list where her numbers come from or how she ended up with this ratio of 66,667 children sold to human traffickers for every one child that dies of COVID-19, and I’m going to admit that it seems a bit high even to me, someone who leans towards more liberal estimates of human trafficking. The biggest problem with her numbers is that nobody actually knows how many children and adults are bought, sold, and enslaved through human trafficking each year; it’s an illegal, hidden, underground industry and the best we can do is estimate. It’s also very easy to misunderstand what the numbers actually mean; for instance, when experts say that an estimated 200,000-300,000 minors in the US are victimized through commercial sex trafficking each year, this is based on a much smaller number of actual reports, data from homeless youth and runaways, the personal narratives of adult sex workers who entered the life as children or adolescents, internet ads through websites like craigslist and backpage, and a variety of other data sources. Unfortunately, the vast majority of children who are being exploited in this way are not known. If we used this estimate (300,000) of US CSEC victims, divided by her 66,667, it would give us just 5 children in the US to die of COVID-19; since this is nowhere close, this clearly cannot be the figure she is referring to.
The experts I trust estimate that there are about 10 million child victims of human trafficking in the world today ( this number does not include the tens of millions of child brides across the globe, nor young or old adults who have been enslaved ever since they were children), and I think this must be the number of she is thinking of; nothing else even gets us close. Working backwards, this would give us an estimate of 150 children (10 million/66,667) who have died from COVID-19 worldwide. This is probably closer to the number of children in the US that have died from the virus; the best estimates that I can put together would put that number at around 100 (it’s tricky since the best data sources I can find don’t distinguish specific ages within the 15-24 yo age group; I don’t know how many from that age group were older adolescents and how many were actually young adults). We could look at this data from every possible angle (I typed a whole other paragraph on hypothetical calculations and assumptions we could make here, but deleted it; it doesn’t add to the discussion), but ultimately we are going to come out with an estimate that is certainly more than 150 but somewhere less than 1,000 child and adolescents deaths from COVID-19 infection worldwide.
So the best guess we can make is that the original author of this meme is comparing the total number of child slaves worldwide to some estimate she has found of the total number of child COVID-19 deaths that is, at least, on the right order of magnitude. There are at least five big problems with this “calculation” of a child being 66,667 times more likely to be sold to traffickers than to die of COVID-19.
First, the 10 million figure is an estimate of current child slaves, not new child trafficking victims; the idea of ‘being sold by traffickers’ paints the situations of enslaved people around the world as a monolith and ignores the debt bondage enslaving millions of families (which is still strongly associated with physical, psychological, and sexual abuse), which is by far the most common scenario for a child slave today. It also glosses over the many forms of control and exploitation included in human trafficking that don’t involve ‘being sold to a trafficker’, which we’ll talk more about in the next section. Sensationalist language hearkening back to ‘Taken’ is not at all helpful in understanding the scope of human trafficking and modern slavery.
Second, it’s very much an apples to oranges comparison since the 10 million estimate is a cumulative total built up over many years, and the number of children dying from COVID-19 is a total from just a few months of a pandemic; it is a comparison of prevalence to incidence, two very different epidemiological concepts. The total number of children trapped in slavery and the total number of children sold into slavery since February are clearly not synonymous, but the author of this meme has treated them as the same thing; this renders her figure, 66,667 to 1, utterly meaningless, since she isn’t even comparing the things she claims she is, let alone statistics that have a logical basis for comparison.
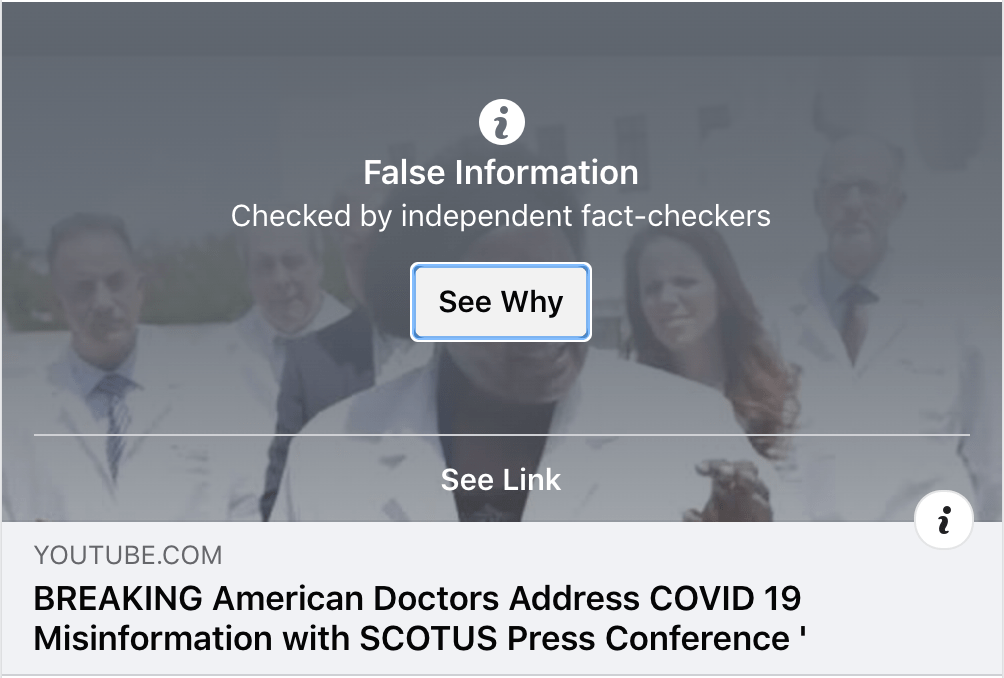
Third, this really is a straw-man. The discussion of whether or not to re-open schools is important, and the conversations I have every day with parents concerned about the risk of their children being harmed by COVID-19 are addressing very real anxiety. We talked about this with last week’s America’s Frontline Doctors video and will be trying to address it more fully in the coming week. But epidemiologists and physicians have at no point argued that COVID-19 was now the greatest threat to children worldwide; in fact we’ve come home from each and every shift incredibly thankful that this isn’t like the Spanish Flu pandemic of 1918, when children were disproportionately affected and killed by the virus. If it were, I’d probably be living in a tent behind our fence instead just changing on the patio and dodging my children on the way to a shower as soon as I come home. Nobody is saying that children dying from COVID-19 is the heart of the pandemic, and memes like this that want to put the number of child COVID-19 deaths ‘in perspective’ are ignoring the fact that child deaths have not been the main motivator for any of our mitigation efforts.
Fourth, and most importantly, the comparison doesn’t matter. Saying that one thing is terrible and dangerous and needs to be fought against doesn’t mean other problems aren’t important. Anyone can do this trick with any two terrible problems. You can say that human trafficking isn’t important because a child is 15 times more likely to be a victim of child abuse within the their own home, or that childhood cancer doesn’t matter because children are 6 times more likely to die from accidents. Just because two things are deadly doesn’t necessitate a comparison of their badness; we can be against both. The cynical side of me says that the only reason to use human trafficking, unless you are really trying to raise awareness about it, is because advocacy for victims of human trafficking confers an immediate moral high ground, and for some reason that is something that COVID-19 deniers feel they must have. They find human trafficking convenient because it paints them as compassionate and ethical and those fighting or concerned about COVID-19 as though they were ignoring this huge human trafficking problem. We wouldn’t expect them to set-up COVID-19 against something more morally benign that harms children, for instance swimming pools or hurricanes. I’d like you to stop and think about that for a moment; think about the fact that some people have decided that their personal crusade against COVID-19 justifies using human trafficking to score rhetorical points; that they have chosen to exploit the plight of human trafficking victims, some of the most exploited people in the history of the world, for their own ends.
Fifth, though it’s not as direct a correlation as with heart disease and immunocompromising conditions like cancer, there is a potential synergy between human trafficking and COVID-19, and it has nothing to do with masks. COVID-19 has, mercifully, killed relatively very few children, but it has left some children without one or both parents, and many more without one or more grandparents; adults who, when they are safe people themselves, confer the safety, security, and support networks that are protective against human trafficking. Despite our fears as parents (I am writing this sitting across from my 8 year old who is working on her math homework) (check that; supposed to be working on her math homework), most children who are victimized through human trafficking are not ‘taken’ from their front yards or from a big crowded event; they are preyed upon by traffickers who look for social vulnerabilities; want of support, care, and love; and circumstances where children and adolescents can be controlled. The logical conclusion of any of the memes or videos or posts that call us to lessen our focus on COVID-19 prevention, regardless of motive, is more deaths from COVID-19 among adults and elders- that is, parents and grandparents- and thus more children at risk for human trafficking in the years to come.
I also said that we would talk about the claim that having children wear masks makes them easier targets for human traffickers. Besides having, as far as I know, no verification for this claim, it also relies on sensationalized concepts of human trafficking and ‘oh that makes sense’ thinking; you are supposed to envision a child being walked along the street by human traffickers with family or friends passing within a few feet and not recognizing them because they are wearing a mask. This ignores the reality of trafficking victims’ experiences and the real methods of control used by traffickers; a problem it shares, though far less gratuitously, with the memes we will look at next.
The Ugly
As bad as it is to essentially make up statistics, and as bad as it is to artificially pit against each other two things that harm children as though you had to choose between them, and as though being vocally against one meant you were in support of or deaf to the other (“You are against a fake virus, while I am against human trafficking”), there is an even more exploitative type of meme going around the internet that takes these same goals and cranks the appeal to visceral emotion up to 11. After careful consideration I have decided not to share these images on my blog; I am sharing heavily redacted versions below, trusting you will recognize the type of macro I am talking about here.

For those of you who have been mercifully spared from seeing the originals of these macros, or the many others circulating right now, they typically show one of three types of images in paired with text minimizing COVID-19 or juxtaposing it to human trafficking; a young child with tears in their eyes and a large hand over their mouth, a terrified child with a shadowy figure standing behind them, or a small girl bound with ropes, often in a basement or darkened room. For those who have seen and shared these images, I want to ask you to do something; go delete them (or change privacy settings; you can choose whether or not to delete them in a few paragraphs) before we move forward.
These images are deeply troubling and problematic for so many reasons that its actually hard to know where to start. “Minor” issues first, as we build towards the very worst and most troubling aspects of these images.
Bad statistics/misinformation:
Trying to get people to accept false numbers or misleading statistics by appealing to emotion rather than logic is a common propaganda tactic and we don’t need it in the fight against human trafficking. The problem is big enough on its own without hyperinflating the scope of it. We talked about the ‘66,667x more likely’ above, but the other number we commonly see is 800,000; 800,000 children are reported missing each year, and the implication is that they become victims of human trafficking. The reality is that most children being trafficked in sex slavery are not reported missing because they are being trafficked by family members or are in vulnerable situations where they would not be considered ‘missing’. Most child sex trafficking victims have not been kidnapped. Moreover, that 800,000 represents mostly missing children who were found very quickly; this is the number from a 2002 study for all children who were reported missing, and includes children who have runaway or gotten lost and family abductions during custody disputes; only 115 of these were what we think of as ‘kidnapping’. Missing children, family and non-family abductions, and all forms of child abuse are serious and important issues, and they all intersect with human trafficking and CSEC to some degree; but using statistics from one problem interchangeably with that of another, or using the most dramatic possible number you can find without careful explanation or honest reflection is not helpful.
Implying silence/neglect of human trafficking issues:
Comment accompanying the second image above reads “time to change the conversation.” This can be taken one of two ways; either ‘it’s time to start talking about human trafficking’, or ‘it’s time to stop talking about COVID-19′. I suggest the real goal of this meme is the latter, because unless you’ve been living under a rock for the past 10 years, we have been talking about human trafficking. To quote a friend who has a degree in modern slavery studies and has worked in this field, even if there are often problems with the organizations that only work to raise awareness of human trafficking without offering other support services or or contributing to the work in other more tangible ways, “they have at least done a good job at that.” Whenever I give lectures on human trafficking and modern day slavery, I always begin the same way; by asking for a show of hands of how many people have heard of this problem before and feel they know something about it. There has been a substantial difference in the response to that question over the past decade. One of the great things about volunteering in this field is that it is one of the few issues where people from all walks of life and ends of the political spectrum find a lot of common ground; we all agree that human trafficking is wrong. Some of us believe that pornography is a major contributing factor (more on that later), while others don’t. Some believe that legalizing prostitution is an important step in fighting it, while others don’t. Some believe that essentially all efforts to confront human trafficking should be secular while others believe that the Church has an important role to play. But despite these differences, there is more common ground to be had here than in the fight against almost any other societal ill. And that has made for fertile ground for grassroots awareness work; telling someone about human trafficking isn’t likely to start a debate or argument. 12 years ago we made shirts that said “slavery still exists” and “27 million slaves: ask me more.” Today the awareness focus has shifted to trying to help people understand modern slavery better and, often, combatting the sensationalist and misleading stereotypes that still persist. COVID-19 has not diminished the conversation around human trafficking, and images like these set it back rather than advancing it.
There is one extremely important point that needs to be made in this section, and I think here is the place to make it. Maybe you are new to human trafficking advocacy; maybe a meme like this is the first you’ve heard of it, and you naturally felt compelled to share. And if that’s the case I want to say two things. First, is that when we are talking about why these memes are problematic and my belief that some of them were made with bad intent, I by no means mean that I believe the people who have shared them have bad motives in doing so; I know for a fact that hasn’t been the case with the people who I’ve seen share the images above. I remember the sense of urgency I felt the first time I heard about children being used as soldiers by the LRA in Uganda; I rushed to my dorm and turned off the Halo game my roommates were playing to try to force them to watch the documentary (it didn’t go well) because I couldn’t believe no one was talking about this. If you are just learning about human trafficking and modern day slavery now, it probably feels the same, and the idea that some awareness efforts aren’t helpful because the images they show or the numbers they quote aren’t quite right must seem a bit strange or overly particular. My goal here is to help you understand why they are problematic, as someone who has been where you are but has since been learning about this for years, and to help you find better resources for raising awareness, like the ones I am sharing in this blog post. And the second thing I want to say is welcome, we are glad you are here; the fight against human trafficking needs you. And the first thing we need from you is to learn more, which is work that none of us can ever actually move on from. I recommend you start with Tuesday Justice’s Primer on Modern Slavery, and then read Kevin Bale’s Disposable People.
Racist overtones:
One of the recurrent visual themes we’ve seen throughout these social media images is the presence of both a child victim and an adult abuser, and the contrast between them. The child is small, the adult large. The child is terrified, the adult commanding and ominous. And often, the child is light skinned, the adult dark skinned. I don’t have exhaustive knowledge of the human trafficking memes that have been shared recently and can’t tell you what percentage of the time this is the dynamic presented. I also can’t tell you if this is done with lighting effects or if the photographer actually recruited white children and POC men for these photoshoots, or which of those options would make it worse; frankly the idea that children were asked to pose for these photos in the first place is troubling enough. But I don’t think these choices are accidental. The history of characterizing black men as hypersexual beasts and violent rapists in order to play into white majority fears of their children and young women being abused stretches back hundreds of years to the very beginning of our nation, and it has been a common theme in lynchings throughout American history. Malcolm Foley, Baylor University Special Advisor to the President for Equity and Campus Engagement and expert on the Church’s response to lynching in America, and my pastor, spoke about this briefly in his interview with Christianity Today following the death of Ahmaud Arbery. He in turn recommends you read Southern Horrors by Ida B. Wells, which addresses this topic in great detail.
“There is hardly a town in the South which has not an instance of the kind which is well known, and hence the assertion is reiterated that ‘nobody in the South believes the old thread bare lie that negro men rape white women.’ Hence there is a growing demand among Afro-Americans that the guilt or innocence of parties accused of rape be fully established. They know the men of the section of the country who refuse this are not so desirous of punishing rapists as they pretend. The utterances of the leading white men show that with them it is not the crime but the class. Bishop Fitzgerald has become an apologist for lynchers of the rapists of white women only. Governor Tillman, of South Carolina, in the month of June, standing under the tree in Barnwell, S.C., on which eight Afro-Americans were hung last year, declared that he would lead a mob to lynch a negro who raped a white woman. So say the pulpits, officials and newspapers of the South. But when the victim is a colored woman it is different.”
Ida B. Wells, Southern Horrors
If playing into sensationalism and parental fears has little to no place in the fight against human trafficking, there is even less justification for drawing on deeply rooted generational racism. By portraying abusers as men of color and victims as predominantly white children, these images are trying to recruit some of the ugliest and most harmful racist ideas buried in the heart of our society in order to fight human trafficking; but the fight against human trafficking doesn’t want or need those racist stereotypes. Moreover, these images are portraying a scenario that is not representative at all of the reality of race within human trafficking, a crime that disproportionately affects children of color, and reinforces stereotypes that themselves go hand-in-hand with racially motivated sexual abuse of trafficking victims. I hope you’ll read the article I’ve just linked from Love 146; it’s very short and shares the stories of three survivors whose race was a selling point their traffickers used to advertise them for sexual exploitation; please take a minute and read their words.
Misrepresenting human trafficking victims:
These images are also damaging and potentially dangerous because they so deeply misrepresent the real situations of victims of human trafficking. Though chains, ropes, cages and locked doors have been used to hold child and adult victims of human trafficking, they are not the most common methods. The techniques that traffickers use to control their victims are varied and sophisticated. Traffickers use shame, fear, and physical closeness in perverse combinations to make victims feel that they are the only person in the world that can be relied on or trusted. Many times they are family members or parents of the child being exploited, and use that relationship to maintain control. Other times they move victims to another city and strip them of their phones, ID’s, and social support networks to make the world outside the trafficker’s control feel even more dangerous and foreign. They use drug addiction, financial entrapment, and poor living conditions to create absolute dependence on the trafficker as a provider. They use psychological torture and manipulation to instill in their victims a sense that they are omniscient and omnipotent; they know everyone, they have contacts with the police, there is nowhere that the trafficking victim can run where they won’t find them. They use threats of violence credible and not; if you leave, I’ll kill your family, I’ll recruit your sister into the life in your place. They forge trauma bonds that make recidivism incredibly high and prosecution against traffickers extremely difficult. These methods, and many we haven’t touched on at all, make chains, ropes, cages, and locked doors unnecessary for controlling victims.
So why does it matter if these images paint a misleading picture of how victims of human trafficking are controlled and exploited? First, because it makes it more difficult for people to notice and report human trafficking when it occurs, something these memes claim to want to promote, if they are only ever looking for physical signs of restraint and enslavement. The work of grassroots advocacy and awareness organizations involves dispelling these myths so that people can really begin to understand the complex, nuanced, and insidious forms of control that are used, and learn to spot them in their interactions with victims of trafficking. When we train medical personnel to detect trafficking, we talk about the presence of a controller, sexualized language and patient narratives that normalize sexual abuse and violence, asking judgement free questions, and understanding the adverse medical findings associated with trafficking; looking for a cage or a rope is going to miss most cases of human trafficking, and all of the cases that could be detected in a medical setting. And second, because the misconception of trafficking control methods being limited to only physical forms of restraint like the ones in these images contributes to shame and victim blaming towards survivors. When we promote the idea that all trafficking victims and modern slaves are bound by ropes or chains, we are also stating the contrapositive; if you aren’t bound by ropes or chains, you aren’t really a trafficking victim. Adolescents are arrested for “prostitution,” a crime that can’t logically exist (children cannot consent to sex; “child prostitution” is always rape), and are frequently further victimized by law enforcement. They are rejected by families and loved ones because their serial victimization and the control methods they have suffered are seen as evidence of poor moral character. Society asks incredulously, “why didn’t you just leave?”, and we tell ourselves narratives that “I would have run away if it had happened to me,” without ever trying to understand what they had to endure. It even contributes to trafficking victims’ difficulty in recognizing their own abuse, because they may believe the cultural narratives that the incomprehensible torment they have endured as serial victims of rape and psychological torture don’t count unless they were handcuffed, caged, or tied-up at all times.
Sensationalizing the sexual abuse of children:
This is the hardest one to write about, and also the reason this post is now over 24 hours late. In my opinion it’s the biggest problem with the images above. Recently the Texas Medical Board began requiring that all licensed physicians complete training in human trafficking, and the Department of State Health Services (DSHS) released standards that those trainings should adhere to. Though the training we conduct had only one major revision because of this, we used it as an opportunity to update the entire presentation and ensure it was something that protected the dignity of human trafficking victims and survivors to the highest degree possible. The one revision; removing an image of two teenage girls standing on a street corner at night. And the reason we removed that image was because of this new training standard:

I’m including this training standard because I want you to understand that my objection to these memes and my request that you take them down if you’ve shared them, and kindly call them out when you see others sharing them, isn’t based on personal distaste or a negative visceral reaction (which is exactly the type of reaction they are meant to provoke). These are agreed upon standards and the idea of these images being harmful is accepted among those who fight against human trafficking every day; it’s just hard to articulate exactly why. We call these types of images sensationalized because we can’t quite call them sexualized; there is nothing sexual about a child experiencing fear and torment. Yet the image is meant to arouse disgust because we know that, to traffickers and johns and others who sexually assault children and adolescents, these are sexual images; in fact, I think you could rightly call them pornography. These images of children with adult hands covering their mouths, or bound and terrified with dark figures standing behind them, clearly send the message, “This child is about to be sexually assaulted.” I don’t know of anything that has less place in the fight against human trafficking than images that, if seen by one of the millions of men and women who have survived sexual assault or the ordeals of abuse through modern day slavery, would potentially traumatize them further and bring to mind those violations. These images are exploitive; they take the worst, most hopeless and fear-filled moments of the lives of real people and reproduce them for use as promotional materials. The fact that what the creators hope to promote is awareness is a mitigating factor, certainly; if these images were used for literally any other purpose we would chase the people creating these memes out of town, society, and history; we would call the FBI on them and put them on social media blast. But the ends do not justify the means, and we do not need simulated pornographic images depicting the moments before a rape or the psychological suffering of a child to convince people that this is an important issue. We need survivors’ stories. We need to understand the factors that contributed to their targeting, their control, and eventually to their empowerment and escape. We need to help young men and adult men understand that “non-consensual sex” is always rape and that desire for sexual interaction with the helpless and those who cannot consent is a serious mental health condition that needs immediate treatment, not a fetish or kink that can be safely indulged in as long as the victims are far enough away. We need to understand the complex networks of organized and non-organized elements that make up the human trafficking industry. We need to fight human trafficking by uniting across political and religious lines against the exploitation of children and the sexualization of innocence, not by dabbling in it as these memes do.
The Good

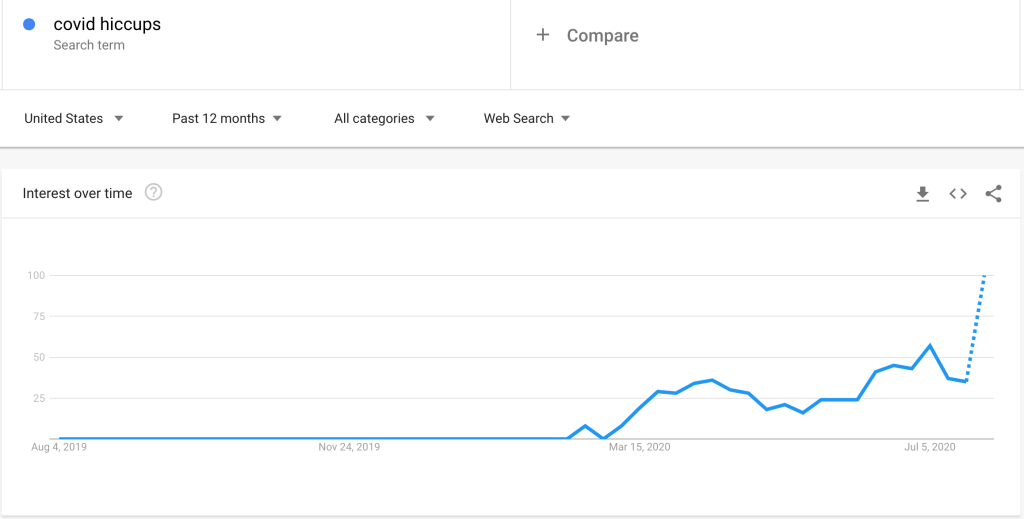
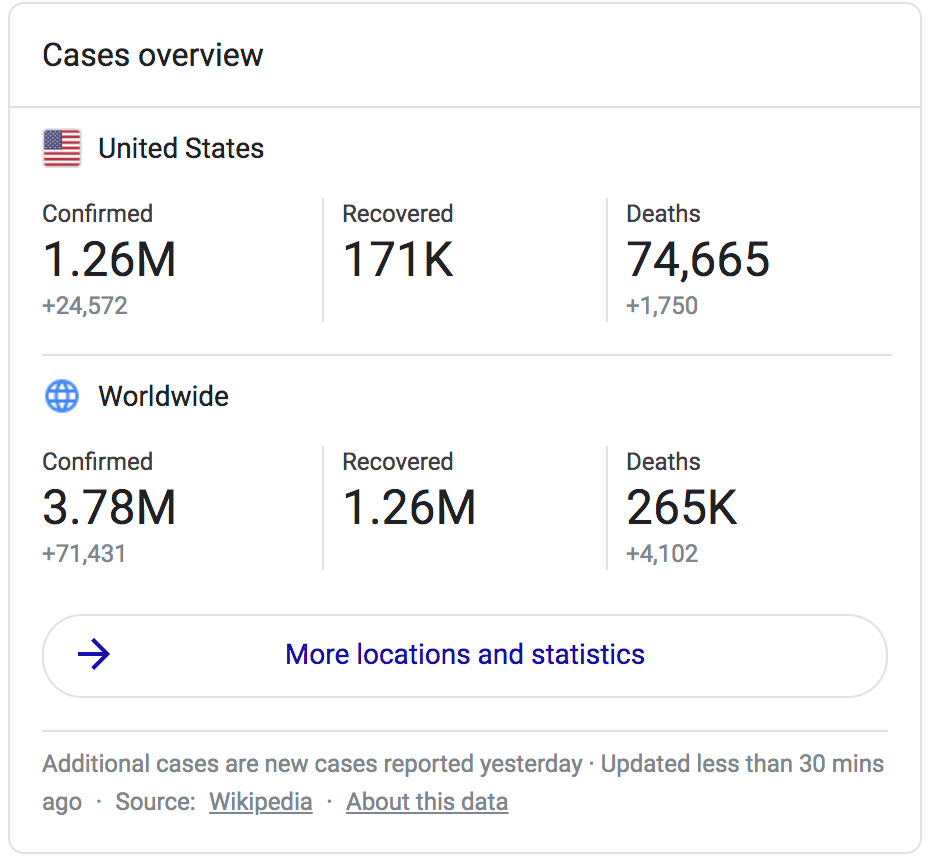
I think it’s important to note that not all memes that compare and contrast human trafficking to COVID-19 are necessarily problematic. The meme above is clearly different, while though it is using COVID-19 to grab your attention it is not trying to diminish the seriousness or reality of the pandemic. Further, it links to the Polaris Project, a reliable source of human trafficking information and resources, which also operates the National Human Trafficking Hotline, a free resource that anyone can call if they themselves need help or support or to report or ask advice about a potential human trafficking situation. Some of the verbiage, like “I wonder if … people would start paying attention?”, isn’t what I would choose and maybe falls under the idea of treating human trafficking like a neglected topic, which we talked about earlier… But this is very minor and may just be an issue of generational differences in meme tone and vocabulary.
This meme also shares data instead of sensationalized images and false statistics, and doesn’t try to play on fears, racist stereotypes, or false narratives about human trafficking. Finally, it comes from a source that is beyond question focused on helping women rather than minimizing COVID-19 concerns; the Montgomery County Women’s Center in Conroe, Texas, which provides sexual assault support services including legal support, crisis intervention, counseling, and advocacy. A quick search of their social media shows that they have indeed taken COVID-19 seriously and have modified their delivery of services and planned programming to keep their staff and clients safe from the virus; once again showing that any dichotomy between caring about COVID-19 and caring about victims of sexual violence is a false one.
How COVID-19 is like Human Trafficking and Modern Day Slavery
I know that by this point the title of this post, “Please keep comparing COVID-19 to Human Trafficking,” must feel like sarcasm or a particularly flimsy misdirect; but I promise you I really mean it. For me personally there are lots of similarities, not the least of which are the real harm and destruction I have seen them both bring to the lives of human beings created in the image of God, and the work I have accepted of helping provide accurate information to replace the misunderstandings about them that lead to deep seated fears. But there are a few other ways I think the comparison between these two pandemics is actually apt, if made responsibly:
There is lots of misinformation out there.
I would hope this post is proof enough that there is misinformation on both human trafficking and COVID-19 circulating widely. I said before that the role of grassroots awareness efforts on human trafficking has shifted from telling people that slavery still exists to helping people understand what modern day slavery is really like. This is invaluable work that is done best when informed and led by survivors or human trafficking, helping those of us in support sectors and the public in general understand the nuanced and complex nature of their experiences. Just like we try to do on this blog with COVID-19 videos and other medical misinformation, organizations like Unbound, Polaris Project, and Free the Slaves carefully break down the myths, popular stereotypes, and outright lies surrounding human trafficking and then tell the real stories of survivors and victims and the real story of human trafficking and modern day slavery. This aids in awareness, victim recognition, survivor support, laws that support survivors, and a culture that treats human trafficking victims as survivors instead of criminals. Without accurate, reliable data, this work is surrounded by a fog of biases and assumptions that inhibits the work of aiding survivors; we need to tell honest stories about human trafficking because when we share trafficking misinformation, it helps the traffickers instead.
You can make both problems worse without realizing it.
We’ve talked before about the danger of asymptomatic transmission of COVID-19, and studies which have shown (though the results are open to some interpretation) that the 48 hours prior to the onset of symptoms might actually be the most contagious period of time during an infection. As someone who has done pretty good but not perfect at social distancing throughout the pandemic, I find this especially concerning; all of us need to fight the false sense of security that comes with feeling healthy at the moment, thinking about our potential exposures and at-risk contacts even when we don’t think we are sick. That’s different from living in fear; living with a healthy respect for what this virus can do to us or our loved ones is wise, not fearful. But in addition to spreading this virus directly, we can make the pandemic worse with our other actions; sharing misinformation on the internet, failing to vet our sources when we share new or emerging information, supporting policies or politicians that minimize the very real danger of the virus, and fighting against non-nefarious common-well-being policies like wearing masks in public spaces. All of this increases the risks from the virus in much more subtle ways by creating a culture that minimizes personal responsibility and obfuscates the reasonable mitigation measures we can all take.
And almost the exact set of actions have a corollary in unwittingly supporting human trafficking. You probably contributed to human trafficking (as I did) today when you purchased products that had slave labor upstream in their supply chain. Some companies are better about monitoring their supply chain for slave labor than others, and there are groups that keep independent report cards for everything from the fashion industry to your local grocery store. But while buying blue jeans, chocolate, or a new smartphone may support labor trafficking and slavery in the supply chain throughout the world, there is one auxiliary consumer industry that supports sex trafficking specifically; pornography. These two industries are indelibly linked. A culture of widespread pornography use and addiction contributes to dehumanization of and violence towards women, and fetishizes demeaning sexual interactions, sexual violence, and rape, and it feeds the demand for sex trafficking from the consumer side. But the connection runs even deeper than that, because if you have consumed pornography you have not only supported the sex trafficking industry financially but have most likely participated in the sexual exploitation of trafficking victims as well. Many pornography websites, including the largest and most visited pornography website in the world (link is to an advocacy group video about the website, not the website itself, obviously), rely mostly or entirely on user uploaded content and do not have sufficient screening criteria in place to prevent the uploading and viewing of content showing the sexual abuse of children or adolescents, or content showing non-simulated rape and sexual torture. In fact, videos are often tagged with words like “teen”, “young girl,” or “innocent” in the title, yet are still streamed from their website without additional vetting or any requirement to prove that the women in the videos are actually consenting adults. This is not a theoretical risk; the sexual abuse of teenage girls and even children being streamed from these sites has been well documented. And once these videos are available on the internet, they can be next to impossible to have removed, as we have heard from survivors who have battled to have videos of their own rape taken down from these websites.
You can fight both right now.
As a physician, I’m here to tell you that you can fight COVID-19 right now in the comfort of your own home (by, you know, staying there). Wear a mask when you leave the house, physical distance while building up your social circle, reaching out to neighbors, loved ones, and friends remotely to see how they are doing 6 months into this pandemic and if there’s anything they need. Help fight against medical misinformation that contributes to unsafe, pro-COVID behaviors and attitudes. And you can fight human trafficking right now as well. Start reading with one of the resources above and keep reading and educating yourself about this important topic that isn’t going to go away even once COVID-19 is a distant memory. Look into the ways that your clothing, your food, and your other purchasing choices might help or hurt the plight of slaves around the world. If you’ve read this post and have decided it’s finally time to stop using pornography, go to a website like Fight the New Drug to get more information, support, and resources, and find an accountability partner to download an app like Ever Accountable and quit porn alongside you. Finally, consider donating to an organization like International Justice Mission that actively works to intervene in situations of slavery around the world, and then sticks around to provide the legal and support services to guarantee that survivors aren’t re-victimized by their traffickers.
So no, there isn’t a fight between awareness of human trafficking and focus on COVID-19, and the people who want you to believe there is may well care about neither one of them; but we are in the fight of our lives against both, and since you do care, we could sure use your help.