
I’m seeing COVID-19 patients every day.
Last week I saw about 80 patients who had screened positive for either exposure to COVID-19 or possible respiratory viral symptoms; this week more of my time is devoted to working in outdoor COVID-19 testing clinics, so it will probably be well over 100. Some of those patients had been ‘caught’ by our screening questions but really had no COVID-19 exposure or symptoms; the lady with a chronic cough who was really just coming for her high blood pressure, the gentleman with a fever that was caused by an abscess under his axilla (we call it ‘axilla’ because ‘armpit’ sounds so un-doctory). I treated them too, of course. But for the most part people were seen in our COVID-19 focused clinic specifically for COVID-19 related concerns. I don’t have exact numbers in front of me, but of the 70 or so I tested for the virus, about 20 came back positive (Epidemiology note: this is too small of a sample to calculate anything like a test positivity rate or prevalence from), and there were at least a couple that, due to certain combinations of exposures and symptoms, I’m convinced had the virus despite a negative test (way, way too small of a sample to make any calculations from; please don’t go and quote me as saying that based on my sample of 2 out of 50 negative tests I think there is a false negative rate of 4% or something crazy like that)(although now that I look at prevalence estimates and test sensitivity, 4% is actually about right. Hmm…).
I called each patient who tested positive personally to give them the news and answer their questions. Amid the many questions I was asked (‘Should I go to the hospital’?; not now, but let’s talk again about red flag symptoms and emergency precautions. ‘Should I isolate from my children?’; that’s really complicated, and it depends on the age of your children, your support structure, and their specific developmental, physical, and emotional needs), one question that came up over and over again is one I sincerely wish I had a better answer to; ‘what medicine can I take to make sure this gets better?’
This is a big and important question. Doctors kind of like medicine; kind of a lot. After all, prescribing them is a big part of our job, and even though adding a medication is not always the right answer (more on this later), it is incredibly satisfying to prescribe the right medication or therapy for the right diagnosis and then see your patient get better. It can also be fairly stressful at times, because no medication (except prenatal vitamins) is perfectly safe; giving someone a medicine, especially one that wasn’t actually necessary, and then seeing them suffer because of drug interactions or unexpected side effects is devastating to a physician. We have taken an oath to ‘first do no harm,’ and we take it seriously. This is why I’ll spend 10 minutes carefully explaining to a parent about how viruses and bacteria infect the body differently and how antibiotics work rather than spend 2 minutes prescribing their child an unnecessary antibiotic for a viral illness, which would surely feel more satisfying for both of us. It is also why, as certain as I am that some of the patients I have shared the news of a positive COVID-19 test result with will end up getting sicker, and as nervous as that makes me on their behalf, I have not been prescribing unproven, untested medications out of desperation, but have instead focused on teaching those patients how to keep themselves and others safe and how to recognize the early signs of a severe infection.
It’s also why I check for new or updated studies or professional recommendations, and review information being shared between doctors and other clinicians on COVID-19 social media groups every every single. The moment that there is a proven, safe early therapy to prevent COVID-19 infections from becoming severe, I will be the first to start using it.
Dr. Richard Bartlett discovers silver bullet for COVID-19.
Last night I came across a viral video, which has since been sent to me multiple times, which seemed to promise exactly this. A doctor here in Texas went on a morning news show to discuss the 100% effective, perfectly safe COVID-19 treatment he is using to prevent severe illness in his patients. If you have any degree of medical training or even personal experience with medical issues, you are probably just as skeptical as I am about both the ‘perfectly safe’ and the ‘100% effective’ claims; few medicines are ever either. We will go through Dr. Bartlett’s interview in detail below and try to evaluate the quality of data he is relying to make these claims, and answer two questions; should you call and ask your doctor for this ‘new’ treatment, and should I call back all of my patients and tell them, much to my satisfaction, that we do have a medication I can put them on after all?
One quick note: the video is about 30 minutes long and trails off a lot into conspiracy territory concerning mandating vaccines, instituting lockdowns to destroy the economy in order to hurt President Trump’s reelection chances, and quite a few other areas. We’ve covered a lot of that before, and frankly a lot of it falls outside the realm of medical misinformation. We will try to cover the most important parts of Dr. Bartlett’s interview regarding his new COVID-19 therapy, but I won’t try to write the 10,000 words it would take for a rebuttal to all of these ideas.
Here is the video:
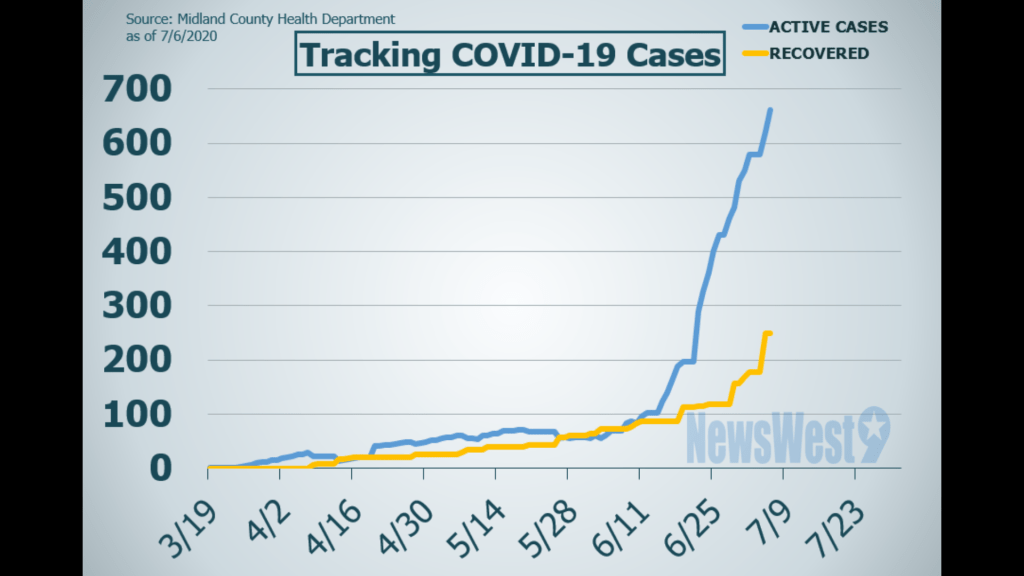
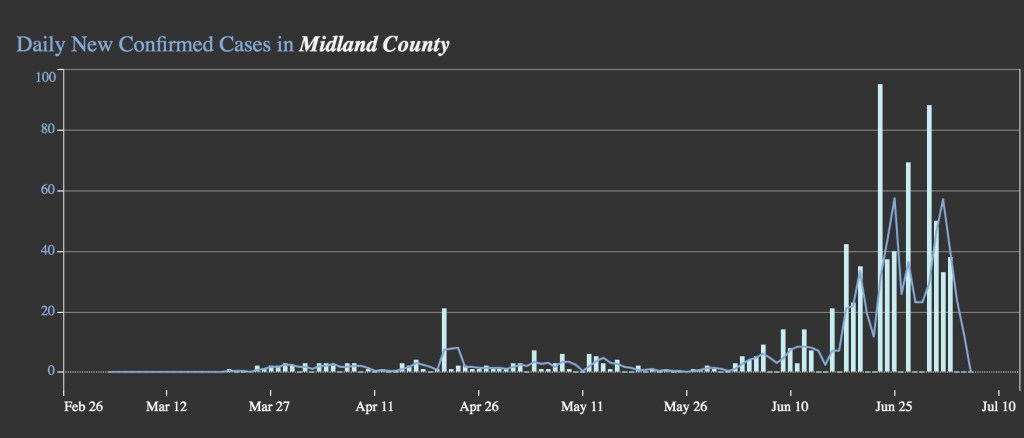
00:16: Midland Texas is located in Midland County, about 6 hours West of Waco (golly, Texas really is huge). With a population of 138,000, it is almost exactly the size of Waco. Just like for us and the rest of Texas, they began to see a significant increase in COVID-19 infections about 3 weeks ago. Before this, they had seen very few cases total, like most pre-surge areas. You can review their data here.

00:33: The article is here; it provides some additional details and we will reference it later.
01:48: Dr. Bartlett’s book is entitled Journey of a Medicine Man: Doctor Confirmed Miracles.
COVID-19 in the USA compared to around the world.
At 02:04 Dr. Bartlett begins his discussion on COVID-19 treatment in earnest by discussing the context for the pandemic in America, namely a comparison to both nations that have fought the pandemic successfully and those who have struggled more with a higher number of infections and deaths. He begins with Taiwan.
02:07 “In the country of Taiwan there’s over 25 million people, they’re stacked on top of each other, if they did social distancing they’d be out in the ocean floating around.”
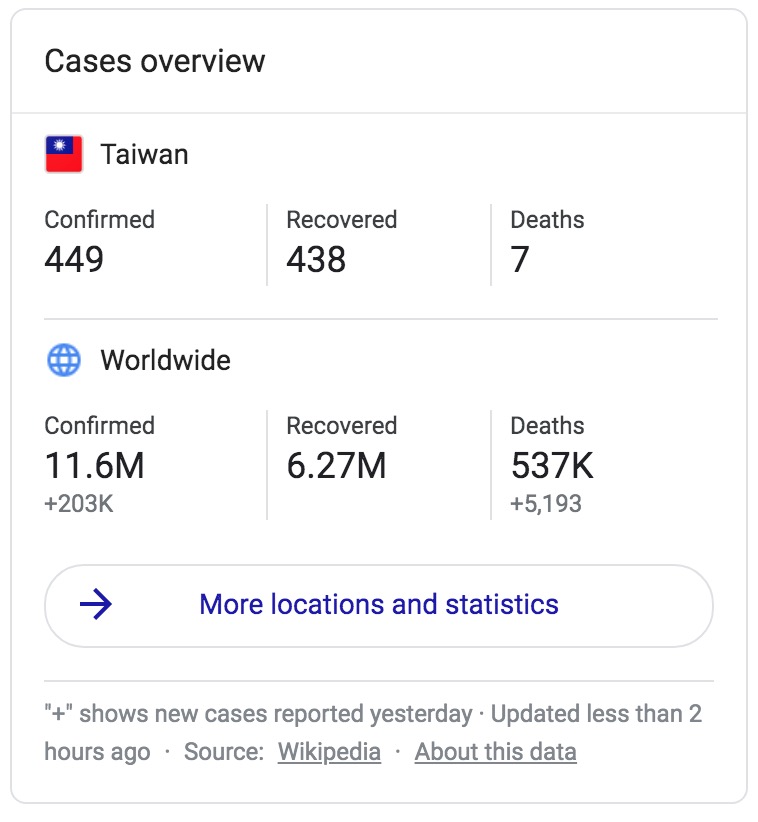
He goes on to say that there isn’t enough room to social distance, and yet the country has seen only 7 COVID-19 deaths, “as many people as you could stack in a minivan.”
The problem here, besides Dr. Bartlett’s strange obsession with stacking people, is that Taiwan has done social distancing. Dr. Bartlett goes on in the video to assert that Taiwan has foregone both social distancing measures and widespread face mask use (which he associates with Communist China). Do any reading on Taiwan’s response to COVID-19 and you will find widespread wearing of face masks and aggressive physical/social distancing measures since the earliest days of the pandemic, in addition to other mitigation strategies such as providing social support for quarantined patients to help them maintain a high level of isolation, and using mobile phone technology to perform extremely precise contact tracing. This is all in the context of a strongly collectivist culture willing to engage in such measures for the good of their neighbors regardless of official mandates, with a history of understanding the stakes in such a pandemic because of their experience with SARS in 2003.
So as Dr. Bartlett moves forward talking about Taiwan later in this video, you need to understand that, perhaps entirely unintentionally, almost everything he has said about their success in fighting COVID-19 so far is the opposite of what they have actually done.
02:41 At this point Dr. Bartlett also mentions Iceland, Singapore, and Japan, who all engaged in some combination of extensive masking and social distancing except Iceland, who used aggressive contact tracing and quarantine measures. Dr. Bartlett’s assertion that they have been successful because they have used similar treatment plans to what he uses for his patients seems entirely unfounded.
02:59 “That’s not possible according to what we’re being told in the mainstream media.”
Literally nobody is hiding this data. If you google “Taiwan COVID” you get this:
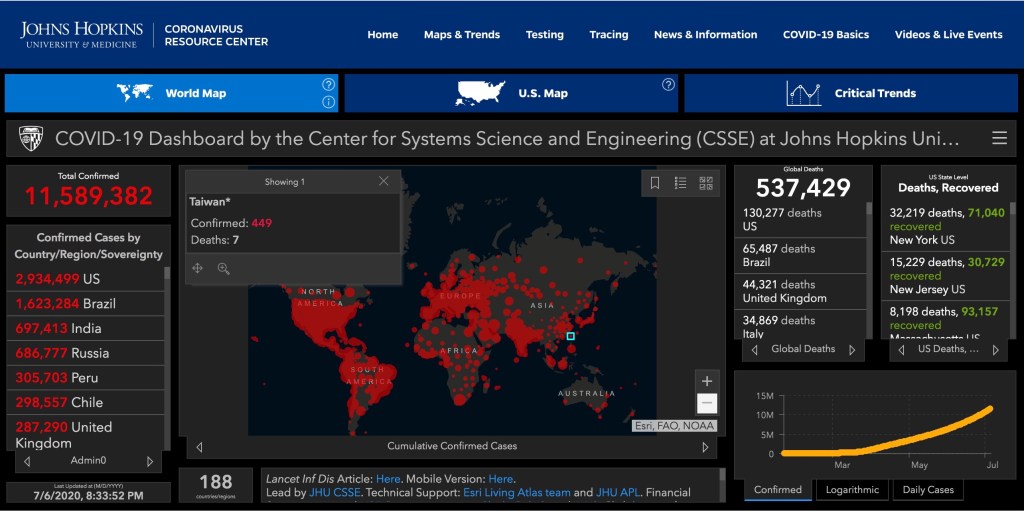
“You can even look it up in the Johns Hopkins COVID website and you’ll see those numbers. They’re hidden in there, but I’m pointing them out.”
I’m concerned that what Dr. Bartlett is doing here is contributing to a false narrative that the powers that be, especially the CDC, the WHO, and the medical establishment (i.e. he and I), doesn’t want people to have access to good reliable data. Maybe this is where Dr. Bartlett’s search for reliable information to back up his COVID-19 treatment has led him; not trusting the available information because he wasn’t able to find the scientific verification he is sure must be out there for his new therapy. Maybe this is strongly ingrained in his political position (he recently ran for office) and he is interpreting the ready availability of this kind of data through a lens of suspicion, or knows that his audience on this show will affirm the idea that this information is being hidden from them and that it is harmless to reinforce that belief. But I am always a little suspicious of physicians who want to weave these tells of conspiracy theories and hidden truths about the pandemic while promoting their own unverified findings, and part of me wonders if they are certain they will face pushback from their fellow doctors and scientists, and want to head it off at the pass by encouraging the idea that those doctors and scientists don’t want you to know ‘the truth.’ I certainly hope this isn’t the case with Dr. Bartlett, but part of me thinks it must be an easy trap to fall into without realizing it.
It isn’t Hydroxychloroquine
03:32 “(In these other countries) they’re doing what I’m doing, which is not hydroxychloroquine, although that works….
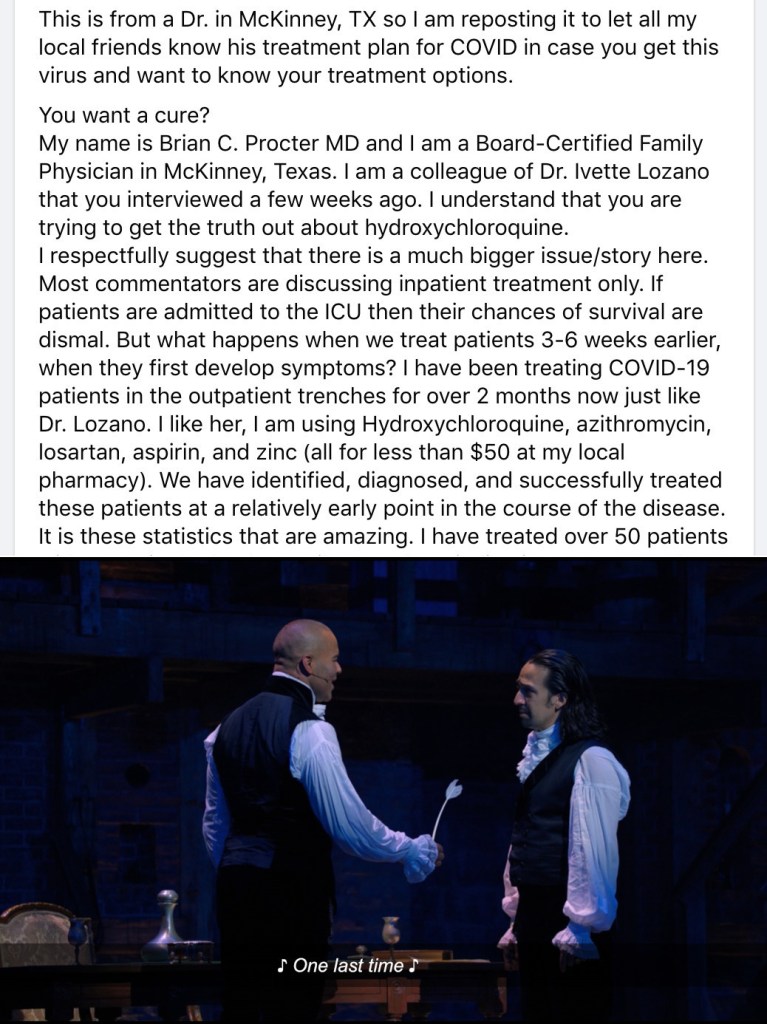
Before he reveals his miracle drug, he gives a brief shout-out to Hydroxychloroquine, stating it does work but not providing further explanation as to how he knows it does or why he doesn’t use it as well. I almost wrote today about a viral post by a doctor in McKinney Texas again promoting outpatient, widespread hydroxychloroquine use in patients regardless of test results and risk factors. We covered this pretty extensively over a month ago following his colleague Dr. Lozano’s speech at the Set Texas Free Rally in Dallas. He also claims that masking, social distancing, and even testing are ineffective. I’ve chosen to write about Dr. Bartlett’s video instead, but in terms of relying on anecdotal evidence and not understanding representative sample sizes, there are a lot of similarities. If things are quiet this week I will try to write about Dr. Procter’s social media post as well and try to tackle hydrochloroquine one last time.
I want to talk hydroxychloroquine.
I want to talk about these scripts that you’re writing;
Put down the pen, stop prescribing.
I want to talk about what I have learned,
About the research you have spurned…
The Silver Bullet: Inhaled Budesonide
03:36 “So what they’re doing is an inhaled steroid. So my silver bullet is inhaled budesonide.”
Dr. Bartlett finally reveals his miracle drug, inhaled budesonide; a commonly used inhaled corticosteroid that is commonly used for patients with Asthma or COPD.
This is the first good place to stop and look at this idea in more detail. The first two questions we need to ask when someone proposes a novel use of a medication or therapy are 1. Is there a proposed mechanism by which this would work? 2. Why did nobody else think of this (has this been tried/studied before)?
Dr. Bartlett’s rationale is that since this is an inhaled respiratory anti-inflammatory, it should work for COVID-19 which is a ‘respiratory inflammatory condition.’ Part of the problem here is that this is gross oversimplification of the virus’s pathophysiology, which is still not completely understood (see below). It is supposed to make you go “wow, that’s just common sense! It causes inflammation in the lungs, so an anti-inflammatory breathed into the lungs will cure it!” But if you reflect on whatever extent of experience you have with medicine, you will realize that things are never quite that simple. If you came to me for your severe, debilitating back pain you’ve been struggling with for years and I said, “oh I’ve got it, back pain is caused by inflammation of the muscles and joints, so I’ll give you a medicine to decrease inflammation; here’s some ibuprofen,” you’d probably lose a great deal of respect for me. You’d be right to. NSAID’s (non-steroidal anti-inflammatory drugs, like ibuprofen) may well be part of your treatment plan, but your back pain is complicated and is going to require more thorough evaluation and treatment. In medicine, you are right to beware of easy answers.
Budesonide is a common medication, as he points out repeatedly beginning in a few minutes, and I think this is actually the strongest argument against his proposed use of it in COVID-19. You read that right; I’ll explain. The usual dosing of budesonide is twice a day as a maintenance medication; by decreasing inflammation and swelling in the airways, it can eventually (it may take weeks to months) lead to less frequent asthma and COPD symptoms like cough and chest tightness, and fewer exacerbations. However, Asthma and COPD patients still have acute exacerbations despite using inhaled corticosteroids. We still see patients on budesonide in the clinic and in the hospital for acute worsening of their symptoms due to respiratory infections. Sometimes these are bacterial infections, but more often they are viral; including coronavirus species. Sometimes these patients go into respiratory distress, and sometimes die, even when the virus they have isn’t nearly as deadly as COVID-19. If budesonide was able to completely prevent viral respiratory illnesses from causing inflammatory respiratory symptoms like cough, shortness of breath, wheezing, and chest tightness, we would never see these patients getting sick from respiratory viruses; but we do, because the medication doesn’t really work that way. If Dr. Bartlett consulted his complex understanding and professional history of treating respiratory infections he would realize that his proposed mechanism really doesn’t make sense, especially as the 100% effective silver bullet he is promoting it to be.
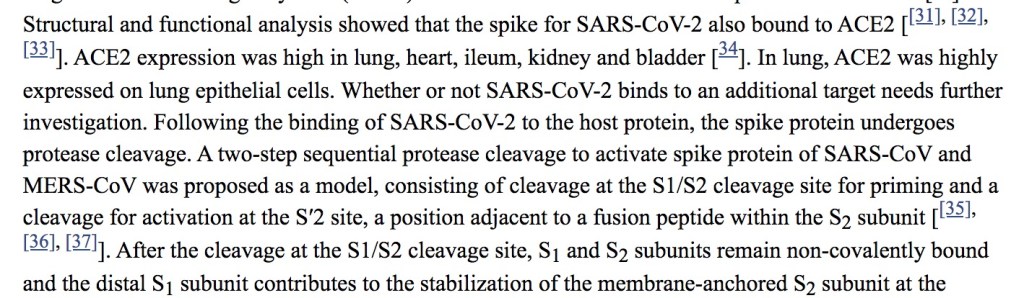
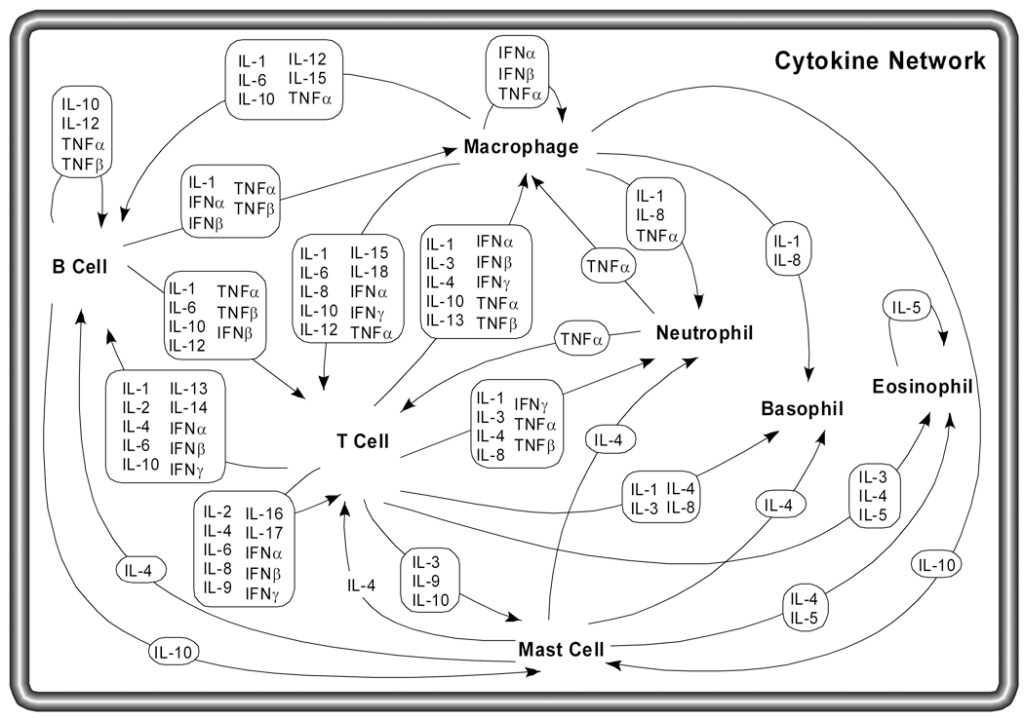
Later in the video (around the 06:36 mark) Dr. Bartlett does talk about the “cytokine storm” in COVID-19 and prevention of the body’s own inflammatory response to the virus. Is it possible that the medication he is using, while not preventing all respiratory viral infections, at least treats this one? Without getting into the weeds too much here (the idea of a cytokine storm being the underlying cause of ARDS in COVID-19 is still controversial), we need to understand that you don’t just have this one thing called ‘your immune system’ causing this process called ‘inflammation’, so that if ‘inflammation’ (or in this case, ‘cytokine storm’) is the problem we can just suppress the immune system and call it a day. The immune system is incredibly complex, and any given immunomodulating medication is going to work on parts of the immune system (and not always in the ways we hope or expect) while not significantly affecting others. As an example, the primary cytokine implicated in the COVID-19 cytokine storm seems to be interleukin 6, a pro-inflammatory cytokine that budesonide, in previous studies unrelated to COVID-19, doesn’t seem to affect appreciably. Studies focused on medications that do appreciably decrease IL-6 activity are currently underway.
The second question, if the mechanism did make perfect sense, would be to ask whether anyone has tried this before. Dr. Bartlett indicates that it has been tried elsewhere; he states that this is what they are doing already in Taiwan and Singapore. I was unable to substantiate this; I cannot find any evidence that these nations have used anything like widespread protocols with inhaled steroids to treat COVID-19 early in the disease course. There are some ongoing trials with use of inhaled corticosteroids (not budesonide, at least that I could find), as Dr. Bartlett mentions, but there is not any data available from them yet; if they prove safe and beneficial for COVID-19 patients, we would start using them in all the clinical contexts where they were shown to be effective.
There are two other data sources we could look at. First, the most successful trial we have right now with use of steroids in COVID-19 is the RECOVERY Trial out of Oxford, which I wrote about recently. In this study patients were put on systemic steroids (dexamethasone) once they were already hospitalized. You might argue that this isn’t what Dr. Bartlett is talking about at all, that he wants to use budesonide before they are sick enough to go to the hospital. I understand that; but the study showed a reduction in mortality in both the groups needing oxygen and those requiring mechanical ventilation, but not in those who didn’t require oxygen. You can only extrapolate so much from this, but if Dr. Bartlett’s theory of the earlier the steroids the better panned out, you would expect the non-oxygen group to see at least as much improvement in outcomes as the patients who were already very, very sick; but that wasn’t the case. We need to remember that even though our first successful randomized drug trial for COVID-19 is indeed a steroid, the role it plays is complex and the benefits limited to certain clinical scenarios; the data still shows that immunocompromised patients, including those on medications that modulate the immune system, are at a higher risk for COVID-19 than those who aren’t.
We can also look at the two closest viruses to COVID-19 that we have experienced, SARS in 2003 and MERS in 2012. These are both Coronaviruses that seemed to involve a ‘cytokine storm’ causing acute respiratory distress syndrome. During these outbreaks inhaled corticosteroids were used more widely, but results were mixed; there was no strong evidence of benefit, and some evidence of worsening of the disease, including increased risks of secondary bacterial pneumonia and prolonging the time it took for the body to clear the virus.
Edit: When discussing this issue, a colleague also pointed that this idea of ‘what about decreasing inflammation in the lungs’ is not novel, and studies have tested inhaled corticosteroids on practically every lung infection (infection is a very pro-inflammatory state) over the past 30 years, not just SARS and MERS. Results have been extremely unimpressive, but there has been consistent evidence of increased risk of certain types of lung infections, including tuberculosis, non-tuberculosis mycobacterium infections, and severe drug-resistant bacterial pneumonia.
So I’ll conclude this section where many people with much more expertise in this area than myself have, by saying that the balance of risks and benefits still doesn’t justify use of an inhaled steroid in people without asthma or COPD who are already taking one or would benefit from one anyway. There is no reason to believe that they will appreciably decrease the chances of developing the severe acute respiratory distress syndrome that makes the virus so dangerous for some people, and for the vast majority of people who will do fine with their own innate immune system fighting the virus, steroids would potentially increase both the risk of worsening infection and delayed clearance of the virus, and the risk for associated bacterial infections (in addition to a host of other potential side effects). If we were to begin using this in patients who don’t have COVID-19 as prophylaxis, we could conceivably increase their likelihood of getting the virus. The mechanism of causing these types of harm is at least as strong as the proposed mechanism of preventing worsening of the disease.

03:46 “It’s super cheap, it costs about $200 for the total treatment if you pay cash.”
I understand that he is probably intending this as a comparison to a hospitalization for COVID-19, which is disastrously expensive, as he truly believes the budesonide will prevent hospitalization. Still, all I can say is that Dr. Bartlett and I have different ideas about what constitutes super cheap medication; most of my patients could not afford a $200 medicine.
“But what does all of that matter? He said it is working for his patients.”
There are some more problematic statements in this video, including the idea that our numbers in Texas are only going up because of increased testing (17:05), revisionist statements that totally invert the sequence of events and thus cause and effect of social distancing and masking measures in the most affected countries (21:50), a troubling statement about Japanese people ‘crawling all over each other in Sushi bars’ (22:55), and strangest of all, repeated statements about how waiting to treat someone until they have symptoms is un-American, whereas early treatment is the American way (both preventative and acute care are part of every healthcare system in the world; there is nothing particularly American about throwing medications at people before you know whether or not they need them).
I hope to update this post with some rapid-fire answers to these issues later, but I want to focus here, for now, because I sincerely believe this is the part of Dr. Bartlett’s interview that people find most convincing.
“One hundred percent of my patients are alive. I’ve been treating this since March.”
I’ve written before about the dangers of anecdotal evidence. I think as physicians we are prone to fall into this trap for a couple of reasons. One is because we want so badly to help our patients, and if we hit on a medication that really feels like it is working, it’s hard to let go of that feeling. Another is because we spend so much time thinking about our patients and working for their well-being that their stories loom very large in our minds, and it’s easy for the relative importance, as data, of our personal small numbers of cases to become overinflated. With that in mind, I think it’s worth looking at Dr. Bartlett’s evidence from the outside and asking whether it really has the value he credits to it.
According to the local news article featuring Dr. Bartlett back on May 21st where he first publicly called budesonide his ‘silver bullet’ against COVID-19, at that time he had treated 12 people. Twelve. This is an incredibly small sample size, but we could hardly expect larger; Dr. Bartlett is not the only doctor in Midland, and throughout March, April, and May the entire county only had 1 or 2 new cases of COVID-19 most days; there just weren’t that many COVID-19 patients to go around. Dr. Lozano had previously gotten around this issue by saying that she wasn’t even testing, but was treating empirically based on symptoms or possible exposure, which doesn’t really make sense in a pre-surge area with incredibly low prevalence. Dr. Bartlett has stated that he believes in testing, and although his comments are mixed on whether he is treating only confirmed COVID-19 cases with budesonide, I think we could credit him with such qualms. Twelve cases over 3 months is an extremely small sample size, and it is important that we understand that this is not coming from someone who has been inundated with COVID-19 cases like our peers in New York; at the time that Dr. Bartlett decided that budesonide was a miracle drug he had practically no experience with the virus. It is certain that his numbers have come up by now, with cases rising all across Texas; but with lag time between exposure and the onset of symptoms, and a second lag between the beginning of symptoms and severe respiratory complications, it is not possible to say that all of Dr. Bartlett’s recent COVID-19 patients are out of the woods yet.
So Dr. Bartlett’s first error is over valuing the data from his sample size, but his second error is in thinking this disease is more dangerous than it actually is. I know that seems like a strange thing to type; the disease is plenty dangerous, and I have encouraged the utmost caution on this blog more times than I can count. We have looked over and over at the hundreds of thousands to millions of lives that might be lost if we do not discover effective drug therapies and if the virus continues to spread unabated because of poor adherence to mitigation strategies like face masks and physical distancing. But the virus has never been estimated as having a 20% fatality rate as Dr. Bartlett says in the video. Dr. Bartlett has no doubt been worried about COVID-19 since March, just like me. Just like me, he probably has friends and classmates working in ER’s and hospitals in New York and New Orleans and other areas that have already been hit hard, and has heard the horror stories about what this can do to both individual patients and entire healthcare systems. Like me, as soon as he started thinking about this respiratory virus he probably immediately thought of the names and faces of two dozen patients that he was particularly worried about. Due to this anxiety, surviving the virus has become, in his mind, the exception rather than the rule. We see this in his account of the woman battling cancer; he says “she should die according to what you hear from the CDC and the WHO,” even though we know that COVID-19 is not universally fatal for any group. By increasing the danger of the virus in his mind, or at least increasing the probability that any given patient will go to the hospital or die, it makes it seemingly unlikely for people to get better without some specific intervention, even though we know that is what happens most of the time; thus the interventions he has chosen (budesonide, zinc, antibiotics) receive the credit for his patients’ recovery.
Put these two biases or statistical errors together and it may be easy for a physician to believe, based on the slightest of clinical experience with this virus, that he has discovered a cure. Each patient you treat this way will confirm it for you, as long as they get better, even if they would have gotten better anyway, and particularly if they tell you they feel better right away, which is such a wonderful feeling even if it doesn’t always correlate to their eventual outcome. If you are willing to loosen your treatment criteria to include people who have had no test or negative tests, or who are fully asymptomatic as Dr. Lozano seems to have done with hydroxychloroquine, you can inflate your treatment numbers even higher. And if you top-out at something manageable for a small-town physician, say in the low 100’s, you might never see a fatality from COVID-19. Imagine that we were back in May when Dr. Bartlett had only treated 12 COVID-19 patients. He states boldly that 100% of his patients were alive, yet we think the death rate is around 1.3%. If just one of his 12 patients had died we might still find this convincing because we are so easily swayed by anecdotal evidence, but that would have been a fatality rate of 8.3% in his budesonide patients. We would have fallen into the same trap as Dr. Bartlett, of picturing those 12 patients heading toward certain demise and all but one rescued by his treatment plan, without which they would have died, when in reality there is no evidence to suggest that they would have been any worse off without the treatment. Dr. Bartlett’s experiences with the virus so far are exactly what we would expect without budesonide and antibiotics.
“Look, he says it is helping his patients and you don’t have to use it for yours, so why does it matter to you?”
Great question, hypothetical person who keeps arguing with me on the internet. Any time we begin talking about someone’s personal experiences, the temptation is to treat their narrative as incontestable; I wasn’t there, I didn’t see his patients, so I don’t have the ability to second-guess his clinical judgement. In a way this is actually sort of fair; Dr. Bartlett had just as many years of medical school and residency as I did, and has many years more clinical experience, and to some degree each physician has earned a degree of professional trust to practice in a way we see fit with accountability only to ourselves and our patients, at least in many circumstances. But we know that this professional leeway has been abused in the past, and even in the absence of abuse of that privilege, lone-wolf medicine is a real problem because by it’s very nature it is disconnected from one of the best tools we have to improve our clinical abilities and correct our errors; the honest feedback and accountability of our fellow doctors. If a physician feels that a patient’s clinical situation calls for a unique approach that is not supported by evidence, this can often still be tried as long it is accompanied by an honest and careful explanation to the patient of the reasoning behind this approach, the unproven nature of the treatment, and the risks involved. If we begin to make a habit of such practices, and particularly if we do so ignoring the voices of our peers around the world saying we’ve tried this before and it didn’t show reliable results on a larger scale, or the voice of researchers and scientists saying that doesn’t actually work the way you think it does, then we are doing so at our own, and more importantly at our patients’, peril.
In many ways I think Dr. Bartlett is actually going about this fairly well. He seems to imply that he is using the medication, which does have a theoretical mechanism of action after all, only on those who really do have COVID-19. He does not seem to be doing television interviews or talking with newspapers in order to make a name for himself and attract clientele from all over the state to help his business, as seems to be the case with some other doctors prescribing unproven treatments, but in order to ‘get the word out there’ to other doctors (as one of those other doctors, I deeply appreciate this impulse), although I am not sure why he has not utilized any of the many avenues on social media that many of use are using to get physician specific feedback and share ideas; maybe he is and we just aren’t part of the same COVID-19 doctor groups. Most importantly, he states that he has written and is submitting a paper for publication, which will provide both more details about his patients, their demographics, commodities, and clinical presentations, and allow for peer review and a higher degree of detail and scrutiny than we could possibly get through a TV interview.
But there are at least three ways (besides the tacit endorsement of several conspiracy theories) that I find Dr. Bartlett’s approach truly troubling. First, he is not presenting his treatment plan as an entirely unsubstantiated experimental approach driven by hope and a hunch, which is what it absolutely is, but as a “Silver Bullet” that is perfectly safe and cannot fail, which is certainly is not. One would hope that this is bravado or enthusiasm for the TV audience and not hubris; in other words, we have to hope that whatever confidence in his treatment regimen he shows in this interview, he is still very carefully explaining to his patients the limitations of his evidence and the potential risks they are taking on if they use it, and the red flags to look for in case it doesn’t work.
Second, he is not just promoting his unproven treatment but also discouraging mitigation measures, such as physical (social) distancing and wearing masks, that actually have been proven to save lives. It is unclear whether he believes the misinformation around these strategies not working or is just so confident in his treatment approach that he no longer thinks they are necessary, but the effect will be the same; as Dr. Bartlett’s video goes viral there will be increased pushback against wearing masks and observing distancing measures by those who find him convincing, which will ultimately lead to more cases, more hospitalizations, and more deaths. His evidence is too weak and his scientific rationale too shaky to convince a conscientious doctor to start using his treatment approach; but he speaks with enough confidence and sincerity to convince some people on the fence not to wear masks. The net effect of his interview, like any viral misinformation, is to make the pandemic more dangerous for everyone.
And third, by presenting his treatment plan as something that it isn’t and ascribing to it all of the confidence and reliability of a truly proven treatment, he is spreading misinformation that blocks out the transmission of reliable information for the public and pollutes the relationship between his listeners and their own doctors and healthcare systems. When I explain to patients that I do not have a proven medication I can in good conscience prescribe them to prevent their COVID-19 from progressing, their exposure to voices like Dr. Bartlett’s, Dr. Lozano’s, and Dr. Procter’s have already sewn the seeds of mistrust in the information I am providing, and they are less likely to believe the other recommendations I am carefully trying to give, such as isolating within their home and monitoring for red flag symptoms, and the reassurance I am trying to provide to alleviate their fear and anxiety as we discuss their individual chances of having a severe course of the virus. It may lead anxious patients to seek additional visits elsewhere and shop for a doctor that will prescribe them what Dr. Bartlett says they need, further increasing their chances of exposing others and potentially increasing the costs associated with their medical care, both to them personally and to an already strained system. It may even lead some patients, convinced by these doctors and desperate for medicines they now believe are their only hope of beating the virus, to misrepresent their symptoms in ways they think might push their doctor into prescribing them.
When lone wolf doctors promote unproven therapies and set themselves up as experts with miracle cures, without having actually done the clinical research to validate their claims, it erodes the fragile trust that we work so hard to build with our patients when we are unwilling to engage in that same type of speculative treatment. This unearned mistrust has the potential to breakdown the patient-physician relationship and affect our patients’ health for years to come. Millions of doctors, nurses, and other medical professionals around the world are working as hard as we can to both care for our patients in the midst of this pandemic and stay up to date with the latest diagnostic and treatment options. Viral voices drowning out the excellent work that is being done researching potential treatments, and calling out any doctor not willing to follow their lead, should humbly re-evaluate their limited clinical experiences in the face of this global pandemic and bring forward their innovations, not with less hope or enthusiasm, but with much more care and a realistic appraisal of the strength, or lack thereof, of their evidence.
