Final Thoughts
I know this seems like a strange place to add my final thoughts (one might have expected them somewhere near… the end), but I want to honor the long tradition of TL;DR that has come before me. PlanDemic has been a fairly unique experience among COVID-19 misinformation videos so far. The production quality is much higher and the narrative, tied to the experiences (questionable though their veracity may be) of an individual scientist, is gripping. The story telling here is far, far better than any of the webcam style videos we have looked at so far, or even the interviews of Dr. Erickson or Dr. Ayyadurai. It’s actually hard to know how to categorize this video; is it an anti-Medicine conspiracy video capitalizing on COVID-19 fears and controversies, or is it a COVID-19 medical misinformation video set in a conspiracy theory narrative? Probably both, but I lean toward the former because while the conspiracy theory is well established and consistent, a brief version of the story Dr. Mikovits has been giving as her own interpretation of the events of her arrest and discreditation for years, the actual arguments surrounding the COVID-19 pandemic are piecemeal and self-contradictory, pulling from any and all vogue COVID-19 misinformation sources rather than forming any new or unified thesis. Still, given the popularity of this video, I will not be surprised if we begin to see more and more of these high production quality misinformation/conspiracy theory pieces; it seems to be an effective amalgamation.
I hope my reflections below prove helpful. My hope is that even if you do not have time to read this entire post (and I can’t blame you there; I don’t have time to read it either), you will be able to navigate to the analyses of one or two of the points from the video that you have particular questions about. If I don’t cover the points you are particularly interested in, feel free to comment below; or better yet, keep digging- I’m sure someone else has done a more thorough debunking on that point than I would have anyway. Thank you to those who have found this analysis relevant enough to share with friends and loved ones who are convinced by or sympathetic to the PlanDemic film; I hope that this information, combined with their affection and trust for you, is enough to open their eyes to the falsehoods being shared so widely, and to convince them to continue exercising caution against this terrible virus.
The link to the video that I originally shared is dead. It is still easy enough to find if you really want to watch it.
First Impression: The production quality here is going to be awesome. (00:04)
Learn about your sources before watching, and then watch critically. (00:10)
This is just good general advice; we trust far too much to our gut feelings (read: confirmation bias) when trying to decide on the veracity of new information. When I wrote about navigating medical misinformation during the pandemic, the first piece of advice I gave was to know your source. I would never argue that arguments can be discounted because of the source; but knowing something about the source is incredibly useful when engaging internally with the arguments, especially when choosing what degree of scrutiny to apply to them. This is especially true with a video like this one. The excellent production quality, the artistic filming and intentional choice of background music, the cinematography and editing, all of it is designed to be emotive and to render the content convincing. That’s not a bad thing; they want you to believe their message, presumably because they strongly believe it themselves. But when all of these features have the net effect of lending credibility to the speakers in the video, we may find ourselves attributing to them a certain expertise or background that may or may not fit. Knowing where they are coming from, who they are, and what they stand for before the emotive music begins gives you some context for weighing their claims outside of how those claims make you feel, or how much you would like to believe them.
By the way, this is the same advice I would give to someone visiting a church for the first time; don’t rely on your gut feeling as a guide to truth; emotive music and a well crafted stage presence can be incredibly convincing.
With that in mind, here are a few links to the main people involved in the video:
Dr. Judy Mikovits is a former researcher who holds a PhD in Biochemistry and Molecular Biology from George Washington University. She published a since-retracted study in Science in 2009 that eventually lead to the legal action she discusses in the video. You can read more about her on her wikipedia page or on the blog Retraction Watch, if it is ever back up again (I believe the viral video has crashed the site multiple times). Since then she is mainly known as a frequent speaker at anti-vaccine events.
Mikki Willis is founder of Elevate, the production company that released the documentary. Their prior work tends to be focused on spiritual energy and positive vibrations (they have a short video talking about restoring your frequency to protect against COVID-19), but this seems to be their first foray into medical misinformation viral videos. You can check out his facebook page here. Before this I believe their biggest documentary was Neurons to Nirvana: Understanding Psychedelic Medicines. Also, as someone who has been interested in televangelists and pseudo-christian faith healers for years, he strikes me as the non-religious, spiritualist version of the young, good looking charismatic faith leader.
The Minions of Big Pharma (O0:38)

This is my first red flag in the video. “For exposing their deadly secrets, the Minions of Big Pharma waged war on Dr. Mikovits, destroying her good name, career, and personal life.” Now, “Minions of Big Pharma” may mean a lot of things; he might be referring to actual lawyers who work for pharmaceutical companies, or to all pharmaceutical employees (although it’s hard to see how drug reps could ruin her personal life), or to some other group altogether. But in the alternative health world this typically refers to doctors and scientists (nurses are generally excluded because as a society we actually like them, so it’s dangerous to the alt-health narrative to loop them in on conspiracy theories)(oh, and happy Nurses Week to my brilliant and beautiful wife!).
Now, I can’t comment much on Scientists working in the lab, since that hasn’t been a major part of my life, but I pretty strongly suspect that they have little to no interest in ruining anyone’s career (and if stereotypes are anything to go off of the only personal lives they are ruining are their own! Bazinga!). I know scientists who have worked for Universities and for major corporations and their main interest has been, unsurprisingly, Science. They love talking about their experiments and research, and their ideas about what might happened next with their project. Remember that these are not nameless and faceless people doing experiments in some hidden lab; these are often the sciency kids that you went to high school with who genuinely loved experiment day in Chemistry class and who were probably reading Lord of the Rings before it was cool. And it’s these science nerds, according to this video, that have now all been recruited into a world wide conspiracy. Tony Fauci calls up one of them and says, ‘we need to discredit a virologist because we don’t like her conclusions about retroviruses; publish a fake study that says she’s wrong.’ It’s really, really far fetched. In fact, if you want evidence of the standards of veracity that scientists generally hold each other’s research to, look no further than Dr. Mikovits’s retracted paper in Science, which was retracted not because she was rocking some boat or bucking some system, but because the methodology was flawed and the results were not reproducible. If you’ve forgotten everything else about those Science Fair geeks from high school, remember this; we loved proving people wrong. The peer review process capitalizes on that, and the conspiracy that there’s a top-down cabal determining what gets published and what doesn’t ignores that one overarching character flaw.
What I can tell you, with no shadow of a doubt, is that your doctor doesn’t work for Big Pharma. In fact, the relationship between your average Physician and the drug reps they interact with range from the politely tolerant to the openly antagonistic.

And this is the case for any part of the medical industry that is primarily profit driven, whether it’s the pharmaceutical companies, fly-by-night medical supply companies, pharmacies, or the insurance companies. Because Physicians are not primarily profit driven; we are driven by a desire to help people. We are driven by a desire to help people so much that it is dangerously cliche to even say so on a medical school admissions essay. We’ve taken on hundreds of thousands of dollars in debt, sacrificed our 20’s and 30’s, and worked thousands of hours of unpaid overtime in order to learn the science and the clinical skills that we need in order to do the grueling work of helping people heal physically, emotionally, and psychologically, and there are just much, much easier ways to make money.
So that creates conflict. Conflict ranging from an annoyed ‘I don’t think that’s accurate’ to a pushy drug-rep overselling the latest product, to absolute rage when the price of a life-saving medication skyrockets for artificial reasons and my patients suddenly have to go without. But while we generally regard for-profit pharmaceutical and insurance companies to be side effects of a deeply broken healthcare system, they are still fixtures that we have to work with; and I guess that looks a lot like collusion to the outside world. Once you’ve bought into the myth that those with the most money universally control the people they interact with and endure no dissent, it’s easy to see conspiracies everywhere; of course the scientists are told what results to report, look who signs the checks. Of course the doctors prescribe what they’re told, their education is controlled by big pharma.

But might I submit that maybe ancient, altruistic, and (let’s face it) fairly egotistical professions don’t just roll over quite so easily? That maybe high standards of truth telling and care for the wellness and suffering of human beings are still the honored core of both the clinical and research branches of Medicine? In fact, I don’t think it’s a stretch to say that, to whatever degree drug or insurance companies really have wanted something like autonomous control over healthcare, it has largely been conscientious Physicians who have fought them.
But you don’t get to see those types of interactions that often at your doctors office, and this leads to a lot of pretty demoralizing misunderstandings; for instance when a patient’s medication should be $5 and they end up paying $50 at their pharmacy and think that I prescribed a more expensive medication because I’m getting a cut (this is why I now say to each patient at the end of each visit where I’ve prescribed a medication, “if you get to the pharmacy and any of your medicines are more expensive than you expected, please don’t buy it yet and give us a call instead”). It also means that when it comes to profits being put above people, we’ve probably just about seen it all, and fought against it all. So when even we have to say, yeah this looks like some pretty crazy conspiracy theory stuff, you need to understand it’s coming not from “Big Pharma’s” willing subordinates, but some of it’s most diligent and ferocious watchdogs.

“The plague of corruption that places all human life in danger.” (00:54)
I think the narrator is just waxing eloquent here, setting us up to understand that the medical field is the real plague or something like that (and if so it’s a good bit of work), but I’ll at least give the video the credit of seeming to take COVID-19 very seriously during the first minute. If you turn this off after minute one, you will at least leave with the idea that 1. there is a plague, 2. human lives are in danger, and 3. it’s a big enough problem that the fate of nations hangs in the balance. That plus the excellent production quality may go a long way towards fighting some of the ‘less dangerous than the flu’ misinformation that is out there already. Way to go, Elevate!
Minute 1 to Minute 10
The bulk of the first 10 minutes of the documentary are spent on Dr. Mikovits’s personal history of maltreatment by the health industry/scientific community. I think people should be able to tell their stories from their perspectives, and I have no doubt that the demolition of her career has been a very difficult experience for her regardless of the circumstances that caused it. Still, it is important to remember that most stories have at least two sides that have to be considered, and other interpretations of those events are available widely on the internet. It’s a very dramatic story and someone other than me will need to dissect it. I will return to this section with a few observations once I have finished the analysis of the rest of the video, but for now my most immediate concerns are the statements related to COVID-19.
Update: Having finally finished this blog post 3 days later, I have had time to read through other articles and watch other videos debunking the claims of PlanDemic. Many do it much better than I can. A great many have focused specifically on the first 10 minutes of the video, and investigating the claims that Dr. Mikovits makes regarding her own history and the conspiracy against her; many have already been familiar with this history and her work in the anti-vaccine movement prior to PlanDemic. I will defer to them. Certainly I have no first hand knowledge of the events and no background in investigative journalism. If you are watching the video, there are 3 things I would point out in this section that I think should at least increase your level of suspicion that you are watching conspiracy theorist/misinformation propaganda. 1. When Dr. Mikovits is talking about her arrest (the video leaves you to assume it was a 5 year imprisonment; it was actually 5 days), they show presumably unrelated footage of SWAT teams and urban tanks in order to inspire fear. 2. The clear implication, towards the end of this section, is that Dr. Mikovits might be assassinated for doing this interview. The credulity people have towards this claim has been amazing, with so many comments along the lines of ‘this woman needs protection now’. Yet, is there any basis for believing that there has been or will be an attempt on her life? And for what? Sharing information about the COVID-19 pandemic that is almost entirely verifiably false? 3. Dr. Mikovits has a book out. I don’t think that this is her primary purpose in giving her interview, and my understanding is that she has been involved in trying to clear her name and garner support against the scientific establishment for years. But so far, financial motivations being tied to viral misinformation videos has been batting a thousand during this pandemic.


Is this an anti-vax video? (9:48)
Dr. Judy Mikovits: “And they will kill millions as they already have with their vaccines.”
Mikki Willis: “So I have to ask you, are you anti-vaccine?”
Dr. Judy Mikovits: “Oh absolutely not!”
‘But see, she’s not anti-vaccine! This is totally mainstream stuff, not anti-vax propaganda at all!’
Rest assured that many people in both alternative health and the anti-vaccine movement see the pandemic as an opportunity to anchor their products and agendas more firmly in the mainstream. While this is often for financial profit or accumulation of power and influence (as has been the case with every single misinformation purveyor we’ve addressed on the blog so far), I still believe that here are many honest people who earnestly believe in these ideas, and merely have their facts and narratives skewed concerning vaccines specifically and the medical field in general. I know and really like some of them. In fact, a lot of friends whom you might call ‘vaccine wary’, medically suspicious, or crunchy and oily (their words!) have been incredibly supportive of me personally and other healthcare workers during this pandemic. They have struck a balance they are personally comfortable with that allows questioning their Physicians and arriving at different conclusions (which is a good thing in general) and still recognizing a bedrock of reliable truth telling regarding danger, disease, and treatment. I think all of us are looking forward to the day when we can just get back to arguing about tea tree oil in your belly button again (or was it thieves?), but with a real crisis like COVID-19 there is no question that we are all on the same side.
The problem is that as a counter-culture, these movements have overall tended to have a very low threshold for whom to trust, assigning credibility and reliability to almost anyone who is comfortable using the same verbiage and demonizing modern medicine. This means that while many people have found a balance that remains very safe for their families, many others who begin as simply cautious of certain chemicals or treatments (as likely as not because their doctor didn’t/couldn’t take the time to explain it to them very well) become entrenched in increasing (and increasingly dangerous) depths of falsehood. For some, this video, with it’s emotive music and deep state conspiracy theory, will be their next step. The leaders of these movements know this and see dollar signs, potential converts, or both; and the pandemic is a golden opportunity for them because we are all looking for answers. I’ve seen the fallout from this on the individual level in my own experiences caring for adults and children, and on a larger scale with measles and pertussis outbreaks that were totally avoidable. My fear is that, with something as dangerous as COVID-19, the suffering that occurs for the people believing these conspiracies could be the worst and most widespread yet.
Just past the ten minute mark, we finally get into a discussion of COVID-19.
Do you think this virus came from a lab? (10:21)
Dr. Mikovits is making claims that come off as extremely authoritative, but which nobody actually knows the answers to. Labs that have sequenced the genome of SARS-CoV-2 have said it appears to be a naturally occurring virus strain, but the idea of zoonotic transmission from meat sold in an open air market in Wuhan has seemed extremely speculative from the beginning. BBC has a good article discussing the difficulties in sorting through the origins of the virus. As a Physician my main concern is with the viral syndrome that it causes, not where it came from; but the idea of it being involved in any way with a research lab is extremely appealing to conspiracy theorists that would like this to be a Dr. Evil style attempt to conquer mankind.
But look what Dr. Mikovits is actually saying here; she doesn’t think this is a bioterrorism weapon that was designed or engineered, but that doesn’t matter because “You can’t say naturally occurring if it came by way of a laboratory.” Um… Why not? A few moments later she says ‘studied in a laboratory’ like it’s damning evidence. But the thing is… laboratories are exactly where you study things. She’s done a fair bit of it herself in the past. I spent a Summer studying Passalidae Beetles in a laboratory and they are pretty naturally occurring.

What they are saying here, really, is that the origin of the virus doesn’t matter for their purposes; whether it had been engineered as a weapon, whether it was accidentally released from a lab, or whether it just happened to be transmitted from an animal that was being studied in a lab. What matters is the word “laboratory”, because with the degree of fear and paranoia about scientific processes already experienced by many of their target audience, combined with anxiety about the pandemic, that is enough to score points as one more piece of evidence of a global conspiracy.
Finally, at the end of this section Dr. Mikovits claims that SARS-CoV-2 must have undergone “accelerated viral evolution” because if it were naturally occurring, it would take 800 years to develop from SARS. First of all, that’s a pretty specific time frame without any further explanation, so I’m going to call ‘citation needed’ on this one. But the biggest problem with that claim is… Nobody thinks it evolved from SARS in the first place. There are a lot of Coronavirus species, and we don’t yet know (and may never know) the evolutionary history of this dangerous, novel virus. It is called ‘SARS-CoV-2’ because it is a Coronavirus (CoV) that causes Severe Acute Respiratory Syndrome (SARS), and it is the 2nd one identified that does this (because MERS is the Rodney Dangerfield of Coronaviruses; it gets no respect).

Ebola couldn’t infect humans until Dr. Mikovits taught it to in 1999. (12:04)
The first major known outbreaks of Ebola occurred in 1976, 23 years before Dr. Mikovits taught it how to infect humans. So this is pretty nonsensical. The CDC has a good article on the history of Ebola Virus, but I suppose if you have chosen to believe the claims in this video you will probably see this as propaganda? The conspiracy theorist world is a much more interesting world, when even fairly blandly written (though quite interesting, to me at least) and well hidden disease history pages on government websites are all deliberate and carefully crafted deceptions.
But if course, she’s not talking about Ebola virus here, not really; the implication of the video is that somebody had to teach the COVID-19 virus how to infect humans. Add this to the list of claims in the video that have zero empirical support, but that devotees will come away 100% believing.
The COVID-19 death toll is inflated (12:22)
The tabulating of deaths from COVID-19 has been written about time and again. I wrote about it here a month ago when these conspiracy theories about doctors faking death certificates and being told to call everything COVID-19 were already being circulated. It’s been debunked thoroughly and frequently, and our best guess is that the actual death toll has actually been underestimated. We’ll do a little more debunking here, yes, but honestly it’s getting a bit old.
But the first thing I want to point out is how this video, as a smorgasbord of COVID-19 conspiracy theories, ends up mixing it’s message and contradicting itself time and again. We just spent several minutes focusing on their belief that the virus was created in a lab, that it was intentionally taught to infect human cells, and that it is part of a government plan (I mean, that’s the name of the video, PlanDemic), and now we are talking about how it really isn’t that dangerous. This video would like to have its virus and eat it too; it wants the numbers to be inflated, but it also wants the deadly disease to be an evil plot. Now, you could come up with some scenario that fits both conspiracy theories; the virus was released by Scientists (the minions of Big Pharma) but wasn’t as deadly as they had hoped, so they have had Physicians (the other minions of Big Pharma) inflate the death numbers. Sure, if you add enough layers to your conspiracy theory you can account for apparently contradictory sub-plots; but you also have to involve more and more willing participants in the conspiracy, and at some point you have many millions of people colluding in order to… what? Get some people to take a vaccine? Credulity can only be stretched so far.
The other thing you need to recognize is that Dr. Mikovits is about to step firmly outside of her training and experience, which has nothing to do with clinical medicine. When she speaks about discerning the cause of death, the interaction of chronic diseases with acute infections, and the realities faced by doctors fighting this horrible virus, she is speaking entirely as a layperson.
COPD deaths are being counted as COVID-19 deaths?! (12:49)
- I am sorry her husband has COPD. That really stinks.
- COPD (Chronic Obstructive Pulmonary Disease) and Pulmonary Fibrosis are different types of lung damage (maybe her husband has both, which is absolutely possible)…
- …and neither looks like SARS.
“But he has no evidence of infection”. Well, that’s a really wonderful thing; it’s also an important point on the natural history of COPD. Most COPD patients do not have thickened mucous, extreme shortness of breath, severe dyspnea, and prominent wheezing all the time. When those symptoms occur we call it a COPD Acute Exacerbation. And when you have an exacerbation, it absolutely is a sign of something acute happening, usually a viral or bacterial infection.
(13:10) No they absolutely wouldn’t. If he walked in with no evidence of infection, he shouldn’t be walking in at all; the ER is a dangerous place for him now more than ever. But if he comes in with acute worsening of his pulmonary symptoms, the worst COPD exacerbation he has had in his life, requiring high levels of oxygen and even intubation and ventilator support, with exposures to the COVID-19 virus or symptoms consistent with the disease in an endemic area, are you really saying that politically motivated incredulity about the virus’s infectivity and lethality trumps the doctor’s diagnostic skills? The thing they have been working their entire lives to develop?
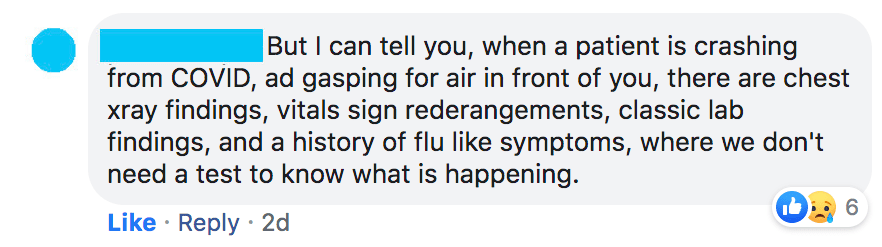
The Doctors are telling us the numbers are inflated. (13:15)
I know hundreds of doctors personally, maybe thousands, and have read or heard from even more. Some of them work in the front lines in places like New York that have been hit hardest (so far) by the pandemic. Throughout this crisis I have reconnected with classmates and friends I hadn’t talked to in years to touch base on how this whole thing is going for them, how they are holding up. None of us are being told to fudge numbers. Even if we were being told to, we wouldn’t. There are over a million doctors in the USA and I am convinced that almost every single one of them would blow the whistle and be on youtube tomorrow if the government was asking them to artificially inflate numbers or lie on death certs. This is ridiculous.
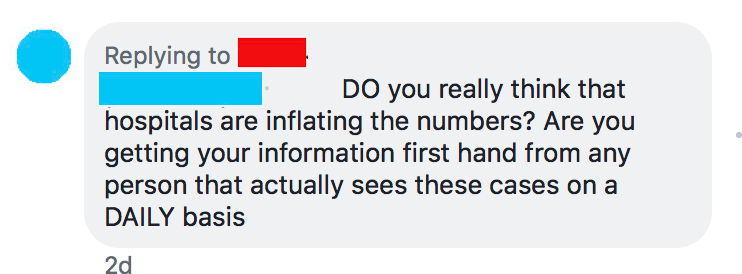
But more to the point, the guidance that has come from the CDC has actually been really reasonable. Even the images shown in the video, which are supposed to be some sort of damning evidence, are reasonable:
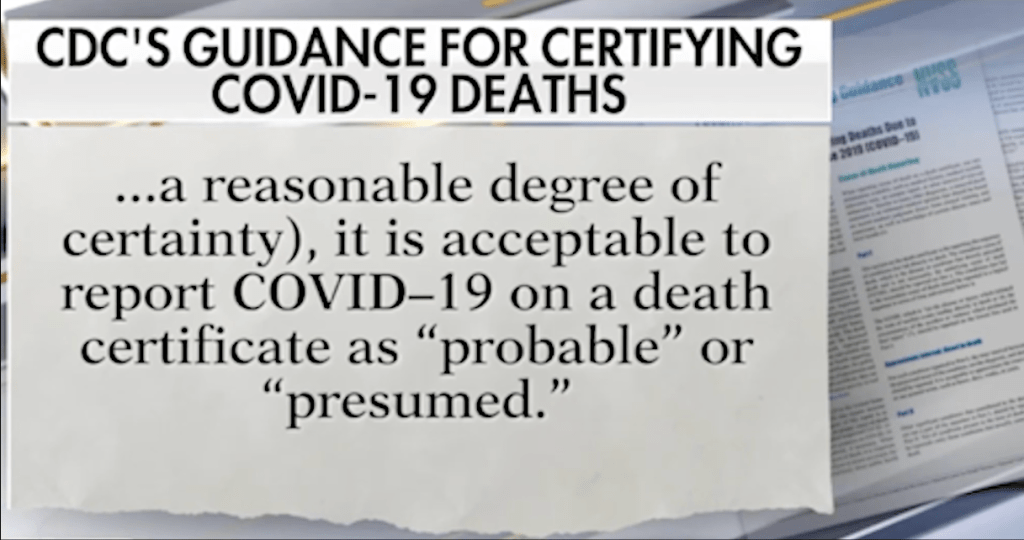
What this is saying is that if it walks like a duck and quacks like a duck, but the COVID-19 test is negative or not available, it’s still reasonable for a Physician to rely on their clinical judgement to determine the diagnosis. This is the opposite of a top-down mandate, and more to the point, it’s already how we practice medicine anyway. If you have a sore throat, fever, red and swollen tonsils, and your son had strep, I don’t test you for strep throat, I treat you for it; you have it, regardless of what the test says. And that test has a much higher degree of reliability than the SARS-CoV-2 antigen test. If you have symptoms of the flu, and it’s flu season, I only test if it would actually help me make a treatment decision, which is fairly rare; the sensitivity of the test is only 50% to 70%, which means that up to half the time you have the flu your test is going to be negative. It’s too early to know exactly what the sensitivity of the COVID-19 test is, but early reports said somewhere around 70%; so doctors very wisely chose not to defer their clinical decision making to a test result.
Finally, there’s the case the doctor in the video discusses around the 13:40 mark: the 86 year old patient who dies from pneumonia, who wasn’t tested for COVID–19, but her son later tested positive for the virus. The doctor asks, incredulously, whether it would be reasonable to list COVID-19 as a possible cause of death?
Every practicing clinician: Um, yeah, it would. In fact, these are the exact people we know are most susceptible to the virus, and the ones we are working our butts off to protect. Most of my 86 year old patients treat me like a grandson; we are treating this virus like it can kill them because it can.
13:50: Dr. Erickson owns Urgent Care Centers in a low-prevalence country in California. He is not being pressured to write COVID-19 on anything, and if he’s writing death certificates with any degree of frequency that is a big, big problem. He would like this pandemic to be not that big of a deal just like the rest of us, only in his case, it’s at least partially because his Urgent Care business is suffering right now. (Update: He has also released a statement saying he has no association with the PlanDemic video).
“You don’t die with an infection, you die from an infection.” (14:38)
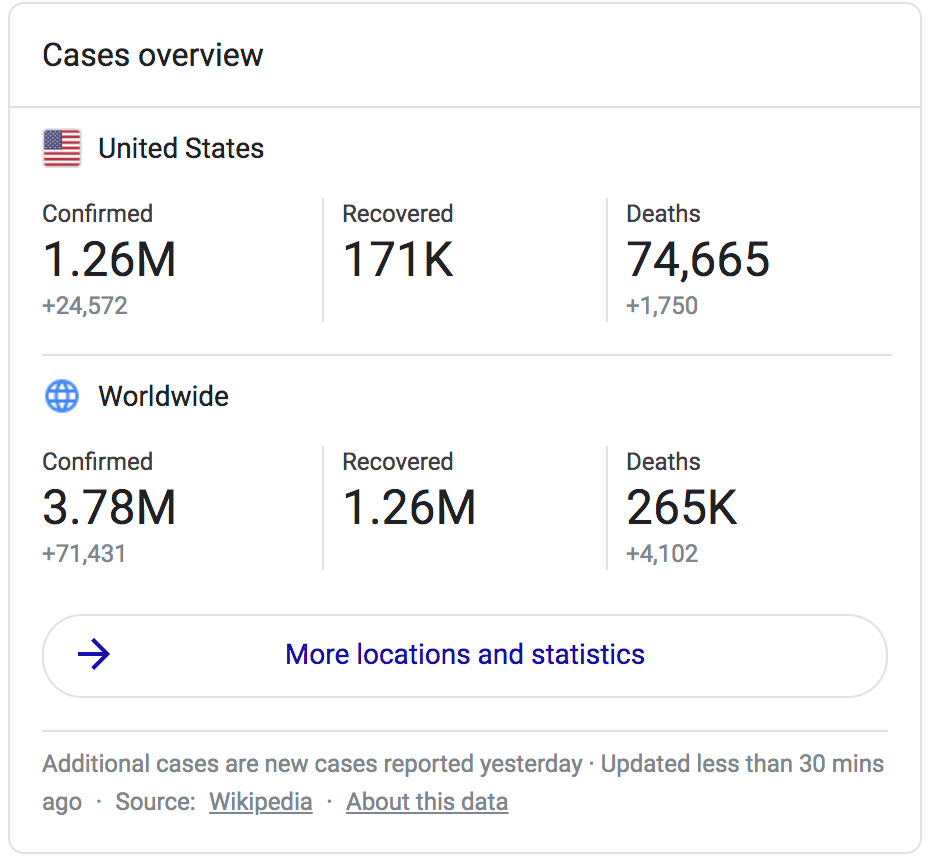
While this is not technically true (people die with infections all the time. You can get hit by a bus on the way back from your abscess drainage), I actually completely agree with Dr. Mikovits here. This is the inverse of the common saying for Prostate Cancer, “most people die with prostate cancer, not from prostate cancer.” It’s a common form of cancer that grows slowly and often near the end of life; most people with it will die from something else. Contrast this to COVID-19, which is an incredibly dangerous virus that has killed 75,000 people as of today in the US alone, and even if you don’t believe those numbers has overwhelmed healthcare infrastructures, exhausted doctors and nurses (and driven some to take their own lives), and decimated entire countries. This is a dangerous virus. It increases risk of blood clots, it seems to be causing strokes, it shuts down the lungs; the idea that people are suddenly dying in large numbers from these types of syndromes and their having the virus is just a coincidence is insane. You die from the virus; not with it.
The numbers have to match the real-life narratives, but by avoiding any discussion of the experiences of doctors, nurses, patients, and families that have been affected by the virus, the misinformation promoters hope to bypass your compassion and even your sense of rational self-preservation and deeply ingrain the idea that the virus isn’t dangerous with fake numbers and false dichotomies between acute infection and chronic disease. If they are successful, then you will be automatically suspicious of any images, narratives, or personal accounts you hear that paint a picture of a deadly virus causing real human suffering. The word ‘trauma actors’ is not far off. Don’t let them rob you of your empathy for their own personal gain.
Doctors are being incentivized to list COVID-19 (14:44)
Check-out this article from PolitiFact that covers this question in some detail. Yes, part of the CARES act was to provide a 20% stipend for treatment of COVID-19 cases. This is being done because hospitals that are hardest hit by the pandemic are also the ones that are going to have trouble staying afloat; they will be cancelling elective cases and other more profitable treatments for longer and focusing entirely on COVID-19, often in the midst of needing to pay nurses and doctors overtime, hire outside help, and wildly exceed their budgets for PPE and supplies. Now, we can talk about whether or not I think hospitals being for-profit is a good model in the first place (hint: I don’t), but the idea that a bipartisan government stimulus for hospitals in the hardest hit epicenters of the pandemic automatically equals corruption and conspiracy is awfully flimsy.
But more importantly, I want you to watch the way the video, with it’s excellent background music and high production standards, weaves this part of the narrative. Go back and watch the 15 seconds from 15:00 to 15:15 and notice the way that the words “you’ll get paid $13,000” and “if that COVID-19 patient goes on a ventilator you’ll get $39,000” are overlaid against medical professionals, in PPE, treating patients in the ICU. Look at all of these doctors just waiting to cash their $39,000 checks from medicare, the video is telling you. The reality is that decisions about diagnosis and decisions about treatment are made by Physicians, who are not paid $13,000 for a certain diagnosis or $39,000 for initiating life-saving treatment. Depending on the way their compensation agreement is structured, they may or may not see any of that additional money (I certainly won’t should we get hit hard here in Waco and I have to admit COVID-19 patients or intubate the critically ill).
Also listen to Mikki Willis’s statement right at the beginning of the segment; “I’ve spoken with doctors who have admitted that they are being incentivized…” This is the verbal equivalent of the above cinematography trick, and is the type of sentence you can utter with impunity because there are so many doctors it would be impossible to prove he hadn’t talked with doctors who said this. But notice how doctors are only a reliable source of truth telling if they are blowing the whistle on some big conspiracy, and not when they are saying, en masse, ‘this virus is dangerous. we are doing the best we can to take care of patients but please stay home. there’s no conspiracy here, just a really, really bad bug.”
The ventilators are what’s killing patients! (15:15)
I’d like you to understand that Dr. Mikovits, who is a PhD virologist and not a medical doctor, is here repeating what she has heard or read and is not speaking as an expert by any means. I’ve had a friend write to me extensively about how dangerous ventilators are. I’ve seen videos and articles and facebook posts saying “88% of people who go on ventilators die”, as though that were proof that ventilators were dangerous, instead of that the virus is dangerous. (here is an article working through those ventilator numbers, by the way). You see, we only intubate the sickest patients, so they already have the highest chance of dying. There’s a confounding variable, and it’s called severe respiratory distress.
Now, I do think there is a discussion to be had here in terms of the best use of our ventilators. The myth here seems to be, as best as I can understand it, that “ventilators” are a discrete treatment the way “ibuprofen” or “knee injections” are discrete treatments; either you do a knee injection or you don’t (ok that’s also not accurate), either you give ibuprofen or you don’t. But ventilators are incredibly complex tools and their use is not monolithic. Here is a very basic but extremely helpful (at least to someone like me who doesn’t use a ventilator on a daily basis) guide to vent strategies from some people I admire over at EmCrit. Did you read it? You got all of that? This is the tip of the iceberg. Even the clip that PlanDemic shows at 15:18 is an ER doctor from New York early in the course of the pandemic arguing for a different ventilator strategy, not against the use of ventilators. His name is Dr. Cameron Kyle-Sidell, and he goes on to say:
“Now, I don’t know the final answer to this disease. I do sense that we will have to use ventilators. We’ll have to use a great number of ventilators, and we need a great number of ventilators, but I sense that we can use them in a much safer way, in a much safer method.“
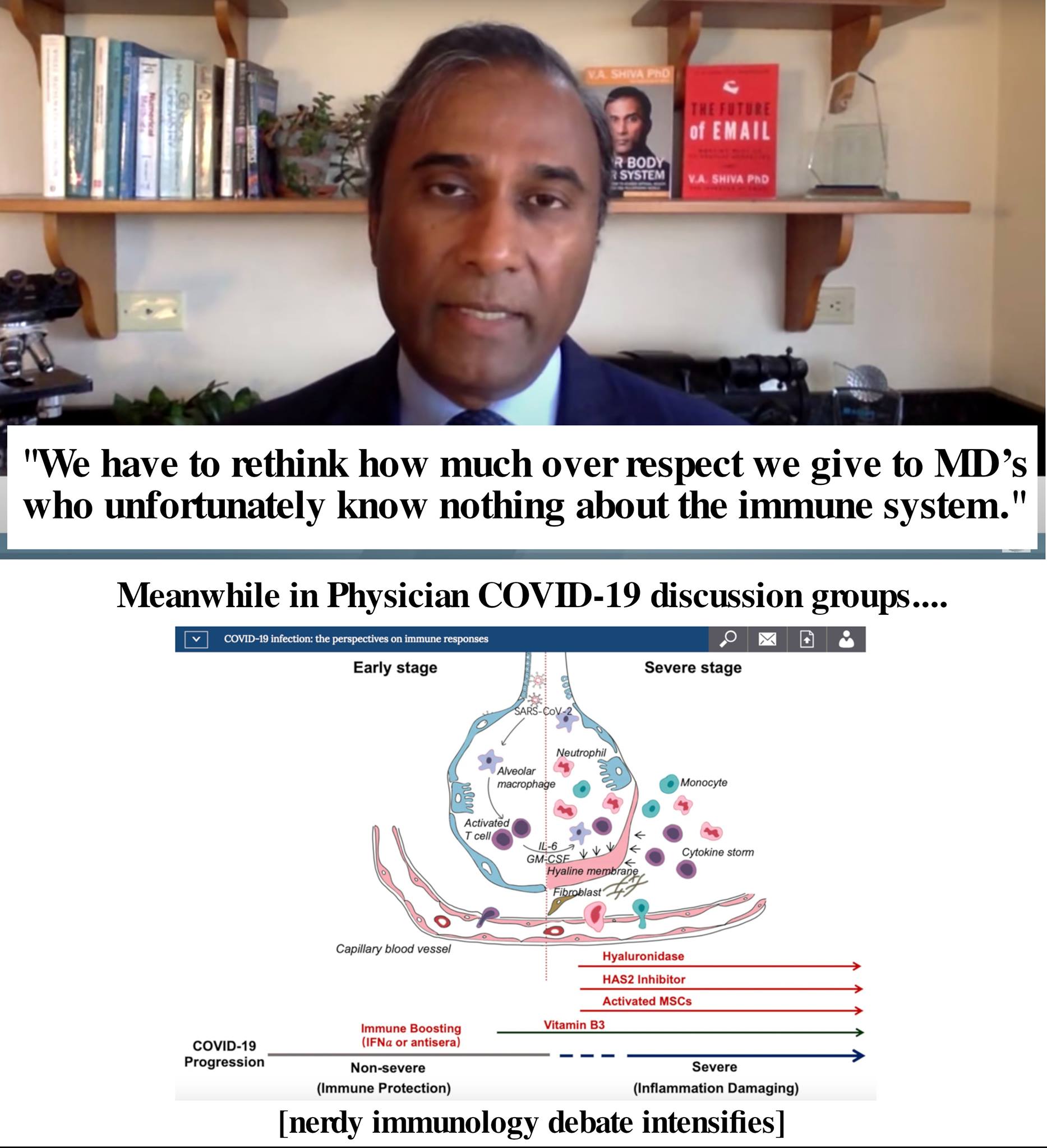
So they’ve shown this clip to make you think, doctors are using ventilators because they get paid more money, even though it kills people, but a few doctors like this one are speaking out against this corruption. The real narrative behind this clip is a lot more reasonable and a lot more hopeful, and it’s this: doctors are trying to fight this new virus with the best tools they have, and impassioned discussions and debates about how to use those tools well are already happening. I am a part of a number of Physician COVID-19 groups on facebook, and both there and in private conversations and discussions within my own clinic system, every aspect of when and how to use ventilators to support COVID-19 patients is being dissected and discussed. It’s a good thing that we know more than we did a month ago, and the more we can delay the spread of this virus, the more we will know when it finally hits your area.
But let me make one thing abundantly clear; this is not a choice between using a ventilator and making more money, and not using one so the patient can get better; that is a false narrative and, frankly, on the grossly cynical side even for the conspiracy theory people. When you intubate a severely hypoxic patient, having tried everything else you know of to keep them off the ventilator, your decision is to use a ventilator or watch them slowly die gasping for air. Unless you’ve been in that situation, your theories on doctors putting patients on ventilators because they were told to or are thinking about their next paycheck don’t carry much weight with me.
And let me just state, for the record, that if you suspect a doctor at your hospital is putting people on ventilators or doing any procedure in order to make more money, you should report that person right away. That’s what I did the one time in my education or career I thought I had seen it happen. And if you believe it’s happening on a large scale, that doctors all over the country are doing it, please start thinking now about what you will do when your child or loved one becomes terribly ill at some point in your life, because if you have that little faith in the good intentions and integrity and medical knowledge of doctors and nurses, I cannot imagine why you would ever come to a hospital (though I honestly hope you do, because I believe we’d have the best chance of helping them, even if you don’t right now).
What about Italy? (15:35)
I just want to say that as little as I’ve found in this video to agree with, I really respect even the willingness to address the parts of the Pandemic that simply can’t fit it into their narratives (ok, I’ve actually found nothing to agree with; but there is at least plenty I can’t comment on. For instance, I can’t say whether or not someone planted evidence in her house before she was arrested).
When the Bakersfield Doctors, misled by their shoddy statistics, concluded that the virus wasn’t at all dangerous, they simply hand-waved New York and Italy as ‘hotbeds’ and moved along; it didn’t fit their narrative and so they didn’t even make a show of trying to explain how a non-dangerous virus could cause such catastrophic damage. The narrative here is infinitely more interesting.
Reason #1 is good; Dr. Mikovits says that Italy “has an older population, and they are very sick with inflammatory disorders.” Now, I don’t have any data on whether Italy has a higher rate of autoimmune disease, which I believe is what she means by inflammatory disorders; but I think we can accept the idea that older populations with more chronic illnesses are going to be at higher risk for complications, including death, from COVID-19. That is very consistent with the data we have seen throughout the pandemic. I would also point out that Italy is not alone in having an older population; many US States have similar demographics. 22.8% of Italy’s population is older than 65; but so is 20.6% of Maine, 20.5% of Florida, and 19.9% of West Virginia. If Italy can experience a surge of cases bad enough to overwhelm their healthcare infrastructure, there is nothing to prevent it from happening here. And of course, age isn’t the only factor; it has happened in New York, and only 16.4% of their population is greater than 65 years old. But the point is, saying ‘Italy is old’ doesn’t explain how a non-dangerous virus can kill so many.
But at 15:47 she loses me. Her claim is that in 2019 Italy had a new, “untested” form of Flu vaccine, and that this explains Italy’s high COVID-19 burden. She says the vaccine was grown in a dog cell line, and that ‘dogs have lots of coronaviruses.’
So, does that even make sense? Well, someone will have to tell me whether the flu vaccine used in Italy last year was new in the sense of being designed or developed differently from flu vaccines used in prior years or in other countries (in another sense, the flu vaccine is new every year because epidemiologists have to decide which flu strains to include based on which are most likely to become endemic). By the way, Italy had a particularly light flu season; so if it was new it may be a really good vaccine. However, the mechanism she is describing isn’t logical. First of all, the flu vaccine they use in Italy includes only killed viruses; your body is exposed to the antigens and can mount an immune response, but the virus cannot ‘come to life’ and cause the flu (or any other ‘inflammatory reaction’ she is hinting at here). The antigens of the dead virus are picked up by circulating white blood cells and presented to the immune system, so that the next time the body sees the virus it has the ability to rapidly produce a robust antibody response, usually before a person is even symptomatic (it does not work by creating a magic forcefield around your body that flu germs bounce off of).

But the trick is preserving the dead flu proteins without eradicating them completely. The idea that Coronaviruses have somehow come from a cell line used to develop the vaccine, have survived the process of creating the vaccine (all of the ‘harsh chemicals and toxins’ we are always hearing about), and have tagged along and actually entered the person’s body through the flu shot is nonsensical. Even if that were true (it’s not), she gives no clear mechanism by which that would have literally anything to do with COVID-19. Remember, Coronaviruses are a big, big family of viruses, and exposure to one would at worst have nothing to do with infection by another, and at best give some degree of cross-reactive humoral immunity, which sadly does not seem to be the case for COVID-19. Really, ‘dogs have lots of coronaviruses’ is little more than word association.
But the title of this article is “The Paradoxes of PlanDemic”, and here is another one. Just 5 minutes ago Dr. Mikovits told us that the COVID-19 virus, SARS-CoV-2, was created in a lab in Wuhan China, and was accelerated and manipulated in bats. So what would a flu vaccine in Italy, created in a dog cell line, have to do with COVID-19? There isn’t even a theoretical mechanism here; just the hope that by saying flu vaccine and Coronavirus close enough together in the video, their viewers will believe that the 30,000 deaths in Italy are actually another crime of the scientific community, instead of a stark warning of how bad this pandemic can become.
At this time the video has been removed from YouTube, Facebook, and Vimeo, the three sources I had used to view it while writing this post. I have mixed feelings about this. I don’t believe in censorship in general, but I also worry about allowing verifiably false propaganda to deceive millions in the name of freedom of speech, and the real human suffering that could occur if these videos were spread unchecked. I am a Physician, and it’s probably more a question for a philosopher or at least a constitutional scholar.
That said, if you do have a source for the video, feel free to send it my way via the “contact” page. Otherwise, the rest of my comments will be given without any time-stamp or specific quotes, though I have viewed the video in it’s entirety prior to now.
Hydroxychloroquine is a miracle drug, which is why they won’t let us use it.
I remember back in March (oh those carefree days, where have they gone?) when an OB/GYN I know, a friend from undergrad, first shared the French study showing promising results in COVID-19 patients treated with hydroxychloroquine, an immunomodulator we use mainly for Lupus, and azithromycin, an antibiotic (but you already knew that because they give it to you every single time you go to an urgent care…). At the time the responses of the clinicians I know ranged from cautiously hopeful to very skeptical. Hydroxychloroquine and azithromycin are not anti-viral drugs, some argued, and the study was so small that the results shouldn’t change our practice. Others argued that both medicines have some theoretical anti-viral properties, so even though they are not anti-virals per se there is at least a reasonable mechanism of action in play. For azithromycin, this involves anti-viral effects on the epithelial cells of the lungs; for hydroxychloroquine, prevention of viral entry into the cytoplasm of host cells.
Since this wasn’t a large randomized double-blind placebo controlled trial, this small article coming from France hardly constituted a gold standard of treatment; but since the medications were fairly safe and somewhat promising, and since it is the middle of a global pandemic, many doctors and hospitals began to use one or both. There were even some promising, but ultimately anecdotal results. Locally we used hydroxychloroquine but not azithromycin, generally, because of the concern that the combination of both could cause prolonged QT syndrome (which can, you know, kill you). Here is the very measured guidance from a field guide a friend sent me:

As far as I know, each hospital and Physician had to weigh this evidence for themselves. The FDA did release an emergency approval for hydroxychloroquine for COVID-19, and at no point were doctors told we weren’t allowed to use it, unless this came from their own clinics, hospitals, or medical societies; certainly I’ve never heard of any of the ‘doctors being threatened if they use hydroxychloroquine’ that they mention in the video. Unfortunately, subsequent larger and more intentionally designed trials have not shown a benefit; not to fault the French trial, they were trying to save lives and were publishing the modest but promising results they had so far, not trying to empirically prove the efficacy of the medicine. Here is an article from the New England Journal of Medicine that explains this all in greater detail, and the rationale by which the authors chose to stop using the medicine to fight COVID-19.
So that’s the story of hydroxychloroquine, and it’s hard to imagine how anyone could think there was any conspiracy behind that pretty straightforward sequence of events. Really, that’s how these things are supposed to work; if the treatment is safe and cheap and seems to help, it’s reasonable to use it while you are waiting for more reliable data. If that data then shows that the benefit just really isn’t there, you stop using it. When the president touted the drug as being promising, it was with his usual bravado but to some degree reflected the hope many of us felt about it at the time; when Dr. Fauci advised caution and stated the evidence was anecdotal, he was right, and was saying exactly what your local Physician might say at that point if she had been reading up on it. I don’t know anything about the doc yelling in the clip they showed, but unless he was actually treating COVID-19 patients and had some really excellent anecdotal results, I really can’t understand the vehemence he felt about the medicine; it hasn’t been warranted at any point by the evidence.
But before we move on, there’s one more thing I wanted to mention (and here is where I feel most keenly the loss of the video itself), and it’s that the idea of anyone in the healthcare industry actually trying to block doctors from using a medication because it is working is obscene in the highest degree. I’ve seen enough corporate espionage movies and read enough Spider-Man 2099 comics to have a healthy suspicion of the big pharmaceutical companies, but I really believe this is beyond even them. But if you wouldn’t put it past them, at least consider this; if the government or big pharma or whoever were really telling doctors they couldn’t use a medicine that the doctors knew was saving lives, how would the doctors react? Would they go along willingly, because their one and only interest is obeying their corporate masters? Would they shrug their shoulders and watch people die who they could have saved?
Would you see just that one angry doctor ranting on YouTube, or hundreds of thousands?
Wearing masks increases your risk of infection, reactivates your own COVID-19.
To me, this is the strangest claim in the entire video, and it’s hard to understand for a number of reasons. First, how in the world is asking people to wear masks a conspiracy? Many of the masks we give to patients even in our own clinic are homemade, so it can’t possibly be Big Mask trying to turn a profit. I know many people chafe under any sense of the government trying to control them; but does this actually count, asking us to wear masks in public, that we’ve either made ourselves or gotten for free at our doctor’s office, to keep ourselves and especially others from getting sick? I don’t like wearing masks much either (unless it’s for Comic-Con), but it always strikes me as a particularly troublesome part of our highly individualistic culture that we oppose on principle so much that we ought to do voluntarily the moment there is even a hint of it being mandatory, particularly acts of charity (financial and otherwise) toward our neighbors. Remember, you don’t wear a mask for yourself; you are wearing it to prevent transmission if you have SARS-CoV-2 and are asymptomatic, to keep from spreading it to others.

Of course, this demands the question of whether or not wearing these homemade masks actually is an act of charity; that is, if it really does protect our neighbors from the virus. And as easy as it would be to simply say, ‘yes, masks obviously decrease transmission of respiratory viruses by blocking droplets’, the reality is that in science, what feels right or makes sense intuitively isn’t always a reliable guide to what’s true (hence this blog). So the real answer is; yes, they probably help. LiveScience has a good summary of the most current info and recent studies. With promising but limited evidence we have to weigh the risks and benefits. Remember what we said about using hydroxychloroquine earlier; if a treatment is promising, cheap, and safe, it’s reasonable to use while waiting for more data, and the same is true about prevention strategies. In this case, while we may well get more data we will likely never have a definitive answer about the degree of benefit. What would it look like, exactly, to do a large double-blind placebo controlled trial of wearing masks?
But Dr. Webb, you said the masks are only a good idea if they are safe, and the video says they aren’t. There is a very strange claim in the video, The idea that wearing a mask is somehow dangerous. I’d be remiss if I didn’t mention that they are once again contradicting themselves, but this time in rapid fire sequence. They want at once for the masks to be bad because they keep viruses and bacteria out (they show the clip of Dr. Erickson talking about how touching your face and eyes is vital for your immune system, failing utterly to distinguish between a deadly pathogen and mere microbes), and for them to be bad because they expose you to your own microbes. This is not only poor science, it’s also poor debating. To borrow from Scott Adams (Dilbert), it’s like saying Sorry, I never got the message to call you. And when I did return the call, you didn’t answer. One excuse is better than two.
But I think what’s really going on with this claim is two things; an appeal to the deep desire we all have for a sense of normalcy, and an exploitation of the sensationalization of wearing masks. The truth is that wearing masks isn’t new, and we do it all the time anyway. I wear a mask frequently at work because it both protects my patients when I have a cough that might be infectious, and protects me from respiratory organisms. But you wear a mask too. You wear one when you have the flu and don’t want your kids to get sick; people ask me for them all the time when they are at the office. You wear them when you go snow skiing, or when you are around dust, or when you are painting or staining wood or doing projects with strong fumes, or at Halloween. I’ve never heard of anyone, health conspiracy theorist or otherwise, crying out that they were dangerous, that they reactivated your own viruses or starved your brain of oxygen. But now that it’s a matter of admitting how deadly and dangerous this virus can be for the people you are interacting with and following a reasonable recommendation from the government, all of the sudden they are part of a conspiracy, a symbol of oppression?
All of that said, there is one situation where wearing masks really is dangerous, and it’s when people treat them as though they alleviate the need for any other safety measures; as though it made them invincible from the virus. With only limited efficacy at protecting against respiratory viruses, masks are not the ultimate answer to COVID-19, and physical distancing, hand washing, and careful mitigation strategies are still vitally important. But most of us can remember to do those things while still wearing a mask.

Healing microbes in the Ocean.
I’m sorry, I’m just totally lost here guys. Maybe she means these?
COVID-19 Deaths from the day PlanDemic was released: