One thing that has become predicable throughout the SARS-CoV-2 pandemic is that any story, any recommendation, any development, or any piece of data that can be interpreted as meaning that the danger of COVID-19 has been inflated, misrepresented, or exaggerated by medical experts will be interpreted that way by a large percentage of our population. This is no longer surprising, but honestly it’s also completely understandable. We all hate this pandemic. Whether you are working on the front lines in clinic or in the trenches at the hospital treating COVID-19 every day, whether the virus has harmed or killed a friend or family member, whether your job or business has been affected, or even if you just really miss people, we are all ready for this to be over. The hard path forward involves biomedical research, redoubling mitigation efforts that we are all exhausted of, and at this point, modifying holiday plans and preparing to deal with the quagmire of cascading clinical probabilities that are required to fight the virus in the midst of cold and flu season. But the quicker and easier path to getting rid of this hated virus is undoubtedly to just choose not to believe in it at all. And while this “just don’t believe in it” approach is likely to be about as effective as it has been for any of the other problems I’ve tried it for (taxes, bills, excess carbs), I am sympathetic to the appeal of it. If the pandemic has not affected you directly- or maybe even if it has- it may be very tempting indeed to buy into a video like Plandemic, which tells you that the whole thing is just a government conspiracy, or into the America’s Frontline Doctors‘ video which tells you that there is already an easy and inexpensive cure if you just drive to the see the right doctor. Life can be normal again right now, these sources say; all of your hopes are true and all of your caution and privations can finally come to an end. I’m not saying it’s right, I’m just saying I get it.
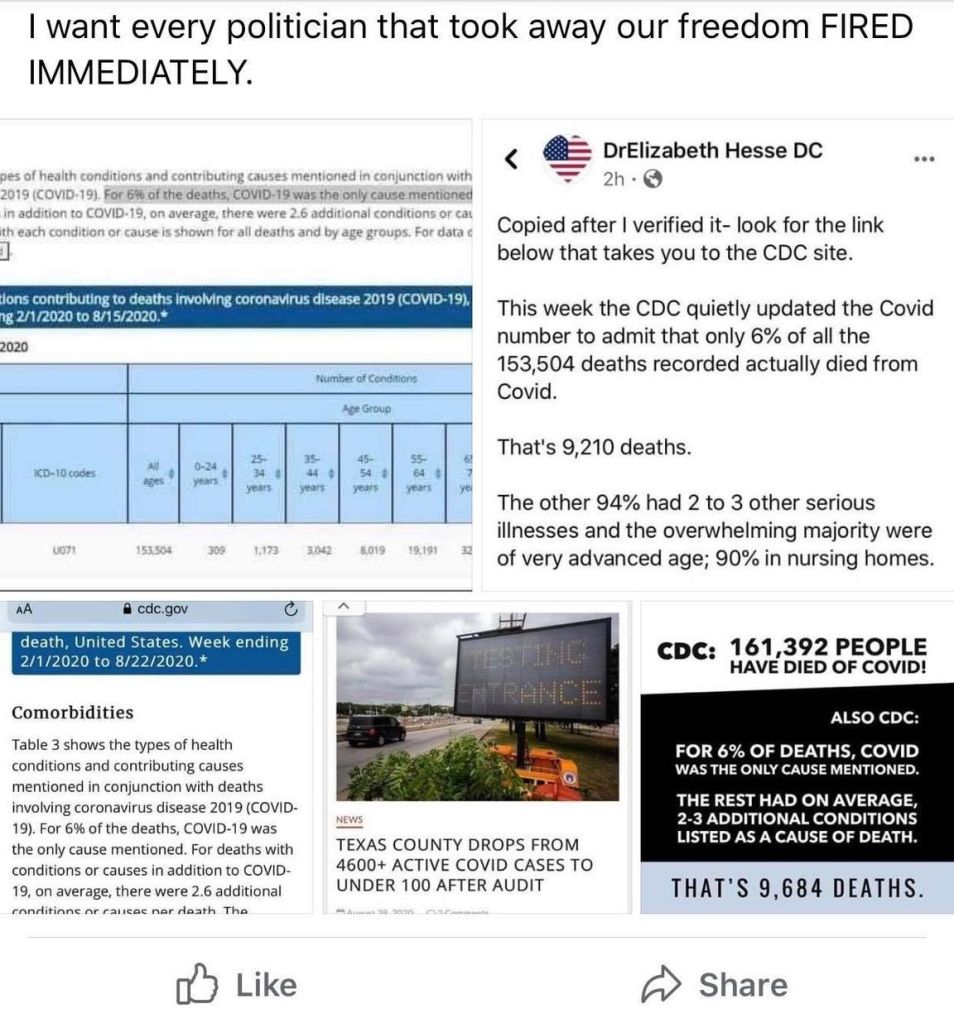
But what has been surprising- and consistently surprising, to me at least- is which wild facts people will latch onto to create these false narratives. Before today, I would never have expected this paragraph from the CDC’s weekly updates by select demographic and geographic characteristics to be the next cause of viral misinformation:

What is the claim being made?
If I chose to end this blog after today, I would feel I had really come full circle; my very first blog post was about the myth, popular late in March (and persistent even today), that doctors were lying on death certificates to make the virus seem more dangerous than it really was. Today’s myth is that analyzing the diagnostic codes on death certificates –those incorruptible sources of reliable data- reveals that the virus isn’t actually very dangerous at all, and the CDC has just admitted to it. Bypassing the irony that this later misinformation is being circulated by exactly the same people who have been sharing the first for months, we can spend today’s blog post (48 hours late as usual, this time because our internet was out all day yesterday!) analyzing these claims. They seem to have taken two forms.
The first, and more moderate, is to claim (or at least strongly imply) that because 94% of deaths from COVID-19 also had other diagnostic codes listed on the death certificate, it means that people without ‘underlying medical conditions’ are not actually at a very high risk of dying from the virus. And in one sense this is true, even if this new data from the CDC doesn’t actually really have anything to do with that. Your Local Epidemiologist says this better and more succinctly than I can:

And she’s absolutely right; we have been saying this from early in the pandemic. But not just saying it; thinking it and believing it, too. Every decision I make as a physician, from admitting someone for COVID-19 to starting or stopping a medication, referring them to a specialist, or even recommending exercise or lifestyle changes has to take into account their medical history (and a host of other factors). While there are some symptoms we can warn everyone about, the counseling and support we provide for patients seeking evaluation and treatment of COVID-19 has a lot to do with their individual risks from the virus and how it might manifest in their lives based on their age and other medical conditions. This 6% misinformation became viral just yesterday, yet if you asked any doctor last week they would have already told you that the younger and healthier you are the less likely you are to end up in the hospital or die from COVID-19, and the more medical complications you have the more concerned they are about you having the virus. I know because this is exactly what I was saying to people in clinic last week, and the week before that, and the week before that. Yes, many young and otherwise healthy people have died tragically and shockingly from complications of the virus; but this is still a rare occurrence on the whole compared to the number of young, healthy people who have had the virus. When I counsel people at low risk of complications from COVID-19, we of course talk about the signs and symptoms they should watch for that would trigger a trip to the ER, like chest pain and shortness of breath; but I also want to make sure they aren’t sitting at home, anxiously wondering when the virus is ‘going to get them’. I want them self-isolating; I don’t want them to be afraid. But this relative reassurance towards the young and healthy is actually undercut ever so slightly when you combine headlines like these with the actual data being reported from the CDC, which I’ve included below.
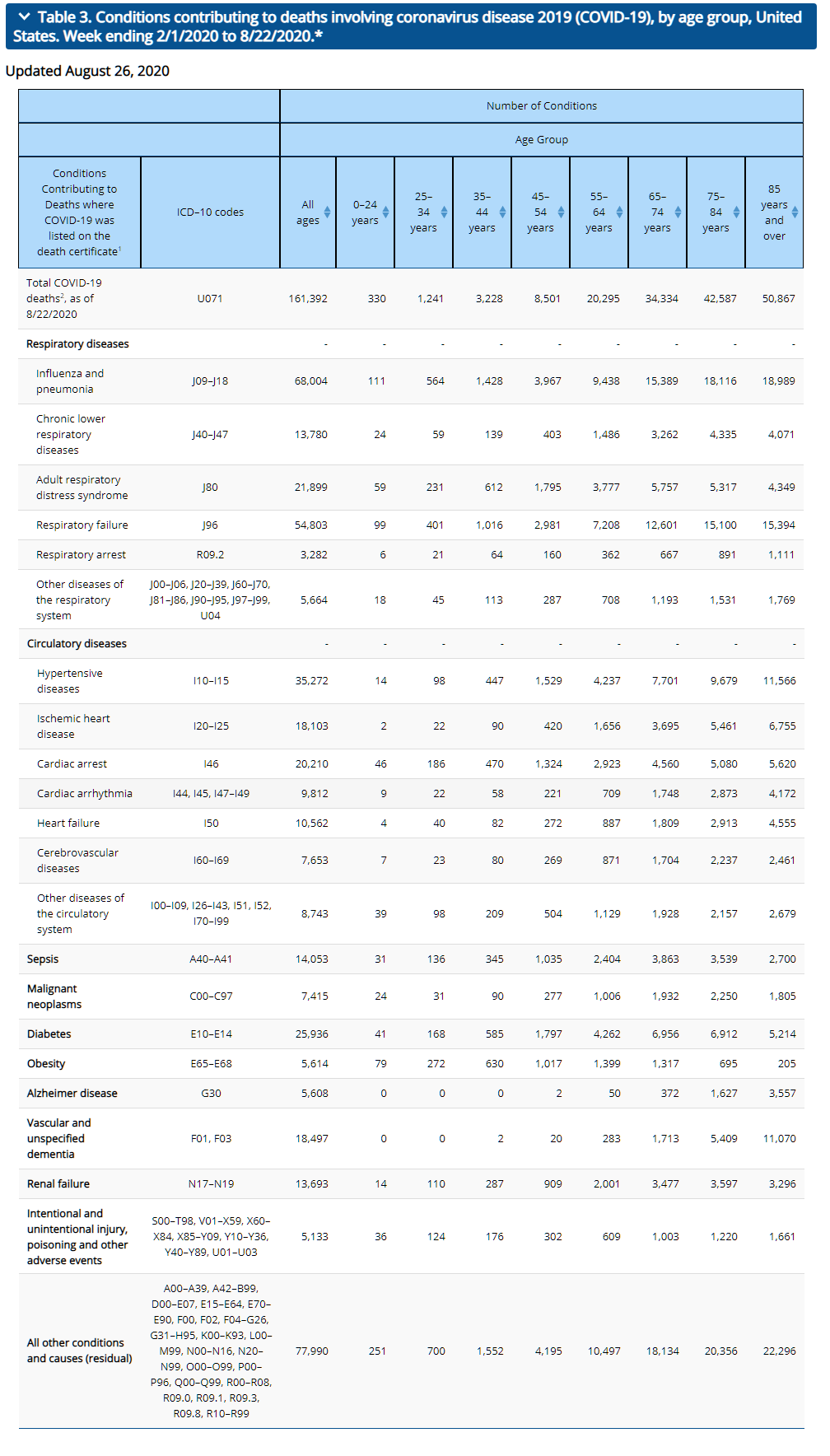
When you look at the other diagnostic codes listed in the table above, you will notice that codes like E78.2 and I10 are listed; high cholesterol and high blood pressure, respectively, both conditions I’ve been diagnosed with in the past (and probably still have, if I would ever go get a check-up. Doctors really do make the worst patients). At 35 and having never spent a night in the hospital as a patient in my life, nobody would call me high risk for complications of COVID-19. In fact, if I contracted COVID-19 and died of it this week, two things would happen. First, my blog would probably get a lot more hits for a couple of days (and this paragraph in particular would seem very bitterly ironic). But second, I would be held up as an example of how being young and in relatively good health is not a perfect guarantee of safety from the virus. Yet I would be a part of the 94%, not the 6%.
The reality is that in saying “94% of COVID-19 deaths had underlying conditions,” these stories are adding nothing to and are in fact dumbing down the more sophisticated knowledge we already have, and share with our patients daily, of the most important risk factors and conditions that predispose someone to COVID-19 being a likely threat to them. They are meant to lure you into a false sense of security, because it’s so easy to think they mean somebody else besides you (even if you do in fact have some of those diagnoses, like I do) and a relatively small group of people. But when I look at the chart, I realize that even I fall into that group with “2 or 3 underlying medical conditions” that they are saying 94% of the COVID-19 deaths occurred in; in fact, most Americans do. And when a statistic includes me, privileged to be in pretty good health as I am, but also my patient battling metastatic kidney cancer and my patient suffering from both CHF and COPD, maybe it just isn’t a very useful statistic in the first place.
But the more dishonest and blatantly ridiculous claim, which has absolutely no justification, is to say that only the 6% of deaths with just COVID-19 listed on the death certificate actually count as COVID-19 deaths. Take this one Facebook poster who has been widely shared, who had the gall to take this to the next step and “calculate” that only 9,210 people had “actually died from Covid.” Probably because she was willing to put a number on the deaths, this post has been shared 21,000 times on Facebook; but it’s hard to believe that someone with a doctorate degree, any doctorate degree, could have such little grasp on basic statistics.
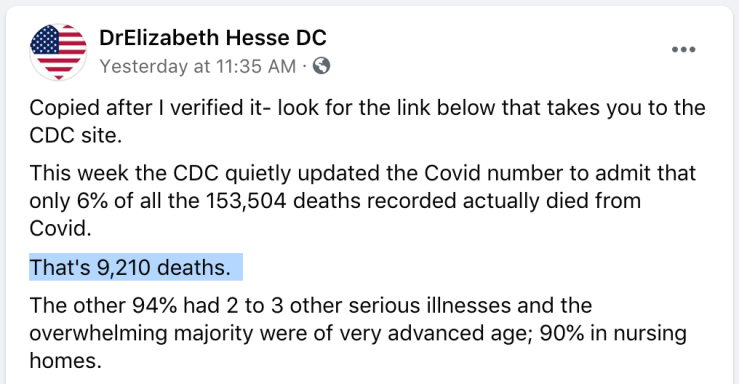
This post entirely misrepresents everything within our complex understanding of medicine regarding the impact of medical comorbidities, the myriad causes and steps leading to death in COVID-19 or any other illness, and even the very process of completing a death certificate. In her estimation, Dr. Hesse is saying that a diagnostic code on the death certificate other than COVID-19, literally any other code, is sufficient evidence that the patient did not die from COVID-19. This is not only preposterous and dishonest but also just plain silly. We are going to explore these issues more thoroughly in the next section, but briefly, just look at the chart above and begin googling ICD-10 diagnostic codes for yourself to test the logic of her interpretation. Yes, I can absolutely believe that some of the patients whose death certificates reflect both COVID-19 and also diagnosis code C71, Malignant neoplasm of brain, may actually have died from the brain cancer and were only found to have the virus incidentally. We can’t tell from the data if that did in fact happen, or how many patients might have such a presentation. But with COVID-19 being an acute illness and brain cancer being a chronic illness, the disease and treatment of which also predisposes you to infectious illnesses, it is at least as reasonable to assume that the majority of patients who died from “COVID-19 and brain cancer” actually died from COVID-19, which they were more vulnerable to because of their pre-existing brain cancer.
But Dr. Hesse’s assertion that only the 9,210 “COVID-19 only” deaths should count also has to stand up to scenarios like, say, any hypothetical patient who was certified as dying with COVID-19 and R09.3, Abnormal sputum, or COVID-19 and N20.0, Kidney stones. Again, we can’t tell from this data whether any such patients with only those codes exists; but neither can Dr. Hesse, and for her argument to be valid, each and every possible diagnostic code included in the chart above would, if added to a COVID-19 death certificate, nullify COVID-19 as a primary or contributing cause of death. That is what she is saying, and it is obviously ridiculous. What this error betrays is a complete misunderstanding, whether intentional or accidental I know not, of how death certificates are completed and the information they are meant to capture. Even though it means a longer essay, I do think it’s worth taking the time to revisit this again.
What information do we include in a death certificate?
Once you have been trained to complete death certificates (and have actually done it), this “6%” argument is not even momentarily tempting or convincing. I know what you are thinking; “but TJ, we haven’t been trained to complete death certificates, so you are asking us to trust you with this area of specialized knowledge we don’t have access to.” Well good news reader, the Texas Department of Health and Human Services, DSHS, has got you covered. If you want to understand this 6% statistic from the CDC, I highly recommend that you watch from 1:44 to 3:08 of this video.
Also, that was a joke.
Obviously each state will have its own version of this software, but they are all intended to convey the same information; the death certificate is not a high-stakes multiple choice interrogation asking the doctor, “What disease caused the patient’s death? Was it COVID-19 or heart failure? ANSWER THE QUESTION!” Rather it is an opportunity to distill the sequence of events leading to the patient’s death, recorded in greater detail in the medical record, into a structured narrative that explains how they died. When a doctor includes coronary artery disease on the death certificate, they are not making a political statement or a value judgement, but rather an honest reflection of the part this disease played in the patient’s death based on their medical knowledge and their intimate understanding of the progression of illness as the patient’s treating physician. And it is exactly the same with COVID-19. Moreover, this is not something that the physician derives a financial benefit from or an opportunity to defend the medical care the patient received (in fact, I have listed iatrogenic injury on the death certificate when I felt that my own mistake or that of another medical professional contributed in some way to the death of the patient), but rather something that is important for public health information and, in various ways, important to the family of the deceased.
Briefly, I’d like us to complete a medical certification for a death certificate together, again using my hypothetical death from COVID-19 as an example. In this scenario, let’s say that I get sick with cough and loss of taste and smell this week and am diagnosed with COVID-19. Around day 10 of my symptoms I begin to experience chest pain and shortness of breath, and I go to the ER. There I am found to be hypoxic and my chest x-ray shows bilateral peripheral consolidation consistent with ARDS. they begin to treat me with dexamethasone, remdesivir, and oxygen. Over the next few days my respiratory distress increases and, even allowing some permissive hypoxia in order to avoid intubation, the doctors simply cannot keep my oxygen level within safe parameters; they make the difficult decision to intubate me and put me on a ventilator. I am ventilated in prone positioning using the latest and best evidence-based ARDS/COVID-19 ventilation strategies from the genius doctors over at EmCrit and PulmCrit. Unfortunately, I continue to become progressively, severely hypoxic, and eventually suffer cardiopulmonary arrest. Resuscitation is attempted but ultimately efforts to revive me prove futile; the lungs are not compliant, effective ventilation still cannot be achieved, and return of spontaneous circulation is impossible. I’d make a joke about making the life insurance check out to my wife, etc. at this point, but honestly when I reflect on how many people have died from this sequence of events over the past six months, it’s pretty sobering. I’ve made myself sad just now thinking about all of the families that have lost a mother, father, sibling or grandparent in exactly this way.
Once I’ve died, the doctor treating me will have to record it in a death certificate; we can use the Texas system, since it’s what I’m familiar with.
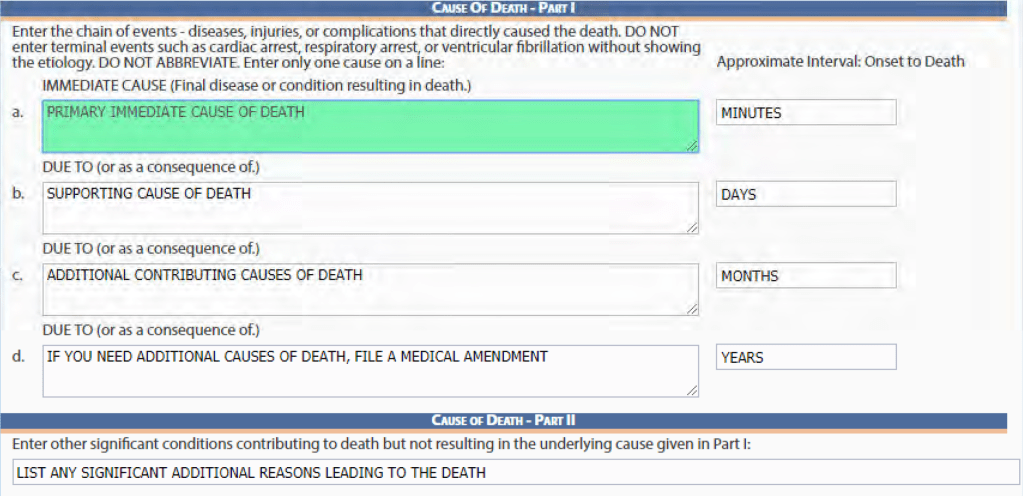
Here in Part I we list the immediate cause of death. In my case, it’s going to be cardiac arrest. Because this is technically the immediate cause of death in every death except those caused by brain death, some doctors would leave this out. Since resuscitation efforts were made and the arrest was a distinct medical event, I would probably include it, but an argument could be made either way. Next we need to describe the events that led to this. I’m not going to include respiratory arrest because I would feel it was a bit redundant, and besides, I was already not breathing on my own when the cardiac arrest happened since I was on a ventilator. Instead, I would say the arrest was due to respiratory failure. The respiratory failure was due to ARDS, Adult Respiratory Distress Syndrome, and you could make a case here for including viral pneumonia as well. Finally, the ultimate cause of this cascade of complications is my infection with COVID-19.
Next I would need to list any other contributing factors in Part II, and here is where the quandary usually comes in, because now I have to decide whether my high blood pressure and high cholesterol belongs in Part II, “other significant conditions contributing to death but not resulting in the underlying cause,” or in Part I further down in the chain of events. In this case it’s easy; my high blood pressure is a significant medical issue and made me at higher risk from the virus, so it belongs in Part II; but it didn’t cause me to get COVID-19, so it doesn’t belong in Part I. My chronic right shoulder pain didn’t contribute at all and gets left off the death certificate. These decisions aren’t always easy; sometimes a condition did lead directly to death in chain of events that are causative narratively even if not pathophysiologically; for instance a patient who is hospitalized for a hip fracture and then develops sepsis from a central line. The hip fracture didn’t cause the infection that kill them, but it was a direct part of chain of events. But what about the vertigo that caused the fall that caused the hip fracture; does that belong in Part I or Part II? I have a physician friend who works in hospice care who completes death certificates almost every day (I have completed maybe a dozen); he says this is typically the hardest decision point when it comes to completing a death certificate, deciding what was really a cause and what was ‘only’ a contributing factor. Still, it’s straight forward enough in my hypothetical case, and we can finalize my death certificate as follows:
Cause of Death – Part I:
IMMEDIATE CAUSE
a. Cardiac Arrest.
DUE TO
b. Respiratory Failure.
DUE TO
c. Adult Respiratory Distress Syndrome.
DUE TO
d. COVID-19.
Cause of Death – Part II
-Hypertension, Hyperlipidemia
So, for young, relatively healthy me who died from the most stereotyped and straightforward case of severe COVID-19 I can conceive of, we have 5 other diagnostic codes listed on the death certificate between direct cause conditions and contributing conditions. Contrast that to what a Texas death certification with only the diagnostic code for COVID-19 -the only types of death certificates Dr. Hesse believes count as COVID-19 deaths- would have to look like:
Cause of Death – Part I:
IMMEDIATE CAUSE
a. COVID-19
DUE TO
b. ________________________
DUE TO
c. ________________________
DUE TO
d. ________________________
Cause of Death – Part II
________________________
My friend, the hospice doctor, has completed over 500 death certificates (a conservative estimate) since finishing residency a few years ago. He says he has included just one diagnostic code alone maybe twice. What Dr. Hesse sees as the ‘real’ COVID-19 deaths, these 9,210 death certificates without any other documented diagnoses, I see as an anomaly; I am forced to ask myself how that many death certificates were complete in what I consider to be such an incomplete and insufficient manner. I have two theories, aside from some doctors simply not giving the proper attention to the task that they should have or not understanding the importance of completing the death certificate thoroughly. One is that some of the doctors who have been taking care of patients in this pandemic simply might not be familiar with how to complete a death certificate. This pandemic has brought doctors out of retirement and graduated 4th year medical students months early to shore up the frontlines; surely some just haven’t had even the 5 minutes of training from the video above and don’t know how to complete the forms properly; frankly it’s a low priority in their training right now. But second, some of the death certificates for COVID-19 patients have been completed by doctors who were incredibly overwhelmed. When we consider places like New York City, where doctors and nurses were dropping from exhaustion during shifts and barely had time to document at all, and were seeing multiple deaths per shift, each and every shift for weeks, it is reasonable to expect that some of those doctors no longer felt that taking the extra time to document a complete death certificate series of events was a priority. I can’t argue with them; it wouldn’t be. As important as the death certificate is to the patient’s family and for public health purposes, it is a low priority in a crisis when your time would otherwise be spent taking care of living patients or trying to shore up your own physical and mental reserves. If this is the case, the doctors who typed “COVID-19” and submitted the death certificates probably had no idea that such an action would contribute to even more dangerous medical misinformation threatening to extend the pandemic a few months later; a lesson in unintended consequences.
So what do all of these other codes mean?
There are many ways to interpret the diagnostic codes listed in the comorbidities table from the CDC’s latest update. We could spend hours in speculation, wild surmises, or careful parsing and analysis (if you’re a nerd) to try to recreate the narratives of the deaths represented by this data. The amount of analyzing, explaining, and even guesswork we could devote to this is endless. But briefly, I’d like to explain how to understand the majority of these diagnostic codes and the diseases, conditions, or symptoms they represent by considering them in three large categories.
Other ways of describing COVID-19.
The first category that these “other diagnostic codes” fit into is simply other ways of describing the symptoms and complications of COVID-19 itself. If I treated you in the hospital for a CVA (cerebrovascular accident; a stroke), but I also added on diagnosis codes for right arm paralysis and slurred speech, you wouldn’t review the medical record and say, “see, I wasn’t treated for stroke after all! They were treating me for right arm paralysis and slurred speech and just added that ‘stroke’ code on because Dr. Webb probably gets some sort of kickback for it.” The paralysis and the slurred speech delineate more specifically which stroke symptoms you experienced; their inclusion creates a more complete record of your presentation and treatment. In fact, it isn’t at all uncommon to have multiple diagnostic codes that actually say the same thing, due to different doctors and different departments interacting with your medical chart and, again, for the sake of completeness. If I have already added “slurred speech” to your chart, the neurologist later adding ‘expressive aphasia’ doesn’t actually add anything to your medical record (except a little reminder that she’s smarter than me); but it might be more appropriate to document it this way for the referral to speech therapy she is ordering for after your discharge, or to have this diagnostic code associated with the MRI. The synonymous diagnostic codes are repetitive, but it doesn’t necessarily follow that they are redundant.
Now apply this logic to death certificates and COVID-19. We’ve already discussed that most doctors would like to be as complete and thorough as possible with death certificates and that it is somewhat odd to list only one diagnostic code without providing a fuller narrative. When we see diagnostic codes like J96 (respiratory failure; 54,803 cases), R09.2 and I46 (respiratory and cardiac arrest, 3,282 and 20,210 cases respectively), and J12.9 (viral pneumonia, unknown number of cases, but contained within the “Influenza and Pneumonia” group), all the doctor is doing is using additional diagnostic codes to clarify the events affecting the patient’s lungs that led to death. In fact, it would not be inappropriate to include all four of these codes for many COVID-19 deaths, because the natural history of viral pneumonia due to COVID-19 leading to respiratory failure and eventual arrest is unfortunately far too common. The same applies to codes like A40 and A41, Sepsis (14,053), which is not even a diagnosis in itself but a syndrome describing the body’s systemic reaction to infection, and many of the “all other conditions” codes like R09.1, pleuritic chest pain and R09.0, hypoxemia.
But the most obvious example is J80, Adult Respiratory Distress Syndrome (21,899 cases). This is literally the severe respiratory syndrome caused by COVID-19, yet people like Dr. Hesse who claim to have evaluated this data carefully did not include these deaths in their “real” COVID-19 death count. To be clear, if a patient’s death certificate listed only COVID-19 and ARDS, these medical misinformation hucksters wouldn’t count them; that patient died of ARDS, they would say, not COVID-19. It’s like saying someone didn’t die from falling off a plane without a parachute, they died from the landing. It’s the bad dad joke of medical misinformation and the clearest piece of evidence we have that those originating this narrative are either extremely unqualified to interpret this information… Or else are not in earnest with their conclusions, but instead are pushing misinformation intentionally from what motivations and purposes I cannot say.
Conditions that really do make COVID-19 more dangerous.
Much of the work I have seen refuting the “6%” misinformation so far has focused on the concept of comorbid conditions or medical comorbidities. Simply stated, these are diseases or conditions that make us more susceptible to other disease processes or more likely to have complications from them. Some of these diseases are also extremely dangerous in themselves, and others are primarily dangerous because of their role in predisposing to other conditions. A good example of the former is Congestive Heart Failure (I50, 10,562 cases). This is an extremely dangerous, chronic disease that has a fairly low 5 year survivability from the date of diagnosis (average of 62%, but as low as 48%, in African American men because of healthcare disparities). You can absolutely die of complications from heart failure, but it also increases your risk for many other diseases and infections. It is both a primary cause of death and a comorbidity, and without a more detailed dataset or an intimate understanding of each case, we cannot possibly say how many of the 10,562 people who died with both COVID-19 and heart failure died from heart failure complicated by COVID-19, from COVID-19 which they were more vulnerable to because of heart failure, or from a more complex clinical picture that involved heart failure, COVID-19, and other contributing factors. But is this information going to change anything for us? The medical misinformation spreaders want you to believe that all 10,562 of the people who died with both heart failure and COVID-19 died at the time they would have from their heart failure with or without a viral pandemic. They want you to believe this based on nothing other than the fact that it fits a more comfortable narrative; but it flies in the face of what we are hearing from doctors, nurses, family members, and patients of those with heart failure about the way that COVID-19 affects those who are already suffering from these types of chronic illnesses.
Other examples in this category include renal failure (N17-N19, 13,693 cases), COPD and other chronic respiratory disease (J40-J47, 13,780 cases), and quite a few of the “other conditions and causes” listed, such as N04 (Nephrotic Syndrome), L93 (Systemic Lupus), and of course B20 (HIV), just to name a few. The people spreading this misinformation are putting the people with these illnesses at greater risk, specifically, by either pretending that COVID-19 is not a threat to them (the “only 6% count” crowd) or by seeming to claim, callously, that caution as a society isn’t warranted on their behalf (the “94% had comorbidities” crowd).
But within this category we also include diseases that are not likely to kill you on their own, and which would have almost certainly been included on the death certificate due to the physician’s conviction that they made the patient more susceptible and less able to resist the complications of their COVID-19 infection. These include Obesity (E65-E68, 5,614 cases), Alzheimer’s disease (5,608 cases), and of course other types of dementia (F01 and F03, 18,497 cases). Do we really believe that a patient with COVID-19 and obesity listed as their causes of death have died from obesity, and that their having COVID-19 was a coincidence? That is not something that happens. Dementia in particular is an interesting conundrum, because with COVID-19 harming so many people in nursing homes it is potentially not only a physical risk factor, which it most certainly is, but also an epidemiological risk factor; many doctors might include a patient’s reason for living in an assisted living facility, such as dementia or disability, within the death certificate as part of the narrative of how the patient came to be exposed to COVID-19, the same way we might list arthritis on the death certificate for a patient who suffered a heart attack during physical therapy. Again, these are not competing diagnoses that draw responsibility for the death away from COVID-19, but rather a fuller picture (that is, as full as can be told with diagnostic codes alone outside of the full medical record) of the patient’s story leading up to their death.

Finally, a few categories of disease deserve some extra discussion, and those are diseases that could cause death all on their own but almost certainly didn’t for the patients reflected in these death certificates. Hypertension (I10-I15, 35,272 cases) is incredibly common and usually leads to longterm organ damage rather than acute crises, but can present with severely elevated pressures that lead to stroke or another vascular event. However, this would typically be indicated with the diagnosis code I16, hypertensive crisis or I16.1, hypertensive emergency, which are specifically not included in the diagnostic codes for the hypertension group in this table. It is possible that this is just a common coding error on death certificates, but I doubt it; if the physician believed that the severity of the patient’s hypertensive crisis led directly to their death, they would likely take pains to emphasize this on the death certificate; applying a code for essential or secondary hypertension instead suggests that they regarded it as a comorbidity or at most a contributing factor. Diabetes (E10-E14, 25,936 case) is another example. Diabetic Ketoacidosis (DKA) is a severe metabolic disorder that often requires ICU level care; but this is primarily due to how labor intensive it is to treat, and the mortality rate remains low. These 25,936 people who had both COVID-19 and diabetes did not die from DKA, which accounts for less than 2,500 deaths annually. Instead, both diabetes and hypertension, just like dementia and obesity, are comorbid conditions that make the patient more susceptible to and likely to experience worse outcomes from other diseases, and as such their role in this list of additional diagnostic codes on COVID-19 death certificates is the same as their role in death certificates for patients who die from stroke, heart disease, and influenza; yet no-one is claiming that because a patient had high blood pressure and diabetes, their death from the flu didn’t count.
Conditions that might have nothing to do with COVID-19 and might have actually caused the patient’s death (maybe)
Finally, we have conditions that, based on the diagnosis code alone, we know to be incredibly dangerous and also to be common causes of death. Some of these, like certain cancers (C00-C97, 7,415 cases plus some of the ‘all other conditions’ group) we can treat similarly to heart failure or COPD; they may predispose you to COVID-19 or raise the risk that your COVID-19 course of illness will be severe, or they may be immediately dangerous in and of themselves and be worsened by COVID-19 or not. If someone wants to ask how many of the thousands of deaths that included a cancer diagnosis were actually caused or hastened by COVID-19, and how many just happened have the virus during the days leading up to to death from a terminal malignancy, I think it’s a fair enough question; though from what I’ve heard from friends who provide hospital and hospice care, the former does seem to be very common. In the latter cases, if such cases are at all common, the additional suffering from COVID-19 must be felt in other ways; in the barriers it places to those individuals being surrounded by family and friends as much as possible during their final days.
We could legitimately ask the same question for some other diagnoses on the list; heart attacks and cardiac arrhythmias (18,103 and 9,812 cases respectively), pulmonary embolism (I26, contained in the 8,743 “other disease of the circulatory system”), and strokes (I60-I69, 7,653 cases) are all very deadly on their own. However, unlike with cancer, which has no known or proposed causal relationship with COVID-19 aside from immunocompromise, the virus is known to cause a hypercoagulable state that has caused all of the above pathologies. How many of the deaths that involved these diagnostic codes were due to these conditions and how many were in turn due to COVID-19 is known only to the doctors, nurses, and family members that were involved in their care. Attempts to make absolute statements that these deaths simply were not caused by COVID-19 (despite the doctor writing the death certificate feeling they the virus did in fact contribute to the death) because another dangerous disease was also involved are based entirely on a desire to minimize the danger of the virus, and not on any interpretation or analysis that can be legitimately conducted from this set of data.
The final set of diagnostic codes we need to look at are the 5,133 included in COVID-19 death certificates under the category “Intentional and unintentional injury, poisoning and other events.” We don’t know which codes specifically show up in these death certificates, but much like the other ‘other’ catch-all categories it contains diagnoses ranging from S00.37XA, Other superficial bite of nose (a diagnosed I received today courtesy of my 16 month old), to X95.9, Assault by firearm. What is going on here? Much like the “other” diagnostic codes we talked about above, there may be any number of reasons that some of these codes might be on a COVID-19 death certificate. Some may be complications that arose in the hospital, such as SO6.9, Intracranial injury, when a COVID-19 patient experienced a syncopal episode and hit their head. Some may be part of a historical narrative, for instance a patient who experienced a prolonged hospitalization following a V03.10XA, Motor vehicle collision injuring a pedestrian, which ultimately ended when they died from respiratory failure due to COVID-19 contracted in the hospital. Again, without access to the actual death certificates, medical records, and medical staff who treated these patients we simply do not know what circumstances or patient history necessitated the physician to include both COVID-19 specific diagnostic codes and codes for accidents or intentional and accidental injuries in the same death certificate; but it absolutely does not stretch the bounds of credulity to believe that such circumstances do indeed occur.
Nevertheless, I want to cede this point to the conspiracy theorists, if only for just a moment. What if we do “admit” (as ridiculous as it is, and with apologies to the families of the individual people whom these death certificates represent) that each and every death certificate listing one or more of these accidental and non-accidental injuries represents a patient who died from some horrible accident, with COVID-19 just tacked on but clinically silent? You see, since the beginning of the pandemic the conspiracy theorists have been telling us, with no evidence, that “if somebody gets hit by a car they are calling it a COVID-19 death” and “if someone gets shot, they call it COVID-19 to inflate the numbers.” This data, from actual death certificates, now shows that the maximum possible number of such falsified death certificates tacking on COVID-19 to an accidental death is 5,133; compared to 183,000 deaths from COVID-19 and an estimated 80,000 total deaths from accidents in that same time frame. And again, that’s assuming that no other possible explanation exists for those “other accidental and non-accidental injuries” contributing to a person’s death from COVID-19.
Conclusion
Many of the diagnostic codes listed don’t fit easily into just one of the above categories, because we just don’t know enough about the history of the people whose battles with and deaths from COVID-19 are represented here. We don’t know, from this data set, whether the physician completing the death certificate was indicating a new stroke as a primary cause of death, or an stroke that lead to a rehab stay where the patient contracted COVID-19. We don’t know whether diabetes was listed because it was poorly controlled and played a major role in the hospitalization, or whether it was well controlled and was only included because that physician knew that diabetes is a risk factor for the patient’s unfortunate bad outcome from COVID-19 infection. We also have no idea what to do with codes that are so benign in themselves that they don’t really seem to have a place on a death certificate at all, yet the physician clearly regarded as an important part of the patient’s history leading up to their death.
But what we do know, with certainty, is that this new data released from the CDC does not mean. If you’ll spend just a few minutes really looking at the data, at the ages and the conditions mentioned, you will realized that it cannot mean that 94% of the people who have died from COVID-19 were incredibly sick, incredibly frail, and incredibly old people with many other diseases who would have died soon anyway; that argument is as bankrupt in its analysis of this data set as it is ugly in its callousness. That is not what the CDC means when they tell us that 94% of death certificates listed ‘more than one diagnostic code’ or contributing factor, as we’ve clearly demonstrated above. And even if it were (and it’s not), it would not somehow mean that the lives lost to COVID-19 were less valuable; those who see this false idea that 172,000 of the 183,000 people who have died from COVID-19 were sick already as a compelling reason to stop mitigation efforts need to carefully consider whether their only motivation for taking caution has been their own personal health and safety this entire time… And then try to understand why that has not been the sole or primary motive for the rest of us; that the safety of those around us, including the medically vulnerable, is actually sufficient reason for some inconvenience and even sacrifice on my part.
And we also know with certainty that no real scientist, statistician, epidemiologist, or physician, and certainly no one who actually treats patients on their death beds and then completes death certificates to capture the complex and detailed medical events of their final days would ever believe the idea that the 6% of death certificates with only COVID-19 listed as a cause of death represents the “real” death told of this horrible virus; at least not without some herculean effort of intellectual dishonesty and self-deception.