I have seen this video of Dr. Simone Gold, Dr. Stella Immanuel, and Dr. Dan Erickson, and other physicians in almost every format over the past 24 hours; from a 45 minute long version to just Dr. Immanuel’s comments. My favorite presentation of it, if I’m allowed to pick a favorite, is the headline that I saw first which read, “American Doctors Address COVID 19 Misinformation with SCOTUS Press Conference.” I know it’s the oldest tactic in the book, but something about people spreading misinformation by claiming they are fighting misinformation still really gets to me. I understand this video was viewed over 14 million times before youtube and social media sites began to take it down, and I understand why. The group, America’s Frontline Physicians, present themselves in patriotic themed lab coats (I did not know that was a thing) in front of the US Capitol (or whatever building that is; I was homeschooled), and tell Americans what we have all so desperately wanted to hear for months; there’s nothing to be worried about, your lives can go back to normal now.
Several of these physicians we are already familiar with. Dr. Dan Erickson’s interview with local news stations was perhaps the biggest COVID-19 misinformation viral video until Plandemic came along (a week later), and Dr. Simone Gold has gone viral multiple times; I addressed her “COVID-19 as a Mass Casualty Event” letter on the blog back in May. Though these doctors don’t know me from Adam, to me they are starting to feel like old friends; or at least old frenemies. They are becoming more sophisticated in the posturing they take around misinformation (that sounded ominous; “they are becoming more sophisticated”, like they were killer robots from SkyNet); including in their talk the idea that they are being ‘silenced’ even though tens of millions of Americans have heard their dissenting minority opinions, claiming to speak for ‘thousands of doctors’ (this is probably an accurate number; there are about 1.1 million doctors in the US), and painting a convincing picture of themselves as the front-line doctors ‘actually diagnosing and treating’ COVID-19 and the people ‘silencing’ (read: disagreeing with) them as shadowy powers-that-be, as opposed to just being the vast majority of conscientious front-line doctors who simply hold to higher standards of evidence and have less tolerance for the invasion of political concerns into our care of patients. All of this is lent some credence by the fact that this video is being censored on Youtube and Facebook, of course; but considering the views they share really are dangerous, I have to admit that I don’t know whether censoring the video is the right call or not; I’m glad it’s not my decision to make. My approach has been to analyse and discuss, and I’m thankful for those who have provided me with the transcript and alternative links to the video for me to try to do that.
Since I worked from 8-5 today, including a morning spent in our outdoor tent clinic diagnosing, treating, and counseling patients with COVID-19, and a motorcycle drive in a torrential downpour (it said 10% chance of precipitation!), I’m about 18 hours behind on responding to this video. In interest of making this analysis available to those who have asked for it more quickly, I’m going to take it one doctor at a time, starting with a response to Dr. Stella Immanuel’s comments. The full transcript is below, up to the Q&A which I won’t spend time addressing. My comments are in blue and will be added as I go.
TL;DR: Posting now, editing and adding to later. Reserve the right to wake up at 3 AM and fix spelling erros.
Congressman Norman: (00:00)
… I’ll turn it over.
I have no idea who Congressman Norman is, but it has a very sinister ‘Spider-Man villian’ ring to it, doesn’t it?
Dr. Simone Gold

Dr. Simone Gold: (00:01)
Thank you. Thank you so much congressmen. So we’re here because we feel as though the American people have not heard from all the expertise that’s out there all across our country. We do have some experts speaking, but there’s lots and lots of experts across the country. So some of us decided to get together. We’re America’s Frontline Doctors. We’re here only to help American patients and the American nation heal. We have a lot of information to share. Americans are riveted and captured by fear at the moment. We are not held down by the virus as much as we’re being held down by the spider web of fear. That spiderweb is all around us and it’s constricting us and it’s draining the lifeblood of the American people, American society, and American economy.
America’s Frontline Doctors seems like a new organization, but for COVID-19 Viral Video enthusiasts like myself, seeing them all together in this video feels like the first time we saw all of the The Avengers together in The Avengers after 4 years of build-up. The group’s logo is a caduceus overlaid with an American flag; a perfectly fine image, I suppose, but taken with their political aims it sends a clear message; “we are the only doctors that true American patriots can trust.” Later, when these physicians make claims that other doctors have not been using hydroxychloroquine, have been encouraging people to wear masks, or have been advising caution and social distancing because of political motivations, please remember exactly who has overtly politicized their medical calling and emblazoned it on their lab coats. You know what my lab coat has it on? Germs (that’s what they all have, which is why I don’t wear one).

I think Dr. Gold’s discussion of the fear capturing the American people here is very interesting. Certainly there are many responses to the deadly viral pandemic that America is facing; fear, anxiety, bravado, calloused indifference, defiance. I’ve had all of those responses myself, and that was just this morning. I have seen many people suffer from anxiety about the virus, for the sake of themselves and their loved ones, and have offered a listening ear and counseling (and, when appropriate, anxiety medication); I have also seen people who consider COVID-19 to be a political tool or a hoax and have shown brazen disregard of the very real danger posed by the virus, and a great many of them are going to watch and share this video. There is something fairly calloused and icky about sharing a message that ‘you don’t have to be afraid anymore’ to people you already know aren’t taking a dangerous thing seriously. Nevertheless, I’ve actually repeated Dr. Gold’s main point here, “I don’t want you to be afraid,” at least 100 times in the past week; probably far more. When I counsel patients who likely have COVID-19, or whose loved ones do, I almost always tell them that I don’t want them to be afraid. I also tell them about social distancing and counsel them on isolation precautions, and talk to them about getting in touch with their close contacts to encourage them to quarantine, and I talk with them about reasons they would return to my clinic or go to the ER or even call 911 if their symptoms worsen. Because my desire for them not to be afraid isn’t because there isn’t anything anything to be afraid of, like Dr. Gold claims, but because because fear leads to anger and anger leads to hate, and hate leads to suffering… Because fear is the mind killer, the little-death that brings total obliteration… Because with great power comes great (no wait that isn’t one, sorry)… But really because God has not given us a spirit of fear, and I believe that my patients will thrive best and be most free from fear when they have a healthy respect and understanding of the virus and how to protect others and respond to complications based on the best, most reliable information possible.
Dr. Simone Gold: (00:53)
This does not make sense. COVID-19 is a virus that exists in essentially two phases. There’s the early phase disease, and there’s the late phase disease. In the early phase either before you get the virus or early, when you’ve gotten the virus, if you’ve gotten the virus, there’s treatment. That’s what we’re here to tell you. We’re going to talk about that this afternoon. You can find it on America’s Frontline Doctors, there’s many other sites that are streaming it live on Facebook. But we implore you to hear this because this message has been silenced. There are many thousands of physicians who have been silenced for telling the American people the good news about the situation, that we can manage the virus carefully and intelligently, but we cannot live with this spider web of fear that’s constricting our country.
Dr. Simone Gold: (01:45)
So we’re going to hear now from various positions. Some are going to talk to you about what the lockdown has done to young, to older, to businesses, to the economy, and how we can get ourselves out of the cycle of fear. Dr. Hamilton.
Dr. Bob Hamilton

Dr. Bob Hamilton: (02:03)
My name is Dr. Bob Hamilton. I’m a pediatrician from Santa Monica, California. I’ve been in private practice there for 36 years. And today I have good news for you. The good news is the children as a general rule are taking this virus very, very well. Few are getting infected. Those who are getting infected are being hospitalized in low numbers. And fortunately the mortality rate of children is about one fifth of 1%. So kids are tolerating the infection very frequently, but are actually asymptomatic.
And thank God for that. As a father of 4 young children, I cannot even imagine the anxiety, fear, and paranoia I would experience if we were living through a pandemic like the Spanish Flu, which disproportionately killed young children. I cannot imagine the pandemonium, the incredible amounts of fear, and even the difficulty in staffing clinics and hospitals if exposure to the virus put our children‘s lives at great risk instead of just our own. Though Dr. Stella Immanuel below discusses the panic that her patients commonly present with when they believe they may have COVID-19, I’ve only see this a few times; many patients need reassurance and education, but only a handful have been truly on the verge of a panic attack. But I have seen many, many people very concerned about their children and grandchildren. In fact, when I inform patients that they have been diagnosed with COVID-19, they usually ask “what about my children?” before they ask any other question.
The truth is we don’t know the mortality rate among children, for a lot of the same reasons that it’s so hard to lock-down a true infection fatality rate in general; imperfect testing, asymptomatic cases, minimally symptomatic cases that are never tested, and still being fairly early in the course of the pandemic and not having all of the data we need. But we all agree it’s smaller than for older patients, and Dr. Hamilton’s estimate of 0.2% is within the commonly accepted range based on the data we do have. I would point out that 0.2% is still a very alarming mortality rate for a virus that is as infectious as COVID-19; but a lot of us hope the rate is actually even lower and that children tend to be asymptomatic or minimally symptomatic at a high enough rate that we are simply missing most cases. We hope, but we don’t know. So while I can counsel the patients who anxiously ask me if their children are going to be ok (which would be the very first question on my mind as well) that they are at less risk from COVID-19 than any other age group, I cannot promise them that their children will be unaffected or free from risk, and I still counsel them on what to watch for.
Dr. Bob Hamilton: (02:38)
I also want to say that children are not the drivers of this pandemic. People were worried about, initially, if children were going to actually be the ones to push the infection along. The very opposite is happening. Kids are tolerating it very well, they’re not passing it on to their parents, they’re not passing it onto their teachers. Dr. Mark Woolhouse from Scotland, who is a pediatric infectious disease specialist and epidemiologist said the following. He said, “There has not been one documented case of COVID being transferred from a student to a teacher in the world.” In the world.
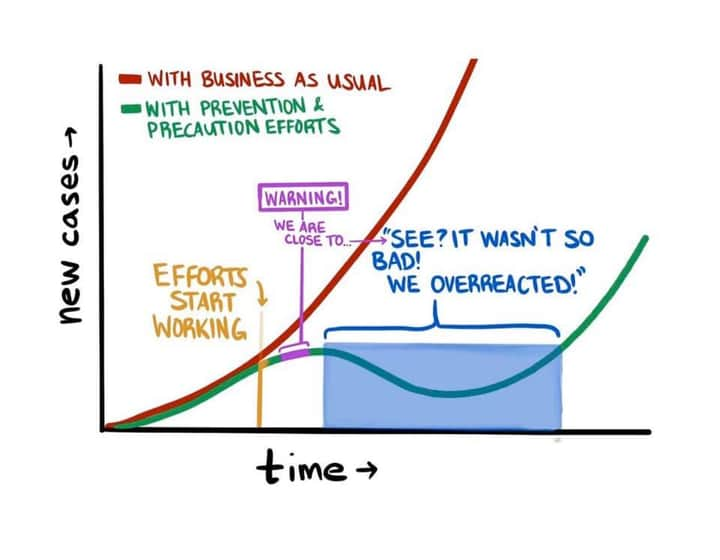
I think here Dr. Hamilton is straying into a fairly disingenuous way of looking at these statistics. One of the first and most widely followed mitigation steps early in the pandemic was to transition schools to online learning. More than closing non-essential businesses, more than observing social distancing, more than wearing masks once sufficient evidence to support mask-wearing was amassed, children were compliant with not being in school at very high rates because schools were, physically, closed. I will accept that children have not been the driver of the pandemic; they are also one of the groups that has been kept at home most successfully during it. Saying children have not driven the pandemic is not the same as saying they would not have or might not if these mitigation measures were not followed. The question of whether or not children can or will drive the pandemic once schools reopen in person is nuanced and difficult; I’ll try to address it in the next paragraph and in greater detail in a later article. But it’s important that we don’t fall into the trap of evaluating the course the pandemic has taken so far without taking into account the effects of the precautions and mitigation measures we have taken in response to it.
Dr. Bob Hamilton: (03:19)
I think that is important that all of us who are here today realize that our kids are not really the ones who are driving the infection. It is being driven by older individuals. And yes, we can send the kids back to school I think without fear. And this is the big issue right now, as Congressman Norman alluded to, this is the really important thing we need to do. We need to normalize the lives of our children. How do we do that? We do that by getting them back in the classroom. And the good news is they’re not driving this infection at all. Yes, we can use security measures. Yes, we can be careful. I’m all for that. We all are. But I think the important thing is we need to not act out of fear. We need to act out of science. We need to do it. We need to get it done.
Again, just because children in school have not driven transmission so far, because they have not been in school, doesn’t mean that it isn’t a risk. I don’t know whether or not we should reopen schools normally in a few weeks. There are lots of reasons I haven’t been able to come to anything like a firm conclusion about it. The data is complicated, and it’s such an important question that it really does require a degree of thorough research and critical thinking that I have not been able to give to it yet. Part of that is my own privilege; my wife and I homeschool our four children (and I include “and I” very generously), so it’s a question that doesn’t personally affect us. Homeschooling has always involved some degree of privilege, even though it is also challenging and requires sacrifice, but that’s never been quite so obvious to me as it is now in the midst of this pandemic, when this one big question mark seems to be looming over nearly every family we know but our own. But even though it doesn’t directly affect our own children, there are many teachers and school aged children that we deeply care about (and tons that we sort of care about or middling care about), and the question has been heavy on my mind, especially as more and more close friends have asked me to research and write about it.
All of that to say, I don’t have an answer today; I hope to write about it soon, but I can’t promise I’ll have an answer then either. For now I’ll say this; I think the burden of proof has to be on the side of proving it’s safe, not on the side of proving it’s not safe. I need to review the studies on transmission and shedding in children, but the claim I’ve seen that children are very unlikely to transmit the virus seems very counter-intuitive. Transmitting respiratory viruses is what children do. I’ve got four of these booger goblins at home; the little one gives kisses by putting his entire mouth around your nose, and the 2nd youngest “whispers” to you by blowing spit into your ear and your eyeball. One of the questions we always ask someone with a cold or flu, even pre-COVID-19, is whether they have been around anyone sick. If the answer is “well I have kids” or “well I work in a school” my response is, “say no more.” If there’s one thing we’ve learned about COVID-19, it’s that it’s different. Maybe kids really don’t shed it, maybe they really don’t spread it to each other or to adults; maybe we can reopen schools with sufficient distancing guidelines that it will not endanger the lives of children or or adolescents or their caregivers, teachers, or families. If that’s the case, that’s wonderful; but it has to be very, very clearly demonstrated by real scientific evidence. It isn’t something we can risk on the type or quality of “evidence” that some of the members of America’s Frontline Doctors seem to find sufficient. We’ll try to look at as much of that evidence as we can in an upcoming post.
Dr. Bob Hamilton: (04:07)
Finally, the barrier, and I hate to say this, but the barrier to getting our kids back in school is not going to be the science, it’s going to be the national unions, the teachers union, the National Education Association, other groups who are going to demand money. And listen, I think that it’s fine to give people money for PPE and different things in the classroom. But some of their demands are really ridiculous. They’re talking about, where I’m from in California, the UTLA, which is United Teachers Union of Los Angeles, is demanding that we defund the police. What does that have to do with education? They’re demanding that they stop or they shut all private charter schools, privately funded charter schools. These are the schools that are actually getting the kids educated.
This gets too deep into politics for me. Look at the various teachers unions’ demands (if they have demands) in your area for yourself and see if you think what they are asking for is reasonable. Better still, talk to teachers you know and ask for their opinion on reopening schools, the same way that you would (hopefully) ask me or another physician you know about our views on wearing masks or other medical issues related to the pandemic. I know some teachers, and I know that their greatest desire (besides something called a “smart board”) is to be back in the classroom educating and pouring life into your children. They want the schools to reopen, but they want to know the safest and wisest way for it to happen, because too much of their job already deals with childhood suffering, and seeing anything like an abnormally high number of their students (your children) die from COVID-19 because we re-opened schools in the midst of a surge of cases would break them. No profession is perfect (something I’m hoping to write about soon too, but in the meantime you should go read Harriet Washington’s Medical Apartheid for yourself), but if you don’t think doctors in general want you to be well and thrive, and you don’t think teachers want your children to grown and learn, I’ve got some questions about who you do trust.
Dr. Bob Hamilton: (04:59)
So clearly there are going to be barriers. The barriers will not be science. There will not be barriers for the sake of the children. That’s going to be for the sake of the adults, the teachers, and everybody else, and for the union. So that’s where we need to focus our efforts and fight back. So thank you all for being here and let’s get our kids back in school.
Leave out that there really are some scientific barriers to knowing whether or not fully reopening schools is actually going to be safe for the children, which is probably the single biggest concern among teachers anyway; there’s still something very calloused about calling out teachers for not wanting to re-open schools because of concerns about their own safety.
Dr. Stella Immanuel

Dr. Stella Immanuel: (05:27)
Hello, I’m Dr. Stella Immanuel. I’m a primary care physician in Houston, Texas. I actually went to medical school in West Africa, Nigeria, where I took care of malaria patients, treated them with hydroxychloroquine and stuff like that. So I’m actually used to these medications.
I’ve learned an awful lot from African physicians over the years, though I’ve never been to Nigeria and have not had the privilege to travel to West Africa since before medical school. I do not know the arc of Dr. Immanuel’s career, how long she practiced in Nigeria and how long she has now practiced in the US (I am told she used to live in the same city where I did undergrad). On my most recent short term trips to volunteer in hospitals in South Sudan and Uganda, I went in a teaching role; and while I did have some things to contribute, there is no question that I gained from doctors there more knowledge and insight than I was able to give, which is what I fully expected would happen. And nowhere was this dynamic more clear than in treating patients with “tropical diseases” like yellow fever and malaria. Diagnostic tests, medications, and clinical pictures that I had encountered primarily in textbooks were bread and butter medicine for the physicians I worked with, and I’m sure I must have seemed fairly slow on the uptake, trying to figure out the right chloroquine dose for pediatric malaria patients or recognize the differences in the clinical picture between malaria and dengue fever. While I’ve now also used these medications for malaria, in addition to prescribing them for lupus here in the US, I would completely concede more extensive experience with antimalarial agents to a West African trained doctor like Dr. Immanuel. What I cannot honestly concede is more extensive experience diagnosing and treating COVID-19.
Dr. Stella Immanuel:
I’m here because I have personally treated over 350 patients with COVID. Patients that have diabetes, patients that have high blood pressure, patients that have asthma, old people … I think my oldest patient is 92 … 87 year olds. And the result has been the same. I put them on hydroxychloroquine, I put them on zinc, I put them on Zithromax, and they’re all well.
The best way to study a medication’s efficacy is a double-blinded, randomized, controlled trial. There are studies that have been done and are being done on hydroxychloroquine for COVID-19 that are designed this way, and if done carefully they will provide the absolute highest quality data we will have on this medication. So far the ones we have do not show benefit. It’s worth pointing out here that one large, well-designed study is of much greater value than many small or poorly designed studies, and of infinitely greater value than any one or a few clinicians’ anecdotal experiences. But in a pandemic I do believe in an all-hands-on-deck approach to both clinical treatment and research, and I appreciate all of the doctors for whom research is not a usual interest or activity taking the time and energy to bring their results forward.
But we would not be wise to digest these results without understanding their significance. When Dr. Immanuel says she has treated 350 patients for COVID-19, that feels like a fairly large number; especially compared to the dozen that Dr. Bartlett had treated to support his claims for budesonide or the 50 that Dr. Procter had treated in a recent viral facebook post. But we still need more information, like how her patient population’s demographics compare to the population in general, which she only hints at, telling us the age of her oldest patient but not providing a median age or other demographics factors or data on comorbidities or high-risk conditions. Depending on their risk factors and their ages, zero deaths out of 350 might be exactly what we would expect. Even if Dr. Immanuel’s population perfectly represented the general population (and we have good reasons to suspect this is not the case, as we will discuss below), where we believe the infection fatality rate is somewhere in the still-very dangerous- range of 0.4% to 1.3%, this would only be 1-4 fewer deaths than expected; wonderful, well worth celebrating, but not miraculous, and certainly not proof of a cure. But aside from the simple numbers, there are bigger issues we need to be honest about here.
Dr. Stella Immanuel: (06:12)
For the past few months, after taking care of over 350 patients, we’ve not lost one. Not a diabetic, not a somebody with high blood pressure, not somebody who asthma, not an old person. We’ve not lost one patient.
As I’ve done for every doctor making claims of perfect efficacy for unproven medications over the past few months, I’d like to look at Dr. Immanuel’s claims in the context of her treatment setting; namely, outpatient Family Medicine in Houston, Texas. Here is the graph of positive cases in Houston.

If this looks familiar to my fellow Wacoans, maybe it’s because it looks almost identical to the trend in cases in Waco, and really in most places around Texas. Here is our trend from April to July from the health department’s tracker at covidwaco.com (based on positive test results).

You’ll note these charts are not to the same scale; Waco does not (yet) have a population of 2.3 million people. But there are only so many patients a doctor can see in a day, and both Waco and Houston have had plenty of COVID-19 cases, and people being evaluated for possible cases, to keep more than one doctor very busy, and it’s pretty hard for me to imagine that Dr. Immanuel has seen many more patients for evaluation of COVID-19 symptoms than I have over the past couple of months. But if we look at these trends it strongly implies that the vast majority of her patients who actually had COVID-19 would have been in the past 6 weeks, just like mine have been; before that the infection rates in Houston and in Waco were too low for either of us to have extensive experience with patients who actually had the virus, regardless of how many people we were evaluating and testing (important work still, since none of us knew when our surge would start). She doesn’t tell us how many of her 350+ patients were in March, April, and May and how many have been since mid-June, just that she has treated that many patients with hydroxychloroquine over the past several months. If we assume that the majority of these patients have been in the last 42 (great number) days since cases began to climb in Houston, it means that a lot of her patients are not out of the woods yet. There is a lag time from the development of early symptoms of COVID-19 to the development of severe complications, and a further lag time from this to death, while patients fight for their lives in the hospital and doctors and nurses do everything in their power to help them. Finding an exact number is difficult because there are so many factors and so many different ways that people are affected by the virus; but the total lag from onset of symptoms to death seems to be around 18 days. Even this is likely an underestimate, however, since any such data would exclude people experiencing a prolonged battle with the virus who are still fighting it at the time the data is collected, but ultimately pass away from it later. This gives us a mere 24 days during which we can say Dr. Immanuel has had time to see a significant number of patients with COVID-19 and feel confident in saying that those patients have fully recovered and are no longer in danger.
I am playing a bit fast and loose with these numbers here, because I don’t actually think Dr. Immanuel means that the majority of her 350 “COVID patients” have been within the past 6 weeks. The point is this; when doctors claim to have been treating COVID-19 a certain way for months, you need to look and see how many months there have actually been COVID patients in their area. Because if the length of time they have been ‘treating COVID’ successfully and the length of time that SARS-CoV-2 has been endemic in their region don’t line up, we have to ask an important question that runs deeper even than the demographics and risk factors of their patients; did the patients they treated even have COVID-19 at all?
You see, over and over when we have heard from physicians like Dr. Irene Lozano and Dr. Brian Procter that they have a 100% cure rate with hydroxychloroquine or another regimen, it turns out that their definition of ‘having COVID-19’ is extremely liberal. One admits to treating patients with minimal symptoms and questionable exposures; the other says he doesn’t even believe in testing for COVID-19. This is the most basic concept of epidemiology imaginable, but you can’t die from a disease you don’t have. If a doctor says they have successfully treated a condition x number of times, but their diagnosis of the condition doesn’t conform to accepted standards of certainty or rely on any evidence other than a hunch or their desire or ideological commitment to ‘diagnose’ and treat the condition, their results are less than useless; they don’t even count as anecdotal evidence.
I don’t know if this is the case for Dr. Immanuel; she doesn’t say that she doesn’t believe in testing, she doesn’t tell us what test her clinic uses or its sensitivity and specificity, or how many of her hydroxychloroquine patients were treated during Houston’s pre-surge months, or if she uses the accepted clinical diagnostic criteria in lieu of a positive test. I cannot say definitively that Dr. Immanuel has done what so many doctors in these videos have done and artificially inflated her COVID-19 patient series by treating people who did not meet any accepted diagnostic criteria but were merely worried they might have the virus. But this is absolutely key to understanding the significance of her success rates, and I do think she gives us a few important clues in that direction.
Dr. Stella Immanuel:
And on top of that, I’ve put myself, my staff, and many doctors that I know on hydroxychloroquine for prevention, because by the very mechanism of action, it works early and as a prophylaxis. We see patients, 10 to 15 COVID patients, everyday. We give them breathing treatments. We only wear surgical mask. None of us has gotten sick. It works.
This is clue number one, and it’s a big one. I sometimes use a phrase I’m pretty sure I’ve coined; “we aren’t keeping the secret medicines for doctors hidden in the back.” I say this, when I think it’s appropriate to the patient, to help dispel the idea that I am holding out some sort of secret treatment that I only prescribe to other doctors and their families, which is something that my patients sometimes believe (and that some of them have very good historical reasons for believing). A compassionate, conscientious physician is going to treat your condition the same whether you have an MD or PhD or have very little education, whether you are rich or poor, and even whether or not they like you or you are mean to them; we don’t keep secret medicines in the back that you don’t unless you are ‘in the club.’ And because I believe that Dr. Immanuel is a compassionate physician, I don’t believe that she would be willing to give herself, her staff, and other doctors and medical personnel hydroxychloroquine as prophylaxis if she were unwilling to do the same for others. If she really believes it works in this clinical setting, it would be consistent of her to offer hydroxychloroquine for patients who have been around others with COVID-19, or thought they might have been, or who work in other high risk environments like nursing homes, food service, and grocery stores. And because she has more extensive experience with hydroxychloroquine for malaria treatment and prophylaxis than most US trained physicians, it would be reasonable to expect her to be somewhat more liberal in prescribing it for this purpose without the same degree of anxiety a doctor might feel who has only used it for lupus.
In claiming that she has successfully treated over 350 patients with COVID-19 with hydroxychloroquine, is Dr. Immanuel including the patients she has treated merely for prophylaxis, who have not been diagnosed with an infection at all? I don’t know, but considering the national stage and the passion she feels on this issue, I would feel a great degree of temptation to include those patients and bolster my treatment numbers, and if I wasn’t including them I would want to be explicit on that point.
Dr. Stella Immanuel: (06:46)
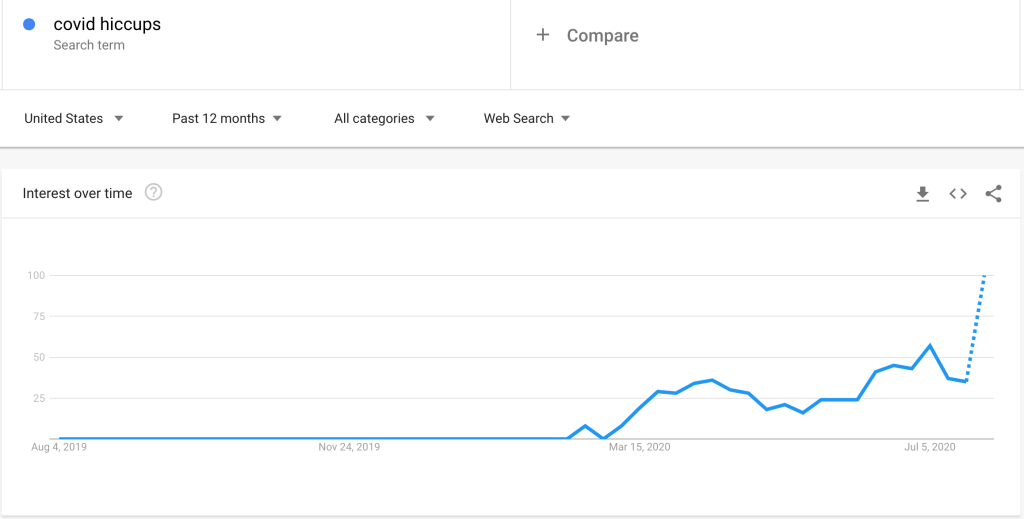
So right now, I came here to Washington DC to say, America, nobody needs to die. The study that made me start using hydroxychloroquine was a study that they did under the NIH in 2005 that say it works. Recently, I was doing some research about a patient that had hiccups and I found out that they even did a recent study in the NIH, which is our National Institute … that is the National … NIH, what? National Institute of Health. They actually had a study and go look it up. Type hiccups and COVID, you will see it. They treated a patient that had hiccups with hydroxychloroquine and it proved that hiccups is a symptom of COVID. So if the NIH knows that treating the patient would hydroxychloroquine proves that hiccup is a symptom of COVID, then they definitely know the hydroxychloroquine works.
Dr. Immanuel is referring to a case report from April of one patient, a 62 year old man who presented to the ER with hiccups; he was found to have diffuse groundglass opacities on CT scan of his lungs and tested positive for COVID-19. The case study mentions that he was treated with hydroxychloroquine exactly once (twice if you count the abstract); it was standard treatment at the time this man was admitted, as it was in most places around the country before more evidence emerged that it wasn’t efficacious. The study draws absolutely no conclusions that his COVID-19 was cured by hydroxychloroquine, but rather was published to emphasize that “physicians should keep COVID-19 infection on their differential as more cases are discovered through atypical presentations.” The idea that this case study somehow proves that the NIH “knows the hydroxychloroquine works” is a complete non-sequitur and betrays either intentional or accidental misunderstanding of the case study. Also, I love it when people google things and then post viral videos telling other people to google those things; it creates fascinating Google Trends graphs:
Dr. Stella Immanuel: (07:42)
I’m upset. Why I’m upset is that I see people that cannot breathe. I see parents walk in, I see diabetic sit in my office knowing that this is a death sentence and they can’t breathe. And I hug them and I tell them, “It’s going to be okay. You’re going to live.” And we treat them and they leave. None has died.
This is clue number two. You see, Dr. Immanuel has fallen into the trap that so many other doctors whose claims we have looked at on this site have fallen into; they are actually treating the virus as though it were even more dangerous than it already is. Most doctors I know would accept a death rate for COVID-19 somewhere between 0.4 and 1.3% based on the best data we currently have available; incredibly dangerous, but not a death sentence. The diabetic patient with COVID-19 is most likely to recover without treatment, but if unchecked the virus could easily kills hundreds of thousands or even millions. That’s what happens in most dangerous, contagious illnesses; if unmitigated, it will kill far too many people, but any particular person is still statistically unlikely to die. In fact, I spend a lot of my time saying to my patients I am testing for COVID-19 almost what Dr. Immanuel is saying. I don’t hug them, but I do offer a therapeutic hand on the arm and say, “I think you’re going to be ok. Most people recover from this and never have to be in the hospital. Let’s talk about what to watch out for and how you can feel a little better while your body fights this.” By believing that this virus is almost universally deadly for certain people, she is ensuring that her evaluation of her treatment numbers is biased, because she then cannot objectively compare her survival rates to the real death rates. Each case proves the drug was the key, miraculous cure, because she’s convinced that each patient she treats would have died without it.
Dr. Stella Immanuel:
So if some fake science, some person sponsored by all these fake pharma companies comes out say, “We’ve done studies and they found out that it doesn’t work.” I can tell you categorically it’s fixed science. I want to know who is sponsoring that study. I want to know who is behind it because there is no way I can treat 350 patients and counting and nobody is dead and they all did better.
Two things on this. Most of the COVID-19 and hydroxychloroquine studies that have come out have not been sponsored by any pharmaceutical company (I can’t think of any that have off the top of my head), and this is the first time I’ve ever seen someone accuse drug companies of fixing data to prove that there was no specific drug therapy available. (yes, yes, I know; they are just setting us all up for a vaccine).
But more importantly, there absolutely is a way that she could treat 350 patients with no deaths and it not be due to hydroxychloroquine, because many doctors around the country have exactly these same types of numbers without using it. In fact, this is almost exactly what my numbers look like. I don’t feel at liberty to disclose the numbers or any details from my clinic without authorization from those patients; but I have been treating at least 20-30 patients for COVID-19 symptoms and exposure daily for weeks, and evaluating a significant number for the symptoms of COVID-19 in the months leading up to the beginning of our surge 6-7 weeks ago. I have treated well over 350 patients for suspected COVID-19, and many have been positive for the virus. None of them have died, praise God. Would I be justified in attributing this to something I am doing? Is it my particular form of counseling and reassurance? Is one of the symptomatic/supportive treatments I am recommending, like tylenol for body aches or hot tea with honey for sore throat, secretly an anti-COVID-19 miracle drug? Does my breath inhibit COVID-19? Of course not. The difference is that none of these have a theoretical mechanism of action against COVID-19 (although my breath may encourage social distancing), and many medications like hydroxychloroquine and budesonide do. I am extremely hopeful that studies will prove some clinical setting or scenario where these really are useful for COVID-19; but using before then because of unreliable anecdotal evidence is irresponsible.
We would be better served looking at my patients, if we could. Some were only recently diagnosed and, as we’ve already stated, aren’t out of the woods yet. If you don’t think I’m deeply concerned about some of these patients getting sick in the next week or two, you haven’t been reading my blog. Many were exposed but did not develop the virus. Many had only a mild clinical course and few risk factors, including age. Many had symptoms that meant they would screen positive for further evaluation for COVID-19, but were actually ultimately due to something else; a bacterial pneumonia, a COVID-19 unrelated COPD exacerbation, migraine headaches, pregnancy. Do I get to count all of them in my ‘COVID-19 treatment’ numbers since I saw them for suspected COVID-19 based on their presenting symptoms? More importantly, these patients self-selected to my clinic by not being ill enough to need to call 911 or present straight to the ER, or by not being elderly enough or having enough medical complications to already live in certain very high-risk settings, like a long term skilled nursing facility, where they would be evaluated by another doctor entirely. If I had placed all of these hundreds of patients on hydroxychloroquine, zinc, and azithromycin, (and if none had adverse events or serious reactions to these medications), their outcomes would have been exactly the same. The only difference would be that they would have purchased and taken unnecessary medications and I would be convinced that I have locked-on to the miracle cure. After that, if any of my patients did die from COVID-19, I would probably be convinced I was still beating the odds.
Dr. Stella Immanuel: (08:21)
I know you’re going to tell me that you treated 20 people, 40 people, and it didn’t work. I’m a true testimony. So I came here to Washington DC to tell America nobody needs to get sick. This virus has a cure. It is called hydroxychloroquine, zinc, and Zithromax. I know you people want to talk about a mask. Hello? You don’t need mask. There is a cure. I know they don’t want to open schools. No, you don’t need people to be locked down. There is prevention and there is a cure.
Do not trust anybody with your medical care who tells you don’t need prevention because you can just do treatment. Please wear a mask.
Dr. Stella Immanuel: (08:48)
And let me tell you something, all you fake doctors out there that tell me, “Yeah. I want a double blinded study.” I just tell you, quit sounding like a computer, double blinded, double blinded. I don’t know whether your chips are malfunctioning, but I’m a real doctor. I have radiologists, we have plastic surgeons, we have neurosurgeons, like Sanjay Gupta saying, “Yeah, it doesn’t work and it causes heart disease.”
I’m a real doctor too and I believe in evidence based medicine. Also, take that all of you radiologists, would-be-plastic-surgeons, and neurosurgeons who did better than me on your boards (you know who you are. Miss you guys); I’m a real doctor!
Dr. Stella Immanuel:
Let me ask you Dr. Sanjay Gupta. Hear me. Have you ever seen a COVID patient? Have you ever treated anybody with hydroxychloroquine and they died from heart disease? When you do, come and talk to me because I sit down in my clinic every day and I see these patients walk in everyday scared to death. I see people driving two, three hours to my clinic because some ER doctor is scared of the Texas board or they’re scared of something, and they will not prescribe medication to these people.
This is clue number three. Just like Dr. Lozano and Dr. Procter, Dr. Immanuel has patients driving across the state to see her because they know she will prescribe these hot-button medications for them even when other doctors wouldn’t. If you don’t understand why this is problematic or how this distorts her treatment numbers, please see my prior posts on those doctors’ claims.
Dr. Stella Immanuel: (09:35)
I tell all of you doctors that are sitting down and watching Americans die. You’re like the good Nazi … the good one, the good Germans that watched Jews get killed and you did not speak up. If they come after me, they threaten me. They’ve threatened to … I mean, I’ve gotten all kinds of threats. Or they’re going to report me to the bots. I say, you know what? I don’t care. I’m not going to let Americans die. And if this is the hill where I get nailed on, I will get nailed on it. I don’t care. You can report me to the bots, you can kill me, you can do whatever, but I’m not going to let Americans die.
I’m choosing to leave this one alone for the most part. Dr. Immanuel has been widely lambasted on social media for holding a number of medical and non-medical beliefs far outside of the norm, some of which are heterodox religious ideas, some of which are conspiracy theories, and some of which are just plain strange. I think her comparison of doctors like myself to Nazi scientists and doctors because we aren’t willing to use unproven medicines and some of the other references in this paragraph hint at that. While I do think that this line of conversation sadly does have some value- it is important to understand if the people we choose to give credence to are reliable sources of truth- I feel that my calling here is to speak to Dr. Immanuel’s arguments, statistics, and scientific interpretations alone.
Dr. Stella Immanuel: (10:09)
And today I’m here to say it, that America, there is a cure for COVID. All this foolishness does not need to happen. There is a cure for COVID. There is a cure for COVID is called hydroxychloroquine. It’s called zinc. It’s called Zithromax. And it is time for the grassroots to wake up and say, “No, we’re not going to take this any longer. We’re not going to die.” Because let me tell you something, when somebody is dead, they are dead. They’re not coming back tomorrow to have an argument. They are not come back tomorrow to discuss the double blinded study and the data. All of you doctors that are waiting for data, if six months down the line you actually found out that this data shows that this medication works, how about your patients that have died? You want a double blinded study where people are dying? It’s unethical. So guys, we don’t need to die. There is a cure for COVID.
This is painful, because she’s absolutely right; dead is dead (although some of us believe that’s not true at all). And if in 6 months I have lost COVID-19 patients and a large, well-controlled, double-blinded placebo controlled study does overturn all the best evidence we have so far and proves that hydroxychloroquine would have saved those patients if I had just given it to everybody who thought they might have the virus or who had certain risk factors or a certain constellation of symptoms, I will be sad that I didn’t use it. I’ll write about it on this blog, and my agony over it will probably come through pretty clearly because I’m not great at hiding that kind of thing. But what I won’t be able to say is “it turns out Dr. Immanuel was right” or “it turns out Dr. Procter was right.” Because recommending a medication that later turns out to be useful based on bad data, misunderstanding statistics, shifting the goalposts of what it means to diagnosis an infection or what constitutes valid evidence, and indiscriminate prescribing designed to bolster my own confirmation bias is still wrong. What’s that saying, something about a blind squirrel is still right twice a day, and we shouldn’t… be blind squirrels… leading the blind? Being right for the wrong reasons is called being lucky (or in the absolute best case scenario, deeply intuitive), and it’s great for you and your patients; it isn’t something anyone can reasonably or ethically follow you in.
How many medications do you take? There are over 20,000 prescription drugs approved by the FDA; unless you take that many, there are probably some out there that might help a symptom or a condition you have; maybe even some that might save your life. We could put you on chemotherapy because you might have cancer. We could put you on daily antibiotics because it might prevent your next urinary tract infection. More to the point, we could treat you with chronic opioids because they have a mechanism for helping your pain, even if your pain is unlikely to have any long-term improvement from them and you run the risk of opioid dependence, a condition I treat every day and have seen ruin lives in ways you wouldn’t believe. We could treat every child who might have an ear infection with antibiotics, regardless of diagnostic standards and the very real risks of antibiotic resistant bacteria (not to mention diarrhea diapers). We could put every flu patient on tamiflu even though it can be a harsh medication and has only limited efficacy in limited clinical scenarios.
No Dr. Immanuel, it is not unethical to refrain from using a medication in a clinical scenario where it has no proven efficacy. This is the philosophy that led to the opioid epidemic and every day leads to polypharmacy, another very real killer of the elderly. We took oaths to first do no harm, and sometimes that means sitting in the tension and anxiety of an unknown future with our patients and admitting, regardless of our own hubris, that we don’t have anything special or prescribable to offer other than our sound advice, sincere compassion, and reliable information. In fact, this is actually a pretty big part of our jobs already.
If 6 months from now (or hopefully sooner) some reliable evidence shows that hydroxychloroquine has a use in specific scenario to treat COVID-19, I will be the first one to prescribe it. Until then, the anecdotal evidence isn’t strong enough, the mechanism of action not surefire enough, and the scientific evidence not promising enough to justify the type of widespread everyone-gets-a-dose treatment these doctors are espousing; and unfortunately, despite her passion and her compassion for her patients, Dr. Immanuel’s clinical evidence, at least as she has shared it here, adds to that data not even at all.
From this point the press conference continued for another half hour. America’s Frontline Doctors is prolific; since this video they have also released additional hour and even three hour long videos. Although I think there are many points from the remainder of the video that could be analyzed, including quite a few I agree with, some that need clarification or explanation, and some that deserve to be debunked, I have to accept my limitations and accept that at this point analyzing the remaining claims is not the most pressing use of my time.
My apologies to anyone who might have been waiting for me to address a specific point in the remainder of the press conference; please do not hesitate to get in contact with me with specific questions, which I may be able to integrate into future posts.
I have deleted the remainder of the transcript since I do not have plans to address the remaining points, but it can be found here and the video can still be found in various places across the internet.