On Monday, during a World Health Organization virtual press briefing, Dr Maria Van Kerkhove issued a statement that seemingly shook our entire understanding of the COVID-19 pandemic. Dr. Van Kerkhove is an Epidemiologist specializing in emerging infectious diseases and has been the technical lead for the WHO COVID-19 response team. The statement, which was immediately picked up by multiple news outlets, was this one:
It still appears to be rare that an asymptomatic individual actually transmits onward.
Dr Maria Van Kerkhove, World Health Organization
Needless to say, the response was immediate, and massive. For months we have been treating every person we interact with, including and especially ourselves, as though we were potential sources of COVID-19, in order to flatten the curve and prevent both a surge of cases and the possibility of our healthcare systems being overwhelmed. We were told, early and often, and with increasing levels of scientific certainty, that it was not enough to simply stay home if you were coughing or had a fever; that we could spread the virus even before we had developed symptoms, or if our symptoms were only very mild, and that the person we spread it to might not be so fortunate. Suddenly, the WHO seemed to be making an about-face.
For those that are exhausted of the caution made necessary by the pandemic, and the associated anxiety (read: all of us) it was welcome, if somewhat annoying, news. For those who have consistently proclaimed the pandemic to be something between an overblown flu being used for political purposes to an actual hoax or planned conspiracy, it was a triumph; even the WHO was saying it wasn’t anything to worry about. But for many of us who have been following emerging evidence, testing methods, contact tracing techniques, and COVID-19 data from around the world since March, it sounded too good to be true.
What we all wanted it to mean.
The idea of asymptomatic transmission, the virus actually being transmitted from a person who does not feel ill, who may not even know they have been exposed, is pretty terrifying. It means that you could, without ever knowing it, be the agent of delivering a deadly pathogen to a loved one; and that you may not ever know you were the one that gave it to them even after the fact. The idea of someone who has never had the virus losing a family member to it, and then finding out months later that they are antibody positive and have thus been a carrier at some point, is heart breaking. For me, it conjures epidemiology computer simulations of faceless grey figures gradually turning red, as the world slowly but surely is overcome.
This is the stuff of nightmares.
If Dr. Van Kerkhove’s statement meant that only those with symptoms could possibly pass along the virus, it would make all the difference in the world. For one thing, it would drastically change our isolation and transmission control strategies, shifting our focus from social (physical) distancing and treating all contacts as possible COVID-19 contacts, to simply monitoring very well for cough and fever and other viral symptoms, like we already do for influenza and other respiratory illnesses. Although it wouldn’t mean the virus was less dangerous, it would mean that exposure to it was somewhat predictable; if we were careful, our biggest risk would be those few bad actors who had symptoms but denied them, and persisted in exposing others.
And yes, it would also mean that many of the experts, epidemiologists, and physicians (including myself) (that’s an oxford comma folks, and I’m definitely only including myself in that last group) had been wrong about both the degree andthe nature of risk to our society. But here’s the thing; we would be fine with that. It would be a big hit to the ego, for sure, and I’d of course have to delete this blog before I applied for my next job, but overall eating crow is an incredibly small price to pay for the assurance of safety for my family and my patients, and for the assurance of a sound strategic path forward in defeating this virus once and for all. As we’ve said all along; every doctor who sounds like an alarmist about COVID-19 also hopes they are wrong. We are the exact people who would be the happiest if it somehow turned out it wasn’t that big of a deal.
It would also mean that somebody had a lot of work to do to figure out how COVID-19 had overwhelmed so many healthcare systems and decimated entire cities and nations. We would need to account for those 404,000 deaths worldwide, a quarter of which have occurred in the United States. If those people were all exposed by individuals with definite and likely identifiable symptoms, we would need to figure out why we had failed so badly at fighting such a straightforward viral disease.
Always go to the source.
When I first read the headlines and articles, I was cautiously optimistic; but very cautiously. This defied what we had believed all along, and it defied most of what we know about the way that respiratory viruses spread. It didn’t make sense with the transmission patterns we have seen and the reported K value of the virus for it to only spread through fully symptomatic patients. It also conflicted with two recent studies from China and Singapore that seemed to indicate that transmission does in fact occur, and at a high rate, from patients without any respiratory or viral symptoms. These studies reached similar conclusions despite very different methodologies, which is always more convincing than reaching the same conclusion with the same method or data set. The Singapore study concluded,
“The evidence of presymptomatic transmission in Singapore, in combination with evidence from other studies, supports the likelihood that viral shedding can occur in the absence of symptoms and before symptom onset. “
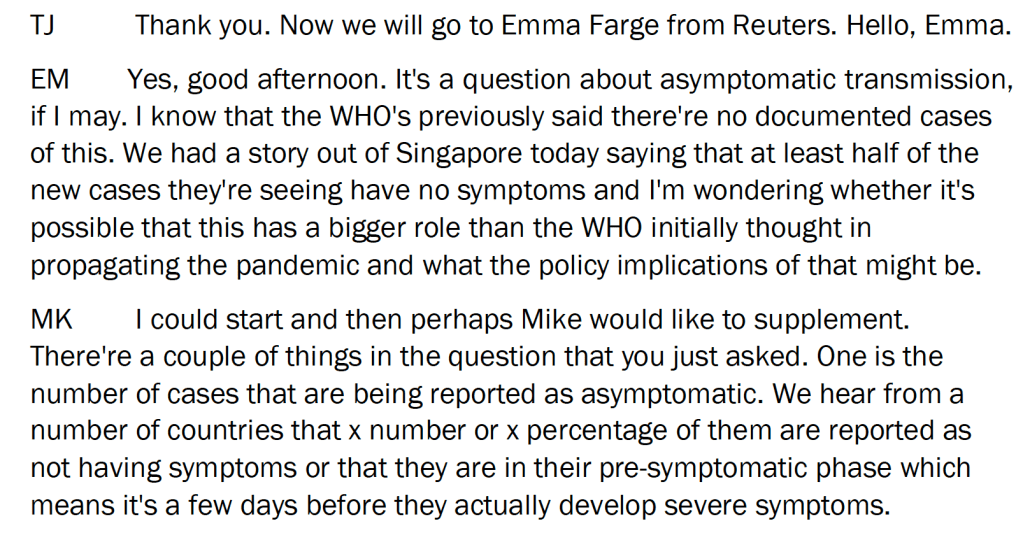
Still, I was hopeful. When I reviewed those studies there had been some assumptions and a few minor (and one major) methodological issues I wasn’t exactly comfortable with, and at any rate those studies were published back in April and we have learned an awful lot about SARS-CoV-2 since that time. I assumed that Dr. Van Kerkhove and the WHO were working from the most up-to-date data, so I did what I always advise people to do when evaluating emerging medical information; I went directly to the source. It’s a bit long but it’s worth reading Dr. Van Kerkhove’s entire answer and not just the excerpts that have been used in the various articles above.
Now, I know what you are asking; if these statements were confusing, why didn’t I ask her to clarify? Well, actually… that was a different TJ altogether.
Asymptomatic vs. Presymptomatic vs. Minimally Symptomatic.
There is one major component of Dr. Van Kerkhove’s answer that has been lost from most of the majors news stories and social media posts. Medicine and public health are subtle and detail heavy sciences, and it is unfortunate but perhaps unsurprising that the nuances of the above statement were lost, and that major news outlets reported “WHO says no asymptomatic spread,” when the real answer is much more restrained.
Dr. Van Kerkhove spends a considerable part of her answer specifically delineating between asymptomatic, presymptomatic, and minimally symptomatic cases, and it’s hard to put too fine a point on this distinction.
Asymptomatic cases are people who have been exposed to the virus, and it has reproduced itself within their bodies at a high enough rate that it becomes detectable by our testing methods; either it is present in their blood stream at a detectable rate at some point in time (they have a positive PCR test) or they have developed an immune response that can be detected after the fact (they have a positive antibody test). They have had the virus. However, they have never at any point had any symptoms they can identify; no day of fever, no fatigue, no cough, no ‘I thought I caught something but it got better’; they are fully non-symptomatic.
Presymptomatic cases are people who meet all of the above criteria at a certain point in time, but will eventually develop symptoms from the virus. Unless they are followed very closely, it is impossible to distinguish them from asymptomatic cases.
Minimally Symptomatic cases are people who have the virus but develop only very mild symptoms, or symptoms not as commonly associated with the COVID-19 syndrome. This is very, very challenging from both a diagnostic and an epidemiological standpoint. Many people have chronic cough, allergy symptoms, or shortness of breath related to chronic medical issues. Figuring out whether these symptoms worsened at a certain time that coincides with their SARS-CoV-2 infection, and that the infection was actually the cause, is nearly impossible, yet the way these cases are treated has huge implications in the way we understand data on asymptomatic transmission.
If you are reading this and thinking that these distinctions seem a little murky and difficult to unravel, you aren’t wrong. I don’t do contact tracing directly, but the idea of clearly delineating, over the phone and after the fact, between these three situations seems like a nightmare. Yet our understanding of the spread of this virus, and thus our risk to one another, hinges strongly on public health workers involved in contact tracing categorizing people into these groups with a high degree of fidelity. It is sound epidemiological work and is necessary and important, but realizing how much subtlety and difficulty is involved should make us wary of any overly optimistic (and yes, overly pessimistic as well) statements about risk based on such data. This is why it is so important that this data is compared to research on modes of transmission, viral shedding, and viral load in asymptomatic patients, and that all of those types of evidence be weighed together very carefully.
When misspeaking and misunderstanding becomes medical misinformation.
So the substance of Dr. Van Kerkhove’s answer is that unpublished data from an unknown number of countries, relying on methodology that is hardly foolproof (but may be the best we have available), seems to show that transmission of SARS-CoV-2, from the subset of people who will never develop even very mild symptoms, is rare. It is good news, but it is an incredibly measured response when properly understood, and the phrasing left it alarmingly ripe for misunderstanding. As soon as media outlets picked up this story it was clear that the original intent had not been understood, and that widespread confusion, vexation, and misinformation would result. On Tuesday, Dr. Van Kerkhove and the WHO attempted to clarify the statement.
“The majority of transmission that we know about is that people who have symptoms transmit the virus to other people through infectious droplets. But there are a subset of people who don’t develop symptoms, and to truly understand how many people don’t have symptoms, we don’t actually have that answer yet.”
Dr. Maria Van Kerkhove
But as you might have suspected, the damage was done. One of the most alarming things about misinformation in general, and medical misinformation in particular, is how those who share it are seemingly impervious to correction. They will choose to continue to believe information that has been demonstrated to be impossible, videos that have been proven to be a hoax, and now even statements that have been immediately retracted and clarified by those who uttered them. When confronted with the retraction, I have seen people essentially say, “well I believe it anyway.” Even today we are seeing people spread the original articles and double-down on the claim that asymptomatic spread (meaning, in their vernacular, ‘anyone without cough and fever’) is not possible, and that the WHO has finally confessed their complicity in this global conspiracy.
So… Is asymptomatic transmission still a thing?
I had hoped that we would be presented with the data Dr. Van Kerkhove had reviewed indicating the rarity of asymptomatic transmission. We have not seen that information yet, but other studies have reviewed available contact tracing data and arrived at a very different conclusion. Two recent studies were published on asymptomatic and minimally symptomatic spread within the last two weeks, one on May 28th in the journal of the Infectious Disease Society of America, and one on June 3rd in Annals of Internal Medicine. They offered similar conclusions:
“This review summarizes evidence that SARS-CoV-2 transmission is not only possible but likely highest during pre-symptomatic and asymptomatic phases.”
“The early data that we have assembled on the prevalence of asymptomatic SARS-CoV-2 infection suggest that this is a significant factor in the rapid progression of the COVID-19 pandemic. Medical practice and public health measures should be modified to address this challenge.”
Both studies supported the high viral load and infectivity of presymptomatic individuals who would later go on to develop symptoms, which had been found in the China and Singapore studies in April. Both established, firmly, that transmission from asymptomatic individuals who would not go on to develop symptoms does in fact occur. They both analyzed the limitations of their methodologies and data sets, and explored the difficulties in distinguishing between asymptomatic, presymptomatic, and minimally symptomatic patients. Hence they both appropriately shied away from assigning any firm degree of risk or responsibility for transmission to asymptomatic spread of the virus. Unfortunately, we do not have reliable numbers for how many people are getting the virus from someone who will never know they have it. More studies are needed, but it seems clear that asymptomatic transmission is here to stay, at least as long as COVID-19 is.
Over the weekend I had several viral medical misinformation videos sent to me, but I chose not to focus an entire essay on any of them for various reasons. One was a nurse speaking at a re-opening rally in Raleigh, North Carolina about empty hospital rooms and postponed surgeries. We’ve talked about healthcare systems being slower in pre-surge areas due to mitigation efforts a good bit in prior blog posts, and since the actual content of her comments were relatively straightforward and could be as easily interpreted as praise for social distancing measures as criticism, I decided it didn’t necessitate and entire post. Another was an interview with Dr. Jeffrey Barke, a concierge medicine doctor in Orange County, California who had recently spoken at a re-opening rally there. While there were a few medical issues he raised that deserved some response (bringing up hydroxychloroquine again, failing to distinguish between the medical realities in pre-surge areas vs. those more heavily effected), his comments were primarily politically rather than medically oriented. Finally, there was an immediately debunked video of Bill Gates briefing the CIA on his plan to release a respiratory virus, and then give a vaccine for it that wouldactually modify people’s brains tomake them hate religion. Which, I mean, come on America. Really?
Instead, what caught my interest is the following letter to President Trump, signed by 600 doctors.
Page 1 Page 2
The remaining 8 pages are a collection of signatures from, presumably, over 600 other doctors. The letter itself was written by Dr. Simone Gold, MD, an ER trained Physician in California who now does concierge medicine as well. It is part of her A Doctor A Day campaign and has been featured on Forbes, Fox News, Breitbart, etc. and circulated widely on the internet. Today I would like to focus on the parts of this letter I agree with, for there is much to agree with, and then explain the one great error I believe Dr. Simone is making. But first, we should address a few preliminaries.
Signed by 600 Doctors
When reading a letter like this, the temptation is to get dragged into those last 8 pages and try to address the motivations, credentials, and biases of the doctors signing. Certainly, with 600 signatures this becomes an investigatory nightmare, but I believe it would be a profitless endeavor even with a more manageable list of names. When a doctor shares blatantly erroneous data, like Dr. Erickson and Dr. Massihi, or a scientist promotes false claims and conspiracy theories like Dr. Mikovits, a closer examination of motives is warranted. But unlike those viral videos, there is as far as I can tell no false medical information contained in this letter. This is a position statement, and while some individual co-signers may have their own political or financial motivations, I earnestly believe it is best to take the stated motivation of advocacy for individual patients and our population as a whole at face value.
That said, I believe we can make some general observations, and to do so I will bring you thought my own process when confronted with this list of names.
First, I checked to make sure my own name wasn’t listed. I don’t remember signing anything like this and don’t believe I would have, but arguing against the letter and then finding out my name was on it would be the most embarrassing (and funniest) complication to my opposition that I could think of.
Whew, close one.
Second, I googled a few of the names. Now nearly 3 months into fighting against medical misinformation in a more formal and deliberate way, I have learned to be surprised by less. I didn’t think anyone would make up 600 doctors to support their letter, but wanted to make sure. I only chose a handful at random, but they were all real life people.
Third, I read about a few of them. The first doctor I looked up had his medical license revoked 20 years ago. Oomph, rough start. But the next practices Family Medicine in California, another is an Ophthalmologist who does LASIK eye surgery, and the one after that is an Emergency Medicine doctor in Connecticut. As I googled a dozen or so names I did not find anybody practicing Emergency or Critical Care medicine in New York, and didn’t really expect to (though maybe there are a handful on this list); but that first doctor who isn’t allowed to practice medicine anymore seems to have been a funny coincidence, and overall it seems that these are, by and large, real practicing Physicians in various specialties around the country. I can in no way vouch for or against their personal experiences with COVID-19, their level of experience or skill as clinicians, or their political views.
Finally, I looked over the list itself and reflected on the numbers. A few Dentists and PhD’s, a few people listed without any credentials, but mainly MD’s and DO’s; Doctors of Medicine. I made a quick scan to make sure there wasn’t anybody I knew, which could get awkward. There are over a million doctors in the United States, as Dr. Gold’s website points out, and here we have 600 names. No doubt there are many, many more who would sign such a letter. If you are trying to google individual names or even just scrolling through, it seems overwhelming; but it’s actually a relatively small group. I am part of one COVID-19 Physician and NP/PA group on Facebook with 150 thousand members, and a Critical Care COVID-19 group with 33 thousand members. The discussions there are focused on treating and preventing the illness, the most recent studies, transmission control strategies, and review of treatment protocols. While many of us are also very concerned about the secondary effects of the virus, such as the complications of isolation and distancing, I have seen no posts and very few comments saying that the whole thing has been overblown. I could not say how many in those groups would or would not sign the letter above, but the idea I am trying to get across is that 600 doctors in a country the size of the US is a fairly small sample. When taken as a whole this letter really does seem to represent a minority opinion, as the website itself alludes to.
A Doctor A Day
Dr. Gold’s personal website, drsimonegold.com (can you believe she used her name as her website url? The arrogance), currently redirects to A Doctor A Day, which almost -but not quite- admits to it’s goal of offering a minority, dissenting opinion of the importance of mitigation strategies in fighting COVID-19. It begins with the following text:
The numbers here send a bit of a mixed message, don’t they? On the one hand, they clearly would like to contrast “ONE opinion” with both the million licensed physicians and the thousands of physicians who have something to tell you. But a straightforward reading is maybe too honest by half; there are nearly a million physicians who seem to be expressing one opinion, that COVID-19 is very dangerous (that’s called a consensus); but thousands of doctors want to give a second opinion, that it isn’t dangerous enough to justify the steps we’ve taken. I’m being quite facetious here, of course, but I do think that they are trying to have their cake and eat it to by implying both that the views of doctors are varied and nuanced, and that the doctors who agree with them are thinking independently while the rest of us are towing the party line and sharing “just one opinion.”
That’s why the second opinion part is what really gets to me, because it so clearly implies that the views expressed by A Doctor A Day are not also being expressed by other physicians who nonetheless support mitigation measures. And that simply isn’t the case. I’ve yet to meet a doctor who isn’t aware of, concerned about, and talking about the potential for secondary harms due to social distancing and quarantine strategies, and the ones I know are working very hard to mitigate those harms. I’ve personally been talking and writing about it since early March. In fact, recognizing how much more vulnerable our patients are in the midst of a pandemic has been a core reason for the mitigation and social distancing measures since day one, because an overwhelmed healthcare system has evenless ability to care for patients with chronic illnesses and mental health conditions than a reduced capacity healthcare system.
March 16thMarch 14th
The A Doctor A Day campaign is promoting a narrative that says the many, many physicians and other healthcare workers encouraging ongoing social distancing and quarantine measures and extreme caution with reopening have simply not thought of, or have refused to acknowledge, the difficulties that those measures create for our patients and our communities. But their second opinion is already contained in the first; it has been weighed carefully, it has been felt deeply, and in the face of a hundred thousand lives lost and who knows how many million in the balance, most of us have found the danger still too great to abandon our fight against the virus. The opposite cannot be said; the doctors vocally forwarding this alternative perspective have been strangely reticent to acknowledge how bad the virus really is, sometimes even leaning on ‘inflated death numbers’ and other misinformation to lessen the reality of what we are facing.
The Videos
Dr. Scott Barbour M.D. you have GOT to turn your camera to landscape…
Besides the homepage and the letter, the main content is a series of videos featuring interviews with Physicians who talk about the damage and potential damage being done by shelter-in-place orders and social distancing. They run about 5-10 minutes long each and so far there are four, though the link for one seems to be broken. Interestingly, some of the interviews are conducted by Dr. Jeff Barke, who seems to be a partner on the project. There are some problematic moments, mostly in the form of leading questions such as when Dr. Gold asks one Physician how he kept his office open when ‘we have heard from around the country that most patients can’t come see their doctor’, without offering any evidence that this is the case, or when Dr. Barke asks a Cardiologist about caring for Congestive Heart Failure patients when ‘they can’t get Echocardiograms’, which also doesn’t seem to be the case. But these doctors being interviewed sort of hedge on those questions, and mostly they spend their time expressing their concern about the potential negative health effects of mitigation strategies on their patients, like most of us would, and the things their clinics are doing to compensate. I think a video series like this invites comparison. Consider this video from Dr. Mike, who does a handsomer and more successful YouTube version of what I am trying to do on this blog.
The most striking thing to me about these videos is that the doctors from both sidesof this discussion seem to be genuinely and primarily concerned about the well-being of their patients. Which shouldn’t be a surprise if you know many physicians. The second thing I notice is that it doesn’t seem hard to get doctors to tell you about their experiences during the COVID-19 pandemic; a contest of who can make the most videos or recruit the most signatures isn’t likely to be helpful, which is why it’s important we look closely at the arguments themselves.
The Letter: What I Agree With
I wrote about treating COVID-19 like a nation-wide mass casualty event back in March, and in many ways I agree with Dr. Gold’s concerns. Faced with such an overwhelming medical reality, one of our first goals has to be to ensure that our vulnerable patients “do not deteriorate a level.” As a primary care physician caring for patients who often have limited access to specialists and treatments at baseline, I and my patients have had to be especially deliberate and strategic about caring for their conditions during COVID-19 while the medical system is even more challenging to navigate. Many of my patients lived pre-COVID-19 in what Dr. Gold describes as ‘triage level red’; poor or no access to cancer screening, unable to afford dental care, not having access to Psychiatry for ongoing and often overwhelming mental health issues. The list could go on; patients with seizures who can’t see a neurologist, those with CHF who can’t get an Echo, not because they aren’t being scheduled right now, but because they cost $2,000. Diabetics whose control has worsened because their insulin prices suddenly skyrocketed in the name of profits. If these doctors are going to advocate for patients who could normally have these services done but might not now because of COVID-19, they should also be advocating for the patients who have never had access to these services and thus live and die in triage level red. Maybe some of them are advocating for those patients; but they all should be, and if they are willing to sign this letter to the president out of that concern then all 600 of their signatures should be on the next petition to improve healthcare access for all.
But COVID-19 is the reality right now, and regardless of the individual examples (it is a hard sell to prove, for instance, that a hip surgery would have reduced someone’s risk of a pulmonary embolism), I have seen many situations similar to the ones they mention in the letter, and some have indeed been made worse by COVID-19; both by fear of the very dangerous virus itself and by the disruptions to ‘normal’ life rhythms and support structures, financial difficulties, and loss of community. I do not have to imagine those stories from the initials and brief vignettes in their letter; I have the names and faces of all of my own.
We all do. Every physician and clinic I know is involved in combatting this, not to mention ministers and priests, social workers, mental health workers, and teachers. I feel like a broken record when over and over again I have to share the changes my own clinic has made to create safe access for patients; seeing patients outside in their vehicles to decrease transmission risk, rapidly building and implementing telephone and video visits without any precedent or prior infrastructure for using those tools, designating COVID-19 testing and treatment sites to keep sick patients and vulnerable patients from putting one another at risk, and all of the individual and corporate work and stress that goes into examining and upending every single protocol and procedure you have used for years. We do all of this because as hard as we worked to ‘flatten the curve’ in March and April, and as loud as are being about preventing a second surge now, we are also worried about that third surge, and are working hard now to flatten that curve, too. The balance of each of those threats has to be weighed in deciding when and how to return to our ‘normal’ routines, if such a thing can even exist again.
Mass Casualty Event
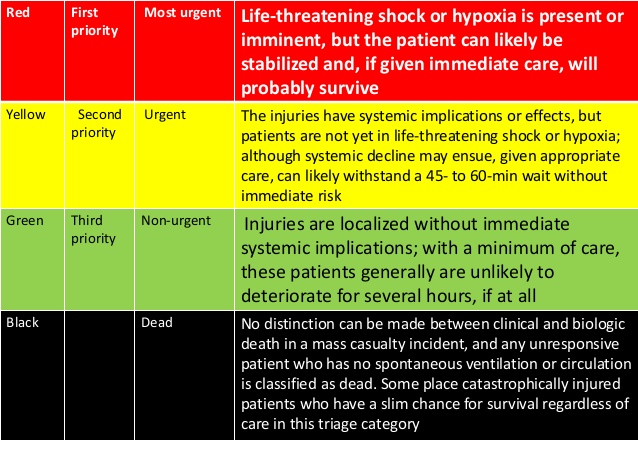
Finally, I want to return to Dr. Gold’s central analogy of COVID-19 as a Mass Casualty Event. A mass casualty event is a situation where so many are injured that the available resources could not possibly care for everyone who needs care. This is the Oklahoma City Bombing, or 9/11. Dr. Gold is right, that in a ‘mass cas’ the most important first step in caring for the injured (besides safety, of course), is an effective triage system. She talks about the color-coding system we use for these types of events, and I think it’s worth studying for a few moments. I’ve provided a couple of different representations, because I want you to understand just how different a mass casualty event is from the normal way we practice medicine.
To the untrained eye, it looks like these diagrams are used to train doctors and other medical professionals to triage patients. But they aren’t. Triaging patients is not a difficult concept, but it does take some time to master. Sorting out those that need immediate attention from those who can safely wait is a skill that is taught early and honed daily. You do this in every context of medicine almost all day long. It is most obvious in the hospital and the ER, when your visit with a sweet older lady recovering from pneumonia is suddenly cut short by sudden shouts from down the hall or a Code Blue over the speaker. But it also happens in clinic, when you hear the crash of a walker in the waiting room or notice that your 2:45 PM “Arthritis recheck” is now listed as having a chief complaint of “Chest Pain,” or your 9:15 didn’t come to clinic even though you know he’s been severely depressed. We triage in our minds constantly, and Mass Casualty is a specialized enough field that our training in it typically comes after we have alreadybeen triaging in our minds constantly for years.
These tables are not for training us how to Triage. They are for re-training us how to Triage in a way we are very, very uncomfortable with. They are, in a way, un-training us.
Think about those categories, and what they mean. Green means that person gets none of my time or attention; even with injuries, even having suffered trauma. People I might otherwise spend an hour with talking through their experience and tending their wounds, I deliberately re-route and ignore to get to sicker patients. Yellow is someone who has urgent needs, who probably needs care within the hour. In the ED this would be considered a very ill patient, and someone who is going to get immediate attention; in a mass cas event, they are set to the side because the sicker, red patients need attention now, and the resources are simply too limited. Finally, think about my examples from the hospital, and look back at those tables one more time. Notice black: “Obvious death,” “Non-survivable injury,” “Cardiac Arrest.” Normally if you are running through your continuous mental triage and suddenly find a patient in cardiac arrest, requiring chest compressions, intubation, and defibrillation, that patient becomes your highest priority. Your time and resources are devoted to that individual for as long as it takes, as long as there is a chance. In a Mass Casualty Event, those patients are left for dead.
This is why we do specialized training in mass casualty; this is why we have to study and internalize and accept a triage system that is alien and even repulsive to our oath as physicians and every carefully fine-tuned impulse of our professional judgement. Because the idea of allowing an untimely death that might have been prevented is so terrible to us that it requires a drastic shift, on some level, away from how we’ve trained and even who we are as physicians.
The physicians who wrote this letter are advocating that life return to normal. They are advocating for this from a noble enough sentiment; concern for the well-being of those who they consider to be at Red, Yellow, and Green levels of risk right now. But just as in every mass casualty, their call to shift our standard of care and give our full attention to those groups by abandoning transmission reduction strategies necessitates allowing some to die who might otherwise have lived. This ‘black’ group that should be forsaken, who in the letter’s own words “require too many resources to save”, are the excess dead from COVID-19, who might have been spared by “reopening” with more caution, more national sacrifice, more people-centered policies, and more patience.
Nowhere in their letter do they mention the 100,000 we have already lost, or the thousands more still fighting for their lives. Nowhere in their letter do they mention the suffering of those families, the sacrifices and risk of their caregivers, or the fear of those exposed. Nowhere do they mention the mental health burden inflicted by the virus itself on all those who come in contact with it. All of these should be crucial factors in our decisions about when and how to decrease mitigation efforts. But if you are going to lead a mass casualty response, I guess you have to be willing to walk past some who are dying and force yourself to live with the fact that you had the skills and the tools to save them, but didn’t. The majority of physicians, myself among them, seem to think that we haven’t reached that point yet; that as a society we can continue to protect one another and the vulnerable among us from COVID-19 and still devote time and energy to keeping others from ‘deteriorating a level’ while we fight it, by rethinking the ways we deliver care and support our patients and communities. Maybe that’s typical physician hubris, and maybe the second opinion offered by Dr. Gold and her colleagues is the only real option; to shift our focus to the ‘survivors’ even if it means giving this virus another 100,000 lives, or more. But I don’t believe that’s where we are, and I know it isn’t a decision we can make without counting the unimaginable costs very, very carefully.
A friend sent this video my way along with some questions from a family member. The questions were of a specific and limited scope, which I deeply appreciate, and I hope I will have answered them satisfactorily within this post. The video is of Dr. Ivette Lozano, MD, who is general surgery trained and now runs a solo general medicine practice in Dallas, an hour and a half North of where I work; I am not sure whether she also works in surgical and/or hospital settings, as this information is not available from her website and does not come up in the video. She was speaking at the Set Texas Free Rally in Dallas on May 9th. Dr. Lozano has done numerous interviews and television appearances during the COVID-19 crisis and has these collected on her practice website; though I will keep commentary focused mainly on the video that was sent to me, watching her other interviews has been helpful in understanding her experiences and position more clearly, and I will refer to those at certain points as well. I do not feel that it would be appropriate for me to link to her practice website directly from a blog post that seeks to discredit and contradict so many of her claims, but if you wish to see her other interviews they seem to be available on YouTube.
I’d like to point out two things about this video right from the start. First, unlike the personal youtube videos we have looked at so far and and the extensively produced PlanDemic documentary, Dr. Lozano is speaking in a live, outdoor forum without the option of editing or multiple takes. She speaks for 13 minutes and seems to consult her notes very infrequently, if at all. That in itself is an impressive feat. I’ve spoken at this type of gathering a few times as a professional, sometimes on very little notice, and I honestly can’t remember half the stuff I said afterwards; it’s just not the most conducive to an academic discussion. With that in mind, if Dr. Lozano does ere in some finer details or specifics, I think a measure of grace is called for; in such a setting, it would be at least as likely that such an error were due to the challenges of that context and not to design.
The second is that Dr. Lozano states multiple times (and we will examine these instances more closely as we come to them) that she is speaking from her own personal experiences. In common experience this tends to serve as a rebuff to any attempts at correction or argument. I do not mean that this is Dr. Lozano’s intent; I only mean that we need to point this out now to preempt any blanket objection to a thorough evaluation of her claims with such phrases as, “well she is sharing her own experiences, so you can’t argue against that with statistics or outside information. She is just telling her story.” In scientific pursuits, and in her role as a physician, her statement that she is relying only on her own experiences should properly be understood as her ceding that her evidence, while compelling to her personally, is in fact anecdotal; that is, based on a small sample size that has not been studied rigorously and is not likely to represent an entire population. Dr. Lozano, as a clinician and scientist, would no doubt understand this.
Anecdotal evidence is important in medicine. It serves as a jumping off point for examining trends and leading to more rigorous research, and as an anchor for contextualizing results and treatment guidelines. In absence of anything better, we rely on our own limited experiences in treating patients; but the principles of evidence based medicine also dictate that, as scientists, we rely on stronger forms of evidence when they are available. If that evidence seems to contradict what we ourselves have experienced, that is reason to both examine the evidence more carefully, and to reflect on our own clinical experiences with a greater degree of scrutiny and honesty. Most often there are factors at play that our limited experiences and volume of data simply cannot reveal, and once we account for these our own experiences really do harmonize with the evidence after all. In fact, it’s fair to say that, to a large degree, what we call high quality evidence is really just the experiences of many, many physicians and patients aggregated and then evaluated rigorously; we ignore the experiences of many in favor of our own individual narratives only at great peril to ourselves and our patients.
So, as we look at these claims, please do not fall into the trap of thinking that as personal experience her claims are exempt from contestation. That is a legitimate and important way to interact with individuals in a great many contexts, and listening to people’s stories without judgement is a vital part of what I do every day as a physician; but it is not the way either Dr. Lozano or myself have been trained to think of medical data.
00:18 “I am currently treating COVID patients in my office.”
I am, too. It is important when we talk about our own anecdotal experiences that we at least give some idea of volume. I have interacted with only a few COVID-19 + patients; our county and city has had a blissfully small burden of disease from this virus and has not yet hit anything like a surge. Dallas, a much larger metropolitan area, has been hit harder, and I would readily believe that Dr. Lozano has seen more COVID-19 patients than I have personally; though she does not here give an indication of the number of cases she has personally treated. Yet, Texas also has had relatively few cases, and so both of our experiences would pale in comparison to those of clinicians in New York, Wuhan China, Italy, Spain, etc. We need to have the humility, as doctors, to recognize that our own small samples cannot lead to definitive clinical data on their own.
00:25 – 1:23 “Let’s start with some simple numbers.”
Populations:
330 million in the US
29 million in the State of Texas
2 million people in Dallas
Deaths:
Dallas: 111
Dr. Lozano: “When you see those numbers it kind of shocks you, that we could stop society for one hundred and eleven deaths.”
Dr. Lozano
So here is my first objection. The Number of deaths in Dallas County, 111 (now 145), has nothing to do with two things. First, it has nothing to do with the populations of either the entire United States or of the State of Texas. If you want to include those numbers, your data set would look something like this:
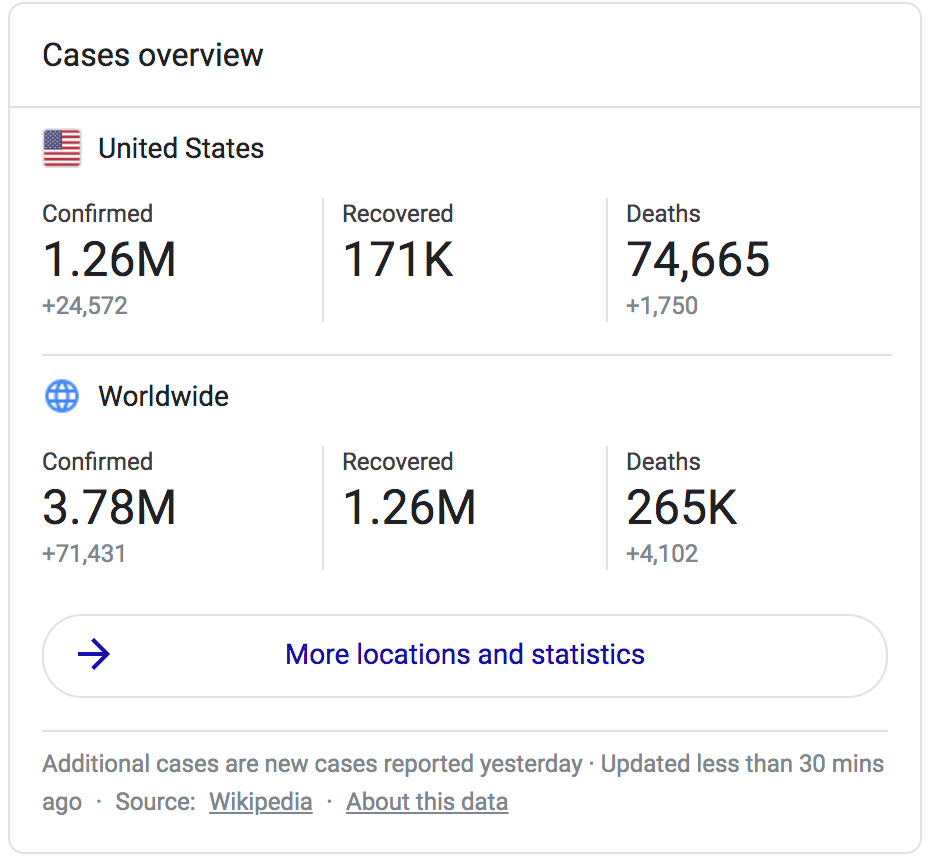
US
Population 330 million
89,932 Deaths from COVID-19
Texas
Population 29 million
1,336 Deaths from COVID-19
Dallas
Population 2 million
111 Deaths from COVID-19
If you are not going to include the number of deaths (underestimated though they may be) in the US and Texas, why include those populations? I believe it’s simply to make the 111 deaths in Dallas seem small in comparison. I could do this in Waco, too; I could stand up at a rally and say “the population of the US is 330 million, and there are 257 thousand people in McLennan Country. We’ve only had 4 deaths. Are we really going to shut down all of society for 4 deaths?” It sounds pretty silly doesn’t it, to invoke that 330 million people without mentioning the 90 thousand lives lost among them?
Now, maybe it sounds like I am splitting hairs, but this is important; the reason that we shouldn’t invoke population numbers detached from death numbers is because the 111 deaths in Dallas also has nothing to do with shutting down Dallas. Think about that for a moment. Cities, States, and Nations that were not hit early by the pandemic have had the privilege of developing their response based on the impact in other places. Shutting down Dallas wasn’t based on 111 people in Dallas losing their lives to COVID-19; it was based on over 15,000 deaths in New York, 27,000 deaths in England, and 32,000 deaths in Italy. It was based on the recognition of what this virus can do to a city or a region, particularly once the healthcare infrastructure is overwhelmed. In fact, in saying that Dallas was shutdown because of only 111 deaths, she is exactly reversing the logical relationship between those ideas; the reality is that there have likely only been 111 deaths because Dallas was shutdown.
Dr. Lozano goes on, “here is how it is notified to you:”
27,000 Positive Covid Tests (??? but probably Texas)
3,000 Recovered (???)
111 Dead (Dallas)
“If 3,000 have recovered, from 127,000 (???) positive tests, that’s 124,000 that have recovered.”
Now it’s clear that Dr. Lozano misspeaks here, either with the 27,000 or the 127,000 above; please remember, she is speaking in a very challenging format and such things happen. However, I honestly cannot tell which is the statistic she intended. Looking back at data from May 9th, Texas had around 37,000 positive COVID-19 cases and 1049 deaths, but listed 19,000 as recovered, not 3,000. Dallas had 111 deaths but to date has only had about 6,000 confirmed cases total, and the US was already in the millions of cases by that time. So, without knowing where her numbers have come from, it’s a bit hard for me to fully examined the claims she is making, but we can safely make at least three observations.
First, she is now directly comparing the number of cases in Texas (the 27,000 above; I cannot imagine where else this number could have come from) to the number of deaths in Dallas only, without mentioning the number of cases in Dallas at all. This is deceitful use of statistics and I sincerely hope it was accidental. Second, her point seems to be that the public is being lied to about the number of cases that are recovered; “27,000 cases, only 3,000 recovered.” But this is not the case; at the time of her speech, official data placed those numbers at 37,000 cases and 19,000 recovered. Third, her final conclusion (here she misspeaks again but her intent is clear) that the number of cases minus the number of deaths equals the number of recoveries is erroneous both because we do not yet know the long term ramifications of the disease, and more to the point, because there are still over a million people with the illness in the US who have not yet recovered. Most of them are at home under close observation and follow-up, but many are fighting for their lives in the ICU and are by no means ‘out of the woods’; some of these people are in the ICU in Texas, and we cannot discount their struggle and the suffering and danger they are still facing. Some will still die, despite the best efforts of their doctors and nurses.
1:23 “I don’t want to bring statistics from other physicians because there is always someone on the Left who wants to contradict me.”
This is the portion of the video where Dr. Lozano begins to speak about her personal experiences, but I want to spend one more moment on this very troubling statement. The politicization of COVID-19 within the medical field is largely a false narrative, and not a particularly coherent one. We’ve talked about this a lot on this blog, on multiple occasions, but basically the conspiracy theorists would like you take any doctors you happen to know and trust, or who share their conspiracy theory, and put them in the “one of the good ones” box; the few honest doctors fighting for the truth. All the rest of us, even if we happen to share your background or faith or even political leanings, are to be put in the “part of the system” box and seen as either infamous conspirators or unwitting patsies. We are, so they argue, inflating death numbers, scamming medicare, and lying to the public in order to… do… something. This part isn’t really clear, you see. Despite the vast scope of different political allegiances, backgrounds, economic views, and personal convictions among doctors, we are all somehow part of a conspiracy to destroy the economy, embarrass Donald Trump, bring about a totalitarian police state, enact socialism, etc. Despite many docs I know getting all of their news from Fox, despite some being close to retirement and watching their 401k’s like hawks, despite many having voted for Trump and planning to again, despite the fact that we are not a monolith. Despite the fact that we have had to work extra hard to take care of our patients in the midst of a pandemic, and the fact that many of us have gotten sick, and some have died, doing so. Despite the fact that, a few minutes later, most conspiracy theorists will point to empty ER’s and closing doctor’s offices in non-surge areas as a sign of the economic injury being done by mitigation measures, their conspiracy theories still call for those doctors struggling the most financially to be a part of a conspiracy to propagate the COVID-19 myth. It’s all rather silly, I’m afraid.
Which is why it is so alarming to see Dr. Lozano adopting it here. What she is saying is that she is only willing to rely on her own anecdotal evidence in talking about and treating COVID-19 because she believes that the experiences of her colleagues and higher quality data from research hospitalsaround the globe are skewed by a Leftist political agenda. This is a very, very dangerous way to practice medicine. At best, Dr. Lozano knows her audience and is willing to let them believe in these conspiracy theories in spite of her knowledge of the way medicine actually works, and the devotion that the overwhelming majority of doctors have to both veracity and the health of their patients regardless of their own political leanings. At worst, she has come to believe in this perverse and pessimistic view of physicians herself. My fear is that this perspective ultimately leads to practicing ‘lone wolf’ medicine detached from evidence, the insights and experiences of peers, and the commiseration and accountability that come from serving within this ancient and altruistic profession.
But because this Southern, Homeschooled, Eagle Scout, 4-wheeler-riding (is that still a conservative credential?) future-missionary-doctor has seen the compassion, the integrity, and the seemingly endless self-sacrifice of fellow physicians from every walk of life and all parts of political spectrum time and time again, I cannot be so quick to attribute to them nefarious political motivations capable of overwhelming their commitment to their calling and Oath. So when discussing Dr. Lozano’s anecdotal evidence, I will be relying on something more substantial than just my own.
1:48-2:05 Discussion of Symptoms
Here Dr. Lozano is discussing the patients with COVID-19 she has seen in clinic. I only point this out to note two things moving forward; first, she does not give us the number of patients she has actually seen in clinic who have the diagnosis. Second, her description of symptoms is interesting. She describes fever, but only fever at nighttime. She describes cough, but only with deep breaths. These are very specific qualifiers and do not exactly match what is known from observations of millions of cases of COVID-19 around the world. Many patients have cough, but not necessary only with deep breathing. Many patients have fever, but not necessarily only at nighttime. To me this suggests that Dr. Lozano may have seen a relatively small number of COVID-19 patients, because there does not seem to be much variability in the presentations she has encountered. It also illustrates the danger of relying on anecdotal evidence alone; once we have cemented a narrative that says this disease will always act like I have personally seen it act before, we put ourselves at risk of delaying the proper diagnosis or missing it entirely. We must learn from each other.
2:06 “These patients are afraid.”
This is true. One of the most important tasks we’ve had as physicians, and really as an entire healthcare field, has been to speak to the fears of our patients in the face of this very dangerous pandemic and help them navigate their medical and mental health needs with safety and confidence. This is an important part of our conversations with patients on every level, from individual encounters to entire populations. Every patient I see who has been exposed to the virus or who has symptoms that might be consistent with COVID-19 needs both reassurance and anticipatory guidance; they need to know what happens next, how to stay safe and keep their loved ones safe, and when they need to seek additional care. Our clinic system has instituted countless measures both to support our COVID-19 patients and to ensure that our patients know they can be safely seen for their chronic conditions as well, from telemedicine systems being built in a matter of weeks to patients being seen in their vehicles so they don’t have to enter into healthcare spaces, and a thousand small steps that probably go unnoticed but reduce our patients’ potential of being exposed to the virus. As physicians, we must combat fear with our compassion and the trust we have built with our patients; never with minimizing their concerns or spreading misinformation.
But Dr. Lozano then goes a step further. At 2:25 she states that the patients who are coming to see her for COVID-19 symptoms are being turned away from the emergency room.She says they are being sent home if they have a fever and told to quarantine, and that during that time they infect their families. She says that doctors are closing their doors and implementing telemedicine, which she considers a scandal because it does not involve a physical exam. She says near the end of the video that they are having patients ‘see their assistants’ instead, implying that they are having Nurse Practitioners and Physician Assistants take on risks they aren’t willing to themselves (and playing to the undeserved discrimination those professionals face in healthcare).
At 3:17, she says that other doctors are hiding in their fancy homes with their fancy cars in the midst of a pandemic, and the contempt for others in her profession is evident in each syllable she pronounces.
Her implication is that doctors are scared of the virus and are too timid to treat their patients; they are refusing to see people, the ER is turning people away, and they are using telemedicine and other tricks to avoid having to give compassionate care that might put themselves in danger from the virus. And if that’s true, it’s a tragedy; it represents the deepest betrayal of our Oaths and the values we hold in common as physicians.
But thankfully, it’s not true. When I heard her say this I really had to grieve for a moment; grieve for a doctor whose experiences and views have so detached her from the rest of her profession that she could hold, and promote, a view of physicians that is such a stark contrast to the reality. Please take a moment and really, honestly compare her narrative to the stories you are hearing and seeing from doctors all over the world; the doctors who are staying in donated hotel rooms or sleeping in the hospital call room between shifts because they are too frightened of the virus infecting their own families. Notice that they aren’t cancelling or no-showing their shifts; they are still taking care of patients every day, placing themselves in harms way and risking their live for others as they have been called to do, but they are also taking on the sacrifice of isolation themselves in order to protect those they love. Consider the doctors, even very old doctors who have come out of retirement to help and young doctors still in residency, who have gotten sick and died in the line of duty. Her narrative, at least on the physician side, doesn’t match the reality. And as much as I love my fancy car (it’s a motorcycle with a sidecar I bought used my first year out of residency; I’ve wanted one ever since I watched Indiana Jones and the Last Crusade as a kid and I’m immensely proud of it), her actively promoting for her audience the myth that most physicians lead lives of extravagant wealth (sidecar motorcycles not withstanding) is not only disingenuous but extremely mean spirited. Many of us are currently drowning in medical school debt.
We also have a used 2012 Honda Odyssey minivan. Jealous?
But what about the patient side? Are patients really being turned away? Well first of all, it’s not only bad business and bad medicine but actually illegal to be denied treatment for an emergent condition at an emergency room. Moreover, in practice I’ve never even seen it done even for non-life-threatening conditions, and in fact one of the biggest problems with our healthcare system is that this means a great many people get all of their care from the ER because they don’t have access to a primary care doctor (when my residency program was founded 50 years ago, this was one of the problems it was created to address). Again, Dr. Lozano’s narrative seems to be the exact opposite of the real situation. From her comments alone you would think that patients with cough and fever were having the doors barred from entering their clinic or the ER; but in many areas that have been working under the assumption that a COVID-19 surge was imminent, most clinics and hospitals have deferred a great deal of other types of care in order to specifically care for large numbers of people with those exact symptoms. We have worked very hard to ensure that our other patients are still getting close follow-up, and things like telemedicinehave been put into place to make sure that my 95 year old patient with COPD and congestive heart failure can still get seen without being exposed to the transmission risks inherent in a clinic waiting room. No, patients with cough and fever are not finding a series of doors slammed in their faces, with Dr. Lozano being their last hope; but that isn’t what she’s actually saying.
4:05 Treatment for COVID-19
I promise we’ll get somewhat political momentarily, at least in the sense of giving governing officials their due while not ascribing to them godlike mastery of all intellectual disciplines, and of honestly reflecting on the merits and limitations of national and state medical associations. But let’s press on for now.
When Dr. Lozano was speaking of the patients being sent home and turned away, it might have sounded, to the casual listener, as though she meant they had been refused care, which has certainly not been the case. She tells us what she really means beginning at 5:12–6:30, and I’d encourage you to listen carefully again, and then I’ll explain the sequence of events she is eluding to.
The patients she is referring to were seen. They were evaluated. They were not sick enough to be admitted to the hospital. Because there is no specific medication that has been proven (by large scale studies, not individual anecdotal evidence) to be effective in an outpatient setting, these patients were not prescribed specific therapy. They were likely given recommendations for symptomatic treatment, instructions for self isolation, and guidelines for seeking out a higher level of care if their symptoms worsen; though the thoroughness of those discussions often depend on the time available, the practice style of the clinician, and the degree to which the patient is interested.
So far, this has actually been perfectly appropriate care. Please keep in mind that the hospital is not a place you want to be unless you absolutely have to be. Most patients (85%) with symptomatic COVID-19 have a “mild course.” This can be anything from a mild cough to significant flu-like symptoms which can be very uncomfortable, but most patients with the viral syndrome will not need to be hospitalized. Filling up hospitals withpatients who do not need to be there is the wrong decision not just for other patients in the hospital, those who might need to be hospitalized later, and for hospital staff, but also for the patient. It puts everyone at risk, including that patient, and it’s irresponsible. Dr. Lozano states that they were ‘sent home to quarantine, exposing their families’ as though this were a scandal. First of all, if these patients were symptomatic, their families had already been exposed. Second, home is where they would be safest and best taken care of unless they actually needed hospital level care. And third, there are no other viable options. Certainly some countries have set up mobile containment hospitals for mildly symptomatic COVID-19 patients to stay in until they are deemed non-contagious. Please ask yourself if that is something Americans would consent to; being told that even though their symptoms are mild, they cannot be trusted to keep from spreading the virus to others and are not allowed to return to their homes. We can’t even get people to wear masks.
Finally, these patients come to Dr. Lozano, who gives them a prescription for hydroxychloroquine and some unspecified antibiotic shots for good measure. It is now clear that way back at 2:25 when Dr. Lozano said these patients weren’t being treated, what she was really saying was that they weren’t being treated exactly the way they wanted. Now, we could go off on a rabbit trail about antibiotic stewardship and doctors prescribing antibiotics, and other medications, unnecessarily for viral conditions because it makes their patients feelthatsomethinghas been done. It builds loyalty, it gives them confidence in you, it keeps them coming back to you for minor conditions because they know you’re going to give them something for it; it does everything except actually treat the virus. Please keep in mind that in over half the viral misinformation videos we’ve seen, this is exactly what doctors are being accused of, despite the fact that most of us fight very hard against this exact mentality. It is much, much quicker and easier (and more lucrative, under many practice models) to tell a patient that the injection you are giving them will make them feel better than to carefully, patiently explain that their own immune system will defeat the virus, that there are no specific therapies but lots of things you can do to try to feel better in the meantime, and that your duty is to “First Do No Harm” to them, including prescribing unnecessary and potentially dangerous medications. The latter, in addition to taking more time, also feels unsatisfying to both the patient and the doctor; it’s also the right thing to do. If your doctor never refuses a single thing you ask for, you probably need a new doctor.
What about hydroxychloroquine?
You should know that no medicationis “considered a candy” or “a vitamin” (except, you know, actual vitamins). All medications have potential side effects and hydroxychloroquine, while relatively safe, should not be used without a specific indication and a careful evaluation of the risks and benefits. No medicine should.
Not Candy.
But even allowing for Dr. Lozano’s waxing a bit eloquent in what comprises the bulk of her arguments in this video, we need to ask some very basic questions about hydroxychloroquine. First, we need to ask whether it works, and second, we need to ask whether her narrative and claims about the medication are true.
Does hydroxychloroquine work?
Because Dr. Judy Mikovits brought up the idea that doctors were being stopped from using hydroxychloroquine in the PlanDemic documentary a few weeks ago, I’ve written about this just recently. In the interest of length I will not reproduce those reflections here. The long and short of it is that the medication showed some promise when it was first used on a small number of patients, and following this it was used widely and we all hoped it would be incredibly effective; but unfortunately subsequent more rigorous trials and widespread physician experience have not shown this to be the case, and now it’s use in COVID-19 has been widely abandoned. For more details, please refer to the section titled “Hydroxychloroquine is a miracle drug” from the blog entry “The Paradoxes of PlanDemic,” or read this article from the New England Journal of Medicine that explains this all in greater detail, and the rationale by which the authors have chosen to stop using the medicine to fight COVID-19.
Update 5/22: Click the image to read a study form the Lance published today.
Claim: Donald Trump taught doctors to use this medicine…
While I’m afraid that I have to consider Dr. Lozano’s claims here to be politically motivated and revisionist, in the interest of fairness I admit that, depending on her individual experiences, what resources she has been using, how she acquires new medical information, and to what degree she was pursuing treatment guidance early in the pandemic, from her own perspective the sequence of events could conceivably appear as she has described them. The French study that originally established the efficacy of hydroxychloroquine for COVID-19 was released in mid march, but there was talk of it being used even prior to this; an article coming out of Wuhan, China was published on March 9th, and by the time of the March 19th press conference where Donald Trump recommended it, all the doctors I know had been talking about it in multiple forums for over a week. I had discussions about it in person and on zoom calls, over text and e-mail, and on social media both on friend’s Facebook walls and in private physician COVID-19 groups. Unless you weren’t paying attention to emerging COVID-19 information (and I think almost all of us were by that time), the president’s mentioning hydroxychloroquine for COVID-19, while certainly contemporary to the discussion, was not breaking news. Though Donald Trump was touting the medication with his usual unmitigated bravado, at the time a lot of us really did feel cautiously hopeful; we really wanted the treatment regimen to be universally effective and live up to the hype as well. We also agreed with Dr. Fauci, who stated that this study was little more than anecdotal, and while promising, shouldn’t be relied on as empirical evidence. This wasn’t a political statement; he was merely bringing to Donald Trump’s enthusiastic endorsement the temper and nuance we would expect from a medical professional. If Fauci’s later being proven right adds fuel to the political fire, it is merely a reflection of how unfortunately politicized this pandemic has become; to medical professionals, the rise and fall of hydroxychloroquine is a normal part of the scientific process, though expedited quite a bit by the pandemic.
But Dr. Lozano goes a step further than even Dr. Mikovits; she really seems to be implying that Donald Trump somehow came across this information on his own. While I understand that is a hallmark of diehard supporters of the president, the desire for him to be the smartest in the room on every subject, the idea that he was personally reviewing medical journal articles and came across this French study independently is really very silly. Of course this information would have been given to him during a briefing by his medical advisors, the same ones who then had to qualify his statements, and the very “bureaucrats standing next to our president” Dr. Lozano later decries for “thinking they know more about medicine than I do.” Notice too this strange juxtaposition; she is willing to stand on her professional pride when confronting Fauci and other advisors to the president with medical backgrounds calling for caution with the medication, calling them ‘bureaucrats’ despite their training; but she is eager to say that the president has taught her how to treat COVID-19.
….while medical societies gave no treatment guidance.
As I’ve said, this French study was published and read and discussed widely in the latter half of March, and many medical associations and news sites offered reflections on it. Treatment regimens were included in the original study, so Dr. Lozano’s saying “you would think I would get some kind of guidance from the American Medical Association” couldn’t refer to needing a hydroxychloroquine dosing schedule, but rather expert opinion on what to do with that already available information. As Dr. Lozano requested, that guidance came out on March 25th. The American Medical Association offered a very measured response, calling for physicians to weigh the evidence carefully and to be ‘just stewards’ of healthcare resources. They reiterated that the French study had been small and only included hospitalized patients, and that medications should always only be prescribed due to an appropriate medical condition. This was in response to reports that some doctors were ordering prescriptions of the medication “for themselves, their families, or their colleagues,” and that some organizations were stockpiling the medication. Indeed, there were reports at the time that some patients with Lupus and Rheumatoid Arthritis were having trouble getting their normal dose of the medication because of this. You can read the AMA’s joint statement with the American Pharmacists Association here; it has since been updated, but a summary of the original from March 25th is also online here.
Claim: Doctors are too scared to use it because it isn’t FDA approved.
The FDA actually issued and Emergency Use Authorization to treat COVID-19 with hydroxychloroquine on March 30th. This is still in effect. The FDA has since issued safety guidelines which also cautioned against its use for COVID-19 outside of the hospital. This is because the medication has many possible side effects including prolonged QT syndrome, which can lead to sudden cardiac death, and because even early evidence only supported use for patients sick enough to be hospitalized, while later, more robust studies have not even supported that. The EUA is still in effect however, which does allow physicians treating extremely ill COVID-19 patients in the hospital to weigh the evidence for themselves.
Why won’t the pharmacy fill these prescriptions?
At 7:36, Dr. Lozano begins the narrative that after her 1st or 2nd or 3rd prescription for hydroxychloroquine, the pharmacist called her to ask for a diagnosis. Dr. Lozano presents this as though it were a conspiracy or scandal, the pharmacist trying to breach patient confidentiality laws. In reality this is very common; knowing the diagnosis is important for the pharmacist for a number of reasons, including counseling the patient appropriately, ensuring that look-alike/sound-alike medicines have not been prescribed on accident (this does happen; I have done it and a smart pharmacist caught the error before the prescription was filled). In fact it is required with certain controlled medications. Your pharmacist is considered to be involved in your care, and sharing your diagnoses with them is not a HIPPA violation if it helps them do their job. Moreover, regardless of Dr. Lozano’s jab that “your job is to put the pills in the bottle,” pharmacists literally go to school for years to study medications; they already know your diagnosis from the medicine alone 99% of the time. No pharmacist is saying, “huh, Mr. Johnson is being prescribed Metformin. I wonder what that could be for?” It’s a diabetes medicine; they know you have diabetes. And that’s fine, because they also abide by patient confidentiality laws and aren’t going to go out and tell people about your diabetes any more than your doctor or nurse would.
With hydroxychloroquine specifically, the pharmacist was likely asking Dr. Lozano for a diagnosis because of the AMA/APhA/ASHP joint statement above, which includes this specific phrasing:
The pharmacist asking for the Diagnosis was wise to do so.
Or maybe it was because of this rule from the Texas State Board of Pharmacy:
If the pharmacist had not asked for a Diagnosis, he would be committing malpractice.
So the pharmacist in this scenario was simply following not only the rules of his state governing board but also the consensus advice of the national organizations that represent his profession. Dr. Lozano states that she got around this by eventually finding a pharmacy that would fill the prescription, and by giving them a diagnosis of hypertension or diabetes instead of COVID-19 (it is unclear from her presentation whether these patients in fact have those diagnoses; presumably not, since her whole point is that she is unwilling to share their medical information with the pharmacy). So this requires us to ask the question; are these rules good? Is it reasonable to tell pharmacists that they shouldn’t or can’t fill prescriptions for this medication unless it is for Lupus, Rheumatoid Arthritis, or Malaria? In other words, should this decision really be up to the individual doctor?
In general, physicians tend to be wary of any rule or law that displaces medical decision making outside of the patient-doctor relationship. Dr. Lozano speaks to this around the 8-9 minute mark. The hope is that the years of careful education and training we receive should be sufficient to instill in us the weight of the responsibility we have to follow the evidence and to treat with a light touch in the absence of strong evidence. I believe it generally is. However, there are over a million physicians in the US alone, and oversight and accountability are necessary. As someone who works in the area of opioid dependence treatment, I strongly believe that top-down measures to curb the prescribing of opioids has helped many people avoid addiction and dependence. In the case of hydroxychloroquine, these decisions were made to prevent stockpiling and overprescribing of the medication that would create a shortage that hurt patients who needed it, including those with conditions such as Lupus, and early on, patients in the hospital who were sick enough to be prescribed it for COVID-19.
But it is possible to imagine scenarios where this medication could have been legitimately prescribed in an outpatient setting, at least early on before more data was available. One could imagine a confluence of circumstances where a patient met or nearly met hospitalization criteria, but could not be hospitalized for some reason; being the sole caregiver for a small child and needing to wait a few days for family to return, for instance, or living in a city where the hospitals were full and they didn’t quite meet criteria for hospitalization during the pandemic, even though they might have under normal circumstances. One could imagine a patient in the midst of a work-up for Lupus, whom their doctor was considering starting on hydroxychloroquine anyway, suddenly being diagnosed with a mild case of COVID-19. Would it be legitimate for this to shift the balance of risk and benefit and justify its use now instead of once the work-up is complete? These situations would be exceedingly rare, but they are possible, and it would indeed be frustrating to be a doctor or patient stuck between these realities and the Pharmacy Board’s rules and be unable to get the medication filled.
But is this the case with Dr. Lozano’s patients? Dr. Lozano gave an interview on Fox News where she shares more details from her experiences with the pharmacy. She states, “Yesterday I wrote 5 prescriptions for hydroxychloroquine… Today was horrible, I had 15 people who needed 15 prescriptions.” I have never been in Dr. Lozano’s clinic; I was not there on the day she gave the interview, and cannot vouch for either the COVID-19 status or the severity of illness of her patients. But the idea of one physician in a solo practiceseeing 20 patients in 2 days who have COVID-19, and are sick enough that they should have been hospitalized but weren’t, in a city that has only had 6,000 confirmed cases total, is extremely far-fetched. Rather, this paints the picture of a physician who has chosen to simply give the people what they want, and instead of following the evidence and carefully weighing risks and benefits on a case-by-case basis, chose to cultivate a reputation (and client base; she says she has patients driving in her to see her from Austin and San Antonio) by being the doctor who would prescribe the medicine that was suddenly being talked about all over social media after the president’s press conference. Any doctor who suspended their clinical judgement and prescribed hydroxychloroquine for every cough and fever patient who wanted it in March and April could have done likewise; and that is exactly the kind of prescribing practice that the Texas Pharmacy Board rules and the statement by the AMA were meant to protect against.
But what about Dr. Lozano’s experiences with the medicine? Doesn’t that prove it works?
Please listen to what Dr. Lozano says at 7:15.
“I have patients at Lozano Medical Clinic who are cured of this disease. I have patients that recovered within 48 hours. In fact, the illness that they had was more caused by the stress and the fear of the propaganda that’s being spewed on the news media than by the actual virus.”
Dr. Lozano has told us that she prescribed these patients hydroxychloroquine. She has told us she prescribed them azithromycin as well. She has told us that she gave them ‘a few antibiotic injections’ just for good measure. She states that the FDA can approve you-know-what because she has seen patients get better with this treatment. She now tells us she believes most of their symptoms were from stress.
I also have patients who are cured of the virus; their immune systems did that for them. That’s what usually happens with most viruses, and it happens all the same without potentially dangerous or potentially lethal combinations of unnecessary medications. The number of cases where symptoms are so severe that someone needs a high level of support is particularly high for this virus, which is why we are dealing with a pandemic; but they are still in the minority, and Dr. Lozano has offered zero evidence (and quite a lot of counter-evidence) that these patients would have needed hospitalization without the medications she prescribed.
As a physician, I have bettertools for treating stress and fear about the virus; compassion, active listening, empathy, and careful explanations of the medical realities they are facing. As far as I know, none of those can cause sudden cardiac death.
“I think when you do things that are incorrect, you need to be thrown under the bus.”
Dr. Ivette Lozano
At 10:12 Dr. Lozano throws Walgreens Pharmacy under the bus. She says that if you have a prescription for hydroxychloroquine, Walgreens will call and ask you to fill the prescription in their drive-through instead of at the counter inside. An immuomodulator, for patients who have autoimmune diseases. That is sometimes being used to treat a virus, in the middle of a pandemic caused by that virus. Surely anyone can see that this is a reasonable request?
10:40 “If you are taking a prescription for hydroxychloroquine, they will ask you to come in through their driveway. Well you know what: maybe eventually they’ll ask you to wear a yellow star on your shirt.”
Internet memes and Godwin’s Law aside, this is an absurd comparison. Every clinic I know of has taken steps to ensure that all their patients stay safe during this crisis, and for many that means seeing patients with risk factors for COVID-19 complications and patientswith symptoms of the virus outside to prevent transmission. For whichever indication this medication was prescribed, picking it up at the drive-through is a reasonable step to keep both you and others safe. Is this what Dr. Lozano’s audience considers “oppression”? Is this comparable to the Holocaust? I understand that many people are legitimately concerned over the balance between safety during a pandemic and preservation of individual rights, but is going through the drive-through at Walgreens really the Rubicon we dare not cross? To quote one Twitter user:
Dr. Lozano then says that she has encouraged all of her patients to get their prescriptions filled elsewhere, and that gives me the opportunity to share my first financial disclosure in several months of arguing against financially motivated medical misinformation; my father manages a CVS (in a different state than where Dr. Lozano and myself practice). And while that doesn’t actually constitute a financial conflict of interest, on some emotional level I’m ok with Dr. Lozano calling out the competition here, the same way I didn’t like K-Mart growing up when dad was managing Wal-Mart stores. Call it tribalism I guess. In practice, the only time I care which pharmacy a patient chooses to use is when I know they will get a more affordable price somewhere else, and that’s when we talk through their pharmacy options more intentionally.
10:57 HIV vs. COVID-19
Dr. Lozano states that she trained in general surgery during a time when there was not a good test for HIV, so they took precautions with every single case and did not discriminate against people if they had the virus. It seems odd to compare a virus like HIV, which is very difficult to be infected by even through contact with blood, to SARS-CoV-2 which is spread by droplets and airborne transmission. Dr. Lozano is right that no patient should be discriminated against because of an illness, infectious or otherwise. She is also right that we should take precautions to keep ourselves, and others, from becoming infected. But this looks different for different type of infections, based on their infectivity, potential severity, and mode of transmission. Refusing to operate on an HIV positive patient because of their diagnosis would be discrimination; asking a patient with COVID-19 to use the drive-through during a pandemic- which we really all ought to be doing anyway if at all possible- is not.
11:22 “This virus is 98% treatable with no medication! For those 2% who are sick, the President of the United States has given us a phenomenal protocol.”
I’m going to pass over the fact that the president has apparently gone from being told about hydroxychloroquine by his advisors, to reading about it in his independent research, to now actually creating the treatment regimen himself. Fine.
The bigger issue with this sentence is the way that Dr. Lozano has distorted these numbers. Without getting into details about the percentage of patients who need hospitalization and the percentage that need to be in the ICU (these numbers have shifted and will continue to shift as we have better and better data and antibody testing, as physicians and epidemiologists have been saying since the start), we can accept and agree with Dr. Lozano’s point that only a relative few patients with COVID-19 will need intense and specific interventions; as we’ve already discussed most will get better on their own.
But it’s important to clarify two things. First, Dr. Lozano never mentions working in a hospital either in her youtube videos or on her website, only seeing patients in her clinic. I think it’s fair to assume she doesn’t see patients in an inpatient setting or treat critically ill patients in the ICU. This means that the small percentage of patients she mentions who are sick enough to need specific treatments and high-levels of care are not the patients she is interacting with.She has presented a narrative that says most patients get better on their own, so go get your hair cut and go shopping and if you happen to get very sick from COVID-19, go see her and she’ll prescribe you hydroxychloroquine. The reality is that the patients she is prescribing hydroxychloroquine for are the patients who would get better on their own; they are part of the “98%,” not the “2%.” They’ve already been evaluated by other doctors and were told, thankfully, that they didn’t need to be in the hospital. The patients who need the high level of care are actually in the ICU, those that made it there, and are fighting for their lives. Many of those who have had the worst cases and needed that level of care have in fact been treated with hydroxychloroquine, and many of those patients did die; this is where the more powerful and reliable data about it’s efficacy comes from, not from a small clinic that has drastically shifted the definition of ‘very sick’ because it never interacts with patients in the hospital and ICU.
And second, that small percentage of patients, for a virus that is this contagious, still represents an astronomical number of people. This is the same misrepresentation that Dr. Erickson spends the majority of his time on during his interview; the idea that if most people get better it means the virus isn’t very dangerous. Early mortality numbers based only on antigen testing have been in the society-ending range of 4%-12%, but we have known these numbers would come down once asymptomatic or minimally symptomatic cases could be accounted for. If this virus has ‘only’ a 1% case fatality rate, it still has the potential to overwhelm our healthcare infrastructures and kill millions without mitigation strategies. The danger is a product of the per-case risk multiplied by the infectivity, and this virus is both very deadly compared to something like the flu, which is scary enough, and also extremely infectious. A non-dangerous virus could not do to New York and Italy what COVID-19 has done.
“It is not dangerous to go to a restaurant, to go get your hair done, to go shopping.”
Well, it might be actually. I realize things are open now. This virus is very dangerous and unfortunately we do nothave a “phenomenal treatment protocol” that renders it harmless. Please make safe decisions for yourself, your loved ones, and your community.
I know this seems like a strange place to add my final thoughts (one might have expected them somewhere near… the end), but I want to honor the long tradition of TL;DR that has come before me. PlanDemic has been a fairly unique experience among COVID-19 misinformation videos so far. The production quality is much higher and the narrative, tied to the experiences (questionable though their veracity may be) of an individual scientist, is gripping. The story telling here is far, far better than any of the webcam style videos we have looked at so far, or even the interviews of Dr. Erickson or Dr. Ayyadurai. It’s actually hard to know how to categorize this video; is it an anti-Medicine conspiracy video capitalizing on COVID-19 fears and controversies, or is it a COVID-19 medical misinformation video set in a conspiracy theory narrative? Probably both, but I lean toward the former because while the conspiracy theory is well established and consistent, a brief version of the story Dr. Mikovits has been giving as her own interpretation of the events of her arrest and discreditation for years, the actual arguments surrounding the COVID-19 pandemic are piecemeal and self-contradictory, pulling from any and all vogue COVID-19 misinformation sources rather than forming any new or unified thesis. Still, given the popularity of this video, I will not be surprised if we begin to see more and more of these high production quality misinformation/conspiracy theory pieces; it seems to be an effective amalgamation.
I hope my reflections below prove helpful. My hope is that even if you do not have time to read this entire post (and I can’t blame you there; I don’t have time to read it either), you will be able to navigate to the analyses of one or two of the points from the video that you have particular questions about. If I don’t cover the points you are particularly interested in, feel free to comment below; or better yet, keep digging- I’m sure someone else has done a more thorough debunking on that point than I would have anyway. Thank you to those who have found this analysis relevant enough to share with friends and loved ones who are convinced by or sympathetic to the PlanDemic film; I hope that this information, combined with their affection and trust for you, is enough to open their eyes to the falsehoods being shared so widely, and to convince them to continue exercising caution against this terrible virus.
The link to the video that I originally shared is dead. It is still easy enough to find if you really want to watch it.
First Impression: The production quality here is going to be awesome. (00:04)
Learn about your sources before watching, and then watch critically. (00:10)
This is just good general advice; we trust far too much to our gut feelings (read: confirmation bias) when trying to decide on the veracity of new information. When I wrote about navigating medical misinformation during the pandemic, the first piece of advice I gave was to know your source. I would never argue that arguments can be discounted because of the source; but knowing something about the source is incredibly useful when engaging internally with the arguments, especially when choosing what degree of scrutiny to apply to them. This is especially true with a video like this one. The excellent production quality, the artistic filming and intentional choice of background music, the cinematography and editing, all of it is designed to be emotive and to render the content convincing. That’s not a bad thing; they want you to believe their message, presumably because they strongly believe it themselves. But when all of these features have the net effect of lending credibility to the speakers in the video, we may find ourselves attributing to them a certain expertise or background that may or may not fit. Knowing where they are coming from, who they are, and what they stand for before the emotive music begins gives you some context for weighing their claims outside of how those claims make you feel, or how much you would like to believe them.
By the way, this is the same advice I would give to someone visiting a church for the first time; don’t rely on your gut feeling as a guide to truth; emotive music and a well crafted stage presence can be incredibly convincing.
With that in mind, here are a few links to the main people involved in the video:
Dr. Judy Mikovits is a former researcher who holds a PhD in Biochemistry and Molecular Biology from George Washington University. She published a since-retracted study in Science in 2009 that eventually lead to the legal action she discusses in the video. You can read more about her on her wikipedia page or on the blog Retraction Watch, if it is ever back up again (I believe the viral video has crashed the site multiple times). Since then she is mainly known as a frequent speaker at anti-vaccine events.
Mikki Willis is founder of Elevate, the production company that released the documentary. Their prior work tends to be focused on spiritual energy and positive vibrations (they have a short video talking about restoring your frequency to protect against COVID-19), but this seems to be their first foray into medical misinformation viral videos. You can check out his facebook page here. Before this I believe their biggest documentary was Neurons to Nirvana: Understanding Psychedelic Medicines. Also, as someone who has been interested in televangelists and pseudo-christian faith healers for years, he strikes me as the non-religious, spiritualist version of the young, good looking charismatic faith leader.
The Minions of Big Pharma (O0:38)
This is my first red flag in the video. “For exposing their deadly secrets, the Minions of Big Pharma waged war on Dr. Mikovits, destroying her good name, career, and personal life.” Now, “Minions of Big Pharma” may mean a lot of things; he might be referring to actual lawyers who work for pharmaceutical companies, or to all pharmaceutical employees (although it’s hard to see how drug reps could ruin her personal life), or to some other group altogether. But in the alternative health world this typically refers to doctors and scientists (nurses are generally excluded because as a society we actually like them, so it’s dangerous to the alt-health narrative to loop them in on conspiracy theories)(oh, and happy Nurses Week to my brilliant and beautiful wife!).
Now, I can’t comment much on Scientists working in the lab, since that hasn’t been a major part of my life, but I pretty strongly suspect that they have little to no interest in ruining anyone’s career (and if stereotypes are anything to go off of the only personal lives they are ruining are their own! Bazinga!). I know scientists who have worked for Universities and for major corporations and their main interest has been, unsurprisingly, Science. They love talking about their experiments and research, and their ideas about what might happened next with their project. Remember that these are not nameless and faceless people doing experiments in some hidden lab; these are often the sciency kids that you went to high school with who genuinely loved experiment day in Chemistry class and who were probably reading Lord of the Rings before it was cool. And it’s these science nerds, according to this video, that have now all been recruited into a world wide conspiracy. Tony Fauci calls up one of them and says, ‘we need to discredit a virologist because we don’t like her conclusions about retroviruses; publish a fake study that says she’s wrong.’ It’s really, really far fetched. In fact, if you want evidence of the standards of veracity that scientists generally hold each other’s research to, look no further than Dr. Mikovits’s retracted paper in Science, which was retracted not because she was rocking some boat or bucking some system, but because the methodology was flawed and the results were not reproducible. If you’ve forgotten everything else about those Science Fair geeks from high school, remember this; welovedproving people wrong. The peer review process capitalizes on that, and the conspiracy that there’s a top-down cabal determining what gets published and what doesn’t ignores that one overarching character flaw.
What I can tell you, with no shadow of a doubt, is that your doctor doesn’t work for Big Pharma. In fact, the relationship between your average Physician and the drug reps they interact with range from the politely tolerant to the openly antagonistic.
Though there are beautiful exceptions.
And this is the case for any part of the medical industry that is primarily profit driven, whether it’s the pharmaceutical companies, fly-by-night medical supply companies, pharmacies, or the insurance companies. Because Physicians are not primarily profit driven; we are driven by a desire to help people. We are driven by a desire to help people so much that it is dangerously cliche to even say so on a medical school admissions essay. We’ve taken on hundreds of thousands of dollars in debt, sacrificed our 20’s and 30’s, and worked thousands of hours of unpaid overtime in order to learn the science and the clinical skills that we need in order to do the grueling work of helping people heal physically, emotionally, and psychologically, and there are just much, much easier ways to make money.
So that creates conflict. Conflict ranging from an annoyed ‘I don’t think that’s accurate’ to a pushy drug-rep overselling the latest product, to absolute rage when the price of a life-saving medication skyrockets for artificial reasons and my patients suddenly have to go without. But while we generally regard for-profit pharmaceutical and insurance companies to be side effects of a deeply broken healthcare system, they are still fixtures that we have to work with; and I guess that looks a lot like collusion to the outside world. Once you’ve bought into the myth that those with the most money universally control the people they interact with and endure no dissent, it’s easy to see conspiracies everywhere; of course the scientists are told what results to report, look who signs the checks. Of course the doctors prescribe what they’re told, their education is controlled by big pharma.
But might I submit that maybe ancient, altruistic, and (let’s face it) fairly egotistical professions don’t just roll over quite so easily? That maybe high standards of truth telling and care for the wellness and suffering of human beings are still the honored core of both the clinical and research branches of Medicine? In fact, I don’t think it’s a stretch to say that, to whatever degree drug or insurance companies really have wanted something like autonomous control over healthcare, it has largely been conscientious Physicians who have fought them.
But you don’t get to see those types of interactions that often at your doctors office, and this leads to a lot of pretty demoralizing misunderstandings; for instance when a patient’s medication should be $5 and they end up paying $50 at their pharmacy and think that I prescribed a more expensive medication because I’m getting a cut (this is why I now say to each patient at the end of each visit where I’ve prescribed a medication, “if you get to the pharmacy and any of your medicines are more expensive than you expected, please don’t buy it yet and give us a call instead”). It also means that when it comes to profits being put above people, we’ve probably just about seen it all, and fought against it all. So when even we have to say, yeah this looks like some pretty crazy conspiracy theory stuff, you need to understand it’s coming not from “Big Pharma’s” willing subordinates, but some of it’s most diligent and ferocious watchdogs.
Tell me ZDoggMD is in the pocket of Big Pharma. I’ll Wait.
“The plague of corruption that places all human life in danger.” (00:54)
I think the narrator is just waxing eloquent here, setting us up to understand that the medical field is the real plague or something like that (and if so it’s a good bit of work), but I’ll at least give the video the credit of seeming to take COVID-19 very seriously during the first minute. If you turn this off after minute one, you will at least leave with the idea that 1. there is a plague, 2. human lives are in danger, and 3. it’s a big enough problem that the fate of nations hangs in the balance. That plus the excellent production quality may go a long way towards fighting some of the ‘less dangerous than the flu’ misinformation that is out there already. Way to go, Elevate!
Minute 1 to Minute 10
The bulk of the first 10 minutes of the documentary are spent on Dr. Mikovits’s personal history of maltreatment by the health industry/scientific community. I think people should be able to tell their stories from their perspectives, and I have no doubt that the demolition of her career has been a very difficult experience for her regardless of the circumstances that caused it. Still, it is important to remember that most stories have at least two sides that have to be considered, and other interpretations of those events are available widely on the internet. It’s a very dramatic story and someone other than me will need to dissect it. I will return to this section with a few observations once I have finished the analysis of the rest of the video, but for now my most immediate concerns are the statements related to COVID-19.
Update: Having finally finished this blog post 3 days later, I have had time to read through other articles and watch other videos debunking the claims of PlanDemic. Many do it much better than I can. A great many have focused specifically on the first 10 minutes of the video, and investigating the claims that Dr. Mikovits makes regarding her own history and the conspiracy against her; many have already been familiar with this history and her work in the anti-vaccine movement prior to PlanDemic. I will defer to them. Certainly I have no first hand knowledge of the events and no background in investigative journalism. If you are watching the video, there are 3 things I would point out in this section that I think should at least increase your level of suspicion that you are watching conspiracy theorist/misinformation propaganda. 1. When Dr. Mikovits is talking about her arrest (the video leaves you to assume it was a 5 year imprisonment; it was actually 5 days), they show presumably unrelated footage of SWAT teams and urban tanks in order to inspire fear. 2. The clear implication, towards the end of this section, is that Dr. Mikovits might be assassinated for doing this interview. The credulity people have towards this claim has been amazing, with so many comments along the lines of ‘this woman needs protection now’. Yet, is there any basis for believing that there has been or will be an attempt on her life? And for what? Sharing information about the COVID-19 pandemic that is almost entirely verifiably false? 3. Dr. Mikovits has a book out. I don’t think that this is her primary purpose in giving her interview, and my understanding is that she has been involved in trying to clear her name and garner support against the scientific establishment for years. But so far, financial motivations being tied to viral misinformation videos has been batting a thousand during this pandemic.
A friend on Facebook, supporting Dr. Mikovits’s video.A commenter, accidentally giving a better rebuttal than anything I could ever come up with.
Is this an anti-vax video? (9:48)
Dr. Judy Mikovits: “And they will kill millions as they already have with their vaccines.”
Mikki Willis: “So I have to ask you, are you anti-vaccine?”
Dr. Judy Mikovits: “Oh absolutely not!”
‘But see, she’s not anti-vaccine! This is totally mainstream stuff, not anti-vax propaganda at all!’
Rest assured that many people in both alternative health and the anti-vaccine movement see the pandemic as an opportunity to anchor their products and agendas more firmly in the mainstream. While this is often for financial profit or accumulation of power and influence (as has been the case with every single misinformation purveyor we’ve addressed on the blog so far), I still believe that here are many honest people who earnestly believe in these ideas, and merely have their facts and narratives skewed concerning vaccines specifically and the medical field in general. I know and really like some of them. In fact, a lot of friends whom you might call ‘vaccine wary’, medically suspicious, or crunchy and oily (their words!) have been incredibly supportive of me personally and other healthcare workers during this pandemic. They have struck a balance they are personally comfortable with that allows questioning their Physicians and arriving at different conclusions (which is a good thing in general) and still recognizing a bedrock of reliable truth telling regarding danger, disease, and treatment. I think all of us are looking forward to the day when we can just get back to arguing about tea tree oil in your belly button again (or was it thieves?), but with a real crisis like COVID-19 there is no question that we are all on the same side.
The problem is that as a counter-culture, these movements have overall tended to have a very low threshold for whom to trust, assigning credibility and reliability to almost anyone who is comfortable using the same verbiage and demonizing modern medicine. This means that while many people have found a balance that remains very safe for their families, many others who begin as simply cautious of certain chemicals or treatments (as likely as not because their doctor didn’t/couldn’t take the time to explain it to them very well) become entrenched in increasing (and increasingly dangerous) depths of falsehood. For some, this video, with it’s emotive music and deep state conspiracy theory, will be their next step. The leaders of these movements know this and see dollar signs, potential converts, or both; and the pandemic is a golden opportunity for them because we are all looking for answers. I’ve seen the fallout from this on the individual level in my own experiences caring for adults and children, and on a larger scale with measles and pertussis outbreaks that were totally avoidable. My fear is that, with something as dangerous as COVID-19, the suffering that occurs for the people believing these conspiracies could be the worst and most widespread yet.
Just past the ten minute mark, we finally get into a discussion of COVID-19.
Do you think this virus came from a lab? (10:21)
Dr. Mikovits is making claims that come off as extremely authoritative, but which nobody actually knows the answers to. Labs that have sequenced the genome of SARS-CoV-2 have said it appears to be a naturally occurring virus strain, but the idea of zoonotic transmission from meat sold in an open air market in Wuhan has seemed extremely speculative from the beginning. BBC has a good article discussing the difficulties in sorting through the origins of the virus. As a Physician my main concern is with the viral syndrome that it causes, not where it came from; but the idea of it being involved in any way with a research lab is extremely appealing to conspiracy theorists that would like this to be a Dr. Evil style attempt to conquer mankind.
But look what Dr. Mikovits is actually saying here; she doesn’t think this is a bioterrorism weapon that was designed or engineered, but that doesn’t matter because “You can’t say naturally occurring if it came by way of a laboratory.” Um… Why not? A few moments later she says ‘studied in a laboratory’ like it’s damning evidence. But the thing is… laboratories are exactly where you study things. She’s done a fair bit of it herself in the past. I spent a Summer studying Passalidae Beetles in a laboratory and they are pretty naturally occurring.
The REAL super-bug (and an important forest decomposer!)
What they are saying here, really, is that the origin of the virus doesn’t matter for their purposes; whether it had been engineered as a weapon, whether it was accidentally released from a lab, or whether it just happened to be transmitted from an animal that was being studied in a lab. What matters is the word “laboratory”, because with the degree of fear and paranoia about scientific processes already experienced by many of their target audience, combined with anxiety about the pandemic, that is enough to score points as one more piece of evidence of a global conspiracy.
Finally, at the end of this section Dr. Mikovits claims that SARS-CoV-2 must have undergone “accelerated viral evolution” because if it were naturally occurring, it would take 800 years to develop from SARS. First of all, that’s a pretty specific time frame without any further explanation, so I’m going to call ‘citation needed’ on this one. But the biggest problem with that claim is… Nobody thinks it evolved from SARS in the first place. There are a lot of Coronavirus species, and we don’t yet know (and may never know) the evolutionary history of this dangerous, novel virus. It is called ‘SARS-CoV-2’ because it is a Coronavirus (CoV) that causes Severe Acute Respiratory Syndrome (SARS), and it is the 2nd one identified that does this (because MERS is the Rodney Dangerfield of Coronaviruses; it gets no respect).
Ebola couldn’t infect humans until Dr. Mikovits taught it to in 1999. (12:04)
The first major known outbreaks of Ebola occurred in 1976, 23 years before Dr. Mikovits taught it how to infect humans. So this is pretty nonsensical. The CDC has a good article on the history of Ebola Virus, but I suppose if you have chosen to believe the claims in this video you will probably see this as propaganda? The conspiracy theorist world is a much more interesting world, when even fairly blandly written (though quite interesting, to me at least) and well hidden disease history pages on government websites are all deliberate and carefully crafted deceptions.
But if course, she’s not talking about Ebola virus here, not really; the implication of the video is that somebody had to teach the COVID-19 virus how to infect humans.Add this to the list of claims in the video that have zero empirical support, but that devotees will come away 100% believing.
The COVID-19 death toll is inflated (12:22)
The tabulating of deaths from COVID-19 has been written about time and again. I wrote about it here a month ago when these conspiracy theories about doctors faking death certificates and being told to call everything COVID-19 were already being circulated. It’s been debunked thoroughly and frequently, and our best guess is that the actual death toll has actually been underestimated. We’ll do a little more debunking here, yes, but honestly it’s getting a bit old.
But the first thing I want to point out is how this video, as a smorgasbord of COVID-19 conspiracy theories, ends up mixing it’s message and contradicting itself time and again. We just spent several minutes focusing on their belief that the virus was created in a lab, that it was intentionally taught to infect human cells, and that it is part of a government plan (I mean, that’s thename of the video, PlanDemic), and now we are talking about how it really isn’t that dangerous. This video would like to have its virus and eat it too; it wants the numbers to be inflated, but it also wants the deadly disease to be an evil plot. Now, you could come up with some scenario that fits both conspiracy theories; the virus was released by Scientists (the minions of Big Pharma) but wasn’t as deadly as they had hoped, so they have had Physicians (the other minions of Big Pharma) inflate the death numbers. Sure, if you add enough layers to your conspiracy theory you can account for apparently contradictory sub-plots; but you also have to involve more and more willing participants in the conspiracy, and at some point you have many millions of people colluding in order to… what? Get some people to take a vaccine? Credulity can only be stretched so far.
The other thing you need to recognize is that Dr. Mikovits is about to step firmly outside of her training and experience, which has nothing to do with clinical medicine. When she speaks about discerning the cause of death, the interaction of chronic diseases with acute infections, and the realities faced by doctors fighting this horrible virus, she is speaking entirely as a layperson.
COPD deaths are being counted as COVID-19 deaths?! (12:49)
I am sorry her husband has COPD. That really stinks.
COPD (Chronic Obstructive Pulmonary Disease) and Pulmonary Fibrosis are different types of lung damage (maybe her husband has both, which is absolutely possible)…
…and neither looks like SARS.
“But he has no evidence of infection”. Well, that’s a really wonderful thing; it’s also an important point on the natural history of COPD. Most COPD patients do not have thickened mucous, extreme shortness of breath, severe dyspnea, and prominent wheezing all the time. When those symptoms occur we call it a COPDAcute Exacerbation. And when you have an exacerbation, it absolutely is a sign of something acute happening, usually a viral or bacterial infection.
(13:10) No they absolutely wouldn’t. If he walked in with no evidence of infection, he shouldn’t be walking in at all; the ER is a dangerous place for him now more than ever. But if he comes in with acute worsening of his pulmonary symptoms, the worst COPD exacerbation he has had in his life, requiring high levels of oxygen and even intubation and ventilator support, with exposures to the COVID-19 virus or symptoms consistent with the disease in an endemic area, are you really saying thatpolitically motivated incredulity about the virus’s infectivity and lethality trumps the doctor’s diagnostic skills? The thing they have been working their entire lives to develop?
My friend and classmate, and ER doc in New York, on the shortage of tests.
The Doctors are telling us the numbers are inflated. (13:15)
I know hundreds of doctors personally, maybe thousands, and have read or heard from even more. Some of them work in the front lines in places like New York that have been hit hardest (so far) by the pandemic. Throughout this crisis I have reconnected with classmates and friends I hadn’t talked to in years to touch base on how this whole thing is going for them, how they are holding up. None of us are being told to fudge numbers. Even if we were being told to, we wouldn’t. There are over a million doctors in the USA and I am convinced that almost every single one of them would blow the whistle and be on youtube tomorrow if the government was asking them to artificially inflate numbers or lie on death certs. This is ridiculous.
My ER Doctor Friend in New York, battling COVID-19 daily
But more to the point, the guidance that has come from the CDC has actually been really reasonable. Even the images shown in the video, which are supposed to be some sort of damning evidence, are reasonable:
What this is saying is that if it walks like a duck and quacks like a duck, but the COVID-19 test is negative or not available, it’s still reasonable for a Physician to rely on their clinical judgement to determine the diagnosis. This is the opposite of a top-down mandate, and more to the point,it’s already how we practice medicine anyway. If you have a sore throat, fever, red and swollen tonsils, and your son had strep, I don’t test you for strep throat, I treat you for it; you have it,regardless of what the test says. And that test has a much higher degree of reliability than the SARS-CoV-2 antigen test. If you have symptoms of the flu, and it’s flu season, I only test if it would actually help me make a treatment decision, which is fairly rare; the sensitivity of the test is only 50% to 70%, which means that up to half the time you have the flu your test is going to be negative. It’s too early to know exactly what the sensitivity of the COVID-19 test is, but early reports said somewhere around 70%; so doctors very wisely chose not to defer their clinical decision making to a test result.
Finally, there’s the case the doctor in the video discusses around the 13:40 mark: the 86 year old patient who dies from pneumonia, who wasn’t tested for COVID–19, but her son later tested positive for the virus. The doctor asks, incredulously, whether it would be reasonable to list COVID-19as a possible cause of death?
Every practicing clinician: Um, yeah, it would. In fact, these are the exact people we know are most susceptible to the virus, and the ones we are working our butts off to protect. Most of my 86 year old patients treat me like a grandson; we are treating this virus like it can kill them because it can.
13:50: Dr. Erickson owns Urgent Care Centers in a low-prevalence country in California. He is not being pressured to write COVID-19 on anything, and if he’s writing death certificates with any degree of frequency that is a big, big problem. He would like this pandemic to be not that big of a deal just like the rest of us, only in his case, it’s at least partially because his Urgent Care business is suffering right now. (Update: He has also released a statement saying he has no association with the PlanDemic video).
“You don’t die with an infection, you die from an infection.” (14:38)
While this is not technically true (people die with infections all the time. You can get hit by a bus on the way back from your abscess drainage), I actually completely agree with Dr. Mikovits here. This is the inverse of the common saying for Prostate Cancer, “most people die with prostate cancer, not from prostate cancer.” It’s a common form of cancer that grows slowly and often near the end of life; most people with it will die from something else. Contrast this to COVID-19, which is an incredibly dangerous virus that has killed 75,000 people as of today in the US alone, and even if you don’t believe those numbers has overwhelmed healthcare infrastructures, exhausted doctors and nurses (and driven some to take their own lives), and decimated entire countries. This is a dangerous virus. It increases risk of blood clots, it seems to be causing strokes, it shuts down the lungs; the idea that people are suddenly dying in large numbers from these types of syndromes and their having the virus is just a coincidence is insane. You die from the virus; not with it.
The numbers have to match the real-life narratives, but by avoiding any discussion of the experiences of doctors, nurses, patients, and families that have been affected by the virus, the misinformation promoters hope to bypass your compassion and even your sense of rational self-preservation and deeply ingrain the idea that the virus isn’t dangerous with fake numbers and false dichotomies between acute infection and chronic disease. If they are successful, then you will be automatically suspicious of any images, narratives, or personal accounts you hear that paint a picture of a deadly virus causing real human suffering. The word ‘trauma actors’ is not far off. Don’t let them rob you of your empathy for their own personal gain.
Doctors are being incentivized to list COVID-19 (14:44)
Check-out this article from PolitiFact that covers this question in some detail. Yes, part of the CARES act was to provide a 20% stipend for treatment of COVID-19 cases. This is being done because hospitals that are hardest hit by the pandemic are also the ones that are going to have trouble staying afloat; they will be cancelling elective cases and other more profitable treatments for longer and focusing entirely on COVID-19, often in the midst of needing to pay nurses and doctors overtime, hire outside help, and wildly exceed their budgets for PPE and supplies. Now, we can talk about whether or not I think hospitals being for-profit is a good model in the first place (hint: I don’t), but the idea that a bipartisan government stimulus for hospitals in the hardest hit epicenters of the pandemic automatically equals corruption and conspiracy is awfully flimsy.
But more importantly, I want you to watch the way the video, with it’s excellent background music and high production standards, weaves this part of the narrative. Go back and watch the 15 seconds from 15:00 to 15:15 and notice the way that the words “you’ll get paid $13,000” and “if that COVID-19 patient goes on a ventilator you’ll get $39,000” are overlaid against medical professionals, in PPE, treating patients in the ICU. Look at all of these doctors just waiting to cash their $39,000 checks from medicare,the video is telling you. The reality is that decisions about diagnosis and decisions about treatment are made by Physicians, who are not paid $13,000 for a certain diagnosis or $39,000 for initiating life-saving treatment. Depending on the way their compensation agreement is structured, they may or may not see any of that additional money (I certainly won’t should we get hit hard here in Waco and I have to admit COVID-19 patients or intubate the critically ill).
Also listen to Mikki Willis’s statement right at the beginning of the segment; “I’ve spoken with doctorswho haveadmitted that theyarebeingincentivized…” This is the verbal equivalent of the above cinematography trick, and is the type of sentence you can utter with impunity because there are so many doctors it would be impossible to prove he hadn’t talked with doctors who said this. But notice how doctors are only a reliable source of truth telling if they are blowing the whistle on some big conspiracy, and not when they are saying, en masse, ‘this virus is dangerous. we are doing the best we can to take care of patients but please stay home. there’s no conspiracy here, just a really, really bad bug.”
The ventilators are what’s killing patients! (15:15)
I’d like you to understand that Dr. Mikovits, who is a PhD virologist and not a medical doctor, is here repeating what she has heard or read and is not speaking as an expert by any means. I’ve had a friend write to me extensively about how dangerous ventilators are. I’ve seen videos and articles and facebook posts saying “88% of people who go on ventilators die”, as though that were proof that ventilators were dangerous, instead of that the virus is dangerous. (here is an article working through those ventilator numbers, by the way). You see, we only intubate the sickest patients, so they already have the highest chance of dying. There’s a confounding variable, and it’s called severe respiratory distress.
Now, I do think there is a discussion to be had here in terms of the best use of our ventilators. The myth here seems to be, as best as I can understand it, that “ventilators” are a discrete treatment the way “ibuprofen” or “knee injections” are discrete treatments; either you do a knee injection or you don’t (ok that’s also not accurate), either you give ibuprofen or you don’t. But ventilators are incredibly complex tools and their use is not monolithic. Here is a very basic but extremely helpful (at least to someone like me who doesn’t use a ventilator on a daily basis) guide to vent strategies from some people I admire over at EmCrit. Did you read it? You got all of that? This is the tip of the iceberg. Even the clip that PlanDemic shows at 15:18 is an ER doctor from New York early in the course of the pandemic arguing for a different ventilator strategy, not against the use of ventilators. His name is Dr. Cameron Kyle-Sidell, and he goes on to say:
“Now, I don’t know the final answer to this disease. I do sense that we will have to use ventilators. We’ll have to use a great number of ventilators, and we need a great number of ventilators, but I sense that we can use them in a much safer way, in a much safer method.“
So they’ve shown this clip to make you think, doctors are using ventilators because they get paid more money, even though it kills people, but a few doctors like this one are speaking out against this corruption. The real narrative behind this clip is a lot more reasonable and a lot more hopeful, and it’s this: doctors are trying to fight this new virus with the best tools they have, and impassioned discussions and debates about how to use those tools well are already happening. I am a part of a number of Physician COVID-19 groups on facebook, and both there and in private conversations and discussions within my own clinic system, every aspect of when and how to use ventilators to support COVID-19 patients is being dissected and discussed. It’s a good thing that we know more than we did a month ago, and the more we can delay the spread of this virus, the more we will know when it finally hits your area.
But let me make one thing abundantly clear; this is not a choice between using a ventilator and making more money, and not using one so the patient can get better; that is a false narrative and, frankly, on the grossly cynical side even for the conspiracy theory people. When you intubate a severely hypoxic patient, having tried everything else you know of to keep them off the ventilator, your decision is to use a ventilator or watch them slowly die gasping for air. Unless you’ve been in that situation, your theories on doctors putting patients on ventilators because they were told to or are thinking about their next paycheck don’t carry much weight with me.
And let me just state, for the record, that if you suspect a doctor at your hospital is putting people on ventilators or doing any procedure in order to make more money, you should report that person right away. That’s what I did the one time in my education or career I thought I had seen it happen. And if you believe it’s happening on a large scale, that doctors all over the country are doing it, please start thinking now about what you will do when your child or loved one becomes terribly ill at some point in your life, because if you have that little faith in the good intentions and integrity and medical knowledge of doctors and nurses, I cannot imagine why you would evercome to a hospital (though I honestly hope you do, because I believe we’d have the best chance of helping them, even if you don’t right now).
What about Italy? (15:35)
I just want to say that as little as I’ve found in this video to agree with, I really respect even the willingness to address the parts of the Pandemic that simply can’t fit it into their narratives (ok, I’ve actually found nothing to agree with; but there is at least plenty I can’t comment on. For instance, I can’t say whether or not someone planted evidence in her house before she was arrested).
When the Bakersfield Doctors, misled by their shoddy statistics, concluded that the virus wasn’t at all dangerous, they simply hand-waved New York and Italy as ‘hotbeds’ and moved along; it didn’t fit their narrative and so they didn’t even make a show of trying to explain how a non-dangerous virus could cause such catastrophic damage. The narrative here is infinitely more interesting.
Reason #1 is good; Dr. Mikovits says that Italy “has an older population, and they are very sick with inflammatory disorders.” Now, I don’t have any data on whether Italy has a higher rate of autoimmune disease, which I believe is what she means by inflammatory disorders; but I think we can accept the idea that older populations with more chronic illnesses are going to be at higher risk for complications, including death, from COVID-19. That is very consistent with the data we have seen throughout the pandemic. I would also point out that Italy is not alone in having an older population; many US States have similar demographics. 22.8% of Italy’s population is older than 65; but so is 20.6% of Maine, 20.5% of Florida, and 19.9% of West Virginia. If Italy can experience a surge of cases bad enough to overwhelm their healthcare infrastructure, there is nothing to prevent it from happening here. And of course, age isn’t the only factor; it has happened in New York, and only 16.4% of their population is greater than 65 years old. But the point is, saying ‘Italy is old’ doesn’t explain how a non-dangerous virus can kill so many.
But at 15:47 she loses me. Her claim is that in 2019 Italy had a new, “untested” form of Flu vaccine, and that this explains Italy’s high COVID-19 burden. She says the vaccine was grown in a dog cell line, and that ‘dogs have lots of coronaviruses.’
So, does that even make sense? Well, someone will have to tell me whether the flu vaccine used in Italy last year was new in the sense of being designed or developed differently from flu vaccines used in prior years or in other countries (in another sense, the flu vaccine is new every year because epidemiologists have to decide which flu strains to include based on which are most likely to become endemic). By the way, Italy had a particularly light flu season; so if it was new it may be a really good vaccine. However, the mechanism she is describing isn’t logical. First of all, the flu vaccine they use in Italy includes only killed viruses; your body is exposed to the antigens and can mount an immune response, but the virus cannot ‘come to life’ and cause the flu (or any other ‘inflammatory reaction’ she is hinting at here). The antigens of the dead virus are picked up by circulating white blood cells and presented to the immune system, so that the next time the body sees the virus it has the ability to rapidly produce a robust antibody response, usually before a person is even symptomatic (it does not work by creating a magic forcefield around your body that flu germs bounce off of).
Glad I got that flu shot
But the trick is preserving the dead flu proteins without eradicating them completely. The idea that Coronaviruses have somehow come from a cell line used to develop the vaccine, have survived the process of creating the vaccine (all of the ‘harsh chemicals and toxins’ we are always hearing about), and have tagged along and actually entered the person’s body through the flu shot is nonsensical. Even if that were true (it’s not), she gives no clear mechanism by which that would have literally anything to do with COVID-19. Remember, Coronaviruses are a big, big family of viruses, and exposure to one would at worst have nothing to do with infection by another, and at best give some degree of cross-reactive humoral immunity, which sadly does not seem to be the case for COVID-19. Really, ‘dogs have lots of coronaviruses’ is little more than word association.
But the title of this article is “The Paradoxes of PlanDemic”, and here is another one. Just 5 minutes ago Dr. Mikovits told us that the COVID-19 virus, SARS-CoV-2, was created in a lab in Wuhan China, and was accelerated and manipulated in bats. So what would a flu vaccine in Italy, created in a dog cell line, have to do with COVID-19? There isn’t even a theoretical mechanism here; just the hope that by saying flu vaccine and Coronavirus close enough together in the video, their viewers will believe that the 30,000 deaths in Italy are actually another crime of the scientific community, instead of a stark warning of how bad this pandemic can become.
At this time the video has been removed from YouTube, Facebook, and Vimeo, the three sources I had used to view it while writing this post. I have mixed feelings about this. I don’t believe in censorship in general, but I also worry about allowing verifiably false propaganda to deceive millions in the name of freedom of speech, and the real human suffering that could occur if these videos were spread unchecked. I am a Physician, and it’s probably more a question for a philosopher or at least a constitutional scholar.
That said, if you do have a source for the video, feel free to send it my way via the “contact” page. Otherwise, the rest of my comments will be given without any time-stamp or specific quotes, though I have viewed the video in it’s entirety prior to now.
Hydroxychloroquine is a miracle drug, which is why they won’t let us use it.
I remember back in March (oh those carefree days, where have they gone?) when an OB/GYN I know, a friend from undergrad, first shared the French study showing promising results in COVID-19 patients treated with hydroxychloroquine, an immunomodulator we use mainly for Lupus, and azithromycin, an antibiotic (but you already knew that because they give it to you every single time you go to an urgent care…). At the time the responses of the clinicians I know ranged from cautiously hopeful to very skeptical. Hydroxychloroquine and azithromycin are not anti-viral drugs, some argued, and the study was so small that the results shouldn’t change our practice. Others argued that both medicines have some theoretical anti-viral properties, so even though they are not anti-virals per se there is at least a reasonable mechanism of action in play. For azithromycin, this involves anti-viral effects on the epithelial cells of the lungs; for hydroxychloroquine, prevention of viral entry into the cytoplasm of host cells.
Since this wasn’t a large randomized double-blind placebo controlled trial, this small article coming from France hardly constituted a gold standard of treatment; but since the medications were fairly safe and somewhat promising, and since it is the middle of a global pandemic, many doctors and hospitals began to use one or both. There were even some promising, but ultimately anecdotal results. Locally we used hydroxychloroquine but not azithromycin, generally, because of the concern that the combination of both could cause prolonged QT syndrome (which can, you know, kill you). Here is the very measured guidance from a field guide a friend sent me:
As far as I know, each hospital and Physician had to weigh this evidence for themselves. The FDA did release an emergency approval for hydroxychloroquine for COVID-19, and at no point were doctors told we weren’t allowed to use it, unless this came from their own clinics, hospitals, or medical societies; certainly I’ve never heard of any of the ‘doctors being threatened if they use hydroxychloroquine’ that they mention in the video. Unfortunately, subsequent larger and more intentionally designed trials have not shown a benefit; not to fault the French trial, they were trying to save lives and were publishing the modest but promising results they had so far, not trying to empirically prove the efficacy of the medicine. Here is an article from the New England Journal of Medicine that explains this all in greater detail, and the rationale by which the authors chose to stop using the medicine to fight COVID-19.
So that’s the story of hydroxychloroquine, and it’s hard to imagine how anyone could think there was any conspiracy behind that pretty straightforward sequence of events. Really, that’s how these things are supposed to work; if the treatment is safe and cheap and seems to help, it’s reasonable to use it while you are waiting for more reliable data. If that data then shows that the benefit just really isn’t there, you stop using it. When the president touted the drug as being promising, it was with his usual bravado but to some degree reflected the hope many of us felt about it at the time; when Dr. Fauci advised caution and stated the evidence was anecdotal, he was right, and was saying exactly what your local Physician might say at that point if she had been reading up on it. I don’t know anything about the doc yelling in the clip they showed, but unless he was actually treating COVID-19 patients and had some really excellent anecdotal results, I really can’t understand the vehemence he felt about the medicine; it hasn’t been warranted at any point by the evidence.
But before we move on, there’s one more thing I wanted to mention (and here is where I feel most keenly the loss of the video itself), and it’s that the idea of anyone in the healthcare industry actually trying to block doctorsfrom using a medication because it is working is obscene in the highest degree. I’ve seen enough corporate espionage movies and read enough Spider-Man 2099 comics to have a healthy suspicion of the big pharmaceutical companies, but I really believe this is beyond even them. But if you wouldn’t put it past them, at least consider this; if the government or big pharma or whoever were really telling doctors they couldn’t use a medicine that the doctors knew was saving lives, how would the doctors react? Would they go along willingly, because their one and only interest is obeying their corporate masters? Would they shrug their shoulders and watch people die who they could have saved?
Would you see just that one angry doctor ranting on YouTube, or hundreds of thousands?
Another Doctor Webb
Wearing masks increases your risk of infection, reactivates your own COVID-19.
To me, this is the strangest claim in the entire video, and it’s hard to understand for a number of reasons. First, how in the world is asking people to wear masks a conspiracy? Many of the masks we give to patients even in our own clinic are homemade, so it can’t possibly be Big Mask trying to turn a profit. I know many people chafe under any sense of the government trying to control them; but does this actually count, asking us to wear masks in public, that we’ve either made ourselves or gotten for free at our doctor’s office, to keep ourselves and especially others from getting sick? I don’t like wearing masks much either (unless it’s for Comic-Con), but it always strikes me as a particularly troublesome part of our highly individualistic culture that we oppose on principle so much that we ought to do voluntarily the moment there is even a hint of it being mandatory, particularly acts of charity (financial and otherwise) toward our neighbors. Remember, you don’t wear a mask for yourself; you are wearing it to prevent transmission if you have SARS-CoV-2 and are asymptomatic, to keep from spreading it to others.
Will protect against certain Psionic attacks; but not against COVID-19
Of course, this demands the question of whether or not wearing these homemade masks actually is an act of charity; that is, if it really does protect our neighbors from the virus. And as easy as it would be to simply say, ‘yes, masks obviously decrease transmission of respiratory viruses by blocking droplets’, the reality is that in science, what feels right or makes sense intuitively isn’t always a reliable guide to what’s true (hence this blog). So the real answer is; yes, they probably help. LiveScience has a good summary of the most current info and recent studies. With promising but limited evidence we have to weigh the risks and benefits. Remember what we said about using hydroxychloroquine earlier; if a treatment is promising, cheap, and safe, it’s reasonable to use while waiting for more data, and the same is true about prevention strategies. In this case, while we may well get more data we will likely never have a definitive answer about the degree of benefit. What would it look like, exactly, to do a large double-blind placebo controlled trial of wearing masks?
But Dr. Webb,you said the masks are only a good idea if they are safe, and the video says they aren’t. There is a very strange claim in the video, The idea that wearing a mask is somehow dangerous. I’d be remiss if I didn’t mention that they are once again contradicting themselves, but this time in rapid fire sequence. They want at once for the masks to be bad because they keep viruses and bacteria out (they show the clip of Dr. Erickson talking about how touching your face and eyes is vital for your immune system, failing utterly to distinguish between a deadly pathogen and mere microbes), and for them to be badbecause they expose you to your own microbes. This is not only poor science, it’s also poor debating. To borrow from Scott Adams (Dilbert), it’s like saying Sorry, I never got the message to call you. And when I did return the call, you didn’t answer. One excuse is better than two.
But I think what’s really going on with this claim is two things; an appeal to the deep desire we all have for a sense of normalcy, and an exploitation of the sensationalization of wearing masks. The truth is that wearing masks isn’t new, and we do it all the time anyway. I wear a maskfrequentlyat work because it both protects my patients when I have a cough that might be infectious, and protects me from respiratory organisms. But you wear a mask too. You wear one when you have the flu and don’t want your kids to get sick; people ask me for them all the time when they are at the office. You wear them when you go snow skiing, or when you are around dust, or when you are painting or staining wood or doing projects with strong fumes, or at Halloween. I’ve never heard of anyone, health conspiracy theorist or otherwise, crying out that they were dangerous, that they reactivated your own viruses or starved your brain of oxygen. But now that it’s a matter of admitting how deadly and dangerous this virus can be for the people you are interacting with and following a reasonable recommendation from the government, all of the sudden they are part of a conspiracy, a symbol of oppression?
All of that said, there is one situation where wearing masks really is dangerous, and it’s when people treat them as though they alleviate the need for any other safety measures; as though it made them invincible from the virus. With only limited efficacy at protecting against respiratory viruses, masks are not the ultimate answer to COVID-19, and physical distancing, hand washing, and careful mitigation strategies are still vitally important. But most of us can remember to do those things while still wearing a mask.
Even if it makes you look silly
Healing microbes in the Ocean.
I’m sorry, I’m just totally lost here guys. Maybe she means these?
COVID-19 Deaths from the day PlanDemic was released:
Yesterday a friend sent me the following video and asked two things; would I write about it, and would I try to make it short! The second skill is not really in my wheelhouse, and it is a very, very long video, clocking in at 52 minutes; I am currently writing a 2 part essay on a video that is less than 5 minutes long.
I’ve chosen the “live tweet” format (I don’t know what else to call it) in order to keep my comments brief and in-line, chronologically, with the video itself; I am sure I will have some additional closing remarks, however.
While most of what I try to address on this blog falls into the first two categories of ‘lies’ and ‘damned lies’, Dr. Erickson’s analysis belongs primarily to the final category. Dishonest statistics are extremely difficult to dispel because those who don’t have a background or training in interpreting them are apt to chalk up disagreements to a mere difference of opinion about what the numbers mean. They are often right. However, in this case Dr. Erickson is actually creating false statistics out of thin air, and then framing his arguments with these imaginary numbers.
(Note on time: with the original video removed from youtube, these time stamps are going to be a bit off. The facebook video above is about 12 seconds ahead of the original video; so 0:22 becomes 0:10, 0:27 becomes 0:15, etc. Sorry for the inconvenience.)
0:22 Kern County California.
0:27 This is my first yellow flag; “ER Physician/Entrepreneur perspective.” Most doctors wouldn’t describe themselves in that terminology even if they run their own practice, so I’m listening very carefully for what the “entrepreneur” angle is.
Over and over again with these misinformation videos, we have seen that the creating of false information has some direct link to attainment of money, power, or fame for the person in the video.
0:45 “If that still makes sense.” This is the question on every person’s mind, and rightfully so. For medical people, clinicians and nurses, it’s a definitive and resounding “yes,” so I’m interested to hear his perspective.
1:00 Already this video is different from most of what’s going around, because these guys are actual doctors.
1:34 Here we reach the “entrepreneur” piece; my understanding is that Dr. Erickson is an owner or partner of Accelerated Urgent Care, a group of 5 Urgent Care centers around Bakersfield CA.
Two things about this: First, we do need to recognize that while Urgent Care centers can and do provide services that help take the pressure off of over-utilized hospital emergency departments, they are NOT emergency rooms, and so unless Dr. Erickson is also working in a hospital context it is not quite accurate to treat him as a practicing ER Physician; he is likely ER trained, but not currently working in that context.
Second, Urgent Care centers are indeed entrepreneurial ventures; they are for profit, like so many fixtures of our broken healthcare system. During this entire video we are going to have to ask ourselves how the pandemic is affecting his business, and how that is implicitly affecting his understanding of the situation and statistics.
1:44 See above.
1:58 I don’t know what “furloughing patients” means, but otherwise this is the exact situation in Waco; we’ll get into this in more detail later because I think it’s an important topic.
One note for now; do not fall into the trap of thinking that “empty ICU’s” means that the pandemic is not real. Cancelled elective cases and alternative delivery of care is part of containment measures in areas where COVID-19 has not yet surged, like Waco or Kern County California. The worst is yet to come.
2:03 Make note of this. Everything else that is said in this video needs to be understood in the context that even Dr. Erickson recognizes that this virus can overwhelm healthcare infrastructures; it’s doing it in New York right now.
2:30-3:02 He’s absolutely right, in a way. As I’ve written before, every single clinic I know of is working hard to make sure that their patients with chronic medical and mental health needs are still receiving the best care possible under the circumstances.
But there is another side to ‘secondary effects’ of COVID-19 as it relates to chronic conditions, and it’s this; as deadly as this virus is for people with the very conditions he is listing (in other words, their fear or caution is not unfounded), an overwhelmed healthcare system is also dangerous even apart from the virus. When patients who have heart failure or diabetes, or depression, or any other medical or mental health condition cannot get care because the healthcare system is overwhelmed with a pandemic, that is no less dangerous than not getting seen for other reasons; and probably much more dangerous in many cases because at least with the ‘minimum capacity’ healthcare usage he is discussing they could still get timely treatment in a true emergency, which is not a guarantee when the local ER’s are overwhelmed. These are difficult decisions that every clinic, hospital, and system is weighing carefully; and the quality of that decision making depends on reliable COVID-19 data, as we will see shortly.
One more note; this absolutely is being talked about, and extensively. Don’t fall for the “why are the higher ups keeping quiet” argument about very complex medical systems and situations; these conversations are being had on every level and have been for months (I have yet another Zoom meeting this afternoon about this very issue).
3:17 I think this is a really misleading way to frame the amount of data we had 1-2 months ago, and at the beginning of our social/physical distancing measures. Cases began to rise outside of China in early to mid February, and We already had 100,000 confirmed cases worldwide by March 7th. It was officially declared a pandemic on March 11th. So those (not) early (enough) decisions to begin social (physical) distancing measures were made based on data, not in the absence of it.
3:33-3:50 This is a false equivalence, and actually rather silly. What would it look like to quarantine the healthy because of ‘normal’ infectious diseases? “Sorry Billy, no school today; somebody at your school has pink eye so everyone is staying home.” “We can’t go to Church today kids; the pastor’s daughter had Hand, Foot, and Mouth Disease.” Pretty ridiculous, right?
But our template for COVID-19 is not pink eye, or strep throat, or even the seasonal flu; it is the 1918 Spanish Flu pandemic, smallpox, and the freaking Black Death. He is acting as though he didn’t study these diseases and periods of history in pre-med and Medical School.
In a Pandemic, social (physical) distancing, what he is calling ‘quarantining the healthy’, absolutely saves lives. If you don’t believe me, read this article. Or go play the Plague, Inc flash game and try not to throw your phone across the room when Madagascar shuts down it’s seaports.
4:21 I didn’t realize what he was trying to say here right at first, but it’s worth pointing it out here instead of 10 minutes later when it finally hit me, since this is actually his main thesis throughout this video.
Kern County:
People tested: 5,213, Positive Cases: 340
Dr. Erickson: “That’s 6.5 percent of the population.”
Wait, no, it isn’t!
“Which would indicate that there’s a widespread viral infection.”
No, it doesn’t.
You see, this is where the statistical bungling really begins; he’s saying that since 6.5% of the people tested were positive for COVID-19, we can conclude that 6.5% of the entire population has it. But that’s an absolutely erroneous conclusion, because the testing wasn’t random. This testing was done, especially early on, primarily on patients who had symptoms of upper respiratory illness and fever, had known medical conditions that made them high risk of complications from COVID-19, and who had some degree of known exposure to the virus.
Do you remember how just a couple of weeks ago so many people were upset that they couldn’t be tested because the criteria for testing was so strict? The fact that only 6.5% of even these patients had positive tests shows that the virus is not yet widespread in Kern County California, just like it isn’t here in Waco, or in any city that hasn’t yet hit a surge in COVID-19 cases yet.
This data cannot be “extrapolated” to the general population to determine the prevalence of the virus because the testing, so far, has not been random or representative. His methodology sounds reasonable enough on the surface, but it is actually leading him to wildly inaccurate numbers and conclusions that are the exact opposite of the case.
“We think it’s kind of ubiquitous throughout California. We are going to go over the numbers a little bit to help you see how widespread COVID is.”
This should properly be understood as Dr. Erickson’s thesis for this video.
4:40 California:
280,900 Tested.
33,865 Positive for COVID-19.
*dubious math*
“That means that 12% of Californias were positive for COVID”
Except it doesn’t,because you can’t get data on the number of cases in the state from non-random testing of symptomatic individuals with known exposures.
5:08 These projections were based on what would happen without social/physical distancing, shelter in place orders, and other mitigation strategies. The fact that it “hasn’t materialized” is evidence that mitigation is working. We have been saying since day 1 that as soon as these strategies started to show success, people would say they weren’t necessary.
But don’t worry; if we work hard to return everything back to normal and forego all mitigation efforts, we can still make these numbers materialize.
5:20 You cannot extrapolate prevalence data from testing of symptomatic individuals. We will explore how you could get this data later on, but for now, each time he ‘extrapolates the data’ you need to realize that the number that results doesn’t actually mean anything.
5:32 “That equates to 4.7 million cases in the state of California.” (No epidemiologist believes this; this is a nonsense number.)
“We’ve had 1,327 (now 1,651) deaths in the State of California with a possible prevalence of 4.7 million.”
“That means you have a 0.03 chance of dying from COVID-19 in the State of California.”
Dr. Erickson
Do you see what he’s done here? He’s multiplied the percentage of tested cases that were positive by the population of the entire stateand called that number, 4.7 million, “prevalence.” He’s then divided the number of deaths by that gigantic made up number in order to make the death rate seem incredibly small.
You are supposed to think, “wait, I heard something like a 3-4% death rate, but he’s saying it’s 0.03%. They’ve blown this whole thing out of proportion!” But the number he is deriving is incredibly small because the fake denominator he has come up with is gigantic; and that is going to be the case for any location regardless of whether they have yet been hit hard by COVID-19, because while he is multiplying the percent of positive tests by the entire population, the number of deaths stays the same. He is comparing known COVID-19 deaths not to known cases, but to a wildly inflated ‘guess’ at the number of cases that is not based on sound epidemiology statistics principles.
In fact, while he isn’t really calculating anything, what he’s closest to deriving by comparing number of deaths to population is what’s called the mortality rate, and since mostpeople don’t die in any given year, this number is always going to be small compared with the general population; any number of deaths looks small compared with 328 million people. This is the reason we talk about mortality and attributable mortality rates in terms of ‘per 100,000 people’, because most of us (myself included) can’t conceptualize the significance of very, very small numbers. If I told you that the mortality rate of heart disease is 0.122% and the mortality rate of cancer is 0.049%, that’s going to be much less helpful than the more typically reported figures of 165 deaths per 100,000 vs. 37 deaths per 100,000, respectively.
So, what he’s giving us is an erroneously calculated ‘death rate’ that is so impressively tiny it cannot be conceptualized and compared well, in place of the commonly discussed and oft debated case fatality rate, which is the chance of dying if you do get the virus.
6:10 “I also wanted to mention that 96% of people in California who get COVID recover.”
Here he has tipped his hat; this is the case fatality rate. You see, the opposite of ‘recovering’ is ‘not recovering’, i.e. dying. He’s sharing the actual case fatality rate, what laypeople call the death rate, but in a form that is unrecognizable.
This is a classic spin technique; flip the statistic so it suddenly sounds like a good thing. “96% is really high! Recovery is good! See, the good thing has a high number, so we are fine!” But if 96% recover it means that 4% die, and that number is astronomical for a case fatality rate, far closer to the Spanish Flu epidemic (2.5%) than to the seasonal flu; and this is just in an area where the healthcare system is otherwise slow due to COVID-19 concerns; in places where hospitals are overwhelmed, the death rate (case fatality rate) is much higher.
6:12 “With almost no significant continuing medical problems (sequelae)”
It is way, way too early to know what the long term sequelae from surviving this virus are going to be.
6:28 “This is our own data, this isn’t data filtered through someone.”
Like, for instance, an epidemiologist who could help make sense of it for you? Sorry, I’m getting snarky again.
6:42 This is exactly backwards; the more the prevalence data goes up, the more positive tests you will get; but because it’s the real prevalence and not the erroneous prevalence he has calculated, that increasing prevalence will be accompanied by increased hospitalizations and increased deaths.
6:47 He’s just admitted to the calculation error I was talking about earlier. Incredible.
6:53“Millions of cases, small amount of death”.
He says this over and over again; it may as well be the title of the video. Except it isn’t true; there isn’t any evidence that there are millions and millions of cases in California (41,000 confirmed at this point), and the number of deaths is anything but small. By the end of this week we will likely have passed the deaths from the worst flu season I’ve ever experienced, 2017-2018 (62,000 deaths), and epidemiologists believe we are underestimating the number of deaths from COVID-19. Moreover, this hasn’t peaked yet in most areas of the country; if we stop mitigation efforts, this could blow anything in our lifetimes right out of the water.
7:05–8:56“So I want to look at New York State.”
25,272 Positive Cases
649,325 Tests
19,410 Deaths (not sure where he got this number from)
“That’s 39% of New Yorkers tested positive for COVID-19”
At this point one of the reporters clarifies that it is not 39% of New Yorkers, but only 39% of people who were tested in New York State, and how if it were 39% of New York’s population that would be nearly 10 million cases of COVID-19 in that state alone. This is an incredibly important distinction. Dr. Erickson acknowledge this but fails to understand the implication; he is still insisting that you can “extrapolate” data from the testing that has been done.
An explanation of why we can’t extrapolate the information he thinks we can, and how we could get that data.
This data can’t be used for the purposes he is trying to use them for, for at least three very compelling reasons. First, it’s the wrong testing strategy. He keeps saying you can extrapolate the test data we have to the general population, but the people who were tested do not represent the general population. They have self selected due to exposure or illness and, especially early on, had to meet very strict criteria (or be an NBA player or celebrity) to even get tested in the first place because of the shortage of tests; these tests were done on the people who were already the most likely people to have COVID-19, and so their percentage of positive tests (39% in New York, 12% in California per Dr. Erickson) is going to be far higher than any other group. Even accounting for asymptomatic carriers, there is no reason to believe that asymptomatic people would have the virus at anywhere near the rate of people who have symptoms of the virus. This is… pretty common sense stuff, actually. For testing to be used to extrapolate to large numbers that give us population level data, it has to be random, and this is the opposite of random. So it’s the wrong strategy for the conclusions he is drawing.
But even if it were random, it simply isn’t the right sort of test for that. The current tests detect COVID-19 (SARS-CoV-2) antigen; circulating proteins specific to the virus; it is detecting the virus itself. It can do this before the patient is symptomatic if the virus is replicating inside them, but not once the virus has been eradicated from the body. Because of this, it’s actually the wrong test for the job; a person can test negative once they have recovered, so they would be miscategorized as a ‘negative’ test even though they had already had the virus. At best, a sufficiently large number of (random) tests done on the same day could give you a snapshot of how many people have the virus at any given time; this is called point prevalence. If this were at all possible, it would indeed be helpful for knowing the current risk of being exposed to the virus (though it would change quickly and require serial rounds of testing). But you can’t use it to determine a death rate; for that we need period prevalence, the total number of cases throughout the time period of the pandemic, and for that we need to know who has had the virus, not just who has it now. So, it’s the wrong test.
But it’s also the wrong time. If we want to know the final, true case fatality rate for COVID-19, which we all expect to end up being very high but much, much lower than the astronomical numbers we are seeing now, we are going to need that period prevalence for the entire period of time of the Pandemic. Even if Dr. Erickson’s calculations were correct up till now (and they are so, so not), it would still be the wrong time to rely on them because many of the regions he is discussing, including his home state of California, have not yet hit their surge. We don’t know what the death rate in California will be because the virus hasn’t come and gone yet; their healthcare system, doctors, and nurses are yet to be tried. It is the same in Waco; we are still in the long calm before the storm, hoping that something will give (a vaccine, a brilliant epidemiological strategy, a radical new treatment being discovered, seasonal decrease in transmission, etc) and we won’t have a surge at all.
So, what would an ideal testing strategy look like if we really wanted good quality case fatality data? It would use antibody testing (which tells us if the person has ever been exposed and had an immune response to the virus, not just if they have it right now), would be random, and would be done after or at least at the tale end of the pandemic. This would take into account asymptomatic and minimally symptomatic cases, and people who had symptoms but never got tested at the time. With a sufficient number of tests it could be used to extrapolate data for the entire population with a good degree of reliability. He’s probably right that we won’t ever do testing quite like that; but since there are potentially lots of other uses for antibody testing, and some of it involves testing people who aren’t actively ill, it is likely that we will get data that can at least be legitimately used to derive some idea of prevalence and true case fatality rate.
While we are discussing New York and possible testing strategies, it is important to note that there is some preliminary data about the actual prevalence coming out based on the antibody testing we discussed earlier, and the news is indeed hopeful; but even the most optimistic numbers so far only get the case fatality rate down to about 0.5% in New York, when you include asymptomatic carriers, assuming the sample is representative; 5 times higher than the number Dr. Erickson has landed on, and still incredibly dangerous. This is a number most of my colleagues would believe sooner than something apocalyptic like the 8-12% in overwhelmed healthcare systems across the globe, and Physicians and Epidemiologists have anticipated and saidfrom the beginning that these numbers would drop significantly once broad-based testing and antibody testing were available. But unlike Dr. Erickson, most doctors I know are not comfortable making that kind of stuff up and would prefer to wait for data that actually has a logical connection to the questions we are asking.
But even as more random antibody testing is done and death rates for COVID-19 hopefully trend down away from the utterly incomprehensible numbers they are at now, please remember; it isn’t just the case fatality rate that makes a disease dangerous, it’s also the degree of infectivity. Even if COVID-19 settles out to be less deadly per case than the bubonic plague or ebola or the Spanish Flu Pandemic of 1918, it can still kill incredible numbers of people if it makes up the difference by being highly contagious… Unless our mitigation strategies can prevent it from spreading.
8:12 Reporter: “Those models were based off if we did no social distancing.”
Dr. Erickson hand waves this off, but it’s an important point for understanding the timeline of this pandemic and understanding that those models are still a real possibility if we stop mitigation efforts.
It’s also an important opportunity for demonstrating some intellectual integrity, since the reporter is correct that those models were for scenarios where social distancing wasn’t followed, and Dr. Erickson has been dismissing them as ‘wildly inaccurate’. Sadly he fails to rise to the occasion and acknowledge this.
8:54 “We extrapolate out and use the data we have, because it’s the most accurate we have, versus the predictive models that have been nowhere in the ballpark.”“
This is a blatant false dichotomy. The predictive models were done to show the range of possibilities of the impending danger if no action was taken; the antigen testing strategy to identify and isolate cases. Neither can be used to establish actual prevalence, but he wants us to think we have to accept his calculations, based on erroneous assumptions, because it’s the only option.
8:59 “So how many deaths do they have? 19,410, out of 19 million people. Which is a 0.1% chance of dying from COVID in the state of New York. And they have a 92% recovery rate! (Edit: That’s an incredibly high known case fatality rate of 8%!) Millions of cases, small amount of death. Millions of cases, small amount of death.“
I want to be as generous as possible here. I really believe that this could be me, were the circumstances different, going on youtube and sharing these false statistics. Yes, Dr. Erickson has financial interests at stake here, but so far I’ve been inclined to think that he really believes his numbers. When you are pouring over data like this for hours or days and you think you’ve hit on some vital statistic that nobody else is picking up on, and it confirms what you already really, really want to believe, it can be so easy to get tunnel vision and not check your math against the backdrop of reality.
But New York should have been the “Aha!” moment for him; the point where he sees the house of cards he’s built collapse so he can start over from scratch with all of his equations. 19,000 deaths; 19,000 deaths in one state, in one month. Overwhelmed hospitals, too few ventilators, nurses and doctors collapsing at work. These stories from the front lines should be enough to make him question the conclusions he is drawing.
If you are calculating a pediatric dose of antibiotics and arrive at instructions that tell the parents to give 28 teaspoons three times per day, you’ve made a mistake somewhere; it doesn’t matter if your math was perfect, something must have gone wrong because those numbers don’t mesh with reality. If you are trying to figure out how long it will take you to drive from San Antonio to Waco and google maps tells you it’s 22 hours, something went wrong; it doesn’t matter how good their calculations and traffic algorithms are if the app thought you meant Waco, Montana instead of Waco, Texas. And if you are trying to derive real-life mortality data from numbers available on google and discover that a virus that is killing tens of thousands in a short amount of time, overwhelming hospital systems, and leaving your colleagues in New York with post traumatic stress disorder is actually not that dangerous, you’ve probably made some flawed assumptions before you even fired up your calculator. Your mathematical conclusions have to line up with reality, and hisdon’t.
He has concluded that COVID-19 is no worse than the flu, which in any given year will kill between 10,000 and 60,000 people nation-wide over 3-5 months. But the deaths of 19,000 human beings, with friends and families, who wouldn’t have ‘died anyway’ at this time, many while their doctors and nurses looked on helplessly because they had not the time or lifesaving equipment to intervene, in one state in one month, should be a wake-up call even for him.
9:48 “We’ve tested 4 million people. Germany is at 2.” The population of the US is 330 million and the population of Germany is 83 million; their tests per capita is double ours. He hand waves this with ‘sure I realize their populations are lower, but…’ Don’t trust anyone with your statistical analysis who waves away the single most important statistical number for comparing countries, their respective populations.
And at this point, mercifully, the video has been removed from Youtube for spreading verifiably false information. This is a double-edged sword, because it inevitably means that copies of it will be spread elsewhere with the heading “BANNED FROM YOUTUBE!”, and even more people will click, watch, and be deceived (or more likely, further entrench the false narratives they have already chosen to believe before watching). If someone does have links to the video when it’s up again, please send it my way so I can finish the other (checks notes) 45 minutes of the video.
But some sanctions cannot be waived away by your being popular with conspiracy theorists. The American College of Emergency Physicians and the American Academy of Emergency Medicine today released a joint statement condemning the irresponsible and flawed information in the video. And while the parts that we have covered so far have been mainly bad statistical analysis disconnected from reality, there are statements made by these doctors later (which I cannot now quote verbatim) that much more flagrantly disregard the oath they took in medical school. I honestly hope these are played back for them the next time they are set to renew their board certifications, and indeed their medical licenses.
With the video down, I’ll have to conclude here for now, and considering the number of charts I need to close for clinic, I can’t thank YouTube enough for taking down the video when they did.
Over the next 10 minutes or so, Dr. Erickson applies his same flawed methodology to other countries, multiplying their positive test rate by their total population to come up with his fake prevalence numbers, and then dividing the number of deaths by that to show how not dangerous the virus actually is. “Millions of cases, very small deaths.” If the video ever comes back, you can watch him do it time and time again, as a tutorial of sorts, so that you too can enjoy creating your own fake statistics at home.
And this leads him to conclusions which, while obvious from his erroneous numbers, defy both our reason and the experience of our fellow human beings. He concludes, remarkably, that the COVID-19 virus has not been that bad even in Italy and Spain, where it decimated the healthcare infrastructure and killed tens of thousands. He concludes that the difference between Norway’s 200 deaths and Swedens’ 2000 deaths is statistically negligible, and therefore social (physical) distancing measures don’t actually matter. He does this because, again, he’s invented a sufficiently high denominator for his “prevalence” that literally any number of deaths is going to seem “insignificant,” at least statistically.
Sweden’s Population: 10.2 million.
Deaths in Sweden (without mitigation strategies): 1,765
Norway’s Population: 5.4 million.
Deaths in Norway (with mitigation strategies): 182
14:30 Dr. Erickson: “1,700 (deaths), 100 (deaths); these are statistically insignificant.”
I want you to stop and say that out loud a few times. Go ahead.
These lost lives are not insignificant; statistically or otherwise.
One more thing I remember specifically, because it was so shocking to me at the time. He goes on to talk about the way that the mortality data is being ‘manipulated’, even saying that a deceased patient with COPD (Chronic Obstructive Pulmonary Disease) who contracted COVID-19 has not actually died of COVID-19, but from 25 years of smoking… As though the medical vulnerabilities that predispose a patient to becoming a victim of this horrible virus and the pathology caused by the virus itself are mutually exclusive. As though tens of thousands of COPD patients who have been smoking for decades were suddenly going to go into respiratory distress in April 2020, apart form any exacerbating factors, and their happening to have the virus that is also killing people with heart disease, diabetes, compromised immune systems, and even the young and healthy is just some weird coincidence.
Bad at statistics is one thing. This is bad at being a Doctor.
I want to begin by acknowledging that the headline to this article is quite snarky. While I try to write about these issues of medical misinformation with some degree of charity towards those I disagree with (and often fail at that), writing titles to posts doesn’t allow for quite so much nuance; I honestly find it to be the most challenging thing about blogging.
Here is a video that was recently shared on my friend’s Facebook timeline. It is mercifully short (less than 5 minutes) and I have included the link for those who would like to watch it in it’s entirety. My friend is an Emergency Physician in New York state, and she was probably on shift when this was shared to her wall. Later on she did leave her own comments, and I have chosen to include some of them, and snippets of our conversation afterward, in this blog post. Let me tell you why.
This was about the guy in the video, not about me. I’m pretty sure.
I tend to believe that while the people generating these conspiracy theory videos are motivated by desire for some combination of fame, power, or fortune (and this video may well be an exception to that) the people who are sharing them widely on social media and forming opinions based on them are more victims than accomplices. They are being given false information exactly calculated to appeal to their fears, their political leanings, and their preconceptions, and they are deciding to place their trust in these so-called experts because they themselves do not have the background or knowledge base to parse the information on their own. Without a background in statistics, medicine, epidemiology, etc. they feel they have no choice but to trust one “expert” or the other, and all too naturally quiet their own discernment and choose the one that reinforces their own views. The problem is that while one group of experts have devoted their lives to rigorously studying disease and the human body so that they can help those who are suffering, the other group of “experts” are actually only experts in engendering this sort of trust, and not in the areas of knowledge they claim to understand; they are essentially false information experts.
Because of this, I do try to approach these topics with gentleness, recognizing that it is easy to be deceived and hard to sort truth from fiction. I have that privilege because right now the COVID-19 pandemic has really impacted my life quite minimally, compared to the rest of the world. Katie is still homeschooling and I am still going into work. We haven’t hit a surge yet and so while I have seen COVID-19 patients, and we have had some deaths due to the virus in Waco, I am not being called upon, at this time, to work extended hospitalist or emergency room shifts trying to care for patients in an overwhelmed hospital with physically and emotionally exhausted staff and colleagues.
But my friend is working under exactly those circumstances, and if she’s a bit more adamant than I am about how hurtful, how dangerous, and how dehumanizing these types of nonsense and lies are to not only the victims of this terrible virus, but also to the healthcare workers fighting it… well, I think she’s perfectly entitled. Please trust me, if she found these falsehoods shared on her Facebook wall by friends or family members when she came home from a shift where multiple patients died or were admitted to the ICU due to COVID-19, she could be considerably more vociferous if she chose.
I’d like to devote a separate essay to the the main point of his video, which to him constitutes “100% proof” of fraud and a major international conspiracy lead by WHO and the CDC, and apparently involving doctors and healthcare workers across the globe. This revolves mainly around CPT codes, and the “two CPT codes” being used for COVID-19 in order to cook the books “right in front of your eyes.” We are going to go into this in more detail, hopefully sometime in the next 2 days, but first I want to discuss the other issues he raises in the video.
Home Isolation
At the 1:46 mark of the video, Mr. McCarthy says, “Here’s a document from the CDC dated July 2020 (Note: this means that the article is due to be published in July, not that this article is from the future, as helpful as those would be if we could get our hands on them) that clearly states…”
“In addition, our findings suggest that home isolation of persons with suspected COVID-19 might not be a good control strategy (McCarthy: Oh there’s a shocker!). Family members usually do not have personal protective equipment and lack professional training, which easily leads to familial cluster infections.”
He concludes, “meaning it’s making it worse, not better folks!”
This is a direct quote from the study below (image links to full article on CDC website).
His point here seems to be that having people who are actually suspected of having the virus stay medically isolated at home is actually worsening the pandemic. Which is… pretty nuts. We are not even discussing broad based social/physical distancing measures and shelter in place orders here, but actual management of suspected cases. It’s hard to imagine in what way, or compared to what strategy, having these patients isolate at home would make things worse. Would he prefer for patients with suspected COVID-19 just go back to work, despite their cough and fever, and wait for their test results? Does he think that patients wouldn’t be in their homes exposing their families at all if not for doctor’s orders? He doesn’t say, but the implication, in the context of the rest of the video, is that having patients who are actually ill keep themselves at home and away from the general public is yet another tool of the COVID-19 conspiracy… As opposed to being a common-sense step we already take for pretty much every other contagious illness.
It’s hard to know whether Mr. McCarthy is simply confused in thinking that the article’s point is that home isolation is too draconian, or if he is intentionally drawing the wrong conclusion in order to deceive his listeners. Sadly, I think it must be the latter, because the very next sentence of the article reads as follows:
“During the outbreak, the government of China strove to the fullest extent possible to isolate all patients with suspected COVID-19 by actions such as constructing mobile cabin hospitals in Wuhan, which ensured that all patients with suspected disease were cared for by professional medical staff and that virus transmission was effectively cut off.“
So the opinion of this articles authors is that having suspected COVID-19 patients isolate at home is not nearly extreme enough to prevent spread of this virus, and that patients should be kept in mobile hospitals instead. Considering that his very next point is that hospitals are manipulating the COVID-19 data to make money, we must concluded that his omission of the very next sentence and his substituting his own conclusion, which is the exact opposite of that drawn by the study’s authors, is actually intentional.
Hospitals are miscategorizing people as COVID-19 patients because of the CARES Act.
This claim, which is implicit throughout the video, is explicitly stated at the 2:56 mark:
“All they have to do is use the right code! Why aren’t they using it? Because the average COVID-19 case for medicare or medicaid is between $13,000 and $100,000 right now folks. So by flipping this number to this number (pointing back to the CPT codes), the hospitals are making a tremendous amount of money off of medicare and medicaid… It’s absolutely fraud.”
Now, there’s a lot wrong and just plain silly with his take here. There’s the fact that our healthcare costs in this country are so inflated (largely because of the hospital-insurance company arms race) that those numbers, which he means to be a ‘they are charging how much!?’ moment… really aren’t all that shocking (also, that’s a pretty big range there). There’s the fact that using one COVID-19 code vs. another based on whether a test was positive isn’t going to affect billing or epidemiology data (we are going to go into this in more detail in the next blog post). And there’s the fact that this really does seem like the type of information that, like the last example, actually proves the opposite of his point if it proves anything at all. Many patients with COVID-19 are incredibly, unbelievably sick and require high levels of support and prolonged hospital stays (we have been closely following the story of a man here in town, a friend’s brother, who has only just returned home after over a month in the hospital, including an extended ICU stay), and quoting numbers about the exorbitant expenses associated the disease really shows two things; we need to move away from a for-profit model of healthcare in this country, and this is a very, very bad bug.
But unlike nonsensical theories of 5G towers reprogramming our DNA or defeating COVID-19 by doing a cellular health detox cleanse, most Physicians are not so quick to dismiss the idea that some in hospital administration and corporate medicine might see government provision for COVID-19 treatment, such as that provided in the CARES Act, as an opportunity to profit; or at least to make up for lost revenue from cancelling elective surgeries and decreased admissions leading up to any COVID-19 surge. I have known hospital and clinic administrators I trust implicitly, and I have known hospital administrators who have lied directly to my face; but most probably fall into a very broad category of people who just have different values and convictions around what medicine is supposed to be than I and most other Physicians hold to. At the end of the day, I tend to think it’s a bad idea in general to have the practice of medicine driven by, in so much as it is driven by, people who have studied and been hired to increase profits and market shares rather than people who have taken an oath to do no harm and to aid the suffering. It would be somewhat naive to expect that dynamic to disappear entirely in a pandemic.
But let me be clear; if a handful, or even a large number, of unethical hospital administrators are actually trying to commit fraud to gain access to additional payments related to COVID-19, either by attempting to influence clinician decision making or by actually modifying medical records, those people should be convicted. But even if this were the case, I do not believe for a moment that such activity has any way of significantly changing the hard data we are seeing, for a few reasons.
First and most importantly, the numbers we are seeing do match the experiences of doctors and nurses on the ground. Doctors have a good gauge for what a bad flu season looks like or when a viral GI bug is going around, and generally have a bead what is happening with the health of their communities. It is absurd to believe that doctors and nurses who are suddenly fighting for their own and their patients’ lives against this horrible virus have all been wrapped into some big conspiracy to profit hospital administrators and stock holders. That’s why the ‘hospital administrator cooking the books’ (note to self: new idea for a Les Mis parody song) idea tends to be a final redoubt for conspiracy theorists once they have been confronted by actual doctors and nurses, who in the cultural atmosphere since COVID-19 they no longer feel they can get away with calling liars and conspirators directly to their faces.
But it also doesn’t make any sense to equate medicare or medicaid fraud related to COVID-19 to an inflation of the epidemiology data, because even if EVERY hospital administrator were in on it, they would still have very limited influence on that data. They would not, for instance, be driving to community based and free standing labs to convince lab techs to report positive tests, so they would have a better COVID-19 paper trail if those patients showed up in their ER’s later. They are not going to unaffiliated, clinics and underserved healthcare centers and convincing Physicians, NP’s and PA’s to fudge their evaluations to make COVID-19 look more prevalent. They are not telling ICU and Emergency Room doctors when a patient’s respiratory status is sufficiently dire to require a ventilator (I have actually heard of such cases in the past, and those administrators were promptly reported for practicing medicine without a license), and at any rate if they were they would be ignored. They are certainly not killing people; it is the virus that is doing that.
Just like with pharmaceutical companies, insurers, drug reps, home medical equipment companies, and so, so many other players in the healthcare arena, Physicians have complicated and often antagonistic relationships with hospital administrators. But even if you believed that every single hospital administrator were corrupt and currently working overtime to try to game the COVID-19 situation, there are just so many other people involved in tracking this data. There are epidemiologists and infectious disease doctors, the local public health department, the coroner’s office, local and state government officials of all political influences, and many, many people evaluating this data from every possible angle to see what we might be missing, or what patterns might help us be prepared for what comes next. And finally there are the people living through this pandemic; the doctors and nurses and respiratory therapists, yes, but also the patients, those living and those deceased, and their friends and family and loved ones. These are the people who are robbed of their dignity and their opportunity to grieve and process in peace when people like Daniel McCarthy erroneously claim that COVID-19 is being blown out of proportion to make money for a fairly small group of businessmen.
The flu kills more people anyway.
It’s hard to know exactly what point he’s trying to make by touching on influenza death and hospitalization data toward the end of the video. My hope is that he’s merely pointing out the importance of having reliable data. If so, I would agree with him, although from the rest of the video I don’t think I would trust him to recognize it once we had it. Unfortunately, however, I think he is simply reviving the ‘it’s just another flu’ rallying cry that we’ve heard consistently for months from those ignoring the realities of the COVID-19 situation; if that wasn’t his intent, my apologies to Mr. McCarthy; it’s a good thing for us to talk about here at some point anyway.
I’m honestly so sick to death of this one. It is the end of April and I am sure that this has been explained to Mr. McCarthy several times by now, so I can only assume he has chosen to perpetuate the lie that COVID-19 is ‘basically just like the flu’ because it fits with his narrative, and not out of actual ignorance. I hope I am wrong about that. I won’t go into extensive detail (I have included a link to an article below), but essentially the flu is a partially vaccine-preventable virus that demonstrates seasonal prevalence and has a high rate of mutation. Because of this, epidemiologists have to try to predict which strains of seasonal flu are likely to be prevalent in the coming flu season so that vaccines can be prepared. Some years these are more effective (and more widely accepted) than in other years, and some years the seasonal flu strains are more dangerous or more widespread than other years. This means that seasonal influenza has the potential to be very, very bad in any given year; but also that there is a high degree of variability.
In addition to flu vaccines, there are several mitigating factors that help keep the flu from overwhelming our hospitals and healthcare infrastructures every Winter. First, flu season is fairly long; usually above 3 months, with a high degree of chronologic and geographic distribution. This means while hospitals are sometimes extremely taxed by the flu, it is rare for them to actually be overwhelmed; though there are certain years and certain locations that come very close. If you consolidated the impact of even a light flu season into a 1 month period, affecting every community in the country at roughly the same time, it would absolutely overwhelm our healthcare systems and people would begin to die not just from the flu but also from our inability to provide care for other conditions while battling it; and this is exactly what COVID-19 does threaten to do (and has done) because of it’s much higher degree of infectivity and, likely, higher degree of asymptomatic or minimally symptomatic spread compared with influenza.
Second, we know the flu is coming. Each year Physician, Nurses, and other healthcare workers make strategic decisions leading up to flu season. When I have taken leave to work internationally, we have always scheduled that time during the late Spring or Summer, when I knew I would be less needed because we wouldn’t be in the midst of fighting the flu. Staffing decisions and other resource organization is made based on the expectation of a surge, even if the exact timing and parameters of that surge are unknown. With COVID-19, there was no preparation time in those regions that were hit earliest, and the rest of us have been scrambling ever since to ensure that our systems are ready for a surge that is unpredictable because there are no decades of past data to help us now what to expect at our hospital or in our region.
Third, we already how to deal with the flu. While influenza seasons and symptom clusters do vary, the syndrome is very recognizable and we generally have a good idea of what to expect with flu cases, and how they interact with other acute and chronic illnesses. As several quotes I’ve read recently have said, “The flu is an old enemy.” Yes, it is a very, very dangerous enemy, but it is definitely ‘the devil we know’ compared to COVID-19. We have years of research and clinical experience to help us. We know which medications have modest therapeutic benefits and which have none, and what strategies to use when patients present for dangerous complications of the flu, such as post-influenza bacterial pneumonia, or when it causes complications in preexisting lung disease. With COVID-19, new data is still emerging continuously about both the strange spectrum of harm that this virus causes, and the possible treatment approaches; those fighting the virus later in the course of this pandemic really do stand a better chance of both diagnosing it accurately and treating it effectively.
Finally, the flu itself is already bad enough, and dismissing COVID-19 as ‘basically another flu’ just shows how the people spreading these ideas are already in the habit of dismissing incredibly dangerous infectious illnesses. Already COVID-19 has killed more people in the US than almost any flu season, and yet people are still waving it off as ‘another flu’ the way they were weeks ago when it had ‘only’ killed a few thousand. In the coming days the total number of deaths in the US will surpass the 62,000 mark set by the 2017-2018 flu season, the worst we’ve had since I’ve been a Physician. Once this benchmark is passed, will these conspiracy theorists finally abandon the ‘it’s just like another flu’ argument, or would they like to hold on to it until COVID-19 has actually surpassed the numbers set by the Spanish Flu pandemic in 1918?
The amount of medical misinformation out there right now is staggering. Would-be alternative health celebrities see the COVID-19 pandemic as their opportunity to make a name for themselves and increase their fame and fortune, and their videos seem to range from 5 minutes of mostly benign half truths, to one I saw today that was 48 minutes of crazed rantings. As a Physician, I despair of being able to address even a fraction of the misinformation my friends and family are being exposed to right now.
But you have to start somewhere. One of the biggest areas around which falsehood and distortion crops up consistently is the role of your immune system in fighting disease in general, and in protecting you against COVID-19 in particular. And in this area there are two dangerous distortions that seem to crop up again and again. But to address those, I think it’s important that we think of the immune system as a Death Star.
Preamble 1: This is written to Christians, and intended as a call to my fellow believers in Christ to hold to very high standards of truth telling, particularly as it relates to the COVID-19 pandemic we are currently facing. I do think that the general principles I am espousing here apply to others as well, and all our welcome to read and comment.
Preamble 2: In this post I do talk quite a bit about holistic healing/alternative medicine. This is an area of complexity and nuance, but here I am primarily talking about self-proclaimed alternative health “experts”: modern day snake-oil salesmen who are seeking to use the COVID-19 crisis to create a name for themselves and garner greater fame and fortune. I know many of my friends lean towards ‘holistic’ alternatives or adjuncts to modern evidence-based medicine (modern medicine IS holistic but that’s another soap box entirely). I have FB and real life friends who are into essential oils, I have family that swear by their chiropractor, and I myself have received acupuncture in the past (it was kind of fun, to be honest). Most of them, thankfully, also choose to bring their children to the doctor when they are ill and to vaccinate them to prevent communicable diseases. Most of them have been very, very supportive of healthcare professionals in general and of me personally during this pandemic, and I have seen them both seek out and share good, reliable medical information. In short, I have been quite proud of these crunchy, oily friends of mine. If you are reading this as someone who identifies strongly with holistic or alternative medicine, I would ask you to please consider carefully whether the conspiracy theorists and COVID-19 deniers who are so prolific on the internet right now really represent your movement well and are espousing the same values that you find important in your area of wellness. My hope is that you wouldn’t be deceived by them easily just because they are comfortable using the same terminology that you hold close to your heart; an error we in the Church have all too often made with false teachers of all stripes.
“Finally, brothers and sisters, whatever is true, whatever is noble, whatever is right, whatever is pure, whatever is lovely, whatever is admirable—if anything is excellent or praiseworthy—think about such things.”
“Keep your tongue from evil, and your lips from telling lies.”
When the initial wave of concern over COVID-19 began for our clinic system a few short weeks ago, there seemed no end to the things that needed to be done. We had to rapidly prepare to protect our staff and patients by minimizing transmission risk and eliminating fomites, go through all of our processes with a fine toothed comb and revise or rewrite a fair number, and innovate and implement novel ways to deliver high quality primary care under circumstances where it was no longer safe for our patients to sit in a crowded waiting room as they wait to see their primary care Physician, or even pass each other in the hallways on the way to the lab or radiology. This all in addition to learning how to work-up and treat the virus itself. During those first few weeks many of us worked until the wee hours of the morning each night and through the weekends, all the while continuing to see patients, return phone calls, and refill medications. But as these systems have been put into place and fine-tuned, and as the physical distancing and other epidemiology measures on a community level have effectively limited the spread of the virus in our area, life has thankfully slowed somewhat again. Many of us that do hospital work are waiting to see whether more doctors will be needed to cover shifts, or if the shelter-in-place orders and distancing measures will be enough to avoid a true, overwhelming surge. In the meantime we read and stay up to date, we see our patients via telemedicine or in outdoor COVID-19 clinics and work hard to make sure they don’t fall through the cracks, and we prepare, personally and professionally, for worst-case scenarios. Throughout all of this we have each continued to ask ourselves what our next responsibility is as Physicians in the midst of this pandemic.
In answer to that last question, I have found myself more and more called on to provide an answer to misinformation around COVID-19, as friends and family have attempted to sort out the unprecedented amount of misunderstanding and abject falsehood that has been circulated over the past month. To be clear, even in the best of times there is already an overwhelming amount of misinformation around health and healthcare. The nuances of human health and disease and the means available to protect the former and fight the latter are unbelievably complex, and because of this it is easy for an individual who hasn’t spent a lifetime studying this area to feel overwhelmed and disempowered. The temptation of easy answers and quick fixes is very real. More to the point, Physicians have historically done a fairly poor job, in my opinion, of helping our patients to feel empowered and knowledgeable to the greatest degree that is possible without them actually entering the medical field themselves. In this context, it is no surprise that during this time of increased health anxiety and uncertainty, and with a myriad of political and economic motivations to obscure the realities around the virus, the amount of misinformation has increased dramatically. Between my day job, extra duties related to the virus, and this small matter of having a wife and four children, I consider it a real privilege when I have the margin to address a video or article that a friend has ‘tagged’ me in asking for my input.
But though there are plenty of unaddressed articles, videos, and memes spreading medical misinformation on my facebook feed this very day, I am writing this afternoon with a slightly different, though related, purpose. I am writing to call the Church to participate in this work with me.
We are called to be a people of the truth; we are not called to be a people of truth and falsehood mingled. When discussing his conversion to Christianity, G.K. Chesterton wrote, “My reason for accepting the religion and not merely the scattered and secular truths out of the religion… I do it because the thing has not merely told this truth or that truth, but has revealed itself as a truth-telling thing.” As followers of Christ, Christians ought also to have a reputation of truth-telling. Truth-telling in love, when the truths are difficult. Truth-telling in courage, when the the truths are spoken to those in places of power. Truth-telling in humility and repentance when those truths reflect poorly on ourselves or our conduct. We cannot afford the damage done to the witness of the Church by our gaining a reputation as unreliable sources of truth. Yes, physical health in general and the COVID-19 pandemic in particular, as devastating as it is, are still ultimately minor issues compared to the eternal importance of the Gospel; but how can the world around us look to us for the Truth of the latter when we have only provided them falsehood about the former? “Whoever can be trusted with very little can also be trusted with much, and whoever is dishonest with very little will also be dishonest with much.”
For this reason, I believe that our willingness as a people of Faith to perpetuate misinformation, particularly when it may truly injure our neighbors, is not a political issue or even an integrity issue, but a spiritual issue. There is no truth, whether philosophical, metaphysical, or scientific, that does not belong to our Creator; there is no Truth that we as Christians should fear, and there is no falsehood, no matter how convenient to our preferred narratives, that does not originate from our Enemy.
What follows is my take, as a Physician, on what a lay person can do when trying to weigh truth and falsehood and judge the reliability of medical information during the COVID-19 pandemic. I want you to know that I realize it is often very, very difficult. As a Physician I have the privilege of years of education and training in thinking about real and reliable truths about our bodies and the diseases that affect us; it is never my place to judge someone for sharing information they find convincing because they do not have those same experiences and have spent their time in other important work. It is my job, I think, to help my fellow believers supplement their God-given discernment with reliable data and professional insight; we are all one Body, but made up of many parts.
1. Understand your source.
Returning to Chesterton, I think it is reasonable to ask whether the author of the article or the self-purported expert we are listening to has a track record of providing reliable medical information; have they proven themselves to be a ‘truth-telling thing (er, person)’. Many of the people generating widely shared false information are political partisans who have no medical or other scientific background; are they sharing the perspective of actual experts, or are they merely creating false narratives and opinions out of thin air? If the source is not a politician but instead claims to be an expert, what is their education and background? So often we give our trust to people whose primary credentials are an attractive and disarming physical presence and a high verbal IQ but who do not have even the basic science background to understand the frameworks they are tearing down. I have seen youtube videos captioned ‘so and so DESTROYS the COVID-19 pandemic myth’ or ‘Dr. X crushes the CDC and WHO conspiracy’, etc., only to find that not a single intelligible sentence of valid scientific information was uttered during the entire 15 minute video. These are the ‘used car salesmen’ (no offense to actual used car salesmen; I am very pleased with my 2012 Honda Odyssey) of medical information, and their true area of expertise is in pretending to be experts.
Please understand what I am not saying; I am not saying that you must have a certain degree or a certain prerequisite combination of education or work experience in order to have a valid take on the pandemic. But often these videos are made by people putting themselves forward as experts without the credentials to support that claim; the first piece of misinformation is imbedded in their own self presentation. An example is a video a friend recently asked for input on, from a doctor putting himself forward as an expert on the immune system. It turns out that he was not an immunologist or a microbiologist, but a disgraced chiropractor turned “cellular detox diet” specialist. Again, this does not negate what he has to say; but it is a vital piece of context for weighing the claims he goes on to make.
This research is sometimes hard. These people are often incredible at building legitimate sounding resumes for themselves and at using terminology on their websites and bios that smacks of authenticity and scientific rigor. Moreover, there are also those who do have impressive credentials yet have strayed from any integrity in their work and have become deeply unreliable sources of healthcare information in their pursuit of fame or fortune (a fellow MD friend and I often joke, darkly, how easy it would be to make tons of money as a Physician, if it weren’t for these pesky morals). But even if you cannot establish someone’s reliability with a few minutes on google alone, conducting such research will help to answer a few basic questions that should set the tone for the information itself. Is there a direct link between the reach of this person’s social media influence and their opportunities for attainment of power and profit, such as a political office being at stake or a website that sells services or goods directly? Such a relationship would be fairly rare in medicine or academic science. Are the claims this person makes the types of things that would fall within their area of knowledge based on their education and work experience? Are they setting themselves up as experts in areas, such as clinical medicine, immunology, or epidemiology, where they seem to have had little to no experience? Finally, do they have a history of fraudulent claims, moral turpitude, or failed (or successful) scams in the past?
This step is sometimes a bit tedious, but I believe vitally important, especially when some of these videos are made by people who have spent a lifetime mastering the art of convincing others with their looks, manners, and likability. When it comes to medical misinformation, these are the wolves in sheep’s’ clothing of the moment.
2. Do your research.
This second point is so similar to the first that I won’t spent much time on it. Though understanding whether the source is reliable is important, I firmly believe that the content of the argument is more important still. When considering any degree of medical information shared on social media, or even mainstream media, pause to reflect on the main themes and content of the article or video. What was the driving point? What information contradicts that which is already widely available? What data seems shocking or seems to rely heavily on the existence of widespread conspiracies? For that matter, do those conspiracies depend on the sudden cooperation of diverse and often opposed sectors of society, such as the sudden cooperation of politically unaligned nations or the widespread collusion of large groups of healthcare professionals? What part of the information is benign and widely accepted already, and is it being presented as such? Or is there a claim that commonly accepted facts are denied by or unknown to ‘the powers that be’ (the CDC, the medical establishment, etc), and does that seem very likely? What would the major implications be if this video were true, and who would stand to profit by its widespread acceptance if it were false?
This list could go on, and in another time we would have only these important critical thinking questions to guide us to the informational content itself. But we live in a technological age and the odds are that if we are seeing a video, or at least a popular video, it has been critiqued or fact checked already. Read these critiques; seek them out. This alternative perspective, even if it comes from a source you normally don’t subscribe to personally (I know people who despise certain fact checking websites), may be enough to give you the ‘aha!’ moment you need to reach conclusions on the information for yourself. And if you believe the information and think it is worth sharing, then understanding the arguments against it will only strengthen your position.
3. Be honest with yourself about your political leanings.
I’ll keep this one brief because I don’t particularly want to be dragged into a specific political debate, at least at this time. As people of faith who are committed to the truth, we will find ourselves politically homeless a fair amount of the time, and holding onto important caveats and a sense of tension even in our areas of agreement with political movements. When the truth conflicts with the narratives of the political groups with which we most closely align, our choice is clear. Before sharing information from questionable sources, that our research tells us is not reliable, we have to check our politics; we have to be very honest with ourselves regarding whether our impulse to perpetuate the information stems from a real belief in its veracity or from a mere desire for it to be true. I have heard fellow Christians tell me “all politicians lie” (generally to excuse untruths from one group or individual), and then have seen them blindly re-post the lies that come from their own side. I may very well have been guilty of this myself. If we believe that politicians are not reliable sources of information in general (and we can debate later if some are worse than others to an almost unprecedented degree), it means that we will sometimes choose for reasons of discernment not to pass along information that, were it true, would be extremely convenient to our party or candidate. In contrast, if we find ourselves always repeating the party line and reinforcing the narratives of those in positions of power, I fear that we are in danger of rendering unto Caesar something that never belonged to him.
4. Beware of easy answers.
“Reality, in fact, is usually something you could not have guessed. That is one of the reasons I believe Christianity. It is a religion you could not have guessed. If it offered us just the kind of universe we had always expected, I should feel we were making it up. But, in fact, it is not the sort of thing anyone would have made up. It has just that queer twist about it that real things have. So let us leave behind all these boys’ philosophies–these over simple answers. The problem is not simple and the answer is not going to be simple either.” C.S. Lewis wrote this when discussing the reality of Christianity and the complaint heard so often that ‘religion ought to be simple.’ But I think this quote is informative for us in this discussion of medical misinformation. Alternative health popularizers like the ones we are seeing in video after video right now have long mastered the art of combining oversimplified ‘common sense’ arguments with the right kind of complex medical vocabulary (some real, some fake), to appeal at once to both our desire that healthcare should be fully comprehensible and explicable to us and our desire to know we are hearing form an expert. They are experts in tickling the ears, in confirming our biases and ingratiating themselves to a public that is anxious over health and disease. For someone who has actually studied both the real concepts they are distorting and the real vocabulary they are misusing, these arguments are as transparent as they are ridiculous; but they are not trying to convince me, they are specifically trying to convince people who don’t have medical training.
That said, you don’t have to spend your life studying pathophysiology and be intimately familiar with medical terminology to spot these patterns for yourself and know when to be wary. These false arguments tend to fall along a few common themes, and once you learn to spot them you will be a big step closer to at least being able to ask the right questions.
The real solution is easy but they don’t want you to know that.
This one has come up a lot recently as people advocating against social/physical distancing measures (for political or financial purposes) are pushing the idea that other simple measures would actually prevent getting sick from COVID-19. Typically these are oriented around the immune system, and the idea that having a healthy immune system would actually prevent the disease entirely. Aside from being untrue, this is extremely problematic for two big reasons. First, I think we should recognize the degree of victim blaming involved in this line of reasoning; if these 41,000 people who have died from COVID-19 in the US had just taken enough Vitamin C or eaten a healthier diet they wouldn’t have died. Certainly the interaction between health and lifestyle, including limitations in choices and socio-economic vulnerabilities, is complex. But there is not a set of choices that can make someone immune to illness in general, and in the case of infectious diseases specifically there is not a combination of lifestyle and nutrition that can make a person invincible (even Chris Trager got the Flu on Parks and Rec). Second, just consider the sheer number of people who would have to be in on such a conspiracy. Millions of doctors, nurses, and public health experts, many of whom have themselves become ill or lost friends and loved ones. The idea that all of these people are interested in covering up that a certain number of milligrams of Vitamin C or a certain number of hours of sunlight exposure could have alleviated all of this suffering is not only incredibly naive, but also unbelievably calloused.
Germs are good for you.
This is an argument that crops up when discussing any infectious disease, but it is particularly popular now. Many alternative health and particularly detox and microbiome style wellness salesmen are all too quick to tell you that viruses, bacteria, and fungi are important for us; that without them we wouldn’t have functioning immune systems. And they are right. But like so many of their arguments, they have taken just one piece of the incredibly complex story of human health and disease and have extrapolated it to illogical and harmful proportions. I have written about this more extensively recently, but they are essentially failing to make two important points. First, the difference between a microbe (any bacteria, virus, or fungi, etc) and a pathogen, which is a microbe known to cause human disease; it is absolutely not true that because ‘germs are good for us’, therefore infectious diseases are good for us. This virus can definitely kill you. And second, the role of an acute infection in establishing a secondary immune response. Yes, exposure to a pathogen does generally cause some degree of enhanced natural immunity against that same pathogen later (this is the entire principal upon which vaccines are based); but it is not necessary to allow yourself to get ill or indeed become as sick as possible in order to build that robust secondary immune response, and sometimes the risk is much greater than the reward. “Whatever doesn’t kill you makes you stronger” still implies that dying is at least on the table.
I won’t rehash all the points I wrote about last week, but instead will share a quick story. When we lived in Denver we were visiting with a friend after church who showed us a fairly deep cut to his finger, near the joint, which he had received that morning. My wife, an RN, asked what he had used to clean the wound. He explained that he had NOT cleaned the wound because his body needed the germs to build an immune response, and that soap and water would prevent his body from fighting off the infection ‘naturally’. Katie attempted to persuade him otherwise and explain the roll of his immune system and ways he could help his body prevent an infection, but he wasn’t convinced. Two weeks later we saw him again, this time with a large bandage over his finger. We asked about this and he explained how his finger had become infected and he had to go to the emergency room, undergo and incision and drainage procedure to remove the pus, and then take antibiotics. He went into glorious detail about the procedure and the appearance of the infection and even showed us pictures. He did all of this without any sign of chagrin, and to this day neither of us is sure whether he had forgotten the first conversation entirely or if he is just the world’s most humble man.
And while what happened to my friend is funny in retrospect, because his finger fully recovered, it is certainly not funny when someone contracts a deadly illness because they are misled into thinking it’s actually better for their health.
The doctors don’t understand (or indeed know about) the immune system.
I’m always amazed when this one makes the rounds because it’s just such an incredibly goofy thing to say. We could spend paragraphs discussing the thousands of hours spent in medical school understanding every aspect of the human body and the huge swaths of microbiology, biochemistry, pathophysiology, infectious disease, anatomy, and pharmacology coursework that were devoted to understanding our fearfully and wonderfully made defenses against infection. I promise you we spent so much time studying the immune system that we dreamed of angry macrophages and inflammatory cytokines. So why such a silly and nonsensical lie? They are setting up a false dichotomy between your own immune system (which they would like to sell you products and services to augment) and the “big-pharma model of medicine”, a red herring of their own invention, which only believes in harsh chemicals. They have to reduce modern medicine and the scientific discoveries of the human body to just this one aspect in people’s minds so that they can claim for themselves the parts of it which seem to sell best. Whether the hucksters making such claims have actually studied the immune system in an intellectually honest and scientifically rigorous way themselves, however, is a question that perfectly justifies speculation.
I explore the rest further in the next section, but a few more, briefly:
The doctors want you to stay sick.
This is 100% a lie. Don’t be fooled by ‘common sense’ arguments that suddenly call for millions of well-meaning people to act nefariously.
The doctors are being controlled by big pharma.
Don’t be fooled by arguments that require passionate, notoriously difficult to control, and (let’s face it) often egoistic people to suddenly be submissive. Physicians are one of the primary reasons that pharmaceutical and insurance companies don’t yet control all of healthcare.
The doctors mean well but have been tricked.
Don’t be fooled by arguments that require very smart people to suddenly be easy to dupe.
5. Ask your brothers and sisters in Christ.
One of the many false narratives that Christians seem to believe at an alarming rate is that the medical field is somehow opposed to the Church. It is easy to point to controversial areas of medicine, or even the general principles of understanding illness and health as primarily physical phenomenon, to say that modern medicine is at it’s core agnostic or secular, and thus antagonistic to the Faith. This is an incredibly profitable narrative for televangelists and healing charlatans who would like you to believe that pursuing any means of healing aside from the overtly miraculous is a sign of lack of faith, and who exploit our fears and insecurities around health to sew mistrust in Physicians and other health professionals for their own profit. Perhaps a step down from the overt chicanery of these false prophets, we also see a strange marriage between Evangelical Christianity and unproven and sometimes even dangerous alternative health measures, which are marketed, sometimes, with a heavy mix of pseudo-Christian spirituality.
But if this is true, what then do we do with the millions of doctors, nurses, scientists, epidemiologists, and others within the healthcare sector that are faithful followers of Jesus Christ? I think the first temptation, too often, is to treat them like they are ‘one of the good ones’; as though a Christian Physician you know personally may be a reliable source of health information, but the medical field, in general, is not. I think this is incredibly problematic. As someone whose 20’s and 30’s were devoted to medical training, I have known hundreds (maybe thousands) of doctors personally. My older children who grew up during my residency thought that “Dr.” was just a gender-neutral way to say “Mr.” or “Mrs.”. Because of where I have trained, many of these have been believers; but just as many that I have trusted and respected have not. Yes, I have certainly met doctors I would not trust with my own care or that of my family, but these have been remarkably, surprisingly few compared to the number of doctors I have known and worked with. In general I can say that Physicians as a group have self-selected for (and certainly this has been reinforced by training) both their desire to see people well and their commitment to scientific accuracy. To be clear, some of these doctors I disagree with vehemently on issues within medicine and the associated underlying moral and societal values. Nevertheless, and regardless of the cultural misrepresentations, your doctor wants you to be healthy and is, in general, a good and reliable source of information about health and disease. If they aren’t, you should get a new doctor immediately.
As we touched on earlier, a second and similar way to treat Christian Physicians and healthcare workers is as well-meaning but ultimately misled pseudo-experts with only a narrow scope of understanding regarding the human body. This is the view pushed by many in alternative health businesses; doctors are generally altruistic or noble, but they have had the wool pulled over their eyes, their education is controlled by Big Pharma and hospital administrators, and really all they are learning is essentially spreadsheet after spreadsheet of ‘if the patient has this, give them one of these drugs (and here are the prices; pick the most expensive one)’. Medical schools and residencies exist to train doctors to create profits for drug companies. Now, this is an incredibly silly idea and we could devote as much time as we wanted to this. I could explain that I never met a drug rep until after residency, because they generally aren’t allowed to interact with medical students or residents, and have never made a medical decision based on the advice of a drug rep in my life (except for Burton “Gus” Guster, of course). I could (and should, at some point) explain the very complex and often antagonistic relationship between systems within medicine that prioritize profits over people, including pharmaceutical companies, and the physicians, nurses, and clinical staff who exhaust themselves to help their patients find something like justice and equity in their healthcare. But these are areas I am passionate about, and I’m afraid this one section would eclipse the rest of the essay entirely.
Instead, I’m willing to bet that if took a step back and consulted even your own experiences with doctors you know personally, you would realize that their knowledge, education, and personal characteristics does not seem to match this narrative. If you have physicians in your family,, or in your church or Sunday school class, or have attended high school or college with them, or have friends who are doctors- in short, if you do know believing medical experts that you would ask for input on these videos and articles being circulated- ask yourself if they are a reliable source of information even aside from their medical background. Are they the type of people who are easily duped? Do they hold to questionable morals or a low view of the truth? Do they seem to possess discernment? Essentially, are they the type of people you would trust outside of a pandemic to answer questions unrelated to viruses and immunology and epidemiological data? If they are not, I would humbly suggest that you do not turn to them now, regardless of how closely the information you need clarified matches their field of work. But if they are, I would recommend showing them the courtesy to believe that they have applied at least that same degree of critical and independent thinking and that same spiritual discernment to the endeavor that has taken up the majority of their adult lives; namely the study of human health and disease.
Finally, my advice when framing these questions: be specific. When I am asked by a friend or acquaintance to address a viral video or a healthcare related article or meme, I try to be as thorough and complete as possible (I do find that after a few thousand words of my ramblings, they usually don’t ask a second time…). This can be time consuming, but I believe it is important work, and I personally have no problem being asked a general “would you give your input on this.” Not all healthcare professionals have the inclination to be quite so verbose, and of course many of us want for the time to do so now more than ever. If you ask for an opinion on a 20 minute video or a 2000 word article, let them know what your specific question is, or what about the content you found either particularly compelling, surprising, or questionable. If you are only looking for a ‘yes this is trustworthy’ or ‘no this isn’t trustworthy’ and are willing to take their word for it without a long explanation, let them know that as well.
6. Repent (or at least, redact).
I hesitate to make this last point because there is no way to express this without sounding somewhat judgmental. I hope it is clear that I intend to hold myself to this same standard as well, and hope that when (not if) I also fall into the ‘fake news’ trap and share misleading or unreliable information, I have the courage to follow my own advice.
What do you do when you have found information available on the internet and outside of your own area of expertise to be convincing and have passed it along, and through the (hopefully) kind input of friends have later discovered it to be untrue? I think there are a few good options. The simplest is to take it down; to delete the post so that others will not either follow you into believing the false information, or else in disbelieving it themselves begin to associate you with it. I think this is the minimum standard we should expect regarding our interactions with falsehood. However, I think an even better idea is what I have seen a family member do consistently in recent years; whenever she has shared a fake article or untrue information, she has then edited her post to clarify that the information is not reliable and why. Rather than distancing herself from those mistakes she embraces them, and in doing so helps protect others against the same errors. I believe that even better than Christians being known for never spreading false information (which is surely not the case now) would be us being known for the integrity and humility to publicly repent of error and embrace truth; in fact I can think of no more Christian way to deal with such a situation.
There is one thing we cannot do. Once we are aware of the falsehoods in something we have shared or promoted, we cannot choose to cling to it because we like the way it sounds or want people to believe that it is true. I have seen this done far too often; when it has been shown clearly that a source is unreliable or has even told outright lies, I have seen friends choose to continue to endorse and share it. There are myriad reasons, from liking a few of the points that weren’t exactly dishonest to wanting people to accept the overall message even if the content isn’t reliable. As people who believe that truth is authored by our Father and that we have an enemy who is only the father of lies, we cannot be comfortable with the mingling of the two. We cannot say, “yes, 7 of his 12 points were deliberately dishonest, and maybe or 3 or 4 were fairly dangers, but I really liked the other 5 and he’s just such an engaging speaker.” We must hold to higher standards of veracity than this. If we really want to promote those other ideas we should be incredibly, unmistakably clear that the rest of the content is not trustworthy… But better still, we should do the difficult work of finding a more consistently reliable source, and say of the first only that “he is a liar and the truth is not in him.”
I will conclude with the words of our Lord from Matthew 10:16: “Behold, I send you out as sheep in the midst of wolves. Therefore be wise as serpents and harmless as doves.” This pandemic is unlike anything we have seen in our lifetimes, and it is already the number one cause of death in the United States. We are living in an era of human history when reliable, true information is really capable of saving lives and when false information endangers our friends, loved ones, and neighbors. As we seek to obey the command of our Savior, let us reflect that we may never again in our lifetimes see such a moment as this, when these two concepts are so closely linked and refusal to be as wise as serpents can lead so directly to a failure to be as harmless as doves.
My name is TJ Webb, and I do NOT endorse this message.
As might be expected, there are a great many videos and articles about health surfacing right now during the pandemic; it’s a topic that is firmly on all our minds, even more so than usual. Unfortunately this means there is a lot of misinformation out there. I am actually really grateful when friends and family ask for my input on health information; I think informing our communities and using our education and experience to aid in the challenging work of discernment in this area is really important work, and one of the roles we need to engage in as Physicians. That said, there is so much misinformation out there right now, and life is already so busy because of the work of fighting the virus itself, that I have pretty much given up on addressing each article or video point by point in the way I normally would. I tend to be excessively verbose so you could imagine that cutting back is a challenge for me!
First, I would say that a good place to start, really with any of these articles or videos, is to ask whether the source is a reliable source of truth, a frequent source of falsehood and misinformation, or something in between. I don’t mean that we could write someone off because they have been mistaken (even brazenly mistaken) in the past, but simply that it is helpful to know their track record of veracity as a starting place for any new claims. It is important to know if the source has, as Chesterton put it, “revealed itself as a truth-telling thing.”
With that in mind I would encourage you to do some research on Dr. Pompa as a backdrop for understanding his perspective. He is not a medical doctor or a scientist. He has a degree as a Chiropractor. A discussion of alternative medicine in general is outside of the scope of this discussion, but I will say Chiropractory is a widely varied field in terms of adherence to scientific evidence and even basic medical ethics. I have known very good chiropractors who genuinely wanted to help with people’s pain and believed their methodology was superior to (or more often, worked in combination with) traditional approaches such as physical therapy, exercise, etc. My parents see a Chiropractor to this day and he came to all of our new year’s gatherings growing up; I like him very much as a person, and I’d like to think they are mostly like that. There are also, unfortunately, some Chiropractors who have discouraged patients from following the advice of their Physicians and receiving necessary treatments, and convinced them instead that a realignment of their spine can cure everything from diabetes to cancer. I have known some to sell unbelievably expensive and entirely unproven supplements from their offices and branch into other facets of alternative medicine even more dubious. Sorry to digress; all of that is to say, we don’t know what kind of Chiropractor he was, but when he speaks on virology, immunology, and microbiology, we need to understand that he is by no means speaking as an expert, or as someone who has actually trained in those areas of study extensively (though I’ll be the first to admit that I don’t actually know how much microbiology and immunology is taught in Chiropractor school; if a Chiropractor reads this and disagrees with my assessment, please feel free to lend your insight!).
Further, I think it bears pointing out that he is no longer practicing Chiropractory. As best I can tell, his license with the Pennsylvania board of Chiropractors has been on probation since 2014. To be fair, this was due to “moral turpitude” over a civil issue (which you could google if you wish, but I won’t share the details of the case here) and not due to issues related to his practice (this is of course assuming I have the correct Dr. Daniel Pompa, Chiropractor. I am ready to retract this information if someone is better at google than me and it turns out to be a different guy!). He currently works as a “cellular healing” and detox consultant and, as far as I can tell, all around alternative health huckster. His website and blog are absolutely full of dubious claims (though I’ve seen worse) and, of course, are oriented around a (presumably) expensive and unproven service that he can provide. Only Dr. Pompa has the key to unlocking your cellular health!
So, what’s the most we can say about Dr. Pompa so far? We know he trained in a fairly mainstream, regulated alternative medicine field, but is no longer able to practice in that field for legal reasons unrelated to chiropractory itself. We know that he now works in an entirely unregulated field of holistic healing/alternative medicine and puts himself forward as a “cellular healing and detox” specialist, which are not real areas of medicine. We also know that he is a very gifted communicator. He is handsome and well spoken, he dresses well and is likable on video, and most importantly he uses the combination of “common sense” arguments and pseudo-science vocabulary that is what makes alternative medicine seem especially convincing; the terminology all seems like the right type of terminology, but there is nothing here that you could say ‘well that doesn’t make sense’ to (in contrast to what C.S. Lewis says about things that are actually real; “the problem is not simple and the answer is not going to be simple either”).
So, with all of my initial apologies about brevity, I find myself out of time and having not even addressed the video itself. To be fair, I didn’t know that there would be so many cautions to share about Dr. Pompa when I first started to research his career. Honestly, that ought to be enough; he is someone who has made a career out of selling unproven treatments based on empty scientific-sounding vocabulary and personal presence alone, once ‘mainstream alternative medicine’ would no longer allow him to practice, and his video above is convincing, where it is convincing, primarily because of these two factors. But I do believe that it is worth addressing the content of the video itself, and if you’ll give me leave I will attempt to do so in a few hours after my children are in bed!
I’ve watched the video a couple of times and taken down a few quotes, but I’d like to start with a short preamble: It’s really not all that bad. Please understand, I’m not saying it’s true; if I were a fact checker I would have no choice but to categorize it as “fake.” But my standard for misinformation has probably shifted a little during this pandemic, and this video is pretty benign overall. Like so much of the alternative health industry, it is an uneven and patchy mingling of truth and falsehood, so you couldn’t say “everything he said is dead wrong.” This is one of the problems with this industry; people who are in it REALLY believe in it, much of the time, and often have a few scientific facts or principles down but without any supporting context or science education, so they easily believe entire narratives that are built up around those few isolated truths.
I’m also not quite sure why he’s making the video. I suppose that in his line of work fame and notoriety do lead directly to financial success, and we are seeing a lot of people in alternative healthcare trying to use the pandemic to make a name for themselves and be seen as an expert. There’s certainly plenty of evidence of that in the video, from him saying ‘bottom line the experts have missed it’ to ‘this study confirms my point’ and lots of other subtleties of language intended to convey that he is the true expert on health and the poor guys at the CDC and WHO just don’t know any better. So, maybe that’s part of it; that is certainly the name of the game in that industry. But I’d like to overall give him the benefit of the doubt and say he really believes his message and wants to get the information out there; maybe I’ve been duped because he’s just so darn handsome so I’d like to believe him.
The problem is that it just isn’t reliable information. There are a few extremely egregious falsehoods, and we might as we’ll get them out of the way now.
“They’re looking at the death rates just sinking around the virus, saying ok it’s probably more like 0.1% at best, which is basically the same as the regular flu.” “The bottom line is the experts have missed it.”
-I have no idea where he got this information from. Maybe he heard it somewhere but misinterpreted it? The ‘no more dangerous than the flu’ line seemed to have quieted down for a while as the pandemic spread, but has resurfaced as social distancing and containment measures have proven effective; it’s a very easy thing to say when you don’t have family and friends who are in the ICU or have died from the virus, and in many places there are so few severe cases that it’s easy to believe that COVID-19 “wasn’t actually that big of a deal”, as though the pandemic 1. Hadn’t already killed over a hundred thousand people, and 2. Was already over and done with. This is something public health experts and lay people alike have been saying since the beginning; if the extreme measures we take now actually work, people will say they weren’t necessary. In places where the healthcare system is particularly overwhelmed, the case fatality rate remains above 5%; astronomically higher than seasonal influenza. In places where the healthcare system can cope with patients at a more routine pace, without running short of either Physicians, Nurses, other support staff, or equipment, the rate is much lower; but still on the order of 2%, not 0.1%. This is an incredibly deadly disease, and before anyone buys into the conspiracy that this was all hype pushed on us for this purpose or that, they should open themselves up to the images and stories coming from Washington, New York, Louisiana, Italy, and Spain. I am sure we will soon enough be told that those people were all “trauma actors.”
The biggest question mark in all of this, of course, is the lack of universal testing. Our testing policies so far have been driven by test scarcity, and there has ALWAYS been the assumption that as more testing on asymptomatic or minimally symptomatic patients occurred we would find a large cohort of people who were more or less healthy despite having the virus. But we are still very, very early into having this sort of testing anywhere, and from colleagues in healthcare system that DO have universal testing policies I am hearing that they just aren’t seeing many asymptomatic carriers. So although we will not be able to come to a final estimate of the death rate from this virus until all is said and done, so far it is too early to see the drop in the death rate due to asymptomatic cases that we all have expected.
“But because they are attributing many different conditions to Corona it’s probably even half that.”
-It’s hard to know what he means, but I believe he is referencing the conspiracy theory that someone is either inadvertently or intentionally inflating the death rate for COVID-19 by attributing deaths due to other conditions to the virus. I’ve addressed this in detail a few days ago on another Facebook post; I am happy to share it with you if you would like.
“Now we know it was a narrow group of people that were truly at risk for this virus.” “You can tell from my past videos that I am not one to have been fearing the virus.” “People are realizing that it’s not as dangerous as we thought and they want to get the antibodies…. Because if this mutates we could all be at risk.”
-This is a bit revisionist. He is making it sound as though we initially thought that every person had a big risk of ending up hospitalized or dying from COVID-19 and now we know it is only people with certain risk factors such as age, other medical conditions, immunocompromise, etc. This is actually the exact opposite of the true history of our understanding of COVID-19, and it was shocking when reports of death in young healthy people began to come out of Europe and then began to occur in the United States as well. Of course older people with medical problems are at higher risk; that is true for any infectious disease. But this is a virus that is, in fact, dangerous even for people who are young and healthy. We are ALREADY all at risk.
As far as the second quote goes, please do not be fooled; this disease is dangerous enough that TRYING to get the antibodies “naturally”, by intentionally being exposed to the virus, would be incredibly foolish and irresponsible. Vaccines were invented because some diseases are so dangerous that taking a chance on the live, unattenuated pathogen is the same as gambling with your life.
“They put things into place not understanding the risks…”
-I’ve included this because, briefly, I think it illustrates this concept of setting oneself up as an expert that is so common in these videos. The idea here is to convey that the people in charge, the epidemiology experts and virologists and the people who have actually spent years and years studying human disease and microbiology and human immunology, all meant well but just didn’t know or understand what he does. He goes on, as we’ll talk about below, to discuss the hygiene hypotheses of autoimmune disease and the ‘dangers’ of wearing masks, and if you connect the threads it really seems as though the physicians and researchers who have recommend ways to slow the spread of the disease just aren’t familiar with the principles he is referencing, which is of course preposterous. Please note, however, that he is releasing this video NOW instead of 2 or 3 weeks ago; now that the “things they put in place” have actually shown some measure of success, he has the luxury to say that none of it was necessary.
The Hygiene Theory
After this, we finally get into the real meat of his argument. He starts by quoting a study, “having fewer sanitary amenities in childhood is linked to a lower risk of having inflammatory bowel disease.” This is a basic concept of the hygiene hypothesis, that exposure to certain microbes is necessary and decreased exposure leads to multiple disease, including autoimmune disease. This is a valid scientific theory with a good bit of evidence. Like most things in medicine (or for that matter, most things in real life period), it is much more complicated than it is presented here. It would be dangerous, for instance, to presume that because some bacteria, viruses, and fungi are important to our growth, development, digestion, and the functioning of our immune systems, that therefore ALL such microbes are healthy and beneficial and we were wrong to want to protect ourselves from them. Concluding that because exposure to more microbes is linked to decrease in risk of inflammatory bowel disease, we should expose ourselves to ALL bacteria and viruses including the one that causes COVID-19, would be particularly illustrative of the clinging to a few points of medical data without actually understanding them that we talked about before, which is so emblematic of this industry.
“The whole point of all of these studies is that more the viruses, bacteria, and pathogens you are exposed to the healthier your immune system is.”
-I cheated there, because I knew he was going to say that already as I was writing that last paragraph. What he’s done is taken one category of disease and one set of risk factors for those diseases, and conflated them with all of human health in general because the words happen to be the same. Because disease, bacteria, and microbe all appear in both discussions of the hygiene hypothesis of autoimmune disease and in concepts related to infectious disease, he believes that data from one can be used to negate data from the other. It is a basic failure to understand the concepts and even the terminology that is being discussed. To put it more simply; he is stating that because some bacteria are good for us, bacteria can’t be bad for us. He probably doesn’t really believe that, but the implication is that if your immune system is healthy enough then everything that would make others sick will just make you stronger.
The failure here is to distinguish between viruses, bacteria, and fungi in general, and pathogens, which are viruses, bacteria, and fungi (and other fun little guys) that cause diseases in humans. Avoiding pathogens that can make you sick is the most basic way of avoiding dying from some of the most painful and devastating killers in our fallen world. It’s the reason we don’t eat raw pork and why we wash off a cut. It’s a very basic concept that is taught even in high school biology, and it isn’t confusing to anyone in the medical field. It isn’t really confusing to anyone at all, until the obfuscation occurs in videos like this. The alternative health industry, and particularly those sectors of it that are focused on ‘restoring natural immunity’ and establishing healthy gut flora, etc, need to convince you that they are the only ones that really understand these concepts, so they obscure simple ideas, minimize complicated ones, and conflate terminology until they have a version of our complex immune systems and interactions with the world around us that is almost, but not entirely, completely untrue. They would like you to believe that everyone else is confused; that doctors think all bacteria are bad and want to sterilize your microbiome and gut flora with antibiotics and hand sanitizer, and can’t distinguish between the presence or absence of an infectious disease. There was even a video recently where an alternative health partisan claimed that doctors don’t study the immune system in medical school at all, which is obvious nonsense. And in trying to convincing you, they do convince themselves.
“Before this we had the hygiene theory: run from bacteria, kill all the bacteria” “Let’s not throw a whole decade of research out the window”
-Again, just to be clear, the hygiene hypothesis IS the theory that decreased exposure to microbes increases the risk of certain diseases. And the theory and research around it has been around for decades. I find it concerning that he keeps exactly inverting the concept of the one scientifically valid theory upon which he has built his entire pseudo-medical philosophy, and then calls it a failed theory that we have to abandon. In his defense, it is a misnomer, since avoiding non-pathogenic microbes has nothing to do with hygiene.
“If I was going into a group of people that was at risk I would wear a mask….” “It wasn’t about killing bacteria and viruses and pathogens, it was about living with them.”
-You might notice, as you watch the video, that he frequently shifts between treating the virus as something to take seriously and something we should live alongside and go ahead and ‘get antibodies’ to as early as possible. We haven’t really beaten this thing yet, so I don’t think that the people making these ‘it isn’t so bad’ videos can be quite so brazen in saying that the virus isn’t dangerous, no matter how much data their audiences are generally willing to ignore… at least, not yet. He is willing to tell you that you should keep your grandmother or immunocompromised friend safe by wearing a mask around them, but at other times in the video he encourages you to touch your face and implies that we need to take this opportunity to get exposed before the virus mutates. In 2-3 months we will see many articles and videos of people telling us that we missed our chance to have “COVID-19 parties” and that this is because big pharma and their pawns, doctors and nurses, want to suppress our natural immunity so they can sell vaccines. But those videos will have to wait until people stop dying from this virus. SARS-CoV-2, at least for the time being, still has to be respected as a pathogen.
“The hygiene philosophy failed. The antibiotic era, hand sanitizers, all of it has FAILED.”
-Let’s be clear; hygiene measures associated with germ theory have saved more human lives than any other intervention in medical history (vaccines and antibiotics are also in the top 5). It is ludicrous to say that hygiene doesn’t save lives. There are places in the world and in the United States where we STILL see the devastating effects and widespread disease and death associated with lack of access to clean water and basic hygiene measures. This is a privileged belief from every standpoint; chronologically, geographically, socio-economically. Living in a hygienic environment with potable water and clean, nutritious food, he has the gall to say that hygiene is a failed concept. He would like us to use the word ‘hygiene’ as a synonym for his red herring of ‘sterile’ and believe that doctors and public health experts want us to never be exposed to the world around us, which is patently false. He then wants to conflate the hundreds of years of excellent hygiene and microbiology work that has been done, which has saved billions of lives, with his own narrative that if they had their way doctors would have us all living in white rooms wearing gloves and afraid to let our kids play in dirt. Why? Because thoroughly undermining generally altruistic physicians and nurses that practice actual evidence-based medicine is very good for the alternative health business.
“The true risk of what we’re calling the new normal.” “People with masks and gloves”
-Please wear masks. Please treat the virus like it can cause terrible respiratory failure and kill you, because it definitely can. Nobody is recommending you lysol your house daily (but please do it to the kitchen counter if you are cutting raw chicken, because Salmonella is a bacteria that IS a pathogen and can also make you sick). Your kids can play in the mud; they can do it today, if you’ve got some mud in your back yard and nobody has been over to cough on that mud. Wearing masks every day of our lives, not hugging each other, avoiding social gatherings, avoiding dirt and trees, and cleaning everything we touch are not practices that have ever been espoused by Physicians or public health experts. Taking precautions as individuals when we are ill, and as a society right now because a particular, new, deadly virus is currently spreading in our communities and threatening to overwhelm our ability to care for those affected, is something we espouse; and I believe that, regardless of what some people might want us to believe, most of us have the common sense to see the difference.
I had hoped at some point this week to write a rebuttal to the incredibly deceitful and frankly quite silly “Dr. SHIVA Ayyadurai, MIT PhD Crushes…” youtube video that has been shared so widely by my facebook friends. I still hope I get the chance, but it’s about 16 minutes long and each minute has about 2-3 nonsensical statements, outrageous falsehoods, or outright lies. In the meantime here is a good start from a fact checking website: