As the pandemic has escalated over the past several months and almost all of us who had been previously unaffected have now had friends, family members, or other people we care deeply about either pass away or at least become very, very ill from the virus, I’ve noticed a trend in the misinformation that we accept, share, and believe. The nature of a global pandemic is that it robs us of our delusions, and we are now many months out from being able to believe what was commonly said in March and April, that the pandemic is not coming, and that even if it does come it is not deadly. The landscape has shifted, and until more conspiracy theories crop up about vaccines or possible outpatient treatments in the coming weeks and months, the misinformation has settled back into the realm where it is most resilient; into the question of motives. It doesn’t matter what actually happens with medications, vaccines, case numbers, and death rates; believing that the people trying to help you are actually trying to control you is always fair game.
Hmm… Gandalf is pretty sus.
In about a week we are going to see the merger of COVID-19 misinformation and the ever-popular “War on Christmas” conspiracy which annually reminds us that dark forces are at work in the world to destroy my favorite holiday and everything it stands for. But until then, Thanksgiving is the target apparent of the powers that be.
Full disclosure, I’ve waged a small private war against Thanksgiving for years, and it has nothing to do with how many people are gathered. My concern is with the way we celebrate and especially teach children about the history of Thanksgiving and the way we sterilize the history of Native America-European settler relations. I also have some concerns, as the doctor to many patients with diabetes and CHF, about the lack of nuance in our culture’s understanding of feasting, and typically resolve this by telling my patients not to check their fasting blood sugar on Black Friday (unless they take correction dose sliding-scale insulin, of course). For me, it’s the most hypocritical holiday of all, because while I caution moderation to my patients I know I will probably fail to practice it myself. Because you see, despite all of my concerns about Thanksgiving as a holiday, I alsolove turkey and dressing, pumpkin pie, and most importantly (as any true Southerner will tell you) green bean casserole, macaroni and cheese, mashed potatoes and brown gravy (I’ll lose readers over that), and a sweet potato and marshmallow dessert we have hilariously convinced ourselves is a side dish instead of a hedonistic excess and probable harbinger of the end times.
(I also like seeing my family and stuff.)
So the togetherness and joy of the thanksgiving holiday is something I’m loath to give up for any reason, and I would be lying if I told you that I knew all along that we would opt for a small family Thanksgiving day in our own home, or that I immediately made that decision after reviewing the trends in COVID-19 numbers or even after reading Dr. Emily Smith’s excellent, excellent review of the relevant epidemiology facts. We earnestly struggled with it. And as we weighed the medical risks of our extended family members against my daily interaction to COVID-19 positive patients and my wife’s recent exposure to the virus, I could taste the potato casserole fading from my future as we made the difficult call and informed very disappointed (but understanding and supportive) family.
Fine, but when I say “Cancel Columbus Day” I definitely mean it.
And I’ve been counseling my patients to do likewise, just like many physicians, epidemiologists, and other health scientists around the country. And despite the suspicion and mistrust that a doctoral degree elicits these days, it has nothing to do with wanting to control my patients lives, training them for future subservience to the government, my crusade against the idea that our relationship with Native Americans was ever truly mutually respectful and supportive, or even the principle that misery loves company and if I don’t get to eat my grandma’s turkey dressing recipe on Thursday they shouldn’t either.
Instead, it’s because we are living today in the most dangerous window of the pandemic so far, and because there are characteristics of Holidays in general, and Thanksgiving in particular, that makes this week an incredibly dangerous one for our country.
3 Reasons that Thanksgiving is Dangerous.
1. Certain holidays are more dangerous than others. Even allowing for difference of culture and family tradition, the innate characteristics of certain holidays make them more or less dangerous in terms of transmission of a respiratory virus. January 2nd, World Introvert Day, will probably be just fine; but the indoor concert you are planning for National Kazoo Day three weeks later on January 28th should be cancelled because that is a lot of aerosolized spittle in an enclosed space (it should be cancelled anyway regardless of COVID-19, but that’s not my point).
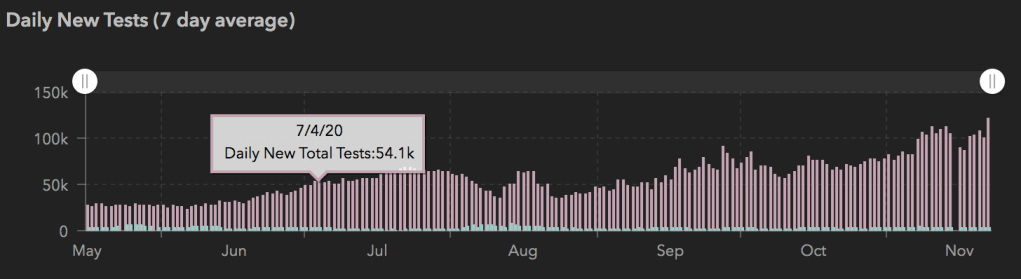
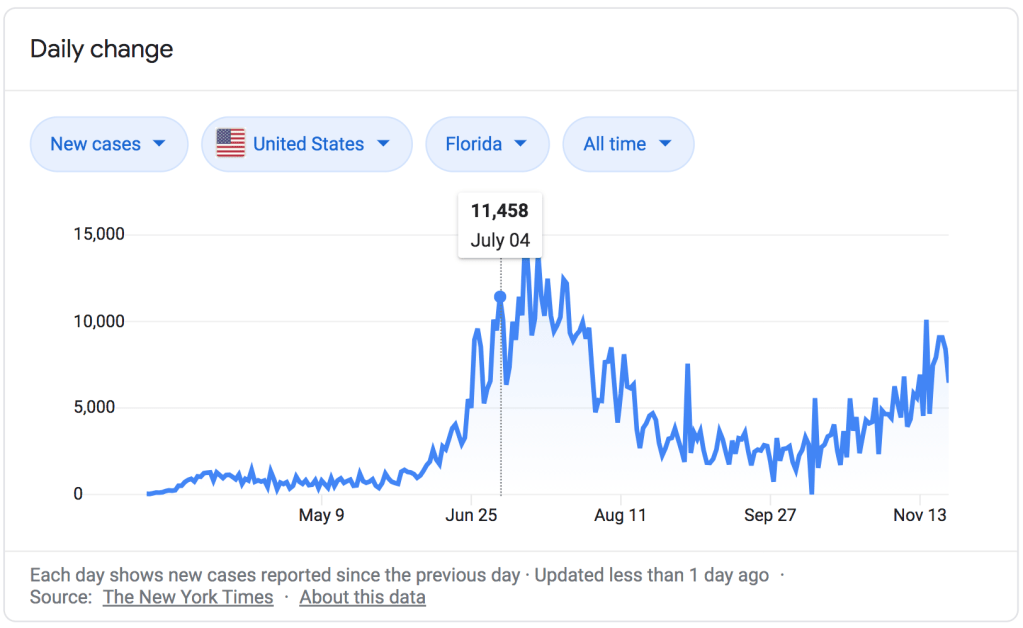
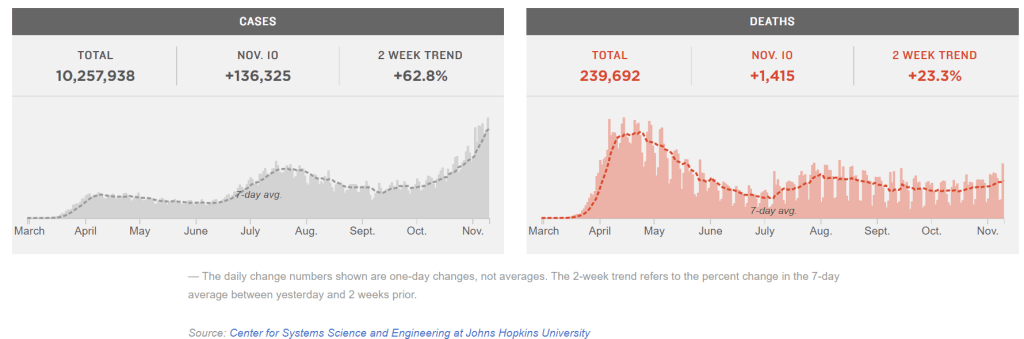
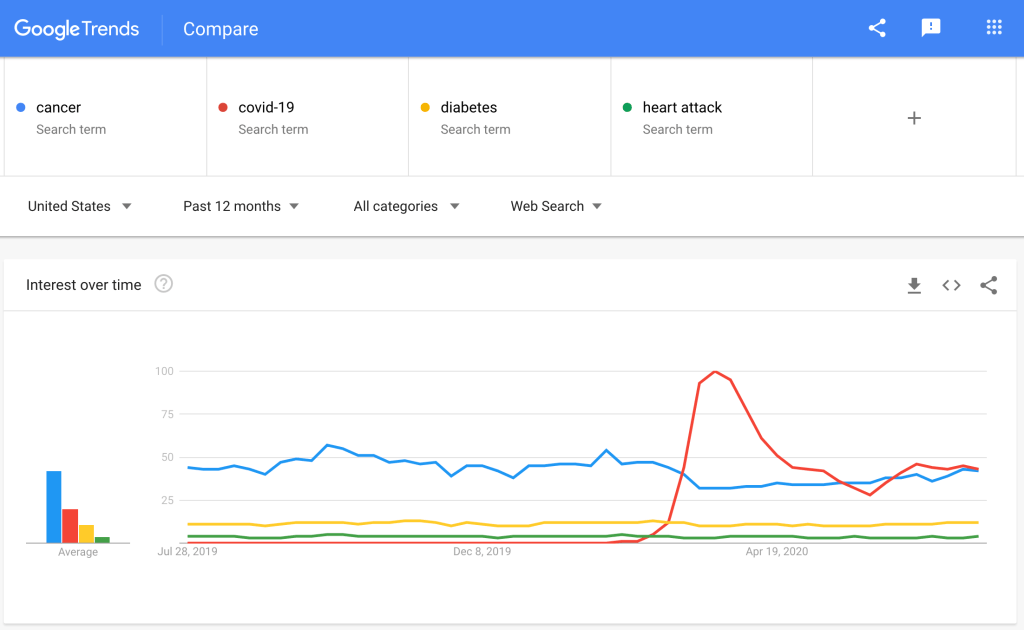
If we are going to discuss the characteristics of Thanksgiving, it would help to compare it to another widely celebrated holiday we’ve experienced during COVID-19, the 4th of July. As a reminder, here is a look at the numbers.
California
Texas
Florida
USA
The two weeks after the 4th of July saw the largest spike in cases of COVID-19 we’ve experienced during the entire pandemic (except for the one we are in now). There’s a strong enough case to be made that the trajectory of that wave was already increasing prior to the holiday; but the public gatherings, parties, and beach trips dramatically contributed to the rise in cases, heightened the severity of that late-July peak, and appreciably altered the curve for the worse in places like Florida and California. In a moment we’ll compare some of the characteristics of these holidays, but that’s really splitting hairs; the biggest reason that Thanksgiving is dangerous is because COVID-19 transmission follows the principles of exponential growth; the more cases you start with going into a time of decreased caution like a holiday, the greater the impact it will have on the curve. We are already close to or above capacity in many hospitals around the country; evenanother 4th of July, with the numbers we have right now, would absolutely drown us. And there’s plenty of reasons innate to the holiday that make Thanksgiving much, much worse.
It’s true that the 4th of July has some characteristics that could make it more likelyto result in spread of COVID-19 than Thanksgiving; mainly that it involved very large events that brought together people from very different spheres of contact. A few cases of COVID-19 could spread easily to multiple social circles and families from one big 4th of July party. But Thanksgiving has some characteristics that make it more dangerous too. First, unlike the 4th of July, most people celebrate Thanksgiving indoors; transmission is more likely indoors than outdoors, all things being equal. Second, contact tends to be prolonged; you aren’t just passing various people for a moment on the way to the beach or grabbing a beer, you are sitting face-to-face for hours while eating and visiting and (unless you are a good-for-nothing-in-the-kitchen family freeloader like me) cooking. If a contact at a 4th of July party has COVID-19, you may or may not have been exposed. If someone at Thanksgiving Dinner has COVID-19, everyone there is definitely an exposed close contact.
This is literally a picture of our Thanksgiving. Except for the 2nd one (I grew up Baptist).
Third, that issue of bringing people together from different spheres of contact is true for Thanksgiving just as much as for the 4th of July. Traveling for the holiday is one of the major things that public health experts are warning against, and even if you aren’t flying or driving across state lines, not everyone’s social circles really overlap much with their cousins’ or grandparents’. One family member who has had an exposure or hasn’t taken precautions in the weeks leading up to Thanksgiving runs the risk of infecting their entire family, and those family members bring their exposure back to the other members of their community. Finally, Thanksgiving brings people together who are not likely to socially distance from one another. It’s all well and good to say ‘we will eat outside and stay 6 feet apart’, but how many times has that actually happened when getting together with family you have been longing to see? There will be hugs, there will be boardgames, there will be long heartfelt conversations- or yelling matches about politics. Not to mention the decision of whether or not to finish off somebody else’s half eaten piece of pumpkin pie if nobody is looking, which is a difficult enough choice even under normal circumstances.
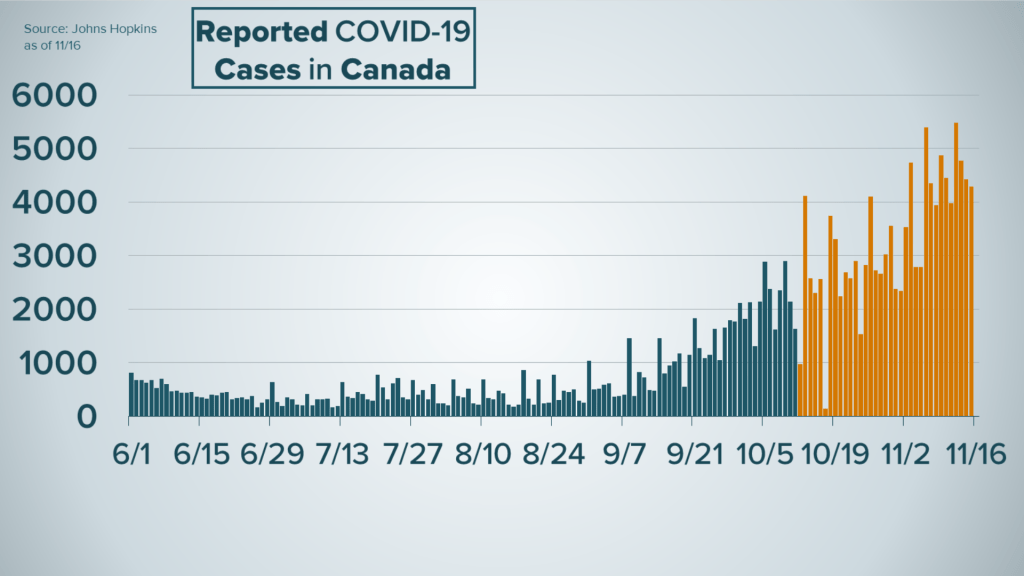
But we don’t have to just take my word for it or guess whether Thanksgiving will be as bad (or worse) as the 4th of July, because Canada has a Thanksgiving too, which they hold (ridiculously) on October 8th.
The Canadian numbers show a miniature warning of exactly what we would expect after a national holiday during a national uptick in cases; a steepening of the curve and a much larger number of new cases over the next month. The difference is that Canada has nowhere near the number of active cases or the amount of community transmission that we have; our increase is going to be much, much more dramatic.
2. Holidays bring together those who are at greatest risk with those who spread the virus best. We talked about the total lack of social distancing between relatives when they finally get together, and nobody is better at not socially distancing than children. If you think about the emotional value we all place on the holidays, probably one of the first images that comes to mind is the sight of your children running to their grandparents and covering them in hugs and kisses. It’s honestly one of my favorite moments each and every time it happens. It’s also a very, very dangerous situation if there’s any possibility those children have COVID-19. Children spread COVID-19 very easily; some studies have shown that children spread it even longer and more efficiently than even the sickest ICU patients. They spread it even when asymptomatic, and are asymptomatic at a higher rate than adults. They are also in school, and schools are full of other small gross people that spread COVID-19 efficiently, and those schools will not be closed for the holidays for any significant period of time prior to Thanksgiving.
And who are they hugging on? Almost certainly the people in your family who are at the highest risk if they do get exposed. We have been discussing the risk factors for severe COVID-19 infection, COVID-19 pneumonia and respiratory distress syndrome, and death on this blog since April and a lot of those factors haven’t changed; age, chronic lung disease, diabetes, heart disease, other chronic medical problems. But age is the first one, and the risk of someone dying from COVID-19 increases dramatically after age 50.
By bringing together the people in your family most likely to have been exposed to COVID-19 over the past few weeks (because of school) and most likely to spread it even when asymptomatic, and the people most likely to get seriously ill if they are indeed exposed to COVID-19, holiday gatherings with extended family really do present a dangerous situation for the most vulnerable members of our families.
I’ve had patients ask my advice on what to do about visiting grandparents and great-grandparents for Thanksgiving over the past few weeks. I hear their anguish, their indecision, their desire to celebrate with family fighting against their fear of spreading the virus to someone they love, and the deeper fear and guilt that they are making the wrong decision by choosing to miss out on those beautiful moments together. My recommendation? If you think that, barring some tragedy, the person you love has some good years of holiday celebrations left, it seems wise to sacrifice thisone in order to safeguard all of the others. This pandemic won’t last forever.
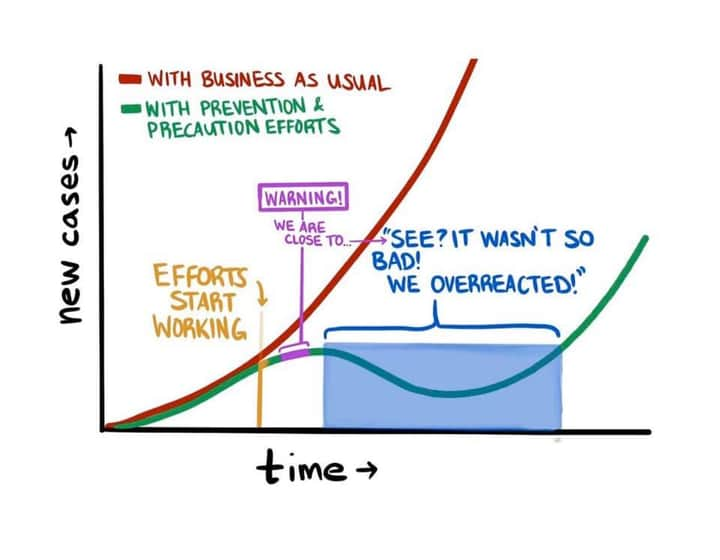
3. It isn’t just COVID. I’ve been reflecting on my very first efforts at writing about COVID-19 back in March, before I even started this blog. At that time the US had 23,604 deaths from COVID-19 and healthcare workers and public health experts were urging caution, which people were generally willing to follow… for a little while. Today it is 260,000 and instead of seeing this as validation of the concern we have had since March about how bad this virus can be, many people havelong since thrown caution to the wind for really no other reason than that we are all incredibly, unbelievably fatigued. I’ll write about that sometime soon; but what I’ve really been thinking about from those first posts is these two short paragraphs, which are just as true today as they were then.
Guess what? We are there.
As I’ve said before, most people don’t understand what an overwhelmed healthcare system looks like because we’ve never experienced it. It means not having access to doctors and nurses when you are in DKA or have a skull fracture. It means your kid can’t get treatment for his seizures or his infected spider bite. It means that every single medical condition is more dangerous (many are more dangerous during the holidays anyway) because medical professionals don’t have the time, the mental energy, the tools and equipment, or even the staffing to deal with them properly. It means not being able to get an ambulance to get you to the hospital or a bed when you get there. At a time when tent hospitals are being put up around the country, we need to decrease COVID-19 transmission right now to prevent permanent injury and death from everything from high-risk pregnancy to Congestive Heart Failure to snow-skiing accidents.
And of course, as we saw in New York, an overwhelmed healthcare system makes the virus itself incredibly more dangerous as well. “I can always go to the hospital if I have a bad case” has never been a good argument against exercising caution; but it is simply not true if you can’t go to the hospital or if they can’t take care of you well once you get there. The death rate has held more or less steady since it started to decline because of our increased understanding of how to fight the virus with targeted, COVID-19 specific ventilator techniques and successful use of medicines like dexamethasone for hospitalized patients. But the biggest factor that will cause it to go up again is doctors who are too tired to think and nurses who are too busy and fatigued to catch their mistakes.
But how can I celebrate Thanksgiving with family safely?
I never want to be accused of being an alarmist, and if we are talking about reliable epidemiology principles and the solid medical realities of how the virus is transmitted, I would say of course there are safe ways to do Thanksgiving together. In theory. We could talk about things like only meeting outside, everyone distancing from people not in their immediate family, no sick people at all being allowed, and everyone strictly quarantining for a full 14 days prior to the Holiday. The problem is, those are things that are hard for anyone to do, let-alone a large group of people, and the chances that every member of your family can or will strictly adhere to those guidelines is very low; and it gets lower with every person you add. If people are working anywhere other than home, or they are traveling at all prior to the holiday, or if you’ve got just one family member that believes the pandemic is a government sponsored hoax meant to force you to wear a mask and will therefore gleefully shirk every precaution the family has agreed upon when the time comes, your gathering has gone from perfectly safe to not perfectly safe; and not perfectly safe is, in aggregate, really really dangerous right now.
Whoever made this meme and then watched it go viral: “Yeah, take that Casey! Hahahaha, hahahaha!”
Or let me put it another way. I’ve seen more patients with COVID-19 than any doctor in my clinic system; maybe more than any doctor in town, though there are those whose exposure risk I would rate as being higher than mine (our pulmonologists and ICU docs, for example, or the young medical residents who are seeing patients with COVID-19 in both the outpatient and inpatient setting and the ICU… and of course our nurses, who typically have more time face-to-face with our patients in the hospital, and in clinic perform procedures like nasopharyngeal swabs that are higher risk for aerosolizing respiratory droplets). I’ve been tested for COVID-19 12 times; half because of symptoms and half because of our internal exposure protocols. I’ve been negative 12 times; my 13th test is tomorrow (and if it’s positive I’m coming back to delete this paragraph). I would never disparage the degree of caution that has been taken by my medical brothers and sisters who have contracted COVID-19 in the line of duty, or imply that I’ve done anything they haven’t; but I’ve been seeing COVID-19 positive patients almost daily since April and have utterly failed to contract the virus. My PPE game is strong. I’m really, really good at being cognizant of fomites and at personal transmission control. I’m confident that if I can design and implement clinic protocols that protect patients and staff 40 hours a week, I could do the same for a 3 hour meal… But I’m staying home for Thanksgiving.
Why? Because it isn’t worth the risk. Because the virus is very, very real and I really care about my relatives and neighbors. I’m not afraid of COVID-19, and I’m not letting it control my life. I’ve heard all of that hyperbolic nonsense and rejected it; prudent action on behalf of those you love is not “living in fear,” and giving up one meal with extended family for one year is not letting it “control your life.” I’ve also heard the rejoinder, “but where do we draw the line?” Somewhere else, obviously. And even though I’ll probably be back here in three weeks encouraging you to have a small family Christmas this year, if you want the best possible chance at a safe Christmas with extended family (after strictly quarantining for 2 weeks and carefully laying out ground rules for everyone attending, and not flying to get there…), the best thing we can do is take wise, collective action to stem the tide now. Turkey and dressing will taste just as good in May or June.
Pretty heavy-handed, I know… But it feels like we are at that point of the pandemic.
After weeks of COVID-19 misinformation being a secondary or minor issue- to me because we have been so busy actually diagnosing and treating the virus, and to the country in general because election misinformation was much more interesting- I suddenly find myself with more pieces of misinformation to write about than I could possibly make time for. There is this meme that probably needs some attention as people who haven’t complied with mitigation measures since March threaten non-compliance with any future mitigation measures because the mitigation measures they already didn’t comply with didn’t work(because they didn’t comply with them). If I get time I’d love to explore that a little further (and, I should hope, a bit more graciously than I did in that last snarky sentence).
This reminds me of the great Chesterton quote; “Christianity has not been tried and found wanting. It has been found difficult; and left untried.” Could we say the same thing about self-quarantine, shelter in place measures, and especially lockdown efforts? And what then shall we say about wearing masks? “It has been found slightly inconvenient and inexplicably controversial, and tried only begrudgingly and inconsistently?”
There’s also a discussion that we need to have, as a nation, about how this pandemic didn’t go away on November 4th and isn’t going to go away when we have a new president in the White House. This virus is pitilessly apolitical. It doesn’t care about Republicans and Democrats, the electoral college, lawsuits in Pennsylvania, or any of the other big problems facing our democracy (did I just include Republicans and Democrats in the list of problems facing our country? Yes, yes I did). In an election year, and particularly one this contentious, there was never any chance that information and understanding about the pandemic would fail to fall out along party lines. Now that the election is over, is it possible for us to drop our politicized misinformation and as a countrymen find some common ground on which to fight this deadly virus together? Probably not. But it doesn’t mean I can’t rant about it for five or six thousand words.
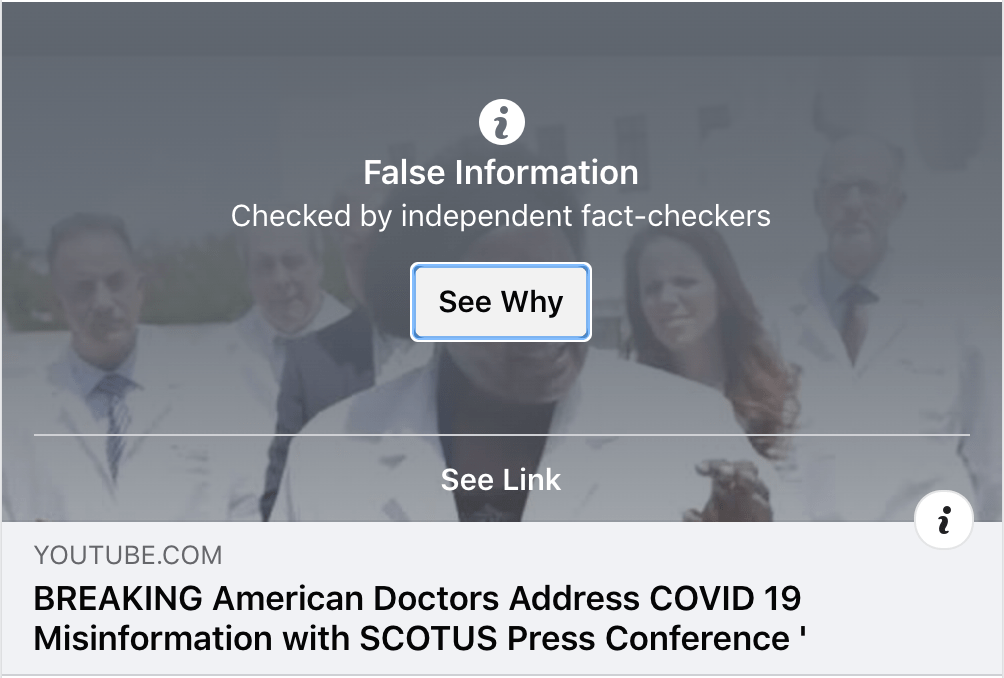
But I think the most pressing is the video I’ll share a little way below, which was sent to me by a Facebook friend. It’s a short misinformation video about the COVID-19 vaccines that are being developed and, like most misinformation, is an amalgam of half-truths, deliberate misrepresentations, and outright lies. It’s very short and I’ve posted it here in it’s entirety with the hope that you will read the accompanying discussion and not just watch the video.
Will I get the COVID-19 Vaccine?
Let me start with a statement that might be a bit controversial; while I’m obviously strongly leaning that way, and hope I have the decision put before me as soon as possible, I haven’t absolutely decided whether or not I will get the COVID-19 vaccine once it is available. That might sound like heresy coming from a doctor, particularly when we are currently in midst of the worst wave of the deadliest pandemic of our lifetimes.
But let me explain what I mean. While it’s encouraging to hear that the new vaccine from Pfizer is 95% effective against this very, very deadly virus, and while a safe and effective and widely accepted vaccine is the best and quickest route we have to beating the COVID-19 pandemic without even more massive loss of life, I remain at heart and by training a scientist, not a science fan; I default to skepticism of any new discoveries or developments until I have reviewed the evidence for myself. With regards to the COVID-19 vaccines that have been in development over the past year, I am like most physicians cautiously optimistic. Before deciding to have the vaccine administered to myself and my four children, however, I plan to review all the data that I can in order to ensure my choice is as informed and sound as possible, just like I would for any medication, surgery, or any other intervention my doctor recommends (or, for that matter, any treatment or medication that I recommend to my patients).
“But Dr. Webb, this is exactly what anti-vax parents are doing when they refuse vaccines.”
Yeah, except that it isn’t. At least, not generally. You see, when I say I plan to review the data I mean the actual data from the clinical trials and independent studies, not misinformation and propaganda. If you are like me and have the privilege of scientific training that allows you to independently parse the information contained in published clinical trials, you probably have no desire whatsoever to outsource this type of academic work to people who do not have that training and who are approaching the information with blatant and unabashed bias. But if you do not have the background to do that work yourself, you still deserve the same degree of reassurance and comfort before choosing to accept a vaccine or have it given to your children; it is just less likely that you have access to the resources you need. The anti-vaccine movement knows this and it is in this gap- the gap between the confidence you need for such an important decision and the degree of explanation, information, and reassurance that you are generally given– that they do their best (or most effective) work.
Who is to blame? Well, obviously, I am. Your local doctor, your pediatrician, your PCP; we carry the burden not of fighting propaganda, the blame for which rightly rests on those creating and spreading it, but of helping you become resilient against propaganda and misinformation through patient-centered health education.
So I am begging you, if you are at all wary of or uncertain about a COVID-19 vaccine, and if you do not have the technical background or family/community resources you need to review the source data independently, ask your primary care doctor. Maybe even give them a heads up when you schedule an appointment so they can look into it beforehand (they probably already will have). If they are active on social media, ask them if they would be willing to write about it and share it openly. Some primary care physicians, like Dr. Ben Brashear here in Texas, believe so strongly in this type of work that they have devoted a large amount of their time and energy to helping their patients and other readers navigate these issues through their clinic websites and social media pages. I think this is the single most effective way to combat Social Media Misinformation; with a hundred or a thousand or ten thousand doctors and scientists in small towns like mine or Dr. Brashear’s helping patients whom they have already built a trusting doctor-patient relationship with navigate what information is reliable and what isn’t.
And of course, on the off-chance that over the past 6 months of my writing these blog posts you have somehow decided you actually trust me, I’ll plan to write a short post about my decision on the vaccine as soon as I’ve decided, for certain, what to do for myself and my family.
I should also point out, while we are dispensing with preliminaries, that this post is not designed to be an overview of the research and development of the various COVID-19 vaccines. For that I will point you to my hero, Baylor Friendly Neighbor Epidemiologist Dr. Emily Smith.
“The ChAd Vaccine” Video Minute-By-Minute Discussion
0:12 Share this everywhere!
I’ve been doing this sort of misinformation debunking work as a hobby for about 8 months now and I’ve come to recognize some of the language or verbiage that ought to make us extremely suspicious that the information we are about to be given is not necessarily reliable. The speaker hits several right out of the gate:
“This is a fact.”
In my experience, things that are facts don’t need the disclaimer “this is a fact.” Both for people spreading misinformation and those of us fighting it, the goal has to be to lay out such a clear and compelling case for the facts that the rhetorical sledgehammer of “I’m telling you the truth, I wouldn’t lie to you” is as unnecessary as it is hollow. If someone finds this verbiage convincing, it is likely because they are anxious to be convinced; and it should put you on your guard. “Let your ‘Yes’ be ‘Yes,’ and your ‘No,’ ‘No.’ For whatever is more than these is from the evil one.” -Matthew 5:37
“Share this everywhere.”
Similar to the last point, I believe that most people giving reliable, expert advice or guidance will never ask you to “share” something they have written. Why? Because the burden of demonstrating that an issue is so important and pressing that it should be shared broadly lies again with the author, and lies in the substance and veracity of the arguments, not with the mere desire of seeing their assertions disseminated broadly. Nevertheless, I do recognize that “share this now” is a part of our vernacular now and used by almost everyone of a certain generation on back; but I think it is most suspicious as a herald of misinformation when it is accompanied by….
“They will take this down.”
I sure that at some point something I write, either here or just on just on social media, will be taken down or marked as inaccurate; and when that happens I will probably throw a fit like I’ve seen others do. Until then, I will hold onto the sanctimonious belief that only those intending to spread misinformation feel that it is necessary to preface each video, meme, and essay with “this will be removed” or “they don’t want you to know this.” Who, exactly? The expansiveness, complexity, absolute loyalty, and conflicting goals and values of all of these conspiracies you believe are striving to prevent you from seeing some silly video are really beyond belief. The reality is that most scientists don’t mind at all if you watch the Plandemic documentary or Dr. Stella Immanuel’s speech on capitol hill; what matters is that you know going into it that this misinformation has already been disproven, and that you are armed with the understanding and data you need to work through and decode it. This presents an easy enough decision for me; my goal of helping you sort through this misinformation is best served when it is accompanied by the source material, and posting the video alongside the discussion is a no-brainer. But I think it’s a much more difficult decision for Facebook, Youtube, and Twitter, because they have to worry about the viral nature of this misinformation and the real potential for harm, and can’t accompany every repost or upload with a detailed analysis. Allowing lies to circulate without any disclaimer or precautions to protect those that are easily deceived is irresponsible and cruel; it submits to the whims of anyone with any lie to tell or anything to sell. But the very act of censoring or cautioning about misinformation also serves to reinforce the narrative of oppression; the last redoubt for conspiracy theorists is to use the very censure called down onto themselves for the unreliability of their assertions as proof of their veracity. It is a poor sort of fortress to be sure; yet there are far, far too many who see it as the last citadel of truth.
And, saddest of all, “Share to all of your Bible groups.”
We will talk about the specifics of what misinformation or misrepresentations in this video specifically might appeal to certain streams or factions within Christianity, but for the time being all I can do is grieve, as a follower of Christ, that a video or meme about the pandemic being spread primarily or at a higher velocity within Christian circles is so often a sure sign that it contains little truth and much that is meant to deceive and disrupt efforts of self-sacrifice and self-denial on behalf of our neighbors and community. I have written about how I believe the Church ought to respond to misinformation and why, but it really does feel as though we are behind the World in this area, both in our discernment and in our charity. Lord Jesus, please teach us to be as wise as serpents so that we might be as harmless as doves!
0:26 “Share with… Anybody that doesn’t want aborted fetal tissue fragments put into them.”
This is actually a major claim of the video and the most compelling topic of discussion of the three the speaker introduces, and we will cover it more extensively in just a couple of minutes. For now, let me just say that it is a fact that the COVID-19 vaccine, or any vaccine for that matter, does not contain any aborted fetal tissue fragments! Share with your Bible group, they will take this down!
It also won’t change your DNA, but we’ll get to that too.
0:40 This is the packaging of the AstraZeneca COVID-19 vaccine.
I have not seen the packaging of the AstraZeneca vaccine or any others for COVID-19 and have no reason to believe this individual photoshopped this package (and compelling reasons to believe they are not capable of doing so, as we shall see).
0:59 “It’s called Chad”
ChAdOx1 stands for Chimpanzee derived Adenovirus-vectored vaccine developed by Oxford University. The 1 means it’s the first of multiple Chimpanzee derived Adenovirus-vectored vaccines for COVID-19 that Oxford is working on.
It does not stand for “Chad- whatever that is, zero, or whatever it is- times one.”
1:19 Go to ResearchSquare.com
Research Square is a fine website, just be aware anything you read there is in pre-print; it hasn’t been finalized or peer reviewed yet. That’s the whole point of the website, for people to get feedback before they publish.
1:21 “I want you to learn to do your own research.”
The speaker claims that she wants her viewers to “do their own research” and begins well enough by directing them to Research Square, a reputable website where you can find original sources. But within about 10 seconds she has transformed “doing your own research” into something about as academic and reliable as a Wikipedia binge (or exactly as academic and reliable, since a Wikipedia binge is exactly what it is); googling random words you don’t understand and reading about them, then deciding whatyou thinkthey mean without any background or context. It’s hard to tell whether she is being intentionally deceptive here, or if she really believes that she has attained a solid grasp of these concepts through the methods she is espousing.
That’s not what research is. In the context she is using it, ‘doing your own research’ at minimum means using the amazing, abundant resources of the internet to learn more about the concepts being discussed, and then using that new knowledge to get yourself over that first hump in the Dunning-Kruger effect and figure out 1. what you need to learn next and 2. what the limits are on how much you can actually learn about this on your own. The good news is, as long as you are humble in your assessment of your own understanding, you can also use that knowledge to 3. verify the reliability of whomever you go to to learn more.
We’ve all done this before, haven’t we? When I wanted to talk to an HVAC specialist about a problem with the air supply plenum in my crawlspace, I studied the anatomy of different HVAC systems, read some discussions on HVAC forums, and watched several videos that addressed similar problems. When this didn’t fully solve my issue, I called the specialist; and I used that research, mixed with a healthy appreciation of my own general ignorance on the topic, to both improve my understanding of his recommendations and to inform my gut decision on whether to trust his expert advice or get a second opinion (for anybody who is curious, he said the squirrels shouldn’t be living in there and he’s coming out to take a look on Monday. Based on my independent research, I’ve decided I believe him… though the squirrels have been waging a fierce misinformation campaign).
I’ve written (though not yet published) about this before; I want my patients to use Google. Really. And then I want them to come and talk with me about what they’ve read so I can help them get further beyond the point they could by themselves. Like I said in the article I’ve written that nobody else has access to:
“Most of all we went to school to become very, very good at parsing information about the human body and its diseases, and when it comes to the research you’ve brought in that is the primary way I can help; by helping you sort out which information is actually going to affect you and which isn’t, which you should worry about and which you shouldn’t, and what the underlying motivations might be for the people that published it. I’ve spent countless hours looking at research and studies and clinical trials and have become very good at determining when a study design is too flawed or data is too skewed to be reliable, when there is a strong bias that makes the data suspect, or when a conclusion is not supported by the evidence as it claims. If you are a scientist or a researcher or have training in those areas you may be able to do the same, maybe just as well or better; but for most people that isn’t the case, and it would be a little silly to trust your doctor when they offer one of the services they are highly trained for, such as looking at your child’s ear and determining if there is a bacterial infection requiring antibiotics, and not trust them when they offer another service they have been highly trained for, such as telling whether the research you’ve brought in about the human body is reliable or not.”
1:28 “Don’t rely on us or anyone else, do it yourself!”
This is so subtle and clever that I just wanted to point it out briefly. “Don’t rely on us or anyone else” when doing your research is an attempt to level the playing field between the different sources you might listen to, and it seems so reasonable on the surface.. Don’t listen to me, or your doctor, or a scientist, or an epidemiologist or researcher, only listen to yourself. The problem is that, at least in the viral version of this video, we have no idea who this lady even is. Telling you not to take her word for itor your doctor’simplies those two sources of information are equally educated, informed, and reliable; this from a lady who just called it the “CHAD Zero Times One Vaccine.”
1:49 “Google every single word on here.”
Again, that’s not “research.” If you need to google some of these words to know what they mean then by all means do so; but that is the pre-research prep work, not the research itself. Thinking you understand a concept because you looked up the definition of a word is unmitigated folly, as she demonstrates in a few moments.
1:58 Recombinant DNA doesn’t mean they are reprogramming your DNA. At all.
The speaker and her assistant begin their “research” by looking up the term “Recombinant DNA” on Wikipedia. Wikipedia is great, and one of my favorite things about it is that most articles are written at a level that most lay people can understand (except the math ones. Yikes). So I think if you want to follow the speaker’s advice here and read that wikipedia article, you should. I’ll wait.
But the thing is, she doesn’t actually read it in this video, does she? She only reads the first sentence and then, despite her prior warnings, asks you to take her word on what that sentence means. But listen to the way she says it! The emphasis, the alarm, the righteous anger as she enunciates “molecular cloning” and “genome”! She spits the words out as though it were self-apparent how evil they are, without seeking (or asking you to seek) any additional understanding of what they actually mean. Just one googled word in, and she has entirely abandoned her ‘method’ of research; don’t google every single word in this article that you don’t understand, just take it on her authority that this is bad, bad stuff. She tells you earlier not to be intimidated by scientific terms; but here she actually wants you to be frightenedby them.
If you actually read that article, you will quickly realize that the idea she implies here (and stated explicitly earlier on), that recombinant DNA reprogramsyour genetic code, is actually complete nonsense. In fact, it’s exactly the type of nonsense you would expect if someone’s entire understanding of the science involved was gained through googling random words and reading the first sentence only of wikipedia articles.
The Recombinant DNA got him!
Recombinant DNA describes how the vaccines or medications were developed, not what they do once they are inside of you. Just look at the ‘applications’ section of that same wikipedia article; rDNA technology has been used to develop insulin, accurate testing for HIV, and safe growth hormone for patients with pituitary failure, not to mention interferon therapy for cancer, treatments for cystic fibrosis, and TPA, a life saving treatment for strokes and heart attacks. None of these therapies change your DNA. Saying recombinant DNA therapies change your DNA is like saying that Mashed Potatoes mash you if you eat them. No, the potatoes were mashed during the preparation phase so that they would be delicious for you later on; you don’t get mashed, they do. DNA of fungal or bacterial or animal cells waschanged in order to develop these treatments, so that they would be safe and effective for the people who need them.
Since I’m waxing eloquent here, I’ll give one more analogy. It’s like my first and only experience in debate club back during Freshman year of college. The topic was “is preemptive war justified.” The first team to debate, the “for” team, got to define the terms of the debate and chose to argue that preemptive war was justified because nations have the right to defend themselves if they are the victims of a preemptive attack; so preemptive war, “war initiated by a preemptive attack,” was 100% justified… on the part of the nation that was attacked first.
They changed the very definition of the term to suit the argument that was easiest to defend; they were arguing for retaliatoryor defensive action instead of preemptive, because it was a much simpler position to defend. And the only problem with that is that words have meanings, Keith!
Sorry, I may still have some baggage to work through there. But that’s exactly what this speaker is doing too; changing the meaning of the term ‘recombinant DNA’ and just hoping you won’t notice or indeed read the very article she has pointed you to herself.
There is one more part of this discussion, and it doesn’t have anything to do with what she’s mentioned here, but intersects with this idea of “reprogramming DNA,” even if I don’t think she has the science background to realize it. Here she’s focused on rDNA, but you’ll also hear discussion about mRNA; messenger RNA, the genetic sequences that organisms use to instruct cellular machinery to build proteins. The two vaccines that have recently shown such promise, from Pfizer and Moderna, both use mRNA technology. Traditional vaccines provoke an immune response, teaching your body to produce it’s own antibodies to fight the infection, by presenting your immune cells with non-dangerous particles of the virus that it can recognize and then build antibodies against. Each of these viral particles has to be produced in a lab and enough of them have to be preserved and injected to ensure some are picked up by your macrophages or dendritic cells and then presented to your lymphocytes (T and B cells) to make sure that you really do develop the ability to mount a robust immune response when you exposed to the virus for real later on.
The mRNA vaccines do the exact same thing, only instead of injecting the deactivated viral proteins directly into your body, they only inject a code for them; a code that teaches the machinery in a few of your own cells to build and release the proteins needed to produce the desired immunity. This outside mRNA hijacks the cellular machinery to produce the proteins needed for immunity without any of the proteins that cause illness; and the rest functions just like a normal vaccine. This is the same naturally occurring ‘technology’ that mRNA viruses use themselves. This is great news for people who want to acquire natural immunity; by mimicking the action that the viruses themselves use, which in turn produces our immune response to them, these vaccines have become the closest you can possibly get to acquiring immunity naturally without actually running the risk of getting sick and infecting others. Instead of getting a deadly mRNA virus from a cough or sneeze, you get a safe mRNA ‘virus’ from a vaccine, and from it your body’s own immune system learns how to kill the deadly virus.
This video below explains these concepts really well, starting at the 1:53 mark.
Again, this mRNA technology doesn’t change your DNA. It just sends a message to some of your cells with a set of instructions, just like any common cold would. Your chromosomes, your genetic code, are unaffected; the vaccine doesn’t even interact with them. If an analogy would help, imagine someone ‘hacked’ your network printer at the office. Normally you are the only person who prints to this printer; you write the document on Word or Notepad (judging you) on your computer and then hit “print,” and the signal goes to the printer, which prints the document. But one day you walk in to find that someone else has been printing things to your network printer. That doesn’t mean that they’ve hacked your computer, it just means they have used your paper and ink (and toner! those monsters).
And what did they choose to print? A detailed set of instructions on how to protect your networked printer from hackers. Big Cybersecurity, at it again.
3:00 “We used direct RNA sequencing to analyse transcript expression from the ChAdOx1 nCoV-19 genome in human MRC-5 and A549 cell lines.”
Here is where we enter what is, I think, the heart of what has drawn most people to this video. I think we can quickly dispense with one piece of false information before entering a more important discussion. The ChAdOx1 nCoV-19 vaccine does not use the MRC-5 cell line. This is an inherent problem with both the ignorance of the speaker (and here I do not mean to be insulting, but merely mean the lack of actual education and experience in the field in which she puts herself forward as an expert) and the deep flaw in her ‘method’ of research. This article is not from the vaccine manufacturer at all; it’s from an independent lab that used these human cell lines to study the vaccine after it was produced. You can find the full text here and read it for yourself. The manufacturers did not use those cell lines. In telling you all about the MRC-5 cell line and warning you that;
“One thing [the ChAdOx1 vaccine] definitely has is the lung tissue of a 14-week-old aborted caucasian male fetus.”
Narrator: “It doesn’t.”
the author is stating an absolute untruth based in her own haphazard and unreliable method of trying to find scientific information and uncover medical conspiracies. If her “research” methodology has left her unable to even grasp the basics of who is doing the study and why they are doing the study, or the difference between making a vaccine and studying a vaccine that has already been made, why would you possibly trust her method of research? For that matter, why trust her at all, when she has proven herself so unreliable? Even her assistant, the enigmatic Claire, tries to offer some clarification that the cell line used in the study has been replicated over and over again since the 60’s; that the researchers did not actually abort a child and then collect its cells to study the vaccine (or make the vaccine, as she mistakenly believes); but that attempt is ignored by the main speaker.
What about fetal cell lines in medical research?
Despite the speaker’s severe misunderstanding, and regardless of the tired horror tactic of trying to get you to visualize fetal parts being injected into your children in order to illicit a visceral reaction (there are no aborted fetal parts or fetal cells in vaccines, even the vaccines developed using human cell lines), this is an important question and I think we should spend some time on an actual discussion of it, instead of the sensationalized and inaccurate rage that characterizes its treatment in the video.
I am a pro-life doctor. Like most physicians my views on abortion are nuanced, deeply felt, and strongly based in the lived experiences of my patients. Since this video was designed to spark a visceral reaction among pro-life people in order to make them more susceptible to vaccine misinformation, I think the issue of abortion and fetal cell lines in research warrants discussion on this blog post. I have helped prevent countless abortions, both through providing high quality women’s health services, often to women who otherwise would not have good healthcare access, and by providing compassionate listening, patient-centered care, and judgement free counsel during the most tumultuous times of an unintended pregnancy. There are those that will argue that doctors shouldn’t be pro-life, that my moral opposition to abortion means I can never truly provide unbiased guidance and information to a woman facing this most difficult and painful decision of her life, or that I am somehow unable to respect my patients’ autonomous decision making in this area and help them leave my office more empowered than when they came in. I don’t believe that matches the experience of my patients. I might argue that informed consent, a core principle of medical ethics, is impossible without a robust patient-focused discussion of the medical realities and practical alternatives surrounding the decision to terminate a pregnancy, and that there is reason to believe that these conversations are too often sacrificed or short-circuited once the specter of abortion first arises. It is a debate for another day, to be sure, and with many of the physicians who hold the opposite view I nonetheless share a strong mutual respect, born of proven care for and dedication to our patients, that overrides even our deeply held reservations on this issue. Even on the question of abortion and consent itself, we both believe, based on all of our medical training and the high degree of altruistic concern we bring to our jobs, that we are striving to do what is best for our patients; to help them in the way that is best for them and most consistent with their own stated goals and deepest felt wishes.
Many medications and vaccines use fetal cell lines. The reason is simple; human cells typically work best for studying and developing treatment for human diseases, and fetal cells have unique characteristics that allow cells to achieve, or nearly achieve, cellular immortality; allowing the same cells to be replicated over and over again without any need for additional cell lines to be collected. There is no question that this is a challenging ethical and moral area for pro-life scientists like myself, and strongly pro-life physician and multidisciplinary healthcare organizations, like the Christian Medical and Dental Alliance (CMDA), have discussed and written extensively about it. Here are a few articles CMDA has published, written by conscientious physicians of deep, theologically sound Christian conviction. I hope you will weigh their words and reflections with at least as much gravity as a random person on the internet telling you to “pray big” and share her video with as many “christian-loving” people as possible.
There are a few salient facts you should know about this area of medicine.
No children are aborted or have been aborted for the purpose of developing medicines or vaccines. The sensationalism that some forces in the anti-vaccine movement are willing to engage in knows no bounds, and it is not uncommon to hear the propaganda that these unborn babies were actually aborted for the purpose of being used in medical research. This is simply wrong. The few unborn children whose cells (or accurately, copies of copies of their cells) are regularly used in medical research and development were likely aborted for the same reasons that most abortions occur; the unbelievably difficult balance of perceived goods and anticipated challenges faced by a woman who had not intended to become pregnant. These mostly occurred in the 60’s and 70’s, and cell lines (copies of cells) derived from those same aborted fetuses have continued to be used ever since without the ‘need’ to derive new cell lines from abortions occurring today. For instance, HEK 293, the actual cell line used in the development of the ChAdOx1 vaccine, was derived from an abortion in The Netherlands in 1973; we simply do not know the story of the woman who chose to have this abortion, or the reasons behind her choice.
There are no fetal cells in vaccines; not even in vaccines developed using fetal cell lines. Vaccines are not a ‘mix’ of fetal cells and viral particles, not by any stretch of the imagination. When fetal cell lines are used to grow viruses that infect humans in the vaccine development process, it is distant to the final product of the vaccine, which has also been through multiple rounds of purification. The human cell lines are used to grow the virus and deactivate it; they are not included in the actual material injected through a syringe to produce an immune response in our bodies.
Not all vaccines use human cell lines. There are vaccines for almost every vaccine preventable illness that are designed using methods that even the most rigorous pro-life groups consider ethical. When the anti-vaccine movement tries to convince you that all vaccines are suspect from a pro-life perspective, they are rather co-opting a pro-life position for their own aims rather than being a legitimate part of the pro-life movement.
Like the CMDA doctors above and most pro-life physicians and scientists, and even the Vatican, I believe that using vaccines and medications not developed using fetal cell lines from aborted human beings is strongly preferable whenever possible, and that this is an area where continued economic and moral pressure can encourage pharmaceutical companies and research institutes to pursue alternative means of developing novel treatments to human disease. However, the principles of whole-life pro-life ethics also dictate that a treatment or preventative measure developed in part through material derived from a past harm through abortion, with no potential to cause further harm in this same way but massive potential to prevent loss of life (including unborn human life) is still, clearly, a moral good; a position even Popes have affirmed. In saving the lives of a great many people from a single death that would not have been prevented regardless, we derive the greatest possible moral good from what was an undeniably tragic situation for all involved.
For pro-life persons, accepting a vaccine that was developed from fetal cells collected 50 or 60 years ago makes them neither complicit with nor promoting of a depreciation of human life. But seeking treatments developed using alternative means may send a message to pharmaceutical companies that these issues are indeed dear to their hearts and that their collective will is that these methods in research would become a thing of the past.
4:23 “This is what they want… They KNOW this vaccine is going to hurt people or kill people so badly.”
A few things here.
If there is a way to kill people not so badly, please let me know. We could be on the brink of a medical breakthrough here.
Who is “they” anyway?
She jumps around so much in this video that the viewer is left to assume, just like with the MRC-5 discussion, that this last bit is screenshot from the original papers from the vaccine manufacturer; that the people making the vaccine have, in their published study, asked the universe at large to supply them with some sort of computer program or something to help them sort through all the people they intend to maim or kill. We’ve talked before how conspiracy theories rely on this weird paradox where shadowy conspirators are both incredibly clever, subtle, and nigh-invulnerable but alsoso clumsy as to announce their real plans in such a way that some random person on the internet can piece it all together with a 5 minute video. Pfizer or Moderna publishing “please help us, our excel spreadsheets aren’t robust enough to keep track of all the victims we are after” at the bottom of their research would certainly fall under this phenomenon.
But this isn’t from the vaccine manufacturers. It’s from the Medicines and Healthcare products Regulatory Agency (MHRA), the British counterpart of the FDA. And it isn’t from a research paper, it’s from their contracts division, announcing the technology services they are hoping to contract with as they anticipate the release of these vaccines.
Why would the MHRA or FDA want to track possible adverse reactions to a new vaccine? Because it’s literally their job.
And why would they anticipate a “high volume” of reported adverse reactions? Because we are in the middle of a highly politicized, deeply contentious global pandemic; billions of people are going to get these vaccines, and some of them are going to have very mixed feelings about it. Adverse reactions to vaccines range from the common but mild to the serious and extremely rare, but reported or perceived reactions are all over the place. I saw a patient yesterday who believed that his flu shot had caused him to feel fatigued and sore the next day (it had), and also to have six days of diarrhea and loss of taste and smell two weeks later (it hadn’t). He tested positive for COVID-19, the true source of his symptoms. I’ve also had patients who believed their flu shot gave them COVID-19, which is utterly impossible.
Vaccines feel scary; they are sciency and mysterious and they are going into your body, and you are taking someone’s word for it that they are safe and a wise decision. I get that. A new vaccine is even scarier, and a new vaccine for a virus that is deadly, has changed our entire lives over the past year, and is surrounded by a thick haze of misinformation and conspiracy theories is even scarier. Some of the folks getting that vaccine are going to do so, probably to keep those around them safe, only after warring within themselves over it (even I told you I’ve still got some research to do before I’m fully satisfied with the decision). For some of those folks, anything medical that happens to them in the next few months might potentially feel like the negative fallout of that one difficult decision. The point of the MHRA using an AI tool to augment their ability to analyze that data is so that they don’t miss any real adverse reactions hidden in all of that noise; to make sure that if the vaccine is dangerous after all, despite the safety demonstrated in clinical trials, they discover it as quickly as possible. Again, because that’s their job. This is evidence that the people tasked with making sure the vaccines are safe really do take that role seriously; not evidence that someone is planning to hurt you and wasn’t sneaky enough in hiding their intentions.
5:01 “I don’t know how you do it, I’m not technical.”
After watching the same 5 minutes of these folks pointing a shaky phone camera at their computer screen and pulling up various image preview programs and web browsers over and over again while writing this blog post, I can now verify that this is the single most true and reliable statement in the entire video.
It looks like I’m just being cheeky at this point, so I guess it’s time to stop there.
The following is a short repost from social media.
Well, call me triggered.
I’m a Family Medicine Physician, and every day for the past 3 months I’ve seen patients for COVID-19. Every day for 3 months, I’ve told every patient I’ve diagnosed with COVID-19, with the exception of the few I’ve sent directly to the hospital because of the severity of their symptoms, the same three things:
1. Don’t be afraid of COVID-19.
I say this to my patients for a few reasons. First, because I am mostly seeing patients in the outpatient setting, my patients and I have the privilege of emphasizing this point. Second, for many patients who have a mild to moderate severity course of COVID-19, anxiety is a very real issue, and I want to make sure that while they are recovering they are not sitting at home wondering when the virus is going to get them. Most people who get COVID-19 don’t end up in the hospital (as we have been saying since the beginning of the pandemic), even fewer end up in the ICU or die from the virus (as we have been saying since the beginning of the pandemic). The virus is very, very dangerous, but our brains are bad at statistics; just because this is the most dangerous viral pandemic since the Spanish Flu of 1918 doesn’t me that your individual chances of dying are high or that getting deathly ill is a foregone conclusion. If I were mainly seeing very sick patients in the hospital or ICU I wouldn’t be saying this as much; we would be talking more about treatment and response than about the patient’s anxiety about getting sicker, though the latter certainly deserves our time and attention in any clinical setting. When a patient is struggling to breathe, “don’t be afraid” is a theological statement rather than a clinically valid reassurance, and it typically gives way to “I am with you; I am here and I am going to do my absolute best for you.” But in the outpatient setting, talking with patients who are worried about how COVID-19 will affect them and their children and their friends, “don’t be afraid” is an extremely important part of the conversation.
2. If you have the following symptoms, go to the hospital.
As important as “don’t be afraid” is, it is equally as important to talk about what we call emergency and return precautions. Yes, for most people COVID-19 is not deadly; but it is for some, for many in fact, and we do not have any perfect way of predicting who will have a more severe course. For my healthy patients in their 20’s and 30’s, the chances of ending up severely ill are extremely low; yet people who are medically just like them- same age, same paucity of risk factors- have died from the virus. The same for parents who are worried about their children; children are at extremely low risk from COVID-19, yet some children have died from the virus. I can look my young, healthy patient in the eye and honestly tell them I expect them to be fine; but I cannot promise them that they will be, and that’s a vital distinction. So with each and every patient, in addition to reassurance, we talk about what to look out for. Shortness of breath. Chest pain. Severe malaise and fatigue, even syncope; passing out or almost passing out from the toll the virus is taking on your body. We talk about oxygen levels if they happen to have a pulse oximeter at home, and signs of hypoxia if they don’t. We discuss both the reasons they would come back to see me in clinic and the reasons they would skip my clinic and go directly to the Emergency Department instead. With my older patients or patients who have known risk factors (most Americans, in fact, including myself, considering that risk factors for a more severe course of COVID-19 include hypertension, diabetes, obesity, chronic lung disease and other very common ailments), this discussion is even more important, because even though the odds are still in their favor, their ending up in the hospital or dying from COVID-19 is not nearly as unlikely. I want my patients to be free from fear; but I also want them to be equipped with the knowledge they need to make sound choices if their symptoms do worsen.
3. Please keep the virus from spreading to others.
This piece of guidance is no less important than the previous two. If you are healthy and young and your chances of dying from COVID-19 are very low, that’s really wonderful; but self-isolation during your illness is still the responsible, kind, and charitable decision because not everyone is as lucky as you. The case fatality rate of COVID-19 is much higher than even very deadly illnesses like the flu, and it is very, very contagious. With each and every patient I discuss the precautions they can take to keep the virus from spreading to their own family, and of course the responsible social decisions like sheltering at home during their contagious window and alerting their close contacts so they can self quarantine. It’s one thing to tell yourself that you’ve only exposed other people at similarly low risk to yourself, but once you have spread the virus to someone else you have no control of whose grandmother, whose father in poor health, or whose immunocompromised child it spreads to from there. I said before that we are bad at intuitively comprehending statistics; the COVID-19 virus, like most illnesses, is unlikely to cause death to any given individual regardless of risk factors, but is extremely deadly in aggregate; containment is still our best strategy for keeping the 210,000 deaths in our country from doubling or tripling by the end of this pandemic. The reality is that most people get this; most people I talk to understand the need and are concerned about keeping their families and communities safe. But there is a counter-narrative being promoted by some that rejoices in defying all calls for caution, sober mindedness, or charity when it comes to COVID-19, and so the reminder from me, the doctor actually seeing the patient face to face in clinic, becomes that much more important in case my patient has been lured by these cruel and irresponsible ideas.
These are the three pieces of advice, the three categories of discussion that I have with each and every patient. It is time consuming; it appropriately turns what might be a 5-8 minute visit into a 10 or 15 minute visit. It requires careful explanation of statistical and clinical concepts that might be challenging. It is worth it, because the proper way to approach a diagnosis of COVID-19 is with caution on behalf of others and preparedness rather than fear for yourself and your family, and it’s my job as a Physician to equip my patients with the knowledge and tools they need to approach the virus this way, even in the face of anxiety and rampant misinformation.
So when I see someone with a platform like President Trump’s endorse the firstpoint of not being afraid of the virus, follow the secondpoint of going to the hospital when his symptoms escalated and he experienced hypoxia and shortness of breath, and finally utterly disregard and contradict the third point of taking precautions on behalf of others, I am, I think very understandably, upset. Because when a doctor or a nurse survives COVID-19 (and many haven’t), contracted by putting themselves in harm’s way every day and despite taking maximum precautions to keep themselves and those around them safe, they rejoice that they are now able to dive back into the fray, fighting the virus with no less caution but somewhat less stress and anxiety for their own health, knowing that reinfection is very likely a rare occurrence. But when the president contracts COVID-19 by ignoring all precautions and survives it with the help of state of the art high-level hospital care, expensive and experimental treatments, and a private team of doctors and nurses, his first statement after leaving the hospital is one that builds upon his long-standing guidance and example of not taking precautions or acting to protect those around you, despite neither you nor your family and community having anything like the medical access that helped him.
Please keep yourself and others safe. Don’t be afraid of the virus, but please act in charity to those around you by taking reasonable and proven precautions like wearing a mask, maintaining physical distancing, and engaging in sound epidemiological principles like getting tested if you are ill, self-quarantining if you are exposed, and honestly and proactively participating in contact tracing if you are diagnosed.
Edit #1: I will go ahead and anticipate a couple of objections to this post. First, some people are going to claim that the facts I’ve shared here are inaccurate; that the ‘CDC admitted’ that only 6% of the deaths were actually from COVID-19, or that the fatality rate is actually lower than the flu, or some such nonsense. For people who still believe these pieces of COVID-19 misinformation, there is no shortage of good explanations and rebuttals available on the internet and I suggest finding and reading one. For people who don’t mind a long and mediocre rebuttal over a good one, I’ve written a few myself over at tjwebbmd.com.
Second, some people are going to look at this tweet from the president and say, “but TJ, he isn’t discouraging caution or telling people to take COVID-19 less seriously! He just said don’t let it dominate your life, that could mean lots of things!” To those people I will say, along with Doctor Archibald from Veggie Tales, “Stop being so silly!”
When I tell my patient “don’t be afraid” after reviewing their vital signs, asking about their symptoms, carefully examining them and listening to their heart and lungs, and carefully talking through emergency precautions and transmission control measures, they are absolutely not confused about what I mean. And nobody in America is confused about what the president means when, after months of promoting misinformation, minimizing the pandemic, shirking transmission control guidelines even to the point of endangering his secret service and staff during his own illness, refusing to wear a mask (and then only wearing one intermittently and with a wink at mask truthers when he does), he then says to ‘not let it dominate your life’. And nobody will be surprised when the ongoing unwillingness of our national leadership to take the pandemic seriously, and encouraging others to do likewise, results in more cases, more severe illnesses (and associated suffering and medical debt), and more deaths.
Edit #2: On the same day that I posted a short essay titled “Don’t Be Afraid of COVID-19”, Dr. Emily Smith, Your Friendly Neighborhood Epidemiologist, posted a short essay saying that Yes, We Should Be Afraid of It. Now, Dr. Smith is so much smarter than me that this would normally be enough to make me immediately delete my post; but thankfully, it turns out we are saying essentially the same thing, despite the seemingly contradictory essay titles. To understand what Dr. Smith and I mean when we say you should/shouldn’t be afraid of COVID-19, go and read her essay where she discusses the difference between unhealthy fear and wisdom, the latter being something our national response to this very deadly and dangerous virus has been sorely lacking.
One thing that has become predicable throughout the SARS-CoV-2 pandemic is that any story, any recommendation, any development, or any piece of data that can be interpreted as meaning that the danger of COVID-19 has been inflated, misrepresented, or exaggerated by medical experts will be interpreted that way by a large percentage of our population. This is no longer surprising, but honestly it’s also completely understandable. We all hate this pandemic. Whether you are working on the front lines in clinic or in the trenches at the hospital treating COVID-19 every day, whether the virus has harmed or killed a friend or family member, whether your job or business has been affected, or even if you just really miss people, we are all ready for this to be over. The hard path forward involves biomedical research, redoubling mitigation efforts that we are all exhausted of, and at this point, modifying holiday plans and preparing to deal with the quagmire of cascading clinical probabilities that are required to fight the virus in the midst of cold and flu season. But the quicker and easier path to getting rid of this hated virus is undoubtedly to just choose not to believe in it at all. And while this “just don’t believe in it” approach is likely to be about as effective as it has been for any of the other problems I’ve tried it for (taxes, bills, excess carbs), I amsympathetic to the appeal of it. If the pandemic has not affected you directly- or maybe even if it has- it may be very tempting indeed to buy into a video like Plandemic, which tells you that the whole thing is just a government conspiracy, or into the America’s Frontline Doctors‘ video which tells you that there is already an easy and inexpensive cure if you just drive to the see the right doctor. Life can be normal againright now, these sources say; all of your hopes are true and all of your caution and privations can finally come to an end. I’m not saying it’s right, I’m just saying I get it.
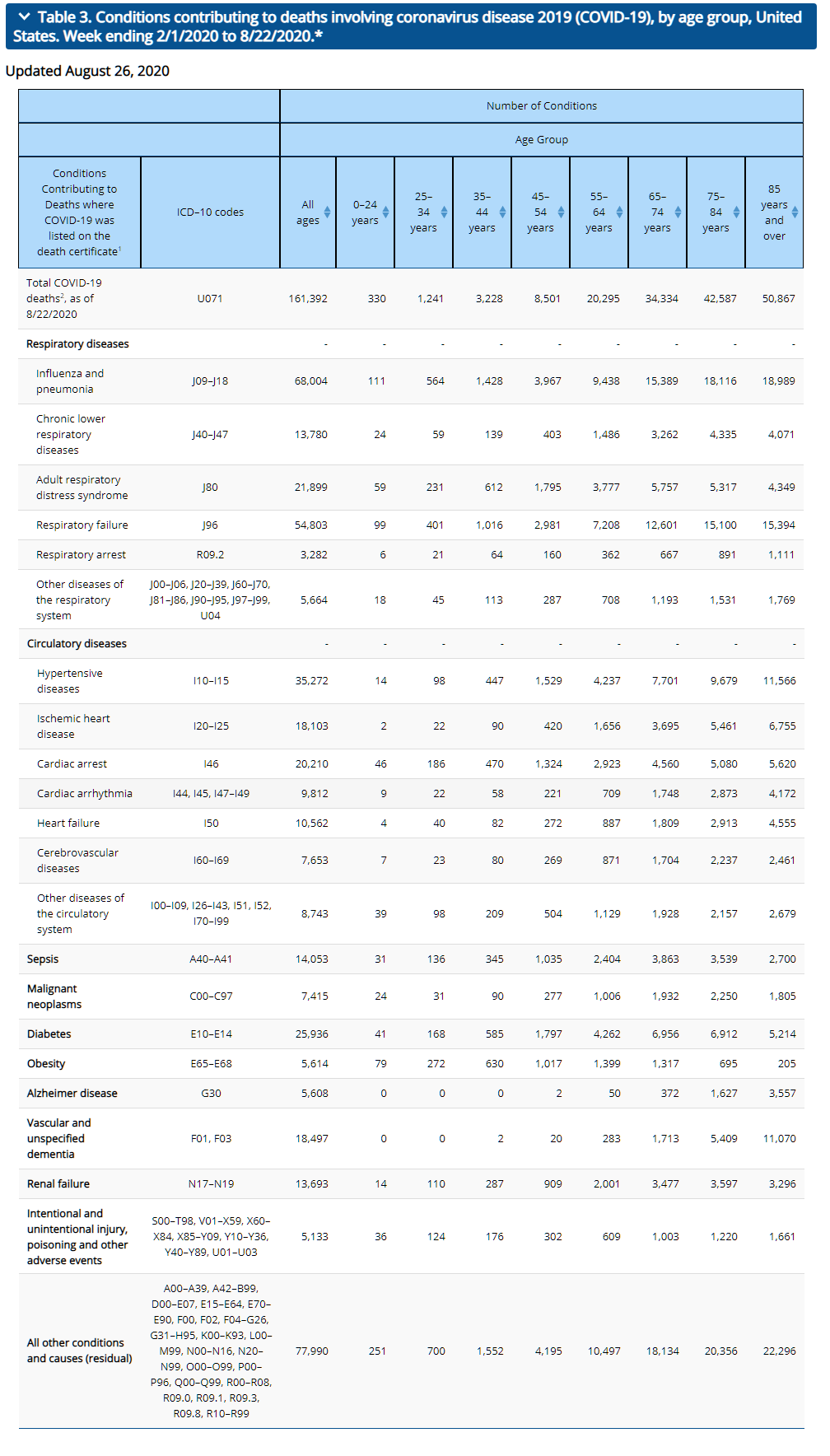
But what has been surprising- and consistently surprising, to me at least- is which wild facts people will latch onto to create these false narratives. Before today, I would never have expected this paragraph from the CDC’s weekly updates by select demographic and geographic characteristics to be the next cause of viral misinformation:
Yet here we are.
What is the claim being made?
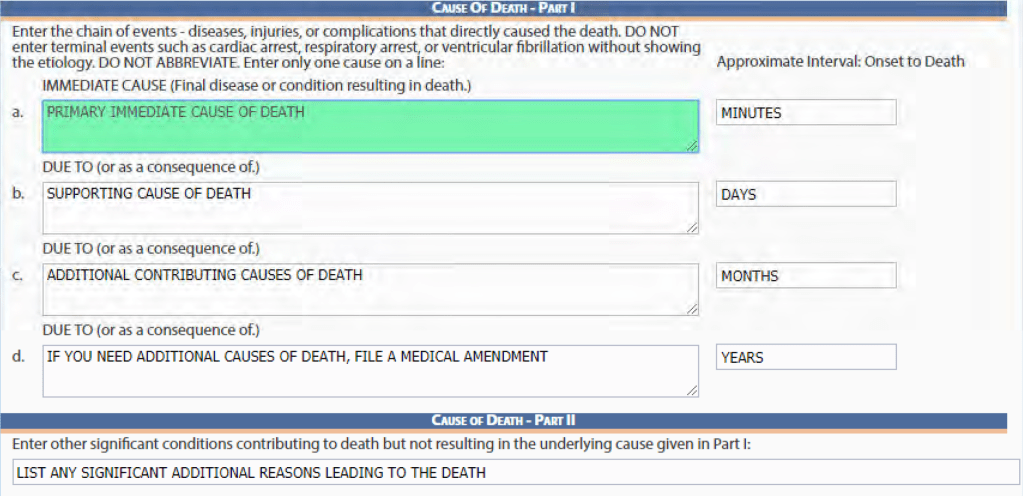
If I chose to end this blog after today, I would feel I had really come full circle; my very first blog post was about the myth, popular late in March (and persistent even today), that doctors were lying on death certificates to make the virus seem more dangerous than it really was. Today’s myth is that analyzing the diagnostic codes on death certificates –those incorruptible sources of reliable data- reveals that the virus isn’t actually very dangerous at all, and the CDC has just admitted to it. Bypassing the irony that this later misinformation is being circulated by exactly the same people who have been sharing the first for months, we can spend today’s blog post (48 hours late as usual, this time because our internet was out all day yesterday!) analyzing these claims. They seem to have taken two forms.
The first, and more moderate, is to claim (or at least strongly imply) that because 94% of deaths from COVID-19 also had other diagnostic codes listed on the death certificate, it means that people without ‘underlying medical conditions’ are not actually at a very high risk of dying from the virus. And in one sense this is true, even if this new data from the CDC doesn’t actually really have anything to do with that. Your Local Epidemiologist says this better and more succinctly than I can:
And she’s absolutely right; we have been saying this from early in the pandemic. But not just saying it; thinking it and believing it, too. Every decision I make as a physician, from admitting someone for COVID-19 to starting or stopping a medication, referring them to a specialist, or even recommending exercise or lifestyle changes has to take into account their medical history (and a host of other factors). While there are some symptoms we can warn everyone about, the counseling and support we provide for patients seeking evaluation and treatment of COVID-19 has a lot to do with their individual risks from the virus and how it might manifest in their lives based on their age and other medical conditions. This 6% misinformation became viral just yesterday, yet if you asked any doctor last week they would have already told you that the younger and healthier you are the less likely you are to end up in the hospital or die from COVID-19, and the more medical complications you have the more concerned they are about you having the virus. I know because this is exactly what I was saying to people in clinic last week, and the week before that, and the week before that. Yes, many young and otherwise healthy people have died tragically and shockingly from complications of the virus; but this is still a rare occurrence on the whole compared to the number of young, healthy people who have had the virus. When I counsel people at low risk of complications from COVID-19, we of course talk about the signs and symptoms they should watch for that would trigger a trip to the ER, like chest pain and shortness of breath; but I also want to make sure they aren’t sitting at home, anxiously wondering when the virus is ‘going to get them’. I want them self-isolating; I don’t want them to be afraid. But this relative reassurance towards the young and healthy is actually undercut ever so slightly when you combine headlines like these with the actual data being reported from the CDC, which I’ve included below.
When you look at the other diagnostic codes listed in the table above, you will notice that codes like E78.2 and I10 are listed; high cholesterol and high blood pressure, respectively, both conditions I’ve been diagnosed with in the past (and probably still have, if I would ever go get a check-up. Doctors really do make the worst patients). At 35 and having never spent a night in the hospital as a patient in my life, nobody would call me high risk for complications of COVID-19. In fact, if I contracted COVID-19 and died of it this week, two things would happen. First, my blog would probably get a lot more hits for a couple of days (and this paragraph in particular would seem very bitterly ironic). But second, I would be held up as an example of how being young and in relatively good health is not a perfect guarantee of safety from the virus. YetI would be a part of the 94%, not the 6%.
The reality is that in saying “94% of COVID-19 deaths had underlying conditions,” these stories are addingnothingto and are in fact dumbing down the more sophisticated knowledge we already have, and share with our patients daily, of the most important risk factors and conditions that predispose someone to COVID-19 being a likely threat to them. They are meant to lure you into a false sense of security, because it’s so easy to think they mean somebody elsebesides you(even if you do in fact have some of those diagnoses, like I do) and a relatively small group of people. But when I look at the chart, I realize that even I fall into that group with “2 or 3 underlying medical conditions” that they are saying 94% of the COVID-19 deaths occurred in; in fact, most Americans do. And when a statistic includes me, privileged to be in pretty good health as I am, but also my patient battling metastatic kidney cancer and my patient suffering from both CHF and COPD, maybe it just isn’t a very useful statistic in the first place.
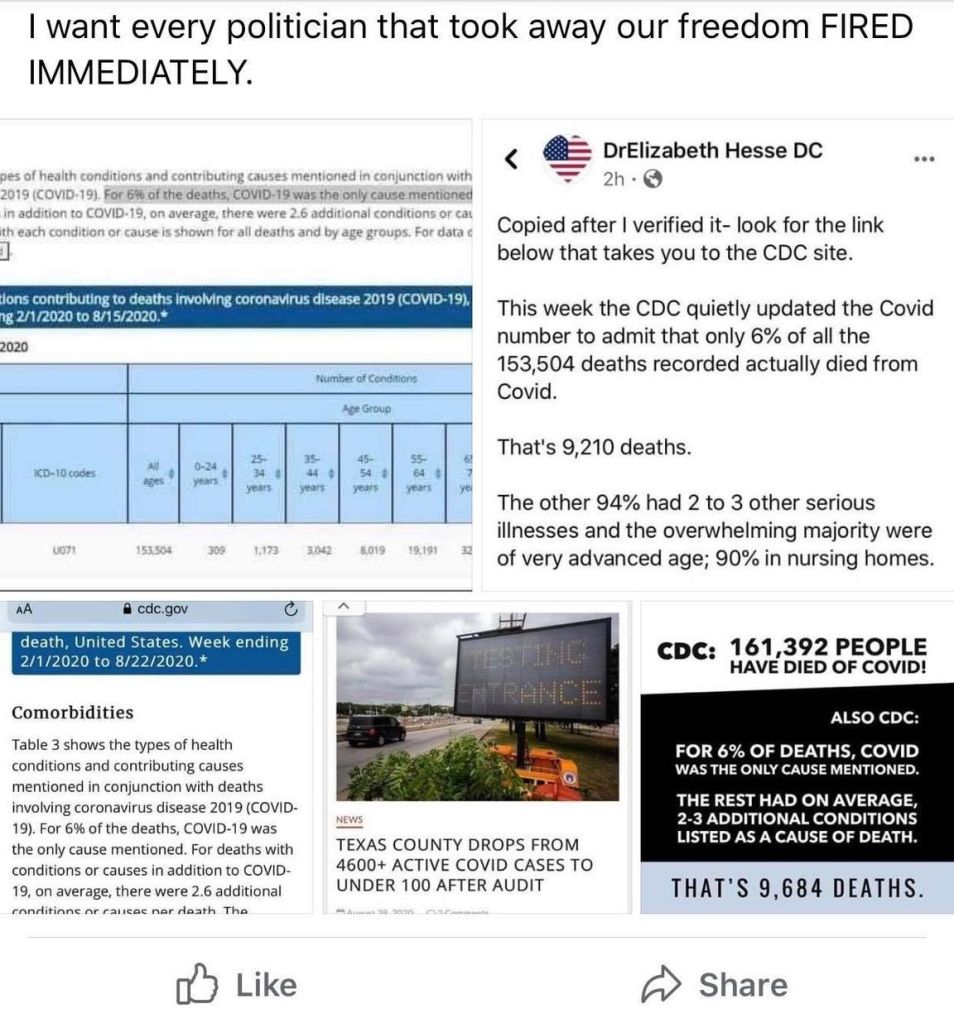
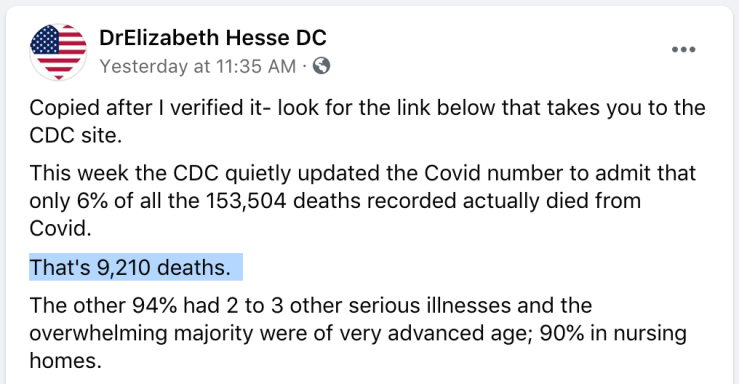
But the more dishonest and blatantly ridiculous claim, which has absolutely no justification, is to say that only the 6% of deaths with just COVID-19 listed on the death certificate actually count as COVID-19 deaths. Take this one Facebook poster who has been widely shared, who had the gall to take this to the next step and “calculate” that only 9,210 people had “actually died from Covid.” Probably because she was willing to put a number on the deaths, this post has been shared 21,000 times on Facebook; but it’s hard to believe that someone with a doctorate degree, any doctorate degree, could have such little grasp on basic statistics.
No, No, No.
This post entirely misrepresents everything within our complex understanding of medicine regarding the impact of medical comorbidities, the myriad causes and steps leading to death in COVID-19 or any other illness, and even the very process of completing a death certificate. In her estimation, Dr. Hesse is saying that a diagnostic code on the death certificate other than COVID-19, literally any other code, is sufficient evidence that the patient did not die from COVID-19. This is not only preposterous and dishonest but also just plain silly. We are going to explore these issues more thoroughly in the next section, but briefly, just look at the chart above and begin googling ICD-10 diagnostic codes for yourself to test the logic of her interpretation. Yes, I can absolutely believe that some of the patients whose death certificates reflect both COVID-19 and also diagnosis code C71, Malignant neoplasm of brain, may actually have died from the brain cancer and were only found to have the virus incidentally. We can’t tell from the data if that did in fact happen, or how many patients might have such a presentation. But with COVID-19 being an acute illness and brain cancer being a chronic illness, the disease and treatment of which also predisposes you to infectious illnesses, it is at least as reasonable to assume that the majority of patients who died from “COVID-19 and brain cancer” actually died from COVID-19, which they were more vulnerable to because of their pre-existing brain cancer.
But Dr. Hesse’s assertion that only the 9,210 “COVID-19 only” deaths should count also has to stand up to scenarios like, say, any hypothetical patient who was certified as dying with COVID-19 and R09.3, Abnormal sputum, or COVID-19 and N20.0, Kidney stones. Again, we can’t tell fromthis data whether any such patients with only those codes exists; but neither can Dr. Hesse, and for her argument to be valid, each and every possible diagnostic code included in the chart above would, if added to a COVID-19 death certificate, nullify COVID-19 as a primary or contributing cause of death. That is what she is saying, and it is obviously ridiculous. What this error betrays is a complete misunderstanding, whether intentional or accidental I know not, of how death certificates are completed and the information they are meant to capture. Even though it means a longer essay, I do think it’s worth taking the time to revisit this again.
What information do we include in a death certificate?
Once you have been trained to complete death certificates (and have actually done it), this “6%” argument is not even momentarily tempting or convincing. I know what you are thinking; “but TJ, we haven’t been trained to complete death certificates, so you are asking us to trust you with this area of specialized knowledge we don’t have access to.” Well good news reader, the Texas Department of Health and Human Services, DSHS, has got you covered. If you want to understand this 6% statistic from the CDC, I highly recommend that you watch from 1:44 to 3:08 of this video.
Sorry, the secret tutorial video they released after COVID-19 is password protected. Also, that was a joke.
Obviously each state will have its own version of this software, but they are all intended to convey the same information; the death certificate is not a high-stakes multiple choice interrogation asking the doctor, “What disease caused the patient’s death? Was it COVID-19 or heart failure? ANSWER THE QUESTION!” Rather it is an opportunity to distill the sequence of events leading to the patient’s death, recorded in greater detail in the medical record, into a structured narrative that explains how they died. When a doctor includes coronary artery disease on the death certificate, they are not making a political statement or a value judgement, but rather an honest reflection of the part this disease played in the patient’s death based on their medical knowledge and their intimate understanding of the progression of illness as the patient’s treating physician. And it is exactly the same with COVID-19. Moreover, this is not something that the physician derives a financial benefit from or an opportunity to defend the medical care the patient received (in fact, I have listed iatrogenic injury on the death certificate when I felt that my own mistake or that of another medical professional contributed in some way to the death of the patient), but rather something that is important for public health information and, in various ways, important to the family of the deceased.
Briefly, I’d like us to complete a medical certification for a death certificate together, again using my hypothetical death from COVID-19 as an example. In this scenario, let’s say that I get sick with cough and loss of taste and smell this week and am diagnosed with COVID-19. Around day 10 of my symptoms I begin to experience chest pain and shortness of breath, and I go to the ER. There I am found to be hypoxic and my chest x-ray shows bilateral peripheral consolidation consistent with ARDS. they begin to treat me with dexamethasone, remdesivir, and oxygen. Over the next few days my respiratory distress increases and, even allowing some permissive hypoxia in order to avoid intubation, the doctors simply cannot keep my oxygen level within safe parameters; they make the difficult decision to intubate me and put me on a ventilator. I am ventilated in prone positioning using the latest and best evidence-based ARDS/COVID-19 ventilation strategies from the genius doctors over at EmCrit and PulmCrit. Unfortunately, I continue to become progressively, severely hypoxic, and eventually suffer cardiopulmonary arrest. Resuscitation is attempted but ultimately efforts to revive me prove futile; the lungs are not compliant, effective ventilation still cannot be achieved, and return of spontaneous circulation is impossible. I’d make a joke about making the life insurance check out to my wife, etc. at this point, but honestly when I reflect on how many people have died from this sequence of events over the past six months, it’s pretty sobering. I’ve made myself sad just now thinking about all of the families that have lost a mother, father, sibling or grandparent in exactly this way.
Once I’ve died, the doctor treating me will have to record it in a death certificate; we can use the Texas system, since it’s what I’m familiar with.
Here in Part I we list the immediate cause of death. In my case, it’s going to be cardiac arrest. Because this is technically the immediate cause of death in every death except those caused by brain death, some doctors would leave this out. Since resuscitation efforts were made and the arrest was a distinct medical event, I would probably include it, but an argument could be made either way. Next we need to describe the events that led to this. I’m not going to include respiratory arrest because I would feel it was a bit redundant, and besides, I was already not breathing on my own when the cardiac arrest happened since I was on a ventilator. Instead, I would say the arrest was due to respiratory failure. The respiratory failure was due to ARDS, Adult Respiratory Distress Syndrome, and you could make a case here for including viral pneumonia as well. Finally, the ultimate cause of this cascade of complications is my infection with COVID-19.
Next I would need to list any other contributing factors in Part II, and here is where the quandary usually comes in, because now I have to decide whether my high blood pressure and high cholesterol belongs in Part II, “other significant conditions contributing to death but not resulting in the underlying cause,” or in Part I further down in the chain of events. In this case it’s easy; my high blood pressure is a significant medical issue and made me at higher risk from the virus, so it belongs in Part II; but it didn’t cause me to get COVID-19, so it doesn’t belong in Part I. My chronic right shoulder pain didn’t contribute at all and gets left off the death certificate. These decisions aren’t always easy; sometimes a condition didlead directly to death in chain of events that are causative narratively even if not pathophysiologically; for instance a patient who is hospitalized for a hip fracture and then develops sepsis from a central line. The hip fracture didn’t cause the infection that kill them, but it was a direct part of chain of events. But what about the vertigo that caused the fall that caused the hip fracture; does that belong in Part I or Part II? I have a physician friend who works in hospice care who completes death certificates almost every day (I have completed maybe a dozen); he says this is typically the hardest decision point when it comes to completing a death certificate, deciding what was really a cause and what was ‘only’ a contributing factor. Still, it’s straight forward enough in my hypothetical case, and we can finalize my death certificate as follows:
Cause of Death – Part I: IMMEDIATE CAUSE a. Cardiac Arrest. DUE TO b. Respiratory Failure. DUE TO c. Adult Respiratory Distress Syndrome. DUE TO d. COVID-19.
Cause of Death – Part II -Hypertension, Hyperlipidemia
So, for young, relatively healthy me who died from the most stereotyped and straightforward case of severe COVID-19 I can conceive of, we have 5 other diagnostic codeslisted on the death certificate between direct cause conditions and contributing conditions. Contrast that to what a Texas death certification with only the diagnostic code for COVID-19 -the only types of death certificates Dr. Hesse believes count as COVID-19 deaths- would have to look like:
Cause of Death – Part I: IMMEDIATE CAUSE a. COVID-19 DUE TO b. ________________________ DUE TO c. ________________________ DUE TO d. ________________________
Cause of Death – Part II ________________________
My friend, the hospice doctor, has completed over 500 death certificates (a conservative estimate) since finishing residency a few years ago. He says he has included just one diagnostic code alone maybe twice. What Dr. Hesse sees as the ‘real’ COVID-19 deaths, these 9,210 death certificates without any other documented diagnoses, I see as an anomaly; I am forced to ask myself how that many death certificates were complete in what I consider to be such an incomplete and insufficient manner. I have two theories, aside from some doctors simply not giving the proper attention to the task that they should have or not understanding the importance of completing the death certificate thoroughly. One is that some of the doctors who have been taking care of patients in this pandemic simply might not be familiar with how to complete a death certificate. This pandemic has brought doctors out of retirement and graduated 4th year medical students months early to shore up the frontlines; surely some just haven’t had even the 5 minutes of training from the video above and don’t know how to complete the forms properly; frankly it’s a low priority in their training right now. But second, some of the death certificates for COVID-19 patients have been completed by doctors who were incredibly overwhelmed. When we consider places like New York City, where doctors and nurses were dropping from exhaustion during shifts and barely had time to document at all, and were seeing multiple deaths per shift, each and every shift for weeks, it is reasonable to expect that some of those doctors no longer felt that taking the extra time to document a complete death certificate series of events was a priority. I can’t argue with them; it wouldn’t be. As important as the death certificate is to the patient’s family and for public health purposes, it is a low priority in a crisis when your time would otherwise be spent taking care of living patients or trying to shore up your own physical and mental reserves. If this is the case, the doctors who typed “COVID-19” and submitted the death certificates probably had no idea that such an action would contribute to even more dangerous medical misinformation threatening to extend the pandemic a few months later; a lesson in unintended consequences.
So what do all of these other codes mean?
There are many ways to interpret the diagnostic codes listed in the comorbidities table from the CDC’s latest update. We could spend hours in speculation, wild surmises, or careful parsing and analysis (if you’re a nerd) to try to recreate the narratives of the deaths represented by this data. The amount of analyzing, explaining, and even guesswork we could devote to this is endless. But briefly, I’d like to explain how to understand the majority of these diagnostic codes and the diseases, conditions, or symptoms they represent by considering them in three large categories.
Other ways of describing COVID-19. The first category that these “other diagnostic codes” fit into is simply other ways of describing the symptoms and complications of COVID-19 itself. If I treated you in the hospital for a CVA (cerebrovascular accident; a stroke), but I also added on diagnosis codes for right arm paralysis and slurred speech, you wouldn’t review the medical record and say, “see, I wasn’t treated for stroke after all! They were treating me for right arm paralysis and slurred speech and just added that ‘stroke’ code on because Dr. Webb probably gets some sort of kickback for it.” The paralysis and the slurred speech delineate more specifically which stroke symptoms you experienced; their inclusion creates a more complete record of your presentation and treatment. In fact, it isn’t at all uncommon to have multiple diagnostic codes that actually say the same thing, due to different doctors and different departments interacting with your medical chart and, again, for the sake of completeness. If I have already added “slurred speech” to your chart, the neurologist later adding ‘expressive aphasia’ doesn’t actually add anything to your medical record (except a little reminder that she’s smarter than me); but it might be more appropriate to document it this way for the referral to speech therapy she is ordering for after your discharge, or to have this diagnostic code associated with the MRI. The synonymous diagnostic codes are repetitive, but it doesn’t necessarily follow that they are redundant.
Now apply this logic to death certificates and COVID-19. We’ve already discussed that most doctors would like to be as complete and thorough as possible with death certificates and that it is somewhat odd to list only one diagnostic code without providing a fuller narrative. When we see diagnostic codes like J96 (respiratory failure; 54,803 cases), R09.2 and I46 (respiratory and cardiac arrest, 3,282 and 20,210 cases respectively), and J12.9 (viral pneumonia, unknown number of cases, but contained within the “Influenza and Pneumonia” group), all the doctor is doing is using additional diagnostic codes to clarify the events affecting the patient’s lungs that led to death. In fact, it would not be inappropriate to include all four of these codes for many COVID-19 deaths, because the natural history of viral pneumonia due to COVID-19 leading to respiratory failure and eventual arrest is unfortunately far too common. The same applies to codes like A40 and A41, Sepsis (14,053), which is not even a diagnosis in itself but a syndrome describing the body’s systemic reaction to infection, and many of the “all other conditions” codes like R09.1, pleuritic chest pain and R09.0, hypoxemia.
But the most obvious example is J80, Adult Respiratory Distress Syndrome (21,899 cases). This is literallythe severe respiratory syndrome caused by COVID-19, yet people like Dr. Hesse who claim to have evaluated this data carefully did not include these deaths in their “real” COVID-19 death count. To be clear, if a patient’s death certificate listed only COVID-19 and ARDS, these medical misinformation hucksters wouldn’t count them; that patient died of ARDS, they would say, not COVID-19. It’s like saying someone didn’t die from falling off a plane without a parachute, they died from the landing. It’s the bad dad joke of medical misinformation and the clearest piece of evidence we have that those originating this narrative are either extremely unqualified to interpret this information… Or else are not in earnest with their conclusions, but instead are pushing misinformation intentionally from what motivations and purposes I cannot say.
Conditions that really do make COVID-19 more dangerous. Much of the work I have seen refuting the “6%” misinformation so far has focused on the concept of comorbid conditions or medical comorbidities. Simply stated, these are diseases or conditions that make us more susceptible to other disease processes or more likely to have complications from them. Some of these diseases are also extremely dangerous in themselves, and others are primarily dangerous because of their role in predisposing to other conditions. A good example of the former is Congestive Heart Failure (I50, 10,562 cases). This is an extremely dangerous, chronic disease that has a fairly low 5 year survivability from the date of diagnosis (average of 62%, but as low as 48%, in African American men because of healthcare disparities). You can absolutely die of complications from heart failure, but it also increases your risk for many other diseases and infections. It is both a primary cause of death and a comorbidity, and without a more detailed dataset or an intimate understanding of each case, we cannot possibly say how many of the 10,562 people who died with both COVID-19 and heart failure died from heart failure complicated by COVID-19, from COVID-19 which they were more vulnerable to because of heart failure, or from a more complex clinical picture that involved heart failure, COVID-19, and other contributing factors. But is this information going to change anything for us? The medical misinformation spreaders want you to believe that all 10,562 of the people who died with both heart failure and COVID-19 died at the time they would have from their heart failure with or without a viral pandemic. They want you to believe this based on nothing other than the fact that it fits a more comfortable narrative; but it flies in the face of what we are hearing from doctors, nurses, family members, and patients of those with heart failure about the way that COVID-19 affects those who are already suffering from these types of chronic illnesses.
Other examples in this category include renal failure (N17-N19, 13,693 cases), COPD and other chronic respiratory disease (J40-J47, 13,780 cases), and quite a few of the “other conditions and causes” listed, such as N04 (Nephrotic Syndrome), L93 (Systemic Lupus), and of course B20 (HIV), just to name a few. The people spreading this misinformation are putting the people with these illnesses at greater risk, specifically, by either pretending that COVID-19 is not a threat to them (the “only 6% count” crowd) or by seeming to claim, callously, that caution as a society isn’t warranted on their behalf (the “94% had comorbidities” crowd).
But within this category we also include diseases that are not likely to kill you on their own, and which would have almost certainly been included on the death certificate due to the physician’s conviction that they made the patient more susceptible and less able to resist the complications of their COVID-19 infection. These include Obesity (E65-E68, 5,614 cases), Alzheimer’s disease (5,608 cases), and of course other types of dementia (F01 and F03, 18,497 cases). Do we really believe that a patient with COVID-19 and obesity listed as their causes of death have died from obesity, and that their having COVID-19 was a coincidence? That is not something that happens. Dementia in particular is an interesting conundrum, because with COVID-19 harming so many people in nursing homes it is potentially not only a physical risk factor, which it most certainly is, but also an epidemiological risk factor; many doctors might include a patient’s reason for living in an assisted living facility, such as dementia or disability, within the death certificate as part of the narrative of how the patient came to be exposed to COVID-19, the same way we might list arthritis on the death certificate for a patient who suffered a heart attack during physical therapy. Again, these are not competing diagnoses that draw responsibility for the death away from COVID-19, but rather a fuller picture (that is, as full as can be told with diagnostic codes alone outside of the full medical record) of the patient’s story leading up to their death.
Finally, a few categories of disease deserve some extra discussion, and those are diseases that could cause death all on their own but almost certainly didn’t for the patients reflected in these death certificates. Hypertension (I10-I15, 35,272 cases) is incredibly common and usually leads to longterm organ damage rather than acute crises, but can present with severely elevated pressures that lead to stroke or another vascular event. However, this would typically be indicated with the diagnosis code I16, hypertensive crisis or I16.1, hypertensive emergency, which are specifically not included in the diagnostic codes for the hypertension group in this table. It is possible that this is just a common coding error on death certificates, but I doubt it; if the physician believed that the severity of the patient’s hypertensive crisis led directly to their death, they would likely take pains to emphasize this on the death certificate; applying a code for essential or secondary hypertension instead suggests that they regarded it as a comorbidity or at most a contributing factor. Diabetes (E10-E14, 25,936 case) is another example. Diabetic Ketoacidosis (DKA) is a severe metabolic disorder that often requires ICU level care; but this is primarily due to how labor intensive it is to treat, and the mortality rate remains low. These 25,936 people who had both COVID-19 and diabetes did not die from DKA, which accounts for less than 2,500 deaths annually. Instead, both diabetes and hypertension, just like dementia and obesity, are comorbid conditions that make the patient more susceptible to and likely to experience worse outcomes from other diseases, and as such their role in this list of additional diagnostic codes on COVID-19 death certificates is the same as their role in death certificates for patients who die from stroke, heart disease, and influenza; yet no-one is claiming that because a patient had high blood pressure and diabetes, their death from the flu didn’t count.
Conditions that might have nothing to do with COVID-19 and mighthaveactually caused the patient’s death(maybe) Finally, we have conditions that, based on the diagnosis code alone, we know to be incredibly dangerous and also to be common causes of death. Some of these, like certain cancers (C00-C97, 7,415 cases plus some of the ‘all other conditions’ group) we can treat similarly to heart failure or COPD; they may predispose you to COVID-19 or raise the risk that your COVID-19 course of illness will be severe, or they may be immediately dangerous in and of themselves and be worsened by COVID-19 or not. If someone wants to ask how many of the thousands of deaths that included a cancer diagnosis were actually caused or hastened by COVID-19, and how many just happened have the virus during the days leading up to to death from a terminal malignancy, I think it’s a fair enough question; though from what I’ve heard from friends who provide hospital and hospice care, the former does seem to be very common. In the latter cases, if such cases are at all common, the additional suffering from COVID-19 must be felt in other ways; in the barriers it places to those individuals being surrounded by family and friends as much as possible during their final days.
We could legitimately ask the same question for some other diagnoses on the list; heart attacks and cardiac arrhythmias (18,103 and 9,812 cases respectively), pulmonary embolism (I26, contained in the 8,743 “other disease of the circulatory system”), and strokes (I60-I69, 7,653 cases) are all very deadly on their own. However, unlike with cancer, which has no known or proposed causal relationship with COVID-19 aside from immunocompromise, the virus is known to cause a hypercoagulable state that has caused all of the above pathologies. How many of the deaths that involved these diagnostic codes were due to these conditions and how many were in turn due to COVID-19 is known only to the doctors, nurses, and family members that were involved in their care. Attempts to make absolute statements that these deaths simply were not caused by COVID-19 (despite the doctor writing the death certificate feeling they the virus did in fact contribute to the death) because another dangerous disease was also involved are based entirely on a desire to minimize the danger of the virus, and not on any interpretation or analysis that can be legitimately conducted from this set of data.
My friend, an ER Doc in New York
The final set of diagnostic codes we need to look at are the 5,133 included in COVID-19 death certificates under the category “Intentional and unintentional injury, poisoning and other events.” We don’t know which codes specifically show up in these death certificates, but much like the other ‘other’ catch-all categories it contains diagnoses ranging from S00.37XA, Other superficial bite of nose (a diagnosed I received today courtesy of my 16 month old), to X95.9, Assault by firearm. What is going on here? Much like the “other” diagnostic codes we talked about above, there may be any number of reasons that some of these codes might be on a COVID-19 death certificate. Some may be complications that arose in the hospital, such as SO6.9, Intracranial injury, when a COVID-19 patient experienced a syncopal episode and hit their head. Some may be part of a historical narrative, for instance a patient who experienced a prolonged hospitalization following a V03.10XA, Motor vehicle collision injuring a pedestrian, which ultimately ended when they died from respiratory failure due to COVID-19 contracted in the hospital. Again, without access to the actual death certificates, medical records, and medical staff who treated these patients we simply do not know what circumstances or patient history necessitated the physician to include both COVID-19 specific diagnostic codes and codes for accidents or intentional and accidental injuries in the same death certificate; but it absolutely does not stretch the bounds of credulity to believe that such circumstances do indeed occur.
Nevertheless, I want to cede this point to the conspiracy theorists, if only for just a moment. What if we do “admit” (as ridiculous as it is, and with apologies to the families of the individual people whom these death certificates represent) that each and everydeath certificate listing one or more of these accidental and non-accidental injuries represents a patient who died from some horrible accident, with COVID-19 just tacked on but clinically silent? You see, since the beginning of the pandemic the conspiracy theorists have been telling us, with no evidence, that “if somebody gets hit by a car they are calling it a COVID-19 death” and “if someone gets shot, they call it COVID-19 to inflate the numbers.” This data, from actual death certificates, now shows that the maximum possible number of such falsified death certificates tacking on COVID-19 to an accidental death is 5,133; compared to 183,000 deaths from COVID-19 and an estimated 80,000 total deaths from accidents in that same time frame. And again, that’s assuming that no other possible explanation exists for those “other accidental and non-accidental injuries” contributing to a person’s death from COVID-19.
Conclusion
Many of the diagnostic codes listed don’t fit easily into just one of the above categories, because we just don’t know enough about the history of the people whose battles with and deaths from COVID-19 are represented here. We don’t know, from this data set, whether the physician completing the death certificate was indicating a new stroke as a primary cause of death, or an stroke that lead to a rehab stay where the patient contracted COVID-19. We don’t know whether diabetes was listed because it was poorly controlled and played a major role in the hospitalization, or whether it was well controlled and was only included because that physician knew that diabetes is a risk factor for the patient’s unfortunate bad outcome from COVID-19 infection. We also have no idea what to do with codes that are so benign in themselves that they don’t really seem to have a place on a death certificate at all, yet the physician clearly regarded as an important part of the patient’s history leading up to their death.
But what we do know, with certainty, is that this new data released from the CDC does not mean. If you’ll spend just a few minutes really looking at the data, at the ages and the conditions mentioned, you will realized that it cannot mean that 94% of the people who have died from COVID-19 were incredibly sick, incredibly frail, and incredibly old people with many other diseases who would have died soon anyway; that argument is as bankrupt in its analysis of this data set as it is ugly in its callousness. That is not what the CDC means when they tell us that 94% of death certificates listed ‘more than one diagnostic code’ or contributing factor, as we’ve clearly demonstrated above. And even if it were (and it’s not), it would not somehow mean that the lives lost to COVID-19 were less valuable; those who see this false idea that 172,000 of the 183,000 people who have died from COVID-19 were sick already as a compelling reason to stop mitigation efforts need to carefully consider whether their only motivation for taking caution has been their ownpersonal health and safety this entire time… And then try to understand why that has not been the sole or primary motive for the rest of us; that the safety of those around us, including the medically vulnerable, is actually sufficient reason for some inconvenience and even sacrifice on my part.
And we also know with certainty that no real scientist, statistician, epidemiologist, or physician, and certainly no one who actually treats patients on their death beds and then completes death certificates to capture the complex and detailed medical events of their final days would ever believe the idea that the 6% of death certificates with only COVID-19 listed as a cause of death represents the “real” death told of this horrible virus; at least not without some herculean effort of intellectual dishonesty and self-deception.
I’ve promised at least a dozen people that I would write about this over the past month and have so far utterly failed them. The truth is that it’s such a huge topic, and so fraught with the risk of saying something too extreme and dogmatic, that it’s hard to even know where to start. In a way, being at least a month late to this topic is much, much more comfortable, because not only do we have much more data now, but I can write in the certain and comfortable knowledge that my essay will have no impact whatsoever on what we do about reopening schools (not that it would have anyway). My goal therefore, besides keeping out of trouble, is to provide whatever insight I can into whether or not it’s safe to reopen schools and then what you, dear reader, can do to mitigate the inherent risks within your own scope of influence. I don’t always lay out a thesis statement at the beginning of these essays, because despite what I learned in Freshman honors English, I usually don’t have one (sorry Mrs. Greer!); but today I want to address whether going back to school is going to worsen the pandemic, whether it is worth the risk, and what parents, educators, and we as a society can do to make this situation as safe as possible.
Is going back to school going to make the pandemic worse?
Answer: Yes, absolutely.
Did you want me to elaborate, or is that sufficient? The reality is that I can see no way that this isn’t going to make the pandemic worse. On some level this math is incredibly simple; more people in close quarters means more cases, and more cases means more deaths. The real question is how much worse will reopening schools make the pandemic, and as we discuss below, whether that risk is justified right now. This question is going to answer itself in a few months, maybe even within a few weeks; but right now the best we can do is guess.
When I first started writing about this issue, I wasn’t sure what conclusions I would draw (which is generally a good way to start, if you can do it). I actually expected to arrive at answers that were cautiously optimistic, but as I went through the current data I became more concerned. My goal in writing this was not to sound an alarm or argue a point but to evaluate the evidence, and if you find my conclusions somewhat more discouraging than you had hoped, please know you aren’t alone; I was discouraged too. We are going to look at three types of evidence; what the epidemiological and experimental data tells us about how children and adolescents spread the virus, what has already happened in other places that have reopened schools, and what the risk is to these populations, to educators, and to the family members of school aged children and adolescents.
Can children spread the virus? I’ve said before that for any discussion of whether or not children and adolescents can spread the SARS-CoV-2 virus, the burden of proof would be on the side of proving that they don’t, not proving that they do. We have decades- nay, millennia- of experience with and evidence of children spreading viral respiratory illnesses. I see it literally every day in my clinic and have experienced it within my own body when I have been laid up for days (I’m told this is called a “man-cold”) from a virus that one of my adorable walking fomites brought home from parents-day-out or Sunday School (or whatever your church calls it to avoid having to call it Sunday School). Under normal circumstances we take this very seriously; we cancel birthday parties when one of our kids has a fever and we regretfully reschedule plans with friends when a respiratory virus has affected our family, because we know that we could spread it to their family. In fact, this is such a truism that it is accepted conventional wisdom, and I regularly have parents tell me of a cold or the flu that their children got it from a cousin and are “just passing it around” within the home. Barring some compelling microbiological difference, there is no reason to assume that it would be any different for COVID-19. Without definitive evidence, I simply do not find claims that ‘children don’t spread the virus’ convincing. It is well and good for people like British Epidemiologist Mark Woolhouse to say that there have been ‘no recorded cases worldwide of a teacher catching the coronavirus from a pupil’ (‘pupil’ is a British word for ‘student’), but aside from the problem of seeming to claim categorical knowledge, saying this in July when schools had been closed since the early days of the pandemic in March paints the risk as being low with much more confidence than the evidence warrants. But epidemiology is an applied science, and what we get wrong in our models and assumptions, the virus will correct for us in the bodies of students and teachers.
Nevertheless, the evidence was initially encouraging. A review of available evidence published on July 31st in the journal of the American Academy of Pediatrics asserted that “children most frequently acquire COVID-19 from adults, rather than transmitting it to them,” while acknowledging that this is a significant divergence from transmission patterns in other viral respiratory illnesses such as influenza. The authors concluded, “On the basis of these data, SARS-CoV-2 transmission in schools may be less important in community transmission than initially feared.” This conclusion is based on a study from Switzerland that tracked cases in 39 households, and another in China that included 68 children with confirmed COVID-19.
The same month, a study from Korea that traced contacts of 5,706 individuals with COVID-19 found that the highest transmission rates were for the household contacts of school-aged children with the virus, and concluded that “rates were higher for contacts of children than adults.” Because we are talking about COVID-19, this claim might be considered controversial. If we were talking about literally any other respiratory virus, every parent I know would respond by saying, “well… yeah.”
This finding, from a much larger study, provides a more balanced context for the major enigma from the AAP article; a German experiment that showed that viral loads in the nasopharynx (nasopharynxes? nasophari?) of children were as high as those in older people, “raising concern that children could be as infectious as adults” (Update: this result has since been confirmed by a study at Massachusetts General Hospital released yesterday, August 19th, which actually found viral loads in children with COVID-19 that were higher than that of severely ill hospitalized adults). The AAP article offered a few possible explanations for why this did not line up with the reassuring findings from the small epidemiological studies they reviewed. First, because children are more frequently mildly symptomatic or asymptomatic, releasing fewer infectious respiratory particles during their illness compared to adults. Sure; but adults don’t generally pick their noses and then touch every single muffin before deciding which one they want for breakfast. Maybe with this disgusting example from my life this morning in mind, the AAP article added, “Another possibility is that because school closures occurred in most locations… most close contacts became limited to households, reducing opportunities for children to become infected in the community and present as index cases.” And if that is the analysis of the most optimistic academic article on reopening schools I’ve seen yet, what will be the conclusions of the epidemiological studies from 2 months from now?
Are we actually seeing COVID-19 cases transmitted by children? The second type of data reveals yet another benefit of pathologic procrastination, because if I had written this a month ago we wouldn’t have some of this data at all. A recent analysis showed a surge of nearly 100,000 new pediatric COVID-19 cases in the latter part of July, prompting Pediatric Infectious Diseases specialist Dr. Sean O’Leary of Children’s Hospital Colorado (where I did all of my pediatric rotations in med school) to say “I think it’s showing that, yes, kids can get infected and can spread the infection.” This trend continued this month, with 75,755 new cases from 7/30 to 8/13. To put this in context, that means that nearly half of US COVID-19 cases in children have been confirmed in the last 4 weeks. Still, while some school-related activities and sports camps were happening over this time frame, this was before most schools actually reopened; once they do, these numbers may end up looking small. In places where they have reopened, we have read about high schools, middles schools, and kindergartens shutting down, quarantining massive number of students, or further delaying reopening due to large numbers of exposures to the virus and increasing numbers of confirmed cases among students and staff. This is mirrored in other places where young people are together en masse. University of North Carolina at Chapel Hill has switched entirely to online classes (and now Notre Dame and Michigan State) for the semester due to multiple clusters of transmission on campus, and we have read reports throughout the Summer of camps closing due to massive outbreaks among campers and counselors.
More to the point, I see this all the time. I’ve evaluated hundreds of patients for COVID-19 over the past several months, and there has not been a strange, unexplained phenomenon of patients not getting sick from their kids. I know there are some people who will never believe in COVID-19 transmission in children from studies in Korea that demonstrate thousands of cases; so I’ll just tell you now, I’ve personally seen many people who got COVID-19 from their children. We’ve seen children stay with cousins who tested positive, and then bring the infection to the adults and other children in their own household. We’ve seen families of 5 or 6 all test positive for COVID-19 after one of the children developed symptoms first. I haven’t seen any teachers get COVID-19 from a student; but I don’t think any of our local schools are actually open at this point. But transmission from children is happening and has been happening, and as much as we all wish against it, there is simply no chance that we won’t see community transmission clustered around schools once they are reopened.
Yeah, but children aren’t at a high risk from COVID-19, right? The inevitable questions is, so what? Aren’t kids immune? Or if not immune, at least far less susceptible to COVID-19 than adults? To some degree, the answer is “yes, thank God.” If this were the Spanish Flu of 1918, which disproportionately killed children, our society would not even be dreaming about reopening schools. As a parent of four small children, the fact that children are relatively safe from the virus has been the main reason I have felt comfortable seeing large volumes of patients with COVID-19-like symptoms daily over the past several months. As we discussed in the article addressing the America’s Frontline Doctors video, and again when discussing misinformation around COVID-19 and Human Trafficking, we don’t actually know the exact mortality rate among children. We do know it is much lower than for other groups.
My 5 year old son is 64x less likely than me to die from COVID-19, and 12,364x less likely to throw out his shoulder playing catch.
We also know it is not zero. While 20 of the states included in the latest analysis by the CDC reported zero child deaths, the rest reported at least one, and the mortality rate was as high as 0.6% in confirmed cases. The state with this frighteningly high mortality rate? Texas. Now before we break out our calculators and start to panic at the realization of what a 0.6% case fatality rate in children means, this is definitely an outlier (and I believe drastically overestimates the actual infection fatality rate in children), and of course it only includes identifiable cases; this mortality rate still cannot account for asymptomatic cases or minimally symptomatic children who don’t get tested. Nevertheless, not-zero multiplied by a lot is still a lot, and there is reason to expect that the 400,000 child cases of COVID-19 in the US so far may soon be a drop in the bucket. Some of the children who become infected over the coming weeks and months as schools reopen will, in fact, die, and for many of us who are affected by these deaths, this pandemic will no longer seem to have miraculously ‘spared children’ the way it has over the past 6 months with schools closed and children mostly kept at home.
But more importantly, death rates do not tell the entire story. While we have seen few child deaths, we have seen many children hospitalized for COVID-19, and an analysis of hospitalizations published just last week reveals that out of all hospitalized children with COVID-19, about one-third require ICU level care (though require mechanical ventilation far less frequently than adults). There are many ways to explain and understand this data, some of which are included in their analysis and some of which aren’t; but their conclusion is 100% spot-on:
“Children are at risk for severe COVID-19. Public health authorities and clinicians should continue to track pediatric SARS-CoV-2 infections. Reinforcement of prevention efforts is essential in congregate settings that serve children, including childcare centers and schools.”
Dr. Lindsay Kim, et. al
Finally, at the risk of sounding like a broken record, we aren’t actually most worried about the kids. If you look back at the chart from the CDC above, the groups that we are worried about most are the ones who are 1,400 times, 3,500 times or 10,000 times more likely to die from COVID-19 infection than school age children; their older parents and grandparents. Without any conclusive evidence that children ‘can’t spread the virus’ and more than enough compelling data that they can, we have every reason to believe that the population at greatest risk from reopening schools will be the grandparents of school-age children, not to mention older parents, teachers, and educators. As a society, we are now in the impossible position of choosing whether our children will forego being educated, socialized, fed, and nurtured inside of schools or whether they will be exposed to a deadly virus (soon, two deadly viruses; flu season is coming) that they can bring home to vulnerable family members.
Is it worth the risk?
Answer: I have no idea.
Child abuse So we know that the COVID-19 pandemic is going to get worse when schools reopen, but we don’t know by how much; and the other side of the equation is the risks associated with not reopening schools, which go far deeper than a semester or two of stymied educational attainment and missing out on the various intracranial and orthopedic injuries associated with high school sports (yes, I was on the Quiz Bowl Team. How did you know?). Since the beginning of the pandemic and the early closing of schools, cancelling of Summer programs and camps for children, and other mitigation measures that meant keeping children within the confines of their homes and family circles, we have been talking about, writing about, and worried about the possibility of child abuse and neglect going up during this crisis, especially when combined with unemployment, increased stress and anxiety, and grief related to the pandemic. And while this has been written about extensively by child advocates and physicians (like myself) who are also very concerned about the very real threat of COVID-19, it has also been used, similar to the issue of human trafficking, by people whose only real goal has been to diminish the threat of the virus and fight against any and all mitigation efforts.
So let me be clear. There is something gross and disturbing about people who have done everything within their power to make the pandemic worse, from neglecting social distancing to spreading misinformation and fighting against mask wearing, now saying that it is the people with legitimate epidemiological concerns about reopening schools who don’t care about child abuse. If it weren’t for people like this, we would be in a position to reopen schools much, much more safely and mitigate both threats more effectively. I deal with child abuse and its ramifications every day of my life; peopledon’t get to use it to try to give their deliberate pattern of denialism and irresponsibility throughout this pandemic the moral high ground. Reopening schools in the middle of a pandemic is an incredibly complex and difficult decision; but we are in this position, at least partly, because of them.
Well, so much for not getting myself into trouble.
The question of child abuse during the pandemic is one that remains unanswered. We all intuitively feel the danger of having children at home more and not having teacher’s eyes on children, especially in the midst of all the other risk factors we mentioned above. We all know of cases where a teacher or other educator has been the key person to report an abusive or neglectful situation and allow social services to intervene; I have seen this happen myself. But the idea that keeping children home from school will lead to a drastic rise in missed child abuse cases may overestimate the efficacy of the systems we have in place to report and investigate child abuse under normal circumstances. An in-depth article from The Marshall Project provides a careful analysis of the dynamics of mandated reporting, and while I think this is still an essential function of teachers, articles like this one from Mother Jones that list the huge drop-off in reports of suspected child abuse following school closures in March may be engaging in sensationalism; the vast majority of calls are not found to represent confirmed child abuse or neglect, and saying that, for instance, Illinois officials “received 6,672 reports of abuse in the week before the governor’s order to close, and 3,675 in the week after” does not mean that 2,997 abused or neglected children were missed.
There’s a balance here; early detection is the key to protecting children in child abuse situations, and there have been some reports by ER physicians that while the numbers of children presenting for child abuse are going down, the cases they do see seem to involve more severe or extensive injuries. Intuitively, we may believe that this is because of school closures… But most of this pandemic has so far taken place during months when schools would have been closed anyway, and it seems every bit as likely that the worsened severity of these child abuse cases is due to the other pressures of the pandemic not related to schools, like stress and anxiety and economic hardships. As the article above points out, we saw similar increases in child abuse severity during the 2008 recession even without school closures. Moreover, the long-held belief that child abuse peaks at all times children are home from school – the Summer, Christmas break, etc- seems to be a myth, and we are left to conclude what we really should have known already about the causes of child abuse; that they are complex. Blaming school closures for child abuse ignores this complexity in favor of a narrative that only seems to make the decision to reopen schools easier.
Other risks to children due to school closures I have a friend who spent his entire Fall and Summer, before leaving a few weeks ago for Physician Assistant school, trying to get food to thousands of children who normally rely on school breakfasts and lunches for a substantial part of their weekly nutrition. I should note that he was working with an organization; he wasn’t just making tons of sandwiches and then driving around handing them out across Texas and Louisiana. Without people like Dustin and organizations like Texas Hunger Initiative, many of those children would have faced significant nutritional deficits throughout this pandemic, and many children across our country don’t have access to programs like this. Moreover, school is not just a center of learning; many essential services such as counseling, speech and physical therapy, and support for learning disabilities and learning disadvantages occur within school walls. Moreover, the families who have least need of these services and the least reliance on school lunches are also the families that are most likely to have educational books in the home, stable internet and redundant internet-capable devices that can be used for distance learning, and other privileges that allow them to engage with learning resources regardless of the status of in-person school. The real threat to education posed by the pandemic isn’t the risk of students missing a year of school across the board (what, are we trying to beat the Russians to the moon?), but the risk of perpetuating and amplifying educational disparities.
But to make things murkier still, those are also the same students that are themselves most likely to become seriously ill from COVID-19, and whose parents and grandparents are at the greatest risk from the pandemic, due to healthcare disparities that often cut along the same racial and socio-economic lines as educational disparities, due to the same historical, systemic injustices. I hope you didn’t come here for answers; it really feels like we are stuck between a rock and a hard place, and the only certainty is that the families and children in our society who are already the hardest pressed on all sides at baseline will suffer the most dire consequences from whatever decision we make. Trying to correct this and share our portion of the burden should be at the forefront of whatever policies or personal decisions we make going forward.
What can we do as parents?
Be responsible I hesitate to put this one first because I realize it might sound accusational. Please look at the section heading; ‘what can we do as parents’; please understand that I’m including myself in this category (since I am not an educator or a society) and preaching this mini sermon to myself as well. Nevertheless, this is not an admonishment but a plea, to all of us, to take this virus seriously. As a primary care physician who sees many children, I have some version of this conversation a few times a week:
Me: Good morning, tell me what brings you guys in today. Parent of child: The school called this morning and said he had a fever of 119. Me, panicky: Wait… 101.9? Parent of child: Right. Me, less panicky: Whew… Ok, so when did his symptoms start? Parent of child: He started with a cough 3 days ago and felt warm last night, but I didn’t have a thermometer. They checked him at school today and called me.
As a parent I’ve done this myself; not just misspoke and said the wrong temperature because I had been up with a fussy child all night, but also sent my child to daycare or school because I didn’t really believe they were sick and I was able to rationalize away their symptoms. I’ve received that phone call before; your 2 year old has a fever at parents-day-out, your 5 year old threw up at Vacation Bible School; come and get your child. And the thing is, out of anybody, I should really have known better. But some children have minor coughs and off days so often that under normal circumstances playing a game of chicken with the symptoms and letting the school or daycare be the ones to make the final call that they are really sick is understandable. Not justified, but understandable.
These are not normal circumstances.
As parents, now is the time to take those minor symptoms more seriously and call your PCP or bring your child to their doctor for milder symptoms than you might have otherwise; or even just to keep them home for a day and monitor their symptoms to see if they really do develop into something serious. This is especially important if your job provides sick days or personal days and you have HR policies and supervisors that don’t penalize you for actually using them, which is a privilege so many people simply don’t have. A certain percentage of those runny noses and mild coughs are going to be COVID-19; better my child stay at home and me call in sick, than him give it to a classmate whose parents’ only option when he becomes ill is to leave him with a grandmother already in poor health. As a community, we have to take the responsibility of protecting other people’s children, and families, as seriously as we do the responsibility of protecting are own; and the time to start that is right now.
Consider alternative schooling/home schooling/schooling at home Homeschooling has always involved a good deal of privilege. I say that as someone who homeschooled until 8th grade, whose wife was homeschooled through highschool, and who(se wife) currently homeschools our children. We did not grow up wealthy and my mother enjoys working (and started working again once we had graduated), but my parents made more sacrifices than I realized at the time to allow her to stay home and teach us, and I’m incredibly thankful for that. Most of the homeschooling families I know (and we know a lot) are not wealthy; keeping one parent at home to teach means financial hardships they wouldn’t have to bare otherwise. And the sacrifices aren’t just financial; my wife has left hobbies unpursued, books unread (and unwritten, if I could ever get her to write that series of children’s books), and a nursing career she loves temporarily on hold, all to teach our children at home.
But the fact that we canchoose to make those sacrifices in the first place represents an awful lot of privilege, and there are many, many families for whom homeschooling is just not a viable option. Under normal circumstances, homeschooling is a hard decision for us. We believe in the public school system, and we realize that keeping our children at home means our voices aren’t contributing to the PTA, advocating for issues at the local elementary school or before the school board, or supporting the teachers and students and families that our own children would be interacting with every day. We try to be involved in and advocate for our community in other ways, but there’s no denying that we are less effective in this by homeschooling. It also means that our children miss out on opportunities to show love and kindness to people outside of their family circle every day. Sure, I guess there’s a possibility that my 8 year old would be the Regina George of the local 3rd grade or my 5 year old would be the Flash Thompson of Kindergarten, but I have enough pride as a parent and faith in my kids that I think it more likely they’d be an influence for good than otherwise. I think it’s fairly certain that somewhere in town an 8 year old is deprived of a best friend because my daughter is doing school at home with us.
So far we still feel that that’s the best decision for our family, but it’s definitely an ongoing discussion each and every year. But right now, with COVID-19, the privileges inherent in schooling at home can actually be used on behalf of the other children and families, and the teachers, at the local schools that our children won’t be attending. Each child that can safely be kept at home and successfully educated this year through distance learning or homeschooling makes it that much easier for teachers to maintain social distancing in the classroom, that much safer for teachers and other school staff in terms of transmission risk, and that much less likely that other students will become infected and bring the virus home to parents and grandparents. This year, at least, homeschooling was an easy decision for us; and if you have the resources, financial and otherwise, to successfully school at home for a semester or a school year, this is definitely the year to give it some careful consideration.
What can you do as an educator?
I just want to say, at the outset of this section, that I think that asking teachers and school principals to do the work of epidemiologists and government health officials and keep children safe from the virus is pretty lame. I am sorry that you are in this position; I hear your stress. I taught high school physics and physical science (and theatre!) for 8 months after college, and realized it was not something I was good at and certainly not something I could do for the rest of my life; I admire anyone who does it, and particularly anyone who does it well. When I left teaching to go to med school, I knew on some level that I was signing up to be on the front lines of any global pandemic that might happen to come our way; but when you became a teacher, you weren’t. So even though this shouldn’t be your job, I’d like to share some advice for how you can help keep yourself and your students, and their families, safe. Being months late with this post, I’m certain that any educators who might read this are already far along in the planning and implementation of their COVID-19 response plan, and those who have reached out to me have shared incredible, creative ideas to keep themselves and their students safe that I never would have thought of.
Seek counsel A physician friend and residency classmate reached out to me in May when her child’s school asked her to give recommendations on reopening school safely. At the time we were operating under the assumption that the pandemic would be well in hand by the Fall, and that the biggest concern would be preventing a second surge. Clearly, this is no longer the case. Nevertheless, we brainstormed on the best and most practical ways to reduce transmission between students while interrupting their education as little as possible. We had ideas for reducing transmission during PE, music class, alternatives to all school assemblies, managing bathroom breaks and lunch and hallways during class changes. I briefly considered sharing a big list of ideas here, but the reality is that the changes that would help will be different for every school, every building and class schedule, and every situation. You know your school, I don’t; your ideas will be better than mine. And better still will be your ideas with the input of a physician or epidemiologist or other medical professional who has an intimate understanding of infection control and viral transmission and who takes the pandemic very seriously. Reach out to one in your community and ask them for help; they have a vested interested in keeping your school safe, even if they don’t have a child that attends there. Most would be honored to help with this work (and would be even more honored if you then actually followed their advice!). This works best as a two-way conversation; the medical professional is going to see opportunities for changing processes and physical spaces and creating a safer school that wouldn’t occur to someone without their education and experience; and you, the educator, are going to be in a position to tell them which of their ideas will work for your students and your classroom, and which need to be modified or scrapped. Then, when things have calmed down and we’ve finally got this virus under control, you can reach out again to seek their advice on deescalating the measures you’ve put into place and slowly returning to normal. And then later in the year when you need someone to speak to your students about going into healthcare at the next career day, guess who you are gonna call…
Get clever As I’ve worked on this post, I’ve heard from teachers whose schools have implemented some incredibly clever and ambitious ideas. I’ve been told about schools keeping kids in cohorts throughout their entire daily schedule, even organizing sports activities and lunch and recess around these small, consistent groups. I’ve heard of multi-grade classrooms to keep siblings, cousins, and neighbors together, limiting the network of contacts per child. I’ve heard of classroom modifications, curriculum changes, changes in sports schedules, and restructuring of school-wide events. I’ve also heard of schools that are doing next to nothing (besides enforcing stricter social media policies for teachers), and teachers who are scrambling to keep their own classrooms as safe as possible within a school that is essentially denying that any danger exists. I’ve even heard of teachers taking a break from teaching this year because they couldn’t see any way to keep themselves, aged parents, or at-risk household contacts safe while being in the classroom every day. As a society, there is no denying that we’ve failed these teachers.
The classroom or school-wide plan that protects children from getting and spreading SARS-CoV-2 better than any other plan in the country is probably not “just keep children 6 feet apart,” “put up plexiglass between desks,” “masks at all times,” or “check temperatures at the door,” though it almost certainly will include some of those components. No, the best plan has probably already been devised by some creative, well-informed, scientifically minded out-of-the-box thinker somewhere. With any luck, it has been listened to and implemented; but unfortunately, too often it will probably be ignored by decision makers for being too weird or wonky, too conceptually challenging, or too inconvenient to implement. But now is exactly the moment that we need those creative and wonky ideas, because the stakes are too high to just hope it goes away if we can just ignore it hard enough.
Can your track or cross country team set up a Fitbit team challenge instead of practicing together after school?
Can you use pegboard and cardboard and printouts (that you’ll have to buy yourself, I realize) mounted on the walls of your STEAM class to make an interactive workspace that keeps students facing toward the walls for most of the class period instead of toward the teacher or across a table toward each other?
Or better yet… Also, is this me? I pulled this image off of google, I don’t remember this at all, and I didn’t wear glasses at that age… But from this angle I feel like there’s still a good possibility that that’s me.
Can you recruit that pop culture savvy AV kid (this is an oxymoron; none of us AV kids are pop culture savvy) to create some awesome Cast of Hamilton style video mash-ups so that your Zoom band rehearsals are Youtube worthy instead of unmitigated disasters?
If this is your music class, I’d be willing to substitute.
Can you use your school’s external doorways and internal layout to create a continuous one-way circuit during classroom changes, like Sylvester McMonkey McBean’s star belly tattoo machine?
Bad social distancing there in the middle, but pretty good otherwise.
I don’t know. Some of those ideas are probably things you’re already doing, or that you’ve already thought of and abandoned because there was just no way to make it work at your school or in your class. That’s my point; decreasing transmission right now is going to mean sound epidemiology principles combined with creative teaching ideas and applied to your individual teaching situation. Even for those schools that are very well prepared already, we have to keep in mind that no battle plan survives first contact with the enemy; once schools do reopen, one size fits all solutions or rigid adherence to plans made over Zoom during the Summer are likely to mean insufficient protection and excessive interruption of learning if they aren’t reevaluated and readjusted. It’s a lot, I know; but all of us fighting to stop misinformation and promote mitigation efforts and health behaviors that would have slowed the virus have, so far, pretty much failed; so now it is apparently your problem to deal with. You need bold strokes because we’ve failed to convince more folks.
Advocate, advocate, advocate Me using my blog to tell educators to advocate for each other, their students, and their communities is like hospital administrators pulling doctors aside to tell us how to treat patients (oh wait, that happens literally every day); this is clearly something you are already doing and is, in fact, a major part of your job. Nevertheless, this is now a more important job than ever, because there are so many stake-holders when it comes to reopening schools and not all of them care about the health of your students or their families.
In a moment we are going to talk about what the rest of us can and should be doing to support you during this time. Please keep lending us your voices. I know it feels like society has decided to ignore the collective and individual voices of teachers (I’m a doctor who writes a blog on medical misinformation; trust me, I feel you), but without understanding what’s happening in your schools and classrooms the rest of us have no hope of advocating for you in the ways you need most. We want to help. If your school has enforced social media policies that don’t allow you to say when you are concerned about the safety of your colleagues or your students, find ways to get that information out there anyway. Be sources of good health information and fight misinformation in the classroom every day. One thing I’ve heard from teacher after teacher is that their students have been amazing; wearing masks at a high rate without grumbling or complaining, practicing good distancing in the classroom, and in general being the best of us in taking the pandemic seriously. That is going to fatigue over the next few months without your example and reinforcement, but you are in a much better position than any of the rest of us to help lead this generation in doing the tedious day-to-day epidemiology work that we, their forebears, have failed at.
What can we do as a society?
Fight the virus on every possible front. If I had written this post a month ago when I should have, I’m sure I’d be saying that the best plan to reopen schools safely would be to spend the next month doing everything in our power to decrease community transmission, and then only reopen schools once we knew it was as safe as we can reasonably expect (for a more epidemiology minded discussion of what that would look like, check out Waco Epidemiologist Emily Smith’s post on “Can we open schools safely?“). In fact, this is still what I think, and if I thought there was any chance of getting it to work, I would be strongly advocating for schools to delay reopening while mitigation efforts were redoubled. In cities like my own, where our testing positivity rates have been steadily declining over the past several weeks, this might not even take that long. But if we’ve learned anything through this pandemic it’s that we cannot rely on strategies that require small individual efforts but a large degree of buy-in. So here we are, with schools reopening in the midst of a pandemic, and bracing ourselves to see how much worse it will get as a result. But as one comedian said, I guess all the bad decisions we’ve made up to this point have made this a good one?
But even if school reopenings aren’t going to be delayed until a set community prevalence or test positivity rate is reached, we can still make every effort now to decrease transmission, especially with a few weeks still to go before all of our schools are opened. We need to be practicing good social (physical) distancing and mask wearing. We need to be participating in the work of informing our own contacts when we are diagnosed with COVID-19 since our public health sectors simply have not had the manpower to keep up. We need to practice diligence in our personal mitigation efforts, even though we are all incredibly fatigued from thinking about this virus and how it has affected our lives. As a society we claim that the safety of our children in schools is one of our highest priorities, and we take massive steps to protect them. Yes, I know there are some pretty obvious areas where we haven’t been taking common sense measures to keep kids safe in schools, but we do a pretty good job of slowing down to 20 MPH and putting down our cellphones when we drive through a school zone, and we make sure kids have those safety scissors that won’t actually cut anything just to reduce the chances of one of them losing a finger. Right now, the efforts you can make to reduce community transmission- social distancing, washing hands, getting tested if you are ill, and wearing a mask- are the efforts that will keep children, their teachers,and their families safe in the coming weeks.
What even is this?
Extend Trust We’ve talked a lot about the role of educators and parents in fighting the virus and keeping our schools safe, but the reality is that those groups are limited in the actions they can take, with freedom from judgement and repercussions, without buy-in and affirmation from the rest of us. It’s well and good to tell parents to keep their child home for a day when they think she might be getting sick, but this requires policy changes that refrain from punishing parents for taking such a responsible action and trusting them to occasionally know, without a doctors note, when their child is too sick to come to school. Yes, that trust will be taken advantage of by some families, nobody knows it better than me; but right now I have visits every single week where parents know their child just has a mild illness and shouldn’t be in school, but had to come to the doctor to get a note for school and work; in the eyes of the school and their employer, they are guilty of faking an illness until my note proves them innocent. In the midst of a viral pandemic is exactly the time to reevaluate the wisdom of such policies and return that trust back to parents; and then keep it that way, because even aside from COVID-19 this dynamic is already dangerous during every single flu season.
Also, let’s get rid of perfect attendance awards.
Lower Our Expectations
And the same is true for our expectations of our teachers and school administrators. Being a high school physics teacher was my first real grown up job, and being a doctor was my second. There are plenty of similarities between the two, but one of the most salient is the constant feeling of being asked to do increasingly more with an ever decreasing amount of time and resources. As a primary care doctor, this often means walking out of one patient room and into the next from 8:00 to 12:30 and then from 1:00 to 5:15, providing extensive evaluation, compassionate listening, diagnosis, treatment, and teaching to each patient within a 10-15 minute window, and being expected to complete the documentation and respond to phone messages and refill requests in the often non-existent minutes “between visits” (we often don’t have time to go to the bathroom or get a drink of water “between visits”). As a teacher, it meant trying to make it through more curriculum than could possibly be covered in a year, prepare students for standardized testing, regulate behavior in the classroom, navigate and manage the interpersonal dynamics and conflicts of 13 years old, and provide counseling and interpersonal support for young people in some of the most formative and challenging years of their lives. Oh, and submit grades, which is just… I think I’ve still got some ungraded quizzes in a manila folder somewhere, and I haven’t taught since 2009.
Add to all of that the expectation that teachers will now be fighting COVID-19 transmission on the front lines of the pandemic and, somehow, teaching both in-person and online classes simultaneously, and you’ll realize what a sick joke it is to say that any adjustments we make to our expectations would be “lowering” them. We are asking so much of our teachers, and this year we are asking even more; we need to be comfortable, as a society, with accepting that less can be expected in terms of our students’ educational progress between now and May 2021 compared to years past and years to come. Somehow, in all of these discussions about reopening schools, I’ve missed all of the articles calling for a hiatus on standardized testing (or at least eliminating punitive measures related to those test results), on colleges using alternative evaluation methods for graduating seniors, and on discussions of exactly what percentage of the standard curriculum we expect teachers to be able to cover this coming semester; 50%, or just 35%? Rather than lowering our expectations, what we would really be doing is finally valuing teachers’ time and acknowledging their efforts, and recognizing that since most teachers are already working at maximum capacity as-is, we have to be willing to let something go when we add something on. If we are saying that schools need to be reopened because it is necessary to keep kids safe, detect cases of domestic violence early, and keep children from regressing academically, we need to realize that those goals do not logically imply that we can also somehow expect teachers and students to maintain the same pace of academic attainment, and that that is no longer our primary goal in reopening schools.
Be ready to pump the brakes I think this is the biggest one, and it’s going to take an awful lot of honesty when we look at the epidemiology data that emerges over the coming weeks and months. As schools reopen around the country, we have to fight stronger than ever against misinformation. We will hear that any increase in cases is due to increased testing, even if it is mirrored by an increasing test positivity rate and hospitalizations. We will be told that the overall mortality rate is dropping and it “isn’t as dangerous as we were told,” because the virus is less dangerous for children than older adults, and seeing a decrease in the overall infection mortality rate is a natural artifact of an increasing number of cases in children and adolescents- even as teachers, school staff, and family members of students are hospitalized and die due to those exposures. As flu season approaches, we will be told every possible version of doctors lying to diminish the flu and inflate the pandemic or misattributing flu deaths to COVID-19 to hurt the economy or this or that politician, as though it mattered which preventable deadly respiratory virus your family member died from.
We have to be willing to cut through the noise and look carefully at the trends in cases in our community and ask continuously whether the risk is still justified today. It would be great if I were completely wrong, if cases continued to decrease even when schools start back in earnest; but it’s hard to imagine that happening, and the decisions are likely to get even more difficult, not less, from here on out. We need to drop our agendas and our egos and our politically motivated methods of interpreting data and meet the emerging information with intellectual honesty. We need to consider school closures and audibles and readjustments as the necessary and humble work that the pandemic requires of us, and work together to keep our kids, our teachers, and our communities safe.
Trigger warning for human trafficking, rape and sexual assault, sexual abuse of children, and exploitation.
The big question we didn’t address yesterday (well, two days ago now) is whether the people making these comparisons between COVID-19 and cancer or diabetes are doing so because they truly care about those medical problems, like the nurses and doctors who treat them and the patients and their family members who are affected by them every day do, or just because they happen to find them convenient comparisons for minimizing or dismissing concerns about the pandemic. And while using a lifelong illness that causes real suffering like stroke or cancer for rhetorical purposes is a bit calloused, I can’t say I find it truly morally repugnant the way I do when the same thing is done, if indeed it has been done, with human trafficking and modern day slavery. Recently, I have started seeing a few different memes/images shared on social media making just such a comparison; but I believe they have very different degrees of merit and, I’m afraid, might be coming from very different places in terms of degree of actual sincere concern about the very real problem of modern day slavery.
Human trafficking is a truly evil industry. Some of the people who have shared these memes have quoted conservative estimates of 25 million slaves worldwide today; I believe the ILO estimates that are closer to 40.3 million, though even that was back in 2016 and the number is likely to be even higher now. This includes 5 million people, 99% of whom are women and girls, who are victims of sex trafficking and forced sexual exploitation. In addition to being robbed of their freedom and dignity, the men and women affected by modern day slavery suffer extensive medical and psychological problems that can last a lifetime, and many are subjected to nearly constant physical, sexual, and psychological violence, torture, and dehumanization. It is one of the worst offenses against human beings occurring today, and its cost in human lives and suffering is incalculable. In one sense, there can be nocomparison between human trafficking and COVID-19, because even the suffering from a respiratory virus that claims your life would be preferable to most of us compared to what is endured by victims of modern day slavery.
I first heard about modern day slavery from my friend Michelle Palmer, co-founder of the blog Tuesday Justice, back in 2008, my first year of medical school. That next year we became involved in grassroots organizations in Denver involved in raising awareness about human trafficking and modern slavery both in the United States and internationally. In medical school I hosted film screenings, attended academic conferences on human trafficking and training with the FBI and GEMS on commercial sexual exploitation of children (CSEC), and once even sat next to the author of The Vagina Monologues on a committee focused on professional collaboration to fight human trafficking in the city and state. When we moved to Waco I got involved with Unbound and eventually became one of their medical professional trainers. Over the last few years myself and one of my clinic partners have trained hundreds of physicians, nurses, other healthcare professionals, and Texas medical students to use their calling in medicine to recognize the signs of human trafficking and help address the unique medical and support needs of survivors, in addition to treating survivors of human trafficking and modern day slavery in our own clinic.
Last week, that partner and I both spent a significant number of hours in full PPE, in the 90-100 degree heat, evaluating, testing, and counseling patients for COVID-19. In 2 weeks, I’m going to lead a group of family medicine residents in a discussion of human trafficking cases; I will be working in the COVID-19 clinic that morning and that afternoon. I recognize that all of this sounds dangerously akin to self promotion, but the reality is that given my privileged position as a doctor and the scope of the problem, I feel that I’ve personally done very little towards combating either COVID-19 over the past 7 months or human trafficking over the past decade. That’s not my point. My point is that there is not a competition of awareness, focus, advocacy, or effort between the fights against these two assaults on our fellow Image-Bearers of God. The people who are fighting human trafficking are often the very same people fighting COVID-19.
And I humbly submit that memes which suggest otherwise may, in fact, be made by people who care about neither.
The Bad
I wanted to start with this one because I believe it’s somewhere in the middle in terms of both dismissiveness about COVID-19 and creating a false opposition between COVID-19 and Human Trafficking advocacy. The meme makes two claims; first a statistics claim about the relative risk of human trafficking and COVID-19, and the second a claim about the increased danger to children posed by masks because it perpetuates trafficking. Let’s look at both.
Though the numbers don’t usually matter much in posts like this one, I always like to know where they come from if possible. I went to the original source, an Instagram user who, apparently, works to promote “vaccine education, toxin free living, and government corruption.” I love it when people have eclectic interests.
At least she’s upfront about it.
Unfortunately, she doesn’t list where her numbers come from or how she ended up with this ratio of 66,667 children sold to human traffickers for every one child that dies of COVID-19, and I’m going to admit that it seems a bit high even to me, someone who leans towards more liberal estimates of human trafficking. The biggest problem with her numbers is that nobody actually knows how many children and adults are bought, sold, and enslaved through human trafficking each year; it’s an illegal, hidden, underground industry and the best we can do is estimate. It’s also very easy to misunderstand what the numbers actually mean; for instance, when experts say that an estimated 200,000-300,000 minors in the US are victimized through commercial sex trafficking each year, this is based on a much smaller number of actual reports, data from homeless youth and runaways, the personal narratives of adult sex workers who entered the life as children or adolescents, internet ads through websites like craigslist and backpage, and a variety of other data sources. Unfortunately, the vast majority of children who are being exploited in this way are not known. If we used this estimate (300,000) of US CSEC victims, divided by her 66,667, it would give us just 5 children in the US to die of COVID-19; since this is nowhere close, this clearly cannot be the figure she is referring to.
The experts I trust estimate that there are about 10million child victims of human trafficking in the world today ( this number does not include the tens of millions of child brides across the globe, nor young or old adults who have been enslaved ever since they were children), and I think this must be the number of she is thinking of; nothing else even gets us close. Working backwards, this would give us an estimate of 150children (10 million/66,667) who have died from COVID-19 worldwide. This is probably closer to the number of children in the US that have died from the virus; the best estimates that I can put together would put that number at around 100 (it’s tricky since the best data sources I can find don’t distinguish specific ages within the 15-24 yo age group; I don’t know how many from that age group were older adolescents and how many were actually young adults). We could look at this data from every possible angle (I typed a whole other paragraph on hypothetical calculations and assumptions we could make here, but deleted it; it doesn’t add to the discussion), but ultimately we are going to come out with an estimate that is certainly more than 150 but somewhere less than 1,000 child and adolescents deaths from COVID-19 infection worldwide.
So the best guess we can make is that the original author of this meme is comparing the total number of child slaves worldwide to some estimate she has found of the total number of child COVID-19 deaths that is, at least, on the right order of magnitude. There are at least five big problems with this “calculation” of a child being 66,667 times more likely to be sold to traffickers than to die of COVID-19.
First, the 10 million figure is an estimate of current child slaves, not new child trafficking victims; the idea of ‘being sold by traffickers’ paints the situations of enslaved people around the world as a monolith and ignores the debt bondage enslaving millions of families (which is still strongly associated with physical, psychological, and sexual abuse), which is by far the most common scenario for a child slave today. It also glosses over the many forms of control and exploitation included in human trafficking that don’t involve ‘being sold to a trafficker’, which we’ll talk more about in the next section. Sensationalist language hearkening back to ‘Taken’ is not at all helpful in understanding the scope of human trafficking and modern slavery. Second, it’s very much an apples to oranges comparison since the 10 million estimate is a cumulative total built up over many years, and the number of children dying from COVID-19 is a total from just a few months of a pandemic; it is a comparison of prevalence to incidence, two very different epidemiological concepts. The total number of children trapped in slavery and the total number of childrensold into slaverysince February are clearly not synonymous, but the author of this meme has treated them as the same thing; this renders her figure, 66,667 to 1, utterly meaningless, since she isn’t even comparing the things she claims she is, let alone statistics that have a logical basis for comparison. Third, this really is a straw-man. The discussion of whether or not to re-open schools is important, and the conversations I have every day with parents concerned about the risk of their children being harmed by COVID-19 are addressing very real anxiety. We talked about this with last week’s America’s Frontline Doctors video and will be trying to address it more fully in the coming week. But epidemiologists and physicians have at nopoint argued that COVID-19 was now the greatest threat to children worldwide; in fact we’ve come home from each and every shift incrediblythankful that this isn’t like the Spanish Flu pandemic of 1918, when children were disproportionately affected and killed by the virus. If it were, I’d probably be living in a tent behind our fence instead just changing on the patio and dodging my children on the way to a shower as soon as I come home. Nobody is saying that children dying from COVID-19 is the heart of the pandemic, and memes like this that want to put the number of child COVID-19 deaths ‘in perspective’ are ignoring the fact that child deaths have not been the main motivator for any of our mitigation efforts. Fourth, and most importantly, the comparison doesn’t matter. Saying that one thing is terrible and dangerous and needs to be fought against doesn’t mean other problems aren’t important. Anyone can do this trick with any two terrible problems. You can say that human trafficking isn’t important because a child is 15 times more likely to be a victim of child abuse within the their own home, or that childhood cancer doesn’t matter because children are 6 times more likely to die from accidents. Just because two things are deadly doesn’t necessitate a comparison of their badness; we can be against both. The cynical side of me says that the only reason to use human trafficking, unless you are really trying to raise awareness about it, is because advocacy for victims of human trafficking confers an immediate moral high ground, and for some reason that is something that COVID-19 deniers feel they must have. They find human trafficking convenient because it paints them as compassionate and ethical and those fighting or concerned about COVID-19 as though they were ignoring this huge human trafficking problem. We wouldn’t expect them to set-up COVID-19 against something more morally benign that harms children, for instance swimming pools or hurricanes. I’d like you to stop and think about that for a moment; think about the fact that some people have decided that their personal crusade against COVID-19 justifies using human trafficking to score rhetorical points; that they have chosen to exploitthe plight of human trafficking victims, some of the most exploited people in the history of the world, for their own ends.
But I’ve been wrong before.
Fifth, though it’s not as direct a correlation as with heart disease and immunocompromising conditions like cancer, there is a potential synergy between human trafficking and COVID-19, and it has nothing to do with masks. COVID-19 has, mercifully, killed relatively very few children, but it has left some children without one or both parents, and many more without one or more grandparents; adults who, when they are safe people themselves, confer the safety, security, and support networks that are protective against human trafficking. Despite our fears as parents (I am writing this sitting across from my 8 year old who is working on her math homework) (check that; supposed to be working on her math homework), most children who are victimized through human trafficking are not ‘taken’ from their front yards or from a big crowded event; they are preyed upon by traffickers who look for social vulnerabilities; want of support, care, and love; and circumstances where children and adolescents can be controlled. The logical conclusion of any of the memes or videos or posts that call us to lessen our focus on COVID-19 prevention, regardless of motive, is more deaths from COVID-19 among adults and elders- that is, parents and grandparents- and thus more children at risk for human trafficking in the years to come.
I also said that we would talk about the claim that having children wear masks makes them easier targets for human traffickers. Besides having, as far as I know, no verification for this claim, it also relies on sensationalized concepts of human trafficking and ‘oh that makes sense’ thinking; you are supposed to envision a child being walked along the street by human traffickers with family or friends passing within a few feet and not recognizing them because they are wearing a mask. This ignores the reality of trafficking victims’ experiences and the real methods of control used by traffickers; a problem it shares, though far less gratuitously, with the memes we will look at next.
The Ugly
As bad as it is to essentially make up statistics, and as bad as it is to artificially pit against each other two things that harm children as though you had to choose between them, and as though being vocally against one meant you were in support of or deaf to the other (“You are against a fake virus, while I am against human trafficking”), there is an even more exploitative type of meme going around the internet that takes these same goals and cranks the appeal to visceral emotion up to 11. After careful consideration I have decided not to share these images on my blog; I am sharing heavily redacted versions below, trusting you will recognize the type of macro I am talking about here.
“Let’s spend 4 paragraphs figuring out where that statistic came from” said no one ever
For those of you who have been mercifully spared from seeing the originals of these macros, or the many others circulating right now, they typically show one of three types of images in paired with text minimizing COVID-19 or juxtaposing it to human trafficking; a young child with tears in their eyes and a large hand over their mouth, a terrified child with a shadowy figure standing behind them, or a small girl bound with ropes, often in a basement or darkened room. For those who have seen and shared these images, I want to ask you to do something; go delete them (or change privacy settings; you can choose whether or not to delete them in a few paragraphs) before we move forward.
These images are deeply troubling and problematic for so many reasons that its actually hard to know where to start. “Minor” issues first, as we build towards the very worst and most troubling aspects of these images.
Bad statistics/misinformation: Trying to get people to accept false numbers or misleading statistics by appealing to emotion rather than logic is a common propaganda tactic and we don’t need it in the fight against human trafficking. The problem is big enough on its own without hyperinflating the scope of it. We talked about the ‘66,667x more likely’ above, but the other number we commonly see is 800,000; 800,000 children are reported missing each year, and the implication is that they become victims of human trafficking. The reality is that most children being trafficked in sex slavery are not reported missing because they are being trafficked by family members or are in vulnerable situations where they would not be considered ‘missing’. Most child sex trafficking victims have not been kidnapped. Moreover, that 800,000 represents mostly missing children who were found very quickly; this is the number from a 2002 study for all children who were reported missing, and includes children who have runaway or gotten lost and family abductions during custody disputes; only 115 of these were what we think of as ‘kidnapping’. Missing children, family and non-family abductions, and all forms of child abuse are serious and important issues, and they all intersect with human trafficking and CSEC to some degree; but using statistics from one problem interchangeably with that of another, or using the most dramatic possible number you can find without careful explanation or honest reflection is not helpful.
Implying silence/neglect of human trafficking issues: Comment accompanying the second image above reads “time to change the conversation.” This can be taken one of two ways; either ‘it’s time to start talking about human trafficking’, or ‘it’s time to stop talking about COVID-19′. I suggest the real goal of this meme is the latter, because unless you’ve been living under a rock for the past 10 years, we have been talking about human trafficking. To quote a friend who has a degree in modern slavery studies and has worked in this field, even if there are often problems with the organizations that only work to raise awareness of human trafficking without offering other support services or or contributing to the work in other more tangible ways, “they have at least done a good job at that.” Whenever I give lectures on human trafficking and modern day slavery, I always begin the same way; by asking for a show of hands of how many people have heard of this problem before and feel they know something about it. There has been a substantial difference in the response to that question over the past decade. One of the great things about volunteering in this field is that it is one of the few issues where people from all walks of life and ends of the political spectrum find a lot of common ground; we all agree that human trafficking is wrong. Some of us believe that pornography is a major contributing factor (more on that later), while others don’t. Some believe that legalizing prostitution is an important step in fighting it, while others don’t. Some believe that essentially all efforts to confront human trafficking should be secular while others believe that the Church has an important role to play. But despite these differences, there is more common ground to be had here than in the fight against almost any other societal ill. And that has made for fertile ground for grassroots awareness work; telling someone about human trafficking isn’t likely to start a debate or argument. 12 years ago we made shirts that said “slavery still exists” and “27 million slaves: ask me more.” Today the awareness focus has shifted to trying to help people understand modern slavery better and, often, combatting the sensationalist and misleading stereotypes that still persist. COVID-19 has not diminished the conversation around human trafficking, and images like these set it back rather than advancing it.
There is one extremely important point that needs to be made in this section, and I think here is the place to make it. Maybe you are new to human traffickingadvocacy; maybe a meme like this is the first you’ve heard of it, and you naturally felt compelled to share. And if that’s the case I want to say two things. First, is that when we are talking about why these memes are problematic and my belief that some of them were made with bad intent, I by no means mean that I believe the people who have shared them have bad motives in doing so; I know for a fact that hasn’t been the case with the people who I’ve seen share the images above. I remember the sense of urgency I felt the first time I heard about children being used as soldiers by the LRA in Uganda; I rushed to my dorm and turned off the Halo game my roommates were playing to try to force them to watch the documentary (it didn’t go well) because I couldn’t believe no one was talking about this. If you are just learning about human trafficking and modern day slavery now, it probably feels the same, and the idea that some awareness efforts aren’t helpful because the images they show or the numbers they quote aren’t quite right must seem a bit strange or overly particular. My goal here is to help you understand why they are problematic, as someone who has been where you are but has since been learning about this for years, and to help you find better resources for raising awareness, like the ones I am sharing in this blog post. And the second thing I want to say is welcome, we are glad you are here; the fight against human trafficking needs you. And the first thing we need from you is to learn more, which is work that none of us can ever actually move on from. I recommend you start with Tuesday Justice’s Primer on Modern Slavery, and then read Kevin Bale’s Disposable People.
Racist overtones: One of the recurrent visual themes we’ve seen throughout these social media images is the presence of both a child victim and an adult abuser, and the contrast between them. The child is small, the adult large. The child is terrified, the adult commanding and ominous. And often, the child is light skinned, the adult dark skinned. I don’t have exhaustive knowledge of the human trafficking memes that have been shared recently and can’t tell you what percentage of the time this is the dynamic presented. I also can’t tell you if this is done with lighting effects or if the photographer actually recruited white children and POC men for these photoshoots, or which of those options would make it worse; frankly the idea that children were asked to pose for these photos in the first place is troubling enough. But I don’t think these choices are accidental. The history of characterizing black men as hypersexual beasts and violent rapists in order to play into white majority fears of their children and young women being abused stretches back hundreds of years to the very beginning of our nation, and it has been a common theme in lynchings throughout American history. Malcolm Foley, Baylor University Special Advisor to the President for Equity and Campus Engagement and expert on the Church’s response to lynching in America, and my pastor, spoke about this briefly in his interview with Christianity Today following the death of Ahmaud Arbery. He in turn recommends you read Southern Horrors by Ida B. Wells, which addresses this topic in great detail.
“There is hardly a town in the South which has not an instance of the kind which is well known, and hence the assertion is reiterated that ‘nobody in the South believes the old thread bare lie that negro men rape white women.’ Hence there is a growing demand among Afro-Americans that the guilt or innocence of parties accused of rape be fully established. They know the men of the section of the country who refuse this are not so desirous of punishing rapists as they pretend. The utterances of the leading white men show that with them it is not the crime but the class. Bishop Fitzgerald has become an apologist for lynchers of the rapists of white women only. Governor Tillman, of South Carolina, in the month of June, standing under the tree in Barnwell, S.C., on which eight Afro-Americans were hung last year, declared that he would lead a mob to lynch a negro who raped a white woman. So say the pulpits, officials and newspapers of the South. But when the victim is a colored woman it is different.”
Ida B. Wells, Southern Horrors
If playing into sensationalism and parental fears has little to no place in the fight against human trafficking, there is even less justification for drawing on deeply rooted generational racism. By portraying abusers as men of color and victims as predominantly white children, these images are trying to recruit some of the ugliest and most harmful racist ideas buried in the heart of our society in order to fight human trafficking; but the fight against human trafficking doesn’t want or need those racist stereotypes. Moreover, these images are portraying a scenario that is not representative at all of the reality of race within human trafficking, a crime that disproportionately affects children of color, and reinforces stereotypes that themselves go hand-in-hand with racially motivated sexual abuse of trafficking victims. I hope you’ll read the article I’ve just linked from Love 146; it’s very short and shares the stories of three survivors whose race was a selling point their traffickers used to advertise them for sexual exploitation; please take a minute and read their words.
Misrepresenting human trafficking victims: These images are also damaging and potentially dangerous because they so deeply misrepresent the real situations of victims of human trafficking. Though chains, ropes, cages and locked doors have been used to hold child and adult victims of human trafficking, they are not the most common methods. The techniques that traffickers use to control their victims are varied and sophisticated. Traffickers use shame, fear, and physical closeness in perverse combinations to make victims feel that they are the only person in the world that can be relied on or trusted. Many times they are family members or parents of the child being exploited, and use that relationship to maintain control. Other times they move victims to another city and strip them of their phones, ID’s, and social support networks to make the world outside the trafficker’s control feel even more dangerous and foreign. They use drug addiction, financial entrapment, and poor living conditions to create absolute dependence on the trafficker as a provider. They use psychological torture and manipulation to instill in their victims a sense that they are omniscient and omnipotent; they know everyone, they have contacts with the police, there is nowhere that the trafficking victim can run where they won’t find them. They use threats of violence credible and not; if you leave, I’ll kill your family, I’ll recruit your sister into the life in your place. They forge trauma bonds that make recidivism incredibly high and prosecution against traffickers extremely difficult. These methods, and many we haven’t touched on at all, make chains, ropes, cages, and locked doors unnecessary for controlling victims.
So why does it matter if these images paint a misleading picture of how victims of human trafficking are controlled and exploited? First, because it makes it more difficult for people to notice and report human trafficking when it occurs, something these memes claim to want to promote, if they are only ever looking for physical signs of restraint and enslavement. The work of grassroots advocacy and awareness organizations involves dispelling these myths so that people can really begin to understand the complex, nuanced, and insidious forms of control that are used, and learn to spot them in their interactions with victims of trafficking. When we train medical personnel to detect trafficking, we talk about the presence of a controller, sexualized language and patient narratives that normalize sexual abuse and violence, asking judgement free questions, and understanding the adverse medical findings associated with trafficking; looking for a cage or a rope is going to miss most cases of human trafficking, and all of the cases that could be detected in a medical setting. And second, because the misconception of trafficking control methods being limited to only physical forms of restraint like the ones in these images contributes to shame and victim blaming towards survivors. When we promote the idea that all trafficking victims and modern slaves are bound by ropes or chains, we are also stating the contrapositive; if you aren’t bound by ropes or chains, you aren’t really a trafficking victim. Adolescents are arrested for “prostitution,” a crime that can’t logically exist (children cannot consent to sex; “child prostitution” is always rape), and are frequently further victimized by law enforcement. They are rejected by families and loved ones because their serial victimization and the control methods they have suffered are seen as evidence of poor moral character. Society asks incredulously, “why didn’t you just leave?”, and we tell ourselves narratives that “I would have run away if it had happened to me,” without ever trying to understand what they had to endure. It even contributes to trafficking victims’ difficulty in recognizing their own abuse, because they may believe the cultural narratives that the incomprehensible torment they have endured as serial victims of rape and psychological torture don’t count unless they were handcuffed, caged, or tied-up at all times.
Sensationalizing the sexual abuse of children: This is the hardest one to write about, and also the reason this post is now over 24 hours late. In my opinion it’s the biggest problem with the images above. Recently the Texas Medical Board began requiring that all licensed physicians complete training in human trafficking, and the Department of State Health Services (DSHS) released standards that those trainings should adhere to. Though the training we conduct had only one major revision because of this, we used it as an opportunity to update the entire presentation and ensure it was something that protected the dignity of human trafficking victims and survivors to the highest degree possible. The one revision; removing an image of two teenage girls standing on a street corner at night. And the reason we removed that image was because of this new training standard:
I mean, it’s the first one!
I’m including this training standard because I want you to understand that my objection to these memes and my request that you take them down if you’ve shared them, and kindly call them out when you see others sharing them, isn’t based on personal distaste or a negative visceral reaction (which is exactly the type of reaction they are meant to provoke). These are agreed upon standards and the idea of these images being harmful is accepted among those who fight against human trafficking every day; it’s just hard to articulate exactly why. We call these types of images sensationalized because we can’t quite call them sexualized; there is nothing sexual about a child experiencing fear and torment. Yet the image is meant to arouse disgust because we know that, to traffickers and johns and others who sexually assault children and adolescents, these are sexual images; in fact, I think you could rightly call them pornography. These images of children with adult hands covering their mouths, or bound and terrified with dark figures standing behind them, clearly send the message, “This child is about to be sexually assaulted.” I don’t know of anything that has less place in the fight against human trafficking than images that, if seen by one of the millions of men and women who have survived sexual assault or the ordeals of abuse through modern day slavery, would potentially traumatize them further and bring to mind those violations. These images are exploitive; they take the worst, most hopeless and fear-filled moments of the lives of real people and reproduce them for use as promotional materials. The fact that what the creators hope to promote is awareness is a mitigating factor, certainly; if these images were used for literally any other purpose we would chase the people creating these memes out of town, society, and history; we would call the FBI on them and put them on social media blast. But the endsdo not justify the means, and we do not need simulated pornographic images depicting the moments before a rape or the psychological suffering of a child to convince people that this is an important issue. We need survivors’ stories. We need to understand the factors that contributed to their targeting, their control, and eventually to their empowerment and escape. We need to help young men and adult men understand that “non-consensual sex” is always rape and that desire for sexual interaction with the helpless and those who cannot consent is a serious mental health condition that needs immediate treatment, not a fetish or kink that can be safely indulged in as long as the victims are far enough away. We need to understand the complex networks of organized and non-organized elements that make up the human trafficking industry. We need to fight human trafficking by uniting across political and religious lines against the exploitation of children and the sexualization of innocence, not by dabbling init as these memes do.
The Good
I think it’s important to note that not all memes that compare and contrast human trafficking to COVID-19 are necessarily problematic. The meme above is clearly different, while though it is using COVID-19 to grab your attention it is not trying to diminish the seriousness or reality of the pandemic. Further, it links to the Polaris Project, a reliable source of human trafficking information and resources, which also operates the National Human Trafficking Hotline, a free resource that anyone can call if they themselves need help or support or to report or ask advice about a potential human trafficking situation. Some of the verbiage, like “I wonder if … people would start paying attention?”, isn’t what I would choose and maybe falls under the idea of treating human trafficking like a neglected topic, which we talked about earlier… But this is very minor and may just be an issue of generational differences in meme tone and vocabulary.
This meme also shares data instead of sensationalized images and false statistics, and doesn’t try to play on fears, racist stereotypes, or false narratives about human trafficking. Finally, it comes from a source that is beyond question focused on helping women rather than minimizing COVID-19 concerns; the Montgomery County Women’s Center in Conroe, Texas, which provides sexual assault support services including legal support, crisis intervention, counseling, and advocacy. A quick search of their social media shows that they have indeed taken COVID-19 seriously and have modified their delivery of services and planned programming to keep their staff and clients safe from the virus; once again showing that any dichotomy between caring about COVID-19 and caring about victims of sexual violence is a false one.
How COVID-19 is like Human Trafficking and Modern Day Slavery
I know that by this point the title of this post, “Please keep comparing COVID-19 to Human Trafficking,” must feel like sarcasm or a particularly flimsy misdirect; but I promise you I really mean it. For me personally there are lots of similarities, not the least of which are the real harm and destruction I have seen them both bring to the lives of human beings created in the image of God, and the work I have accepted of helping provide accurate information to replace the misunderstandings about them that lead to deep seated fears. But there are a few other ways I think the comparison between these twopandemics is actually apt, if made responsibly:
There is lots of misinformation out there. I would hope this post is proof enough that there is misinformation on both human trafficking and COVID-19 circulating widely. I said before that the role of grassroots awareness efforts on human trafficking has shifted from telling people that slavery still exists to helping people understand what modern day slavery is really like. This is invaluable work that is done best when informed and led by survivors or human trafficking, helping those of us in support sectors and the public in general understand the nuanced and complex nature of their experiences. Just like we try to do on this blog with COVID-19 videos and other medical misinformation, organizations like Unbound, Polaris Project, and Free the Slaves carefully break down the myths, popular stereotypes, and outright lies surrounding human trafficking and then tell the real stories of survivors and victims and the real story of human trafficking and modern day slavery. This aids in awareness, victim recognition, survivor support, laws that support survivors, and a culture that treats human trafficking victims as survivors instead of criminals. Without accurate, reliable data, this work is surrounded by a fog of biases and assumptions that inhibits the work of aiding survivors; we need to tell honest stories about human trafficking because when we share trafficking misinformation, it helps the traffickers instead.
You can make both problems worse without realizing it. We’ve talked before about the danger of asymptomatic transmission of COVID-19, and studies which have shown (though the results are open to some interpretation) that the 48 hours prior to the onset of symptoms might actually be the most contagious period of time during an infection. As someone who has done pretty good but not perfect at social distancing throughout the pandemic, I find this especially concerning; all of us need to fight the false sense of security that comes with feeling healthy at the moment, thinking about our potential exposures and at-risk contacts even when we don’t think we are sick. That’s different from living in fear; living with a healthy respect for what this virus can do to us or our loved ones is wise, not fearful. But in addition to spreading this virus directly, we can make the pandemic worse with our other actions; sharing misinformation on the internet, failing to vet our sources when we share new or emerging information, supporting policies or politicians that minimize the very real danger of the virus, and fighting against non-nefarious common-well-being policies like wearing masks in public spaces. All of this increases the risks from the virus in much more subtle ways by creating a culture that minimizes personal responsibility and obfuscates the reasonable mitigation measures we can all take.
And almost the exact set of actions have a corollary in unwittingly supporting human trafficking. You probably contributed to human trafficking (as I did) today when you purchased products that had slave labor upstream in their supply chain. Some companies are better about monitoring their supply chain for slave labor than others, and there are groups that keep independent report cards for everything from the fashion industry to your local grocery store. But while buying blue jeans, chocolate, or a new smartphone may support labor trafficking and slavery in the supply chain throughout the world, there is one auxiliary consumer industry that supports sex trafficking specifically; pornography.These two industries are indelibly linked. A culture of widespread pornography use and addiction contributes to dehumanization of and violence towards women, and fetishizes demeaning sexual interactions, sexual violence, and rape, and it feeds the demand for sex trafficking from the consumer side. But the connection runs even deeper than that, because if you have consumed pornography you have not only supported the sex trafficking industry financially but have most likely participated in the sexual exploitation of trafficking victims as well. Many pornography websites, including the largest and most visited pornography website in the world (link is to an advocacy group video about the website, not the website itself, obviously), rely mostly or entirely on user uploaded content and do not have sufficient screening criteria in place to prevent the uploading and viewing of content showing the sexual abuse of children or adolescents, or content showing non-simulated rape and sexual torture. In fact, videos are often tagged with words like “teen”, “young girl,” or “innocent” in the title, yet are still streamed from their website without additional vetting or any requirement to prove that the women in the videos are actually consenting adults. This is not a theoretical risk; the sexual abuse of teenage girls and even children being streamed from these sites has been well documented. And once these videos are available on the internet, they can be next to impossible to have removed, as we have heard from survivors who have battled to have videos of their own rape taken down from these websites.
You can fight both right now. As a physician, I’m here to tell you that you can fight COVID-19 right now in the comfort of your own home (by, you know, staying there). Wear a mask when you leave the house, physical distance while building up your social circle, reaching out to neighbors, loved ones, and friends remotely to see how they are doing 6 months into this pandemic and if there’s anything they need. Help fight against medical misinformation that contributes to unsafe, pro-COVID behaviors and attitudes. And you can fight human trafficking right now as well. Start reading with one of the resources above and keep reading and educating yourself about this important topic that isn’t going to go away even once COVID-19 is a distant memory. Look into the ways that your clothing, your food, and your other purchasing choices might help or hurt the plight of slaves around the world. If you’ve read this post and have decided it’s finally time to stop using pornography, go to a website like Fight the New Drug to get more information, support, and resources, and find an accountability partner to download an app like Ever Accountable and quit porn alongside you. Finally, consider donating to an organization like International Justice Mission that actively works to intervene in situations of slavery around the world, and then sticks around to provide the legal and support services to guarantee that survivors aren’t re-victimized by their traffickers.
So no, there isn’t a fight between awareness of human trafficking and focus on COVID-19, and the people who want you to believe there is may well care about neither one of them; but we are in the fight of our lives against both, and since you do care, we could sure use your help.
Update 11/30/2020: For some reason this particular post got picked up by Google’s algorithms and ended up on the first page of results for a few search terms like “COVID vs. Car Crashes,” and so continues to get visits frequently almost 4 months later. Which is pretty cool I guess. But the big take away here is this; just like the graphs showing COVID-19 death data from March were already inaccurate and undersold the severity of the pandemic compared to car crashes by August when I wrote this post, so the graphs and data from this post are now out of date. We were at 165,000 deaths then; it’s 267,000 now. I’ll post some updated graphs below to illustrate this, but when I said in August “there is reason to believe that COVID-19 will settle in as the 3rd leading cause of death in 2020” it just so happens I was exactly correct. It wasn’t a hard guess; the gap between Heart Disease and Cancer and the 3rd and 4th leading causes of death is so great that it was a no brainer, as anyone who plays the board game Wits and Wagers will tell you. The real question is whether or not COVID-19 will overtake even Cancer and Heart Disease in 2021. I highly doubt it, especially with effective vaccines available soon and constantly improving treatment techniques and medication regimens… But it largely depends on how overwhelmed the medical infrastructure becomes over the next few months following Thanksgiving and Christmas.
Updated graphs from November 30th, 2020:
(Flu deaths not adjusted due to seasonality)
I first saw this graph on Facebook last month; at the time I was writing extensively about asymptomatic cases, death statistics, herd immunity, and other topics and didn’t have much margin to spare for it. Besides, multiple people have written extensively and well about this topic over the last several months as these silly comparisons between COVID-19 deaths and car accidents, heart disease, cancer, and any number of other causes of human death and suffering have been rampant.
But yesterday evening, when falling asleep at 7 PM exhausted and slightly delirious from what I thought might be COVID-19 but turned outto be from not drinking enough water while working at our outside COVID-19 clinic in 95 degree heat, which is not technically a COVID-19 related illness (and would not be recorded as one regardless of what the conspiracy theorists tell you), I came across a meme along the same lines and felt it was time to say something about these fallacious comparisons. I’m going to start with traffic accidents and heart disease today, for the sake of thoroughness, but tomorrow I’ll try to address the memes that really got my blood boiling; the ones comparing COVID-19 to human trafficking and modern day slavery.
Contagious vs. Non-Contagious Illnesses
You have no doubt seen some version of this argument before now. It usually has a very simple formula, which we will try to tackle one by one:
Compare COVID-19 deaths to another leading cause of death.
Ask why the other cause of death isn’t being talked about/doesn’t shutdown the economy/isn’t a national issue.
Imply or outright state it’s because the media/doctors/the powers that be want you to be afraid for some nefarious purpose.
(In all fairness, the authors of the article above seemed to be writing it just to raise awareness about programs to help teens drive safer; the headline comparing it to COVID-19, while typical of the format this argument has taken across the internet, is seemingly just to garner clicks in this case)
We’ve seen charts like the one above, showing the “incredibly small number of deaths” from COVID-19 compared to real killers like heart disease and stroke. “See, it isn’t even as bad as the flu!” We’ve seen statistics that are next to meaningless, like “COVID-19 will only make up 5% of deaths in the US this year,” which is supposed to sound to laypeople like COVID-19 isn’t that big of a deal, but is actually a terrifying thing to hear as a physician. We’ve been asked, knowingly, why we didn’t “shut-down the economy” for H1N1 in 2009… Maybe because nobody was trying to undermine the president’s chances of re-election? We’ve been asked why we don’t social distance because of car accidents, and then been told the answer; because COVID-19 is all about creating fear.
During the SARS-CoV-2 pandemic we’ve seen physicians, epidemiologists, laypeople, politicians, and misinformation hucksters compare COVID-19 to the common cold, influenza, measles, ebola, HIV, SARS and MERS, and the Spanish Flu pandemic of 1918. While these comparisons have often been made with false statistics or poor understanding of epidemiology and thus led to incorrect, often diametrically misleading conclusions, the comparisons themselves are indeed apt. SARS-CoV-2 is a contagious, viral illness, just like those other diseases, and the danger it poses depends on how contagious it is, how deadly each individual case is, and the long-lasting sequelae it causes, just like those other illnesses.
But the comparisons in the chart above are not all apt, because most are not contagious diseases, and fighting them requires entirely different monitoring, treatment, and prevention principles compared to viruses like measles, ebola, or COVID-19. Yes, preventing diabetes would be easier if we, as a society, decided to rearrange our lives and our community norms to focus on physical activity and healthy eating, eliminate food desserts (or is it deserts? both contribute to diabetes so I’m going to leave it as-is), provide nutrition education as core curriculum in our high schools, and take any number of other steps to become a healthier nation with better and more equitable access to healthy choices overall. But those changes take a lot of time to implement. While there are plenty of ways to help in such efforts, such as shopping at grocery stores intentionally built in food deserts, places like Waco’s Jubilee Food Market, there’s very little that you can do, right here in the middle of your afternoon, to prevent someone you are coming into casual contact with from developing diabetes or heart disease today. As passionate as you are about fighting heart disease and diabetes, you can’t go to a coffee shop and start yelling about metabolic syndrome to try to raise awareness; they kick you out for stuff like that. But you can do things today to prevent the spread of COVID-19, like wearing a mask and social distancing, and a big societal push in that direction makessense for COVID-19, where for chronic illnesses with modifiable risk factors it makes more sense to focus on sustained, long-term efforts over generations than urgent, short-term pushes.
Me at Pinewood Roasters, trying to warn people about chronic illnesses.
Moreover, diseases like diabetes and coronary artery disease don’t typically kill you all at one time. As we’ve discussed multiple times before, these chronic diseases increase your risk of multiple other ailments, including your risk of a severe case of COVID-19. Saying we shouldn’t worry about COVID-19 because ‘look how bad heart disease is’ is a bit like saying the people on the Titanic shouldn’t worry about the iceberg, because it’s really the water that ultimately killed most of them. There’s a synergy between COVID-19 and heart disease, lung disease, diabetes, and other chronic health conditions, and you aren’t doing congestive heart failure patients any favors by trying to shift the focus off of COVID-19 transmission and slowing the spread of the pandemic; that kind of approach is only going to increase the number of deaths from both conditions.
“Why don’t we shut down the economy for ________?”
But the other reason these comparisons fail is because, to the degree that the approach to treating and preventing them is similar, the responses of the media and doctors to these causes of death has been similar to that of COVID-19. Various people who share these statistics say things like, “we don’t shut down the economy over diabetes,” “we don’t close schools because of car accidents,” and “we don’t social distance and stop going to bars because of liver disease” (I made that last one up because it was the most ironic possible instance of that line of argument). Dr. Phil made this exact same argument on Fox News back in April.
But none of this is actually true, is it? One of the reasons that school gets cancelled on days with severe snow storms (or in Texas, days where someone might have seen some white stuff falling from the sky when it was the wrong season for Crepe Myrtles) is because severe ice on the roads would increase the risks inherent in traveling back and forth to schools; we cancel school precisely because there is an increased risk, above that at normal times, of people dying in car accidents. We also have tons of laws related to traffic safety, including speed limits and traffic signals, without which we could no doubt get to work quicker and be more productive, and laws about texting while driving without which doctors, at the very least, could be much more productive during our commutes. We have all of these rules and regulations in place because the danger has been recognized.
Becoming the Sorcerer Supreme occurs in less than 1 in 14 million cases of physician texting-while-driving accidents. Don’t do it.
We also have laws about cigarette advertising and smoking inside restaurants and places of business, laws regarding industrial and toxic exposures, laws about medical leave for chronic, progressive illnesses like cancer, and laws about sick leave and not being fired because of medical issues. It’s true that these laws often provide depressingly little protection for employees, but they are in place and it’s erroneous to say that we don’t “allow” these medical issues to affect ‘the economy’ or ‘our freedoms’. The one key difference is that none of these approaches are proactive the way that masking, social distancing, and strategic closings are in a viral pandemic. Things like scheduled exercise breaks and company-sponsored healthy mealsare proactive ways to fight heart disease and diabetes and would definitely boost the economy if adopted widely, but they are difficult to implement and need a high degree of buy-in from both businesses and employees; they are going to require cultural changes that take time, something we don’t have a lot of in the midst of a viral pandemic. Yet the economic costs of these diseases is so great that if we could somehow drastically reduce deaths and hospitalizations from them by strategically shutting down non-essential businesses and engaging in social distancing and mask wearing for a discrete period of time, it would be an obvious win for the economy, even aside from the question of the inestimable value of those human lives. But while heart disease doesn’t work that way, contagious illnesses like COVID-19 do, and the idea that any of the measures we have adopted have been ‘overreactions’ that we ‘wouldn’t do for any other disease’ belies the fact that we definitely would if we had similar options to fight those diseases (or I hope we would; I’m probably letting my naive optimism show a little too much here).
But even apart from questions of economics, diseases like cancer, diabetes, and coronary artery disease are important topics that are talked about constantly in the news, and that millions of people like me devote literally every day of their full time jobs to fighting, preventing, diagnosing, treating, and counseling people about. COVID-19 is causing a pandemic, and it’s understandable to feel some frustration that it has sometimes seemed like the only thing the news has been reporting on; but we shouldn’t pretend that sensationalization of medical topics is new or that the media has never spent significant energy and focus on these other diseases. When something negatively effects peoples’ lives to an extreme degree, like COVID-19 and these other diseases do, people are going to read and write about it; but unlike COVID-19, the interest is more or less sustained over the years. This isn’t just true for the news; it’s true for us, too; just look at this graph of searches from Google Trends. We are always thinking about these issues, as a society, at a pretty steady rate; COVID-19 is new and very dangerous, and so we are thinking about it now all at the same time.
I am uncertain of how many of the searches for “heart attack” are related to the Demi Lovato song.
COVID-19 is just as incredibly dangerous as the leading causes of death.
But the final and most important issue here, and maybe the one I should have started with, is that these statistics are lies, at least when you are seeing them shared on social media now. That graph above showing COVID-19 deaths compared to cancer and heart disease is from March, when ‘only’ a few thousand people had died from COVID-19 and the US had yet to hit any regional surges. It compares cases at the beginning of the pandemic to deaths from other causes for the entire year. But by the second week in April COVID-19 had become theleading cause of death, in deaths per day, and stayed there throughout all of April and half of May. Since then it has continued to jockey for position with cancer and heart disease (while disproportionately affecting people already battling these diseases), and is now on the rise again.
If we want to compare apples to apples, we could wait to compare the number of deaths once COVID-19 had an appreciable impact; the 2nd graph below shows COVID-19 deaths compared to other causes of death today. If we wanted to compare same-sized apples, we could look at deaths from COVID-19 since the first death was reported in the US on February 29th; the 3rd graph below shows deaths from COVID-19 compared to an equivalent time period, 154 days (and for the 2017 flu and 2009 H1N1, the slightly shorter period encompassing their entire flu seasons).
Ask yourself why people are sharing only the top graph on facebook, 4 months and 160,000 deaths later
Looking at the 2nd graph, COVID-19 has already surpassed stroke, drug overdose, and the very deadly Seasonal Flu of 2017-2018, and there is zero chance that it won’t also surpass accidents and chronic respiratory diseases soon. But unlike the flu, COVID-19 did not begin to disappear in the late Spring and early Summer, and we are once again seeing a surge in deaths from the virus as we enter August. If we look at the 3rd graph, there is reason to believe that COVID-19 will settle in as the 3rd leading cause of death in 2020; but it has already dwarfed all other causes except heart disease and cancer. Even this graph undersells the true impact of the virus, since the proportion of deaths occurring in February and March was very low. If we were to look at the number of deaths in the 120 days since COVID-19 deaths began to rise at the end of March, the picture would be even more bleak; but posting more and more alarming graphs by limiting the time frame to the most dangerous months of the pandemic so far, in order to show how dangerous COVID-19 really is, feels a little too much like manipulating the data in the virus’s favor; and COVID-19 doesn’t need or deserve any help from us.
So these comparisons are problematic because they ask us to believe that our society doesn’t already devote enormous resources to these other problems and that they don’t have incredible impacts on the economy, and because they are comparing very different causes of suffering, disease, and death that have to be combatted very differently. And they are deceptive because they are deliberately using old data from early in the pandemic (using old data when you know new data is available is also called lying) and discounting whatever time period of the pandemic doesn’t support their narrative. But I think the mostfrustrating thing for someone like me who spends hours every day talking about and thinking about diabetes and heart disease, has devoted extra time and effort to gaining proficiency with methods of treating drug dependence and preventing drug overdose, and has spent hundreds of hours working in emergency rooms and treating people following accidents and motor vehicle collisions, is that peopleoften seem to be sharing these comparisons not because they actually care about these other important medical issues, but because they don’t mind using themto reinforce their COVID-19 denialism and conspiracy theories… and then droppingthem again once they are no longer useful or convenient. But because I’ve lost my lisinopril bottle again and apparently want to see how high I can get my blood pressure this week, we are going to save that discussion for tomorrow when we talk about the comparisons being made between COVID-19 and Human Trafficking.
I have seen this video of Dr. Simone Gold, Dr. Stella Immanuel, and Dr. Dan Erickson, and other physicians in almost every format over the past 24 hours; from a 45 minute long version to just Dr. Immanuel’s comments. My favorite presentation of it, if I’m allowed to pick a favorite, is the headline that I saw first which read, “American Doctors Address COVID 19 Misinformation with SCOTUS Press Conference.” I know it’s the oldest tactic in the book, but something about people spreading misinformation by claiming they are fighting misinformation still really gets to me. I understand this video was viewed over 14 million times before youtube and social media sites began to take it down, and I understand why. The group, America’s Frontline Physicians, present themselves in patriotic themed lab coats (I did not know that was a thing) in front of the US Capitol (or whatever building that is; I was homeschooled), and tell Americans what we have all so desperately wanted to hear for months; there’s nothing to be worried about, your lives can go back to normal now.
Several of these physicians we are already familiar with. Dr. Dan Erickson’s interview with local news stations was perhaps the biggest COVID-19 misinformation viral video until Plandemic came along (a week later), and Dr. Simone Gold has gone viral multiple times; I addressed her “COVID-19 as a Mass Casualty Event” letter on the blog back in May. Though these doctors don’t know me from Adam, to me they are starting to feel like old friends; or at least old frenemies. They are becoming more sophisticated in the posturing they take around misinformation (that sounded ominous; “they are becoming more sophisticated”, like they were killer robots from SkyNet); including in their talk the idea that they are being ‘silenced’ even though tens of millions of Americans have heard their dissenting minority opinions, claiming to speak for ‘thousands of doctors’ (this is probably an accurate number; there are about 1.1 million doctors in the US), and painting a convincing picture of themselves as the front-line doctors ‘actually diagnosing and treating’ COVID-19 and the people ‘silencing’ (read: disagreeing with) them as shadowy powers-that-be, as opposed to just being the vast majority of conscientious front-line doctors who simply hold to higher standards of evidence and have less tolerance for the invasion of political concerns into our care of patients. All of this is lent some credence by the fact that this video is being censored on Youtube and Facebook, of course; but considering the views they share really are dangerous, I have to admit that I don’t know whether censoring the video is the right call or not; I’m glad it’s not my decision to make. My approach has been to analyse and discuss, and I’m thankful for those who have provided me with the transcript and alternative links to the video for me to try to do that.
Since I worked from 8-5 today, including a morning spent in our outdoor tent clinic diagnosing, treating, and counseling patients with COVID-19, and a motorcycle drive in a torrential downpour (it said 10% chance of precipitation!), I’m about 18 hours behind on responding to this video. In interest of making this analysis available to those who have asked for it more quickly, I’m going to take it one doctor at a time, starting with a response to Dr. Stella Immanuel’s comments. The full transcript is below, up to the Q&A which I won’t spend time addressing. My comments are in blue and will be added as I go.
TL;DR: Posting now, editing and adding to later. Reserve the right to wake up at 3 AM and fix spelling erros.
Congressman Norman: (00:00) … I’ll turn it over.
I have no idea who Congressman Norman is, but it has a very sinister ‘Spider-Man villian’ ring to it, doesn’t it?
Dr. Simone Gold
Dr. Simone Gold: (00:01) Thank you. Thank you so much congressmen. So we’re here because we feel as though the American people have not heard from all the expertise that’s out there all across our country. We do have some experts speaking, but there’s lots and lots of experts across the country. So some of us decided to get together. We’re America’s Frontline Doctors. We’re here only to help American patients and the American nation heal. We have a lot of information to share. Americans are riveted and captured by fear at the moment. We are not held down by the virus as much as we’re being held down by the spider web of fear. That spiderweb is all around us and it’s constricting us and it’s draining the lifeblood of the American people, American society, and American economy.
America’s Frontline Doctors seems like a new organization, but for COVID-19 Viral Video enthusiasts like myself, seeing them all together in this video feels like the first time we saw all of the The Avengers together in The Avengers after 4 years of build-up. The group’s logo is a caduceus overlaid with an American flag; a perfectly fine image, I suppose, but taken with their political aims it sends a clear message; “we are the only doctors that true American patriots can trust.” Later, when these physicians make claims that other doctors have not been using hydroxychloroquine, have been encouraging people to wear masks, or have been advising caution and social distancing because of political motivations, please remember exactly who has overtly politicized their medical calling and emblazoned it on their lab coats. You know what my lab coat has it on? Germs (that’s what they all have, which is why I don’t wear one).
I think Dr. Gold’s discussion of the fear capturing the American people here is very interesting. Certainly there are many responses to the deadly viral pandemic that America is facing; fear, anxiety, bravado, calloused indifference, defiance. I’ve had all of those responses myself, and that was just this morning. I have seen many people suffer from anxiety about the virus, for the sake of themselves and their loved ones, and have offered a listening ear and counseling (and, when appropriate, anxiety medication); I have also seen people who consider COVID-19 to be a political tool or a hoax and have shown brazen disregard of the very real danger posed by the virus, and a great many of them are going to watch and share this video. There is something fairly calloused and icky about sharing a message that ‘you don’t have to be afraid anymore’ to people you already know aren’t taking a dangerous thing seriously. Nevertheless, I’ve actually repeated Dr. Gold’s main point here, “I don’t want you to be afraid,” at least 100 times in the past week; probably far more. When I counsel patients who likely have COVID-19, or whose loved ones do, I almost always tell them that I don’t want them to be afraid. I also tell them about social distancing and counsel them on isolation precautions, and talk to them about getting in touch with their close contacts to encourage them to quarantine, and I talk with them about reasons they would return to my clinic or go to the ER or even call 911 if their symptoms worsen. Because my desire for them not to be afraid isn’t because there isn’t anything anything to be afraid of, like Dr. Gold claims, but because because fear leads to anger and anger leads to hate, and hate leads to suffering… Because fear is the mind killer, the little-death that brings total obliteration… Because with great power comes great (no wait that isn’t one, sorry)… But really because God has not given us a spirit of fear, and I believe that my patients will thrive best and be most free from fear when they have a healthy respect and understanding of the virus and how to protect others and respond to complications based on the best, most reliable information possible.
Dr.Simone Gold: (00:53) This does not make sense. COVID-19 is a virus that exists in essentially two phases. There’s the early phase disease, and there’s the late phase disease. In the early phase either before you get the virus or early, when you’ve gotten the virus, if you’ve gotten the virus, there’s treatment. That’s what we’re here to tell you. We’re going to talk about that this afternoon. You can find it on America’s Frontline Doctors, there’s many other sites that are streaming it live on Facebook. But we implore you to hear this because this message has been silenced. There are many thousands of physicians who have been silenced for telling the American people the good news about the situation, that we can manage the virus carefully and intelligently, but we cannot live with this spider web of fear that’s constricting our country.
Dr. Simone Gold: (01:45) So we’re going to hear now from various positions. Some are going to talk to you about what the lockdown has done to young, to older, to businesses, to the economy, and how we can get ourselves out of the cycle of fear. Dr. Hamilton.
Dr. Bob Hamilton
Dr. Bob Hamilton: (02:03) My name is Dr. Bob Hamilton. I’m a pediatrician from Santa Monica, California. I’ve been in private practice there for 36 years. And today I have good news for you. The good news is the children as a general rule are taking this virus very, very well. Few are getting infected. Those who are getting infected are being hospitalized in low numbers. And fortunately the mortality rate of children is about one fifth of 1%. So kids are tolerating the infection very frequently, but are actually asymptomatic.
And thank God for that. As a father of 4 young children, I cannot even imagine the anxiety, fear, and paranoia I would experience if we were living through a pandemic like the Spanish Flu, which disproportionately killed young children. I cannot imagine the pandemonium, the incredible amounts of fear, and even the difficulty in staffing clinics and hospitals if exposure to the virus put our children‘s lives at great risk instead of just our own. Though Dr. Stella Immanuel below discusses the panic that her patients commonly present with when they believe they may have COVID-19, I’ve only see this a few times; many patients need reassurance and education, but only a handful have been truly on the verge of a panic attack. But I have seen many, many people very concerned about their children and grandchildren. In fact, when I inform patients that they have been diagnosed with COVID-19, they usually ask “what about my children?” before they ask any other question.
The truth is we don’t know the mortality rate among children, for a lot of the same reasons that it’s so hard to lock-down a true infection fatality rate in general; imperfect testing, asymptomatic cases, minimally symptomatic cases that are never tested, and still being fairly early in the course of the pandemic and not having all of the data we need. But we all agree it’s smaller than for older patients, and Dr. Hamilton’s estimate of 0.2% is within the commonly accepted range based on the data we do have. I would point out that 0.2% is still a very alarming mortality rate for a virus that is as infectious as COVID-19; but a lot of us hope the rate is actually even lower and that children tend to be asymptomatic or minimally symptomatic at a high enough rate that we are simply missing most cases. We hope, but we don’t know. So while I can counsel the patients who anxiously ask me if their children are going to be ok (which would be the very first question on my mind as well) that they are at less risk from COVID-19 than any other age group, I cannot promise them that their children will be unaffected or free from risk, and I still counsel them on what to watch for.
Dr. Bob Hamilton: (02:38) I also want to say that children are not the drivers of this pandemic. People were worried about, initially, if children were going to actually be the ones to push the infection along. The very opposite is happening. Kids are tolerating it very well, they’re not passing it on to their parents, they’re not passing it onto their teachers. Dr. Mark Woolhouse from Scotland, who is a pediatric infectious disease specialist and epidemiologist said the following. He said, “There has not been one documented case of COVID being transferred from a student to a teacher in the world.” In the world.
I think here Dr. Hamilton is straying into a fairly disingenuous way of looking at these statistics. One of the first and most widely followed mitigation steps early in the pandemic was to transition schools to online learning. More than closing non-essential businesses, more than observing social distancing, more than wearing masks once sufficient evidence to support mask-wearing was amassed, children were compliant with not being in school at very high rates because schools were, physically, closed. I will accept that children have not been thedriver of the pandemic; they are also one of the groups that has been kept at home most successfully during it. Saying children have not driven the pandemic is not the same as saying they would not have or might not if these mitigation measures were not followed. The question of whether or not children can or will drive the pandemic once schools reopen in person is nuanced and difficult; I’ll try to address it in the next paragraph and in greater detail in a later article. But it’s important that we don’t fall into the trap of evaluating the course the pandemic has taken so far without taking into account the effects of the precautions and mitigation measures we havetaken in response to it.
Dr. Bob Hamilton: (03:19) I think that is important that all of us who are here today realize that our kids are not really the ones who are driving the infection. It is being driven by older individuals. And yes, we can send the kids back to school I think without fear. And this is the big issue right now, as Congressman Norman alluded to, this is the really important thing we need to do. We need to normalize the lives of our children. How do we do that? We do that by getting them back in the classroom. And the good news is they’re not driving this infection at all. Yes, we can use security measures. Yes, we can be careful. I’m all for that. We all are. But I think the important thing is we need to not act out of fear. We need to act out of science. We need to do it. We need to get it done.
Again, just because children in school have not driven transmission so far, because they have not been in school, doesn’t mean that it isn’t a risk. I don’t know whether or not we should reopen schools normally in a few weeks. There are lots of reasons I haven’t been able to come to anything like a firm conclusion about it. The data is complicated, and it’s such an important question that it really does require a degree of thorough research and critical thinking that I have not been able to give to it yet. Part of that is my own privilege; my wife and I homeschool our four children (and I include “and I” very generously), so it’s a question that doesn’t personally affect us. Homeschooling has always involved some degree of privilege, even though it is also challenging and requires sacrifice, but that’s never been quite so obvious to me as it is now in the midst of this pandemic, when this one big question mark seems to be looming over nearly every family we know but our own. But even though it doesn’t directly affect our own children, there are many teachers and school aged children that we deeply care about (and tons that we sort of care about or middling care about), and the question has been heavy on my mind, especially as more and more close friends have asked me to research and write about it.
All of that to say, I don’t have an answer today; I hope to write about it soon, but I can’t promise I’ll have an answer then either. For now I’ll say this; I think the burden of proof has to be on the side of proving it’s safe, not on the side of proving it’s not safe. I need to review the studies on transmission and shedding in children, but the claim I’ve seen that children are very unlikely to transmit the virus seems very counter-intuitive. Transmitting respiratory viruses is what children do. I’ve got four of these booger goblins at home; the little one gives kisses by putting his entire mouth around your nose, and the 2nd youngest “whispers” to you by blowing spit into your ear and your eyeball. One of the questions we always ask someone with a cold or flu, even pre-COVID-19, is whether they have been around anyone sick. If the answer is “well I have kids” or “well I work in a school” my response is, “say no more.” If there’s one thing we’ve learned about COVID-19, it’s that it’s different. Maybe kids really don’t shed it, maybe they really don’t spread it to each other or to adults; maybe we can reopen schools with sufficient distancing guidelines that it will not endanger the lives of children or or adolescents or their caregivers, teachers, or families. If that’s the case, that’s wonderful; but it has to be very, very clearly demonstrated by real scientific evidence. It isn’t something we can risk on the type or quality of “evidence” that some of the members of America’s Frontline Doctors seem to find sufficient. We’ll try to look at as much of that evidence as we can in an upcoming post.
Dr. Bob Hamilton: (04:07) Finally, the barrier, and I hate to say this, but the barrier to getting our kids back in school is not going to be the science, it’s going to be the national unions, the teachers union, the National Education Association, other groups who are going to demand money. And listen, I think that it’s fine to give people money for PPE and different things in the classroom. But some of their demands are really ridiculous. They’re talking about, where I’m from in California, the UTLA, which is United Teachers Union of Los Angeles, is demanding that we defund the police. What does that have to do with education? They’re demanding that they stop or they shut all private charter schools, privately funded charter schools. These are the schools that are actually getting the kids educated.
This gets too deep into politics for me. Look at the various teachers unions’ demands (if they have demands) in your area for yourself and see if you think what they are asking for is reasonable. Better still, talk to teachers you know and ask for their opinion on reopening schools, the same way that you would (hopefully) ask me or another physician you know about our views on wearing masks or other medical issues related to the pandemic. I know some teachers, and I know that their greatest desire (besides something called a “smart board”) is to be back in the classroom educating and pouring life into your children. They want the schools to reopen, but they want to know the safest and wisest way for it to happen, because too much of their job already deals with childhood suffering, and seeing anything like an abnormally high number of their students (your children) die from COVID-19 because we re-opened schools in the midst of a surge of cases would break them. No profession is perfect (something I’m hoping to write about soon too, but in the meantime you should go read Harriet Washington’s Medical Apartheid for yourself), but if you don’t think doctors in general want you to be well and thrive, and you don’t think teachers want your children to grown and learn, I’ve got some questions about who you do trust.
Dr. Bob Hamilton: (04:59) So clearly there are going to be barriers. The barriers will not be science. There will not be barriers for the sake of the children. That’s going to be for the sake of the adults, the teachers, and everybody else, and for the union. So that’s where we need to focus our efforts and fight back. So thank you all for being here and let’s get our kids back in school.
Leave out that there really are some scientific barriers to knowing whether or not fully reopening schools is actually going to be safe for the children, which is probably the single biggest concern among teachers anyway; there’s still something very calloused about calling out teachers for not wanting to re-open schools because of concerns about their own safety.
Dr. Stella Immanuel
Dr. Stella Immanuel: (05:27) Hello, I’m Dr. Stella Immanuel. I’m a primary care physician in Houston, Texas. I actually went to medical school in West Africa, Nigeria, where I took care of malaria patients, treated them with hydroxychloroquine and stuff like that. So I’m actually used to these medications.
I’ve learned an awful lot from African physicians over the years, though I’ve never been to Nigeria and have not had the privilege to travel to West Africa since before medical school. I do not know the arc of Dr. Immanuel’s career, how long she practiced in Nigeria and how long she has now practiced in the US (I am told she used to live in the same city where I did undergrad). On my most recent short term trips to volunteer in hospitals in South Sudan and Uganda, I went in a teaching role; and while I did have some things to contribute, there is no question that I gained from doctors there more knowledge and insight than I was able to give, which is what I fully expected would happen. And nowhere was this dynamic more clear than in treating patients with “tropical diseases” like yellow fever and malaria. Diagnostic tests, medications, and clinical pictures that I had encountered primarily in textbooks were bread and butter medicine for the physicians I worked with, and I’m sure I must have seemed fairly slow on the uptake, trying to figure out the right chloroquine dose for pediatric malaria patients or recognize the differences in the clinical picture between malaria and dengue fever. While I’ve now also used these medications for malaria, in addition to prescribing them for lupus here in the US, I would completely concede more extensive experience with antimalarial agents to a West African trained doctor like Dr. Immanuel. What I cannot honestly concede is more extensive experience diagnosing and treating COVID-19.
Dr. Stella Immanuel: I’m here because I have personally treated over 350 patients with COVID. Patients that have diabetes, patients that have high blood pressure, patients that have asthma, old people … I think my oldest patient is 92 … 87 year olds. And the result has been the same. I put them on hydroxychloroquine, I put them on zinc, I put them on Zithromax, and they’re all well.
The best way to study a medication’s efficacy is a double-blinded, randomized, controlled trial. There are studies that have been done and are being done on hydroxychloroquine for COVID-19 that are designed this way, and if done carefully they will provide the absolute highest quality data we will have on this medication. So far the ones we have do not show benefit. It’s worth pointing out here that one large, well-designed study is of much greater value than many small or poorly designed studies, and of infinitely greater value than any one or a few clinicians’ anecdotal experiences. But in a pandemic I do believe in an all-hands-on-deck approach to both clinical treatment and research, and I appreciate all of the doctors for whom research is not a usual interest or activity taking the time and energy to bring their results forward.
But we would not be wise to digest these results without understanding their significance. When Dr. Immanuel says she has treated 350 patients for COVID-19, that feels like a fairly large number; especially compared to the dozen that Dr. Bartlett had treated to support his claims for budesonide or the 50 that Dr. Procter had treated in a recent viral facebook post. But we still need more information, like how her patient population’s demographics compare to the population in general, which she only hints at, telling us the age of her oldest patient but not providing a median age or other demographics factors or data on comorbidities or high-risk conditions. Depending on their risk factors and their ages, zero deaths out of 350 might be exactly what we would expect. Even if Dr. Immanuel’s population perfectly represented thegeneralpopulation (and we have good reasons to suspect this is not the case, as we will discuss below), where we believe the infection fatality rate is somewhere in the still-very dangerous- range of 0.4% to 1.3%, this would only be 1-4 fewer deaths than expected; wonderful, well worth celebrating, but not miraculous, and certainly not proof of a cure. But aside from the simple numbers, there are bigger issues we need to be honest about here.
Dr. Stella Immanuel: (06:12) For the past few months, after taking care of over 350 patients, we’ve not lost one. Not a diabetic, not a somebody with high blood pressure, not somebody who asthma, not an old person. We’ve not lost one patient.
As I’ve done for every doctor making claims of perfect efficacy for unproven medications over the past few months, I’d like to look at Dr. Immanuel’s claims in the context of her treatment setting; namely, outpatient Family Medicine in Houston, Texas. Here is the graph of positive cases in Houston.
If this looks familiar to my fellow Wacoans, maybe it’s because it looks almost identical to the trend in cases in Waco, and really in most places around Texas. Here is our trend from April to July from the health department’s tracker at covidwaco.com (based on positive test results).
You’ll note these charts are not to the same scale; Waco does not (yet) have a population of 2.3 million people. But there are only so many patients a doctor can see in a day, and both Waco and Houston have had plenty of COVID-19 cases, and people being evaluated for possible cases, to keep more than one doctor very busy, and it’s pretty hard for me to imagine that Dr. Immanuel has seen many more patients for evaluation of COVID-19 symptoms than I have over the past couple of months. But if we look at these trends it strongly implies that the vast majority of her patients who actually had COVID-19 would have been in the past 6 weeks, just like mine have been; before that the infection rates in Houston and in Waco were too low for either of us to have extensive experience with patients who actually had the virus, regardless of how many people we were evaluating and testing (important work still, since none of us knew when our surge would start). She doesn’t tell us how many of her 350+ patients were in March, April, and May and how many have been since mid-June, just that she has treated that many patients with hydroxychloroquine over the past several months. If we assume that the majority of these patients have been in the last 42 (great number) days since cases began to climb in Houston, it means that a lot of her patients are not out of the woods yet. There is a lag time from the development of early symptoms of COVID-19 to the development of severe complications, and a further lag time from this to death, while patients fight for their lives in the hospital and doctors and nurses do everything in their power to help them. Finding an exact number is difficult because there are so many factors and so many different ways that people are affected by the virus; but the total lag from onset of symptoms to death seems to be around 18 days. Even this is likely an underestimate, however, since any such data would exclude people experiencing a prolonged battle with the virus who are still fighting it at the time the data is collected, but ultimately pass away from it later. This gives us a mere 24 days during which we can say Dr. Immanuel has had time to see a significant number of patients with COVID-19 and feel confident in saying that those patients have fully recovered and are no longer in danger.
I am playing a bit fast and loose with these numbers here, because I don’t actually think Dr. Immanuel means that the majority of her 350 “COVID patients” have been within the past 6 weeks. The point is this; when doctors claim to have been treating COVID-19 a certain way for months, you need to look and see how many months there have actually been COVID patients in their area. Because if the length of time they have been ‘treating COVID’ successfully and the length of time that SARS-CoV-2 has been endemic in their region don’t line up, we have to ask an important question that runs deeper even than the demographics and risk factors of their patients; did the patients they treated even have COVID-19 at all?
You see, over and over when we have heard from physicians like Dr. Irene Lozano and Dr. Brian Procter that they have a 100% cure rate with hydroxychloroquine or another regimen, it turns out that their definition of ‘having COVID-19’ is extremely liberal. One admits to treating patients with minimal symptoms and questionable exposures; the other says he doesn’t even believe in testing for COVID-19. This is the most basic concept of epidemiology imaginable, but you can’t die from a disease you don’t have. If a doctor says they have successfully treated a condition x number of times, but their diagnosis of the condition doesn’t conform to accepted standards of certainty or rely on any evidence other than a hunch or their desire or ideological commitment to ‘diagnose’ and treat the condition, their results are less than useless; they don’t even count as anecdotal evidence.
I don’t know if this is the case for Dr. Immanuel; she doesn’t say that she doesn’t believe in testing, she doesn’t tell us what test her clinic uses or its sensitivity and specificity, or how many of her hydroxychloroquine patients were treated during Houston’s pre-surge months, or if she uses the accepted clinical diagnostic criteria in lieu of a positive test. I cannot say definitively that Dr. Immanuel has done what so many doctors in these videos have done and artificially inflated her COVID-19 patient series by treating people who did not meet any accepted diagnostic criteria but were merely worried they might have the virus. But this is absolutely key to understanding the significance of her success rates, and I do think she gives us a few important clues in that direction.
Dr. Stella Immanuel: And on top of that, I’ve put myself, my staff, and many doctors that I know on hydroxychloroquine for prevention, because by the very mechanism of action, it works early and as a prophylaxis. We see patients, 10 to 15 COVID patients, everyday. We give them breathing treatments. We only wear surgical mask. None of us has gotten sick. It works.
This is clue number one, and it’s a big one. I sometimes use a phrase I’m pretty sure I’ve coined; “we aren’t keeping the secret medicines for doctorshidden in the back.” I say this, when I think it’s appropriate to the patient, to help dispel the idea that I am holding out some sort of secret treatment that I only prescribe to other doctors and their families, which is something that my patients sometimes believe (and that some of them have very good historical reasons for believing). A compassionate, conscientious physician is going to treat your condition the same whether you have an MD or PhD or have very little education, whether you are rich or poor, and even whether or not they like you or you are mean to them; we don’t keep secret medicines in the back that you don’t unless you are ‘in the club.’ And because I believe that Dr. Immanuel is a compassionate physician, I don’t believe that she would be willing to give herself, her staff, and other doctors and medical personnel hydroxychloroquine as prophylaxis if she were unwilling to do the same for others. If she really believes it works in this clinical setting, it would be consistent of her to offer hydroxychloroquine for patients who have been around others with COVID-19, or thought they might have been, or who work in other high risk environments like nursing homes, food service, and grocery stores. And because she has more extensive experience with hydroxychloroquine for malaria treatment and prophylaxis than most US trained physicians, it would be reasonable to expect her to be somewhat more liberal in prescribing it for this purpose without the same degree of anxiety a doctor might feel who has only used it for lupus.
In claiming that she has successfully treated over 350 patients with COVID-19 with hydroxychloroquine, is Dr. Immanuel including the patients she has treated merely for prophylaxis, who have not been diagnosed with an infection at all? I don’t know, but considering the national stage and the passion she feels on this issue, I would feel a great degree of temptation to include those patients and bolster my treatment numbers, and if I wasn’t including them I would want to be explicit on that point.
Dr. Stella Immanuel: (06:46) So right now, I came here to Washington DC to say, America, nobody needs to die. The study that made me start using hydroxychloroquine was a study that they did under the NIH in 2005 that say it works. Recently, I was doing some research about a patient that had hiccups and I found out that they even did a recent study in the NIH, which is our National Institute … that is the National … NIH, what? National Institute of Health. They actually had a study and go look it up. Type hiccups and COVID, you will see it. They treated a patient that had hiccups with hydroxychloroquine and it proved that hiccups is a symptom of COVID. So if the NIH knows that treating the patient would hydroxychloroquine proves that hiccup is a symptom of COVID, then they definitely know the hydroxychloroquine works.
Dr. Immanuel is referring to a case report from April of one patient, a 62 year old man who presented to the ER with hiccups; he was found to have diffuse groundglass opacities on CT scan of his lungs and tested positive for COVID-19. The case study mentions that he was treated with hydroxychloroquine exactly once (twice if you count the abstract); it was standard treatment at the time this man was admitted, as it was in most places around the country before more evidence emergedthat it wasn’t efficacious. The study draws absolutely no conclusions that his COVID-19 was cured by hydroxychloroquine, but rather was published to emphasize that “physicians should keep COVID-19 infection on their differential as more cases are discovered through atypical presentations.” The idea that this case study somehow proves that the NIH “knows the hydroxychloroquine works” is a complete non-sequitur and betrays either intentional or accidental misunderstanding of the case study. Also, I love it when people google things and then post viral videos telling other people to google those things; it creates fascinating Google Trends graphs:
Dr. Stella Immanuel: (07:42) I’m upset. Why I’m upset is that I see people that cannot breathe. I see parents walk in, I see diabetic sit in my office knowing that this is a death sentence and they can’t breathe. And I hug them and I tell them, “It’s going to be okay. You’re going to live.” And we treat them and they leave. None has died.
This is clue number two. You see, Dr. Immanuel has fallen into the trap that so many other doctors whose claims we have looked at on this site have fallen into; they are actually treating the virus as though it were even more dangerous than it already is. Most doctors I know would accept a death rate for COVID-19 somewhere between 0.4 and 1.3% based on the best data we currently have available; incredibly dangerous, but not a death sentence. The diabetic patient with COVID-19 is most likely to recover without treatment, but if unchecked the virus could easily kills hundreds of thousands or even millions. That’s what happens in most dangerous, contagious illnesses; if unmitigated, it will kill far too many people, but any particular person is still statistically unlikely to die. In fact, I spend a lot of my time saying to my patients I am testing for COVID-19 almost what Dr. Immanuel is saying. I don’t hug them, but I do offer a therapeutic hand on the arm and say, “I think you’re going to be ok. Most people recover from this and never have to be in the hospital. Let’s talk about what to watch out for and how you can feel a little better while your body fights this.” By believing that this virus is almost universally deadly for certain people, she is ensuring that her evaluation of her treatment numbers is biased, because she then cannot objectively compare her survival rates to the real death rates. Each case proves the drug was the key, miraculous cure, because she’s convinced that each patient she treats would have died without it.
Dr. Stella Immanuel: So if some fake science, some person sponsored by all these fake pharma companies comes out say, “We’ve done studies and they found out that it doesn’t work.” I can tell you categorically it’s fixed science. I want to know who is sponsoring that study. I want to know who is behind it because there is no way I can treat 350 patients and counting and nobody is dead and they all did better.
Two things on this. Most of the COVID-19 and hydroxychloroquine studies that have come out have not been sponsored by any pharmaceutical company (I can’t think of any that have off the top of my head), and this is the first time I’ve ever seen someone accuse drug companies of fixing data to prove that there was no specific drug therapy available. (yes, yes, I know; they are just setting us all up for a vaccine).
But more importantly, there absolutely is a way that she could treat 350 patientswith no deaths and it not be due to hydroxychloroquine, because many doctors around the country have exactly these same types of numbers withoutusing it. In fact, this is almost exactly what my numbers look like. I don’t feel at liberty to disclose the numbers or any details from my clinic without authorization from those patients; but I have been treating at least 20-30 patients for COVID-19 symptoms and exposure daily for weeks, and evaluating a significant number for the symptoms of COVID-19 in the months leading up to the beginning of our surge 6-7 weeks ago. I have treated well over 350 patients for suspected COVID-19, and many have been positive for the virus. None of them have died, praise God.Would I be justified in attributing this to something I am doing? Is it my particular form of counseling and reassurance? Is one of the symptomatic/supportive treatments I am recommending, like tylenol for body aches or hot tea with honey for sore throat, secretly an anti-COVID-19 miracle drug? Does mybreath inhibit COVID-19? Of course not. The difference is that none of these have a theoretical mechanism of action against COVID-19 (although my breath may encourage social distancing), and many medications like hydroxychloroquine and budesonide do. I am extremely hopeful that studies will prove some clinical setting or scenario where these really are useful for COVID-19; but using before then because of unreliable anecdotal evidence is irresponsible.
We would be better served looking at my patients, if we could. Some were only recently diagnosed and, as we’ve already stated, aren’t out of the woods yet. If you don’t think I’m deeply concerned about some of these patients getting sick in the next week or two, you haven’t been reading my blog. Many were exposed but did not develop the virus. Many had only a mild clinical course and few risk factors, including age. Many had symptoms that meant they would screen positive for further evaluation for COVID-19, but were actually ultimately due to something else; a bacterial pneumonia, a COVID-19 unrelated COPD exacerbation, migraine headaches, pregnancy. Do I get to count all of them in my ‘COVID-19 treatment’ numbers since I saw them for suspected COVID-19 based on their presenting symptoms? More importantly, these patients self-selected to my clinic by not being ill enough to need to call 911 or present straight to the ER, or by not being elderly enough or having enough medical complications to already live in certain very high-risk settings, like a long term skilled nursing facility, where they would be evaluated by another doctor entirely. If I had placed all of these hundreds of patients on hydroxychloroquine, zinc, and azithromycin, (and if none had adverse events or serious reactions to these medications), their outcomes would have been exactly the same. The only difference would be that they would have purchased and taken unnecessary medications and I would be convinced that I have locked-on to the miracle cure. After that, if any of my patients did die from COVID-19, I would probably be convinced I was still beating the odds.
Dr. Stella Immanuel: (08:21) I know you’re going to tell me that you treated 20 people, 40 people, and it didn’t work. I’m a true testimony. So I came here to Washington DC to tell America nobody needs to get sick. This virus has a cure. It is called hydroxychloroquine, zinc, and Zithromax. I know you people want to talk about a mask. Hello? You don’t need mask. There is a cure. I know they don’t want to open schools. No, you don’t need people to be locked down. There is prevention and there is a cure.
Do not trust anybody with your medical care who tells you don’t need prevention because you can just do treatment. Please wear a mask.
Dr. Stella Immanuel: (08:48) And let me tell you something, all you fake doctors out there that tell me, “Yeah. I want a double blinded study.” I just tell you, quit sounding like a computer, double blinded, double blinded. I don’t know whether your chips are malfunctioning, but I’m a real doctor. I have radiologists, we have plastic surgeons, we have neurosurgeons, like Sanjay Gupta saying, “Yeah, it doesn’t work and it causes heart disease.”
I’m a real doctor too and I believe in evidence based medicine. Also, take that all of you radiologists, would-be-plastic-surgeons, and neurosurgeons who did better than me on your boards (you know who you are. Miss you guys); I’m a real doctor!
Dr. Stella Immanuel: Let me ask you Dr. Sanjay Gupta. Hear me. Have you ever seen a COVID patient? Have you ever treated anybody with hydroxychloroquine and they died from heart disease? When you do, come and talk to me because I sit down in my clinic every day and I see these patients walk in everyday scared to death. I see people driving two, three hours to my clinic because some ER doctor is scared of the Texas board or they’re scared of something, and they will not prescribe medication to these people.
This is clue number three. Just like Dr. Lozano and Dr. Procter, Dr. Immanuel has patients driving across the state to see her because they know she will prescribe these hot-button medications for them even when other doctors wouldn’t. If you don’t understand why this is problematic or how this distorts her treatment numbers, please see my prior posts on those doctors’ claims.
Dr. Stella Immanuel: (09:35) I tell all of you doctors that are sitting down and watching Americans die. You’re like the good Nazi … the good one, the good Germans that watched Jews get killed and you did not speak up. If they come after me, they threaten me. They’ve threatened to … I mean, I’ve gotten all kinds of threats. Or they’re going to report me to the bots. I say, you know what? I don’t care. I’m not going to let Americans die. And if this is the hill where I get nailed on, I will get nailed on it. I don’t care. You can report me to the bots, you can kill me, you can do whatever, but I’m not going to let Americans die.
I’m choosing to leave this one alone for the most part. Dr. Immanuel has been widely lambasted on social media for holding a number of medical and non-medical beliefs far outside of the norm, some of which are heterodox religious ideas, some of which are conspiracy theories, and some of which are just plain strange. I think her comparison of doctors like myself to Nazi scientists and doctors because we aren’t willing to use unproven medicines and some of the other references in this paragraph hint at that. While I do think that this line of conversation sadly does have some value- it is important to understand if the people we choose to give credence to are reliable sources of truth- I feel that my calling here is to speak to Dr. Immanuel’s arguments, statistics, and scientific interpretations alone.
Dr. Stella Immanuel: (10:09) And today I’m here to say it, that America, there is a cure for COVID. All this foolishness does not need to happen. There is a cure for COVID. There is a cure for COVID is called hydroxychloroquine. It’s called zinc. It’s called Zithromax. And it is time for the grassroots to wake up and say, “No, we’re not going to take this any longer. We’re not going to die.” Because let me tell you something, when somebody is dead, they are dead. They’re not coming back tomorrow to have an argument. They are not come back tomorrow to discuss the double blinded study and the data. All of you doctors that are waiting for data, if six months down the line you actually found out that this data shows that this medication works, how about your patients that have died? You want a double blinded study where people are dying? It’s unethical. So guys, we don’t need to die. There is a cure for COVID.
This is painful, because she’s absolutely right; dead is dead (although some of us believe that’s not true at all). And if in 6 months I have lost COVID-19 patients and a large, well-controlled, double-blinded placebo controlled study does overturn all the best evidence we have so far and proves that hydroxychloroquine would have saved those patients if I had just given it to everybody who thought they might have the virus or who had certain risk factors or a certain constellation of symptoms, I will be sad that I didn’t use it. I’ll write about it on this blog, and my agony over it will probably come through pretty clearly because I’m not great at hiding that kind of thing. But what I won’t be able to say is “it turns out Dr. Immanuel was right” or “it turns out Dr. Procter was right.” Because recommending a medication that later turns out to be useful based on bad data, misunderstanding statistics, shifting the goalposts of what it means to diagnosis an infection or what constitutes valid evidence, and indiscriminate prescribing designed to bolster my own confirmation bias is still wrong. What’s that saying, something about a blind squirrel is still right twice a day, and we shouldn’t… be blind squirrels… leading the blind? Being right for the wrong reasons is called being lucky (or in the absolute best case scenario, deeply intuitive), and it’s great for you and your patients; it isn’t something anyone can reasonably or ethically follow you in.
How many medications do you take? There are over 20,000 prescription drugs approved by the FDA; unless you take that many, there are probably some out there that might help a symptom or a condition you have; maybe even some that might save your life. We could put you on chemotherapy because you might have cancer. We could put you on daily antibiotics because it might prevent your next urinary tract infection. More to the point, we could treat you with chronic opioids because they have a mechanism for helping your pain, even if your pain is unlikely to have any long-term improvement from them and you run the risk of opioid dependence, a condition I treat every day and have seen ruin lives in ways you wouldn’t believe. We could treat every child who might have an ear infection with antibiotics, regardless of diagnostic standards and the very real risks of antibiotic resistant bacteria (not to mention diarrhea diapers). We could put every flu patient on tamiflu even though it can be a harsh medication and has only limited efficacy in limited clinical scenarios.
No Dr. Immanuel, it is notunethical to refrain from using a medication in a clinical scenario where it has no proven efficacy. This is the philosophy that led to the opioid epidemic and every day leads to polypharmacy, another very real killer of the elderly. We took oaths to first do no harm, and sometimes that means sitting in the tension and anxiety of an unknown future with our patients and admitting, regardless of our own hubris, that we don’t have anything special or prescribable to offer other than our sound advice, sincere compassion, and reliable information. In fact, this is actually a pretty big part of our jobs already.
If 6 months from now (or hopefully sooner) some reliable evidence shows that hydroxychloroquine has a use in specific scenario to treat COVID-19, I will be the first one to prescribe it. Until then, the anecdotal evidence isn’t strong enough, the mechanism of action not surefire enough, and the scientific evidence not promising enough to justify the type of widespread everyone-gets-a-dose treatment these doctors are espousing; and unfortunately, despite her passion and her compassion for her patients, Dr. Immanuel’s clinical evidence, at least as she has shared it here, adds to that data not even at all.
From this point the press conference continued for another half hour. America’s Frontline Doctors is prolific; since this video they have also released additional hour and even three hour long videos. Although I think there are many points from the remainder of the video that could be analyzed, including quite a few I agree with, some that need clarification or explanation, and some that deserve to be debunked, I have to accept my limitations and accept that at this point analyzing the remaining claims is not the most pressing use of my time.
My apologies to anyone who might have been waiting for me to address a specific point in the remainder of the press conference; please do not hesitate toget in contactwith me with specific questions, which I may be able to integrate into future posts.
I have deleted the remainder of the transcript since I do not have plans to address the remaining points, but it can be found here and the video can still be found in various places across the internet.
At some point in this sort of voluntary, part-time work, you have to face the fact that people can produce misinformation, honest misunderstandings, and conspiracy theories far more rapidly than you can write about them, and that it is literally, physically impossible to keep up. For me, this realization came around the first week of April. At times like that I am thankful for people like Dr. Mikhail Varshavski (“Dr. Mike”) and Dr. Zubin Damania (“ZDoggMD”) who are doing this work consistently on Youtube and their own websites, and for people like Dr. Emily Smith, Your Friendly Neighborhood Epidemiologist, and the anonymous Your Local Epidemiologist, who for all I know might also be Dr. Emily Smith (I’m just saying, have you ever seen them together in the same room at the same time? Probably not. Because quarantine). If you have a question about a piece of misinformation or something that’s unclear about COVID-19 that I haven’t addressed on this blog, or (as seems more likely) that I’ve addressed in such a wordy and convoluted way that you are actually worse off than you were before my ‘explanation’, chances are one of these folks has got your back. There must be many people out there doing this type work that I am missing; please feel free to link to their sites in the comments.
With so many pieces of misinformation floating around out there and so little time to write 3,000-5,000 word blog posts, today’s post is just an attempt to debulk the malignant tumor of COVID-19 misinformation. The rules are simple:
Memes only.
Each meme gets one paragraph only (paragraph length unspecified)(and it still counts as one paragraph if it is interrupted by pictures or videos).
The crazier or less sincere the meme, the snarkier the response.
COVID-19 Medical Information.
We’ll start out with a light one. I’ve seen this posted with the comment “Coronavirus is a cold.” It’s hard to derive any sort of conclusions from just that. Does the meme intend to convey that the entire worldwide pandemic is a hoax? Are they are trying to say that literally all of the deaths and suffering have somehow been fabricated? If I posted this meme with the comment “wow, look how much we’ve learned about Coronaviruses in the last 3 decades,” it would completely change the meaning; but the meme as written is clearly designed to imply that the pandemic has been faked because coronaviruses only cause colds. I think there’s at least three legitimate ways we could debunk this idea, and I can’t really decide between them, so we’ll do all three. First, we could do some basic education on medical history. ARDS, Acute Respiratory Distress Syndrome, was first described in 1967, just one year before Coronaviruses were classified; but the first Coronavirus that was known to cause ARDS was SARS in 2003. Obviously it wouldn’t have been known in 1989 that Coronaviruses would emerge that caused such severe respiratory complications, and thinking of them as a virus that typically only causes a common cold was perfectly reasonable. If you want a thorough explanation of the history of coronaviruses and ARDS, I recommend this article, which could have been written as debunking of this meme: A Brief History of Human Coronaviruses by Shawna Williams. It contains an excellent visual timeline, which I’ve included only a fragment of here.
The second approach I think is valid is to point out how silly it would be to fake a pandemic using a virus that is known to cause only a common cold. It seems like faking infections, hospitalizations, chronic complications, and deaths in every single country in the world and having doctors, nurses, respiratory therapists, researchers, and millions of non-medical people pretending to be patients, would take an awful lot of effort; maybe it would have been worth devoting some of that untold energy and seemingly infinite resources to attributing your fake pandemic to a pathogen that couldn’t be disproved by by pulling up any old text book from before 2003. This is what makes me think that the meme was knowingly deceptive on the part of the original creator, because it’s so hard to believe that somebody actually found this in a 30 year old text book and said to themselves“aha! got ’em!” The third and final point we could make is to just point back at the meme itself, just eight lines up:
This textbook page doesn’t list cervical cancer as a disease linked to the Papovaviruses family, which under the classification scheme used at that time included human papillomavirus; HPV. Maybe it’s a good thing that medical knowledge and research has continued to progress since 1989?
This is one of my favorites, and was actually shared to my Facebook wall by my mom (I should clarify; she shared it because she also thought it was ridiculous and knew I would enjoy it). Something like this almost has to be written facetiously, right? But for the sake of thoroughness, let’s clarify a few points here. First of all, the reason the collection is done in the nasopharynx really isn’t that complicated; that’s where the virus is more densely populated, compared to other locations that could be swabbed, and going deeper in increases the chances of picking up the virus on the swab. I know it’s uncomfortable; I’ve had it done three times now, and the second time was especially awful. Despite what people may think, doctors and nurses don’t like causing pain, and we wouldn’t use it if we felt like there were other reliable options. But so far studies comparing the sensitivity and specificity of Nasopharyngeal swabbing to other swab techniques and locations have been mixed in terms of how determining how necessary the Nasopharyngeal swab actually is. Some have shown that it clearly gives us the most reliable way to tell if you have the virus or not, and others have shown that other swab locations might be just as good. But until something like a definitive answer emerges, doesn’t it make sense for your doctor’s office to use the technique that everyone agrees is as accurate as possible? This is all pretty obvious, but doesn’t answer the question of ‘if the virus is so contagious, why wouldn’t a less invasive test work?’ The other part of this meme seems to call into question that the virus is contagious if we have to do such an uncomfortable test to detect it, and the answer here is simple too; when we test for the virus, unlike when you get infected with the virus, we don’t have the virus’s help. You see, your body is a good breeding ground for certain viruses, who use your own cellular machinery to reproduce and, when they reach a certain point (viral load), begin to cause disease. This takes time; the incubation period (how long it takes the virus to reproduce enough to cause illness) of COVID-19 is 2 to 14 days; the COVID-19 test we use in our clinic comes back in 15 minutes. That’s because the tests we use aren’t trying to let the virus go through multiple reproduction cycles until it has proliferated enough to be detected; this is a good way of testing for pathogens called a culture, but it takes longer. The rapid tests rely on detecting some part of the virus, such as its DNA or specific proteins, and the more of the virus that is collected for the test, the more likely it is for the test to be accurate. In other words, the test may require more of the virus to be reliably accurate than the virus requires of itself to make you sick. Finally, the part about the microchip is really, really silly, and if you believe it there probably isn’t much I could say to change your mind; but if it helps here are two videos; the first showing exactly what our swabs look like, and the second showing me getting the Nasopharyngeal swab done at one of our clinics.
I realize some microchips are smaller than what my phone’s camera can pick up, but I’m not buying a digital microscope to appease conspiracy theorists.
This was swab #1 of 3 since April, and I’m worried the microchips are starting to build-up in there.
Two signs that your meme is bad:
Your main point can be summed up as, “people with certain medical conditions deserve to die.”
You add a picture of Morgan Freeman and I still don’t read it in his voice.
There’s not much to do with this one. Sometimes high blood pressure, diabetes, and obesity are significantly attributable to personal decisions, and sometimes not. It’s always, and I mean always, much more complicated than people know from the outside, and managing these conditions both as a doctor and as a patient is hard, frustrating, and often feels like an uphill battle. Sometimes people can exercise, and sometimes they can’t. Yes, smoking is bad for you, and I spend a lot of time trying to help people quit (by the way, one of the most effective and least utilized methods for quitting is getting a smoking cessation coach. You can get one for free at https://www.yesquit.org, and they can even help set you up with free nicotine patches or other medications), and you should quit, but we know it isn’t easy. The idea that anybody should be shamed or punished for a medical condition, let-alone medical conditions that are only partly modifiable with behavioral changes, is obscene. Shame on you to whoever made this meme and to anyone who shared it, and on Morgan Freeman for endorsing it.
Before I get angry e-mails, that last part was a joke; I realize that Morgan Freeman has no idea this meme exists. But isn’t there something disturbing about both this and the next meme exploiting the images of Black men- one for his gravitas, acting talent and air of wisdom, and the other for his strength, hard work and physical prowess- to minimize a pandemic that is disproportionately killing Black and minority men and women?
I’m going to just admit now, figuring out the origin of this picture took me longer to research than almost any medical question I’ve addressed on the blog so far. At first glance I had no idea what was going on here, but I braved the internet so that you don’t have to, and here’s what I came up with. According to my research, the image depicts champion body builder Blessing Awodibu, known both for his multiple body building titles and his various comedic Youtube videos, flexing next to “Daddy Long Neck”, a social media personality and musician who has Marfan Syndrome, a connective tissue disease. The two did a sketch together on Youtube back in December of 2018 where they arm wrestle, and this image appears to have been taken at the same time. We’ve already addressed this idea that by taking precautions to avoid COVID-19 you are somehow coddling you immune system into a state of weakness back when we compared your immune system to a Death Star, and on a few other occasions early on in the blog, so I won’t rehash it here. Suffice to say that while exercising is of course a healthy habit, none of the things listed by Awodibu are going to protect someone from COVID-19, and I’m fairly grossed out by the fact that whoever made this doesn’t wash their hands before eating.
Really, this meme is just the jock version of this nerdy Star Wars meme I made back in April.
There’s also a good bit of irony here, since in the original Youtube sketch Daddy Long Neck actually won the arm-wrestling match, prompting Blessing Awodibu to ask “which protein do you use?” This would imply that the immune system in the meme that is wearing a mask, using hand sanitizer, and doing curbside pickup for groceries is less likely to get sick from COVID-19, so I guess I do agree with this meme after all.
COVID-19 Statistics (Yay!)
I’ve included a few statistics memes that were sent to me recently, and this first one is the most straightforward of the bunch. Unlike the others, which make a few important intentional or accidental statistics errors, this one is clearly written by someone who has no grasp of statistics at all. Let’s look at the three statistics it gives:
0.94% of Americans have contracted the virus. This is actually a really terrifying statistic, because if it were true, it would mean that the now 143,000 deaths (up over 10,000 since this meme was made last week) are just the tip of the iceberg; that we’ve had that many people die and over 99% of the population hasn’t even had the virus yet. Fortunately, this meme is only accounting for confirmed cases, and does not take into account any of the antibody testing and studies that have helped us get a better estimate of the number of asymptomatic and minimally symptomatic people who have already been infected with SARS-CoV-2 without realizing it. Even in areas that have already survived a surge of cases, these numbers have not been anywhere near high enough to confer herd immunity, and we definitely aren’t out of the woods yet; but if only 0.06% of people have even had COVID-19 at this point, we would be on track to blow even the most dire models from March or April completely out of the water.
The survival rate is 95.72%. We talked about this a lot back in the posts about the Dr. Erickson/Bakersfield Urgent Care Doctors video. The easiest way to make a really alarming statistic seem mild is to just present the inverse. A “95.72% survival rate” sounds like a good thing, because survival is good and 95% is a ‘high’ number; “see, the good thing has a high number! It’s not that bad!” But this is exactly the same as saying that COVID-19 has amortality rate of 4.3%, instead of the still scary but much less catastrophic 0.5% to 1.3% most doctors I know would be willing to accept. A mortality rate of 4.3% is terrifying for a virus that is this contagious, and flipping it to “95.7 survival” makes it exactly 0% better.
So the first two statistics by themselves actually constitute a form of misinformation about the virus we’ve seen only rarely, in that it makes this already terrible pandemic seem even more dangerous than it actually is. Which is what makes the final statistic so baffling.
Only 0.04% of Americans have died, so the survival rate is 99.96%. This is why you don’t make memes as a group project; it’s obvious that the person who wrote the last part hadn’t looked at the rest of the presentation, since the line immediately before this claimed a survival rate of 95.72%. What they’ve done here is divided the number of deaths by the entire population whether they’ve had the virus or not, very similar to what Dr. Erickson did in his video when looking at deaths early in the pandemic (“millions of cases, very little death”). But that’s not what a “survival rate” is at all, because you are basically making the claim that hundreds of millions of people have ‘survived’ something they haven’t been exposed to yet. I can think of exactly one type of scenario where it would be helpful to calculate a “survival rate” based on the entire population instead of just the people actually effected (i.e. the people who have survived), and that would be after an extreme mass casualty event. For example, in the 1997 movie The Lost World: Jurassic Park, a T-Rex makes it from Isla Sorna to San Diego to rescue his baby by… Swimming? Stowing away on a boat? That movie was so crazy I can’t remember. He weaves a path of destruction across the city until… something happens to stop him, I think. Anyway, in a situation like that, it would be reasonable to calculate a survival rate for the entire city once the dust settles; but using the current number of deaths compared to the US population to calculate what percentage of Americans have “survived” COVID-19 right now is like calculating the T-Rex survival rate for San Diego while it’s still running behind you on Harbor Drive.
Dinosaurs aren’t that dangerous; most San Diegans weren’t even on that bus.
I like this meme for three reasons: 1. It starts and ends reasonably, 2. It comes from my home state, and 3. It is the best statistics example I’ve seen yet of comparing apples to oranges, only in this case somebody has painted an orange red and glued a stem to the top to try to pass it off as an apple. Let’s break it down a bit: “Here are some numbers that are confusing to me.” This is a great start, and honestly if all misinformation could start out this way instead of “READ THIS BEFORE FACEBOOK DELETES IT” we would be a lot better off. Covid-19: 3,399 deaths/88,691 cases = 4% of the people with cases have died.“ This is actually a great way to phrase this, because it emphasizes a few points that we can’t be too precise about. Louisiana has had 88,691 confirmed cases (now 95,002), but we can’t be sure how many people have had the virus without getting sick and getting tested, so saying that 3,399 of the people with confirmed cases have died, to get a case fatality rate of 4% is precisely correct. It also uses the present perfect tense instead of the past tense, a nod of recognition that this pandemic is not over. For people in Louisiana with confirmed cases of COVID-19, 4% have died up to this point; many are still fighting for their lives, many are recovering, and many more are being diagnosed as we speak; this number is dynamic.
Flu: 1,400 deaths/14,000 cases = 10% of the people with cases died. Notice the past tense? Because the 2018-2019 flu season is over now? Masterful. But unfortunately, here’s where it all goes off the rails, because Louisiana did not have 14,000 cases of flu last year; it had 14,000 hospitalizations for flu. And that completely changes the meaning of the statistic, because now you are comparing the very sickest flu patients with the most dangerous risk factors to all confirmed COVID-19 cases and getting a number on the same order of magnitude. That makes COVID-19 insanely scary. And we don’t yet know how many hospitalizations for COVID-19 this pandemic is going to have, or how many deaths, because we are still in the middle of the pandemic. We’ve talked about the problems inherent in comparing flu and COVID-19 before, and we’ll cover some of them again below; but if we want to compare something at least in the same fruit family, there are studies that have looked at the number of deaths compared to hospitalizations in Louisiana hospitals from COVID-19, just as this meme does for the flu. One study from the New England Journal of Medicine, which also looks at the increased burden of COVID-19 on African Americans due to chronic health disparities, found a hospital death rate of 24%,compared to the 10% for the flu in the meme above.
So, I don’t understand why we haven’t been wearing masks already? This meme is so precise in every other respect, and the mistake between 2017-2018 flu cases and flu hospitalizations is so glaring, that I can’t help but believe it was intentional. I find that really disappointing, because otherwise I really like this one, and I definitely agree with the final point. Why haven’t we been wearing masks before now? 15,000 to 60,000 deaths from flu each season may not be COVID-19 pandemic levels, but it still represents a lot of human pain, suffering, and grief, and wearing masks during flu season would cut down flu transmission a lot. Here’s hoping that our experience with COVID-19 will teach us some useful transmission control skills as a society going forward, just as SARS did for Taiwan in 2003.
We can move due West to my new home state, Texas, to see another meme explaining to us, contrary to what every doctor and epidemiologist has been saying for months, why COVID-19 just isn’t very dangerous compared to the flu. In a perfect world, it would be enough to explain that this is a fake, and move on with our lives. This is not a table published or endorsed by the Texas Department of Health and Human Services. There are a few ways to tell. First, it looks fake.
And second, DSHS said it wasn’t from them.
And really, do we need to say anything else about it? If the meme is a lie in the first place, do we need to spend the energy picking through the data? I will never understand the mentality that says, “sure, it was a lie, but I still think it makes some good points!” When you have discovered that something (or someone) is not a truth telling thing, stop going to it for truth.
Flu Rates, 2017-2018, 2018-2019 We can ignore the negativity and positivity rates, because they really don’t matter for this discussion. The rest of these took me a minute, because I’ve never seen these numbers before, and they didn’t really make sense. You see, the commonly acceptedcase fatality rate of the flu is 0.1%, and I couldn’t figure out either how or why a meme trying to show that the flu was more dangerous than COVID-19 would cut the death rate of flu by more than half. It took a few minutes (honestly, as many times as I’ve seen this dumb trick played since I started this blog, I’m embarrassed it took that long), but then it hit me; they are dividing the numbers from the top the rows by the population of Texas to get the numbers in the bottom 5 rows. It’s the same nonsensical math they did in the first stats meme we look at in this blog post! Look at the “Seasonal 2018”:
They calculate the “infection rate” by dividing the number of positive tests by the population of Texas. 35,339/29,677,668×100=0.11908%. The problem is, that isn’t the number of flu cases, it’s just the number of positive flu tests. I saw scores of flu patients in both of these years, in the state of Texas, but most of them aren’t represented by this data because most didn’t get a flu test. Why? Because it’s primarily a clinical diagnosis and the flu test has a sensitivity of 50-70%. Unless it’s a clinical scenario where having a specific test result is going to change the patient’s treatment, the flu test isn’t useful to me. I often offer it to people who ‘just want to know’, but if they have flu-like symptoms and flu exposure in the middle of flu season, I’ll explain that ‘if this flu test is negative, I’m not going to believe it because you definitely have the flu.’ So that infection rate isan extremely inaccurate, way too low estimate of how many Texas had the flu during the 2017-2018 flu season. Why does that matter? It doesn’t really, for this discussion, except as a hint at the fuzzy math strategy they are going to take with the more vital numbers.
They calculate the “death rate” by diving the number of deaths by the population of Texas. 11,917/29,677,668×100=.04015%. Again, that’s not anything. You could compare the death impact of flu to other diseases by comparing the deaths per 100,000 people, or you could compare the case fatality rate by dividing the deaths by the total number of cases; but just diving the number of deaths by the total population conflates these two important numbers and gives us nothing useful at all. But it gets worse.
They calculate the “recovery rate” by subtracting the number of deaths from the population and then dividing by the population. (29,677,668-11,917)/29,677,668 x100=99.95985%. So by their own math they are saying that 29,665,751 people in Texas recovered from the flu, including 29,642,329 people that never had it.This is by far the strangest use of the word “recovery” I’ve ever heard. Please, tell a friend that you’ve recovered from measles and when they ask, “when did you have measles?” tell them, “I didn’t; that’s why I said I’ve recovered from it. Duh.” See if you don’t get punched.
So what do they do with the COVID-19 data? Well, pretty much all the same nonsense; claim that tens of millions of people have ‘recovered’ from COVID-19 who haven’t even had it yet, divide the deaths by population instead of by confirmed cases to get a “death rate” of 3,112/29,677,668×100=0.01049% instead of 3,112/250,462×100=1.3%, and produce an infection rate that is utterly meaningless. But the two worse misinformation sins are these: first, they have gravely misunderstood the differences in our testing strategies for flu and COVID-19. In flu we test the sickest patients or the patients for whom a certain test results really guides our clinical judgement, which means we test a relative few of our actual flu patients. In COVID-19, we are testing many patients including people we don’t think have the virus because it is important for contact tracing and other epidemiology measures (and of course because we want to implant as many of those microchips as possible). This means that positive tests vs. deaths is not a useful statistic unless you really understand the testing strategy, because the COVID-19 strategy is going to catch a far higher percentage of the mildly symptomatic COVID-19 cases than we ever would for flu. But the point of this meme, I honestly believe, is to draw your eyes to the four cells right here, to try to trick you into thinking that COVID-19 is orders of magnitude less dangerous than the flu, which couldn’t be further from the truth.
But the second misinformation sin is also the most important, practically speaking, and it’s this; that they made this meme in the middle of the pandemic, and COVID-19 is still killing Texans. Since this meme appeared a week ago, we’ve gone from 250k cases to 332k, and from 3,112 deaths to 4,111. 1,000 lives in less than 10 days. The meme calls flu season a whole year (“10/17-10/18”) and tries to stretch the COVID-19 pandemic in Texas to as long as possible to make them seem comparable; “1/20-7/20”. But in January and February we had zero deaths. By the end of March we had 42, and by the end of April, 782. This has been a Summer pandemic for Texas, and the people who will increase that total by next week are fighting for their lives today. In real life, in a hospital; not on a spreadsheet. I don’t know if COVID-19 will cause more than 10,000 deaths in Texas. I hope it won’t, but it probably will; I can’t see a way around it. The people who are sharing this meme have apparently already determined, right now, that those deaths will not impact their beliefs about this pandemic. Those lives won’t count. Whether it’s because they are nameless and faceless to them, or because they were ‘faked’ by the doctors, or because they heard that somebody who was in a car accident ‘got counted as a COVID death’, they’ve decided that no matter how many human lives are lost in our state, country, or world, it can all be waved away as long as you can find some way to arrange the numbers that makes those lives seem insignificant. Until it affects them personally, which is the very thing the rest of us are all working so hard to keep it from doing.
Political Stuff (Boo!)
I don’t know about international politics, and it’s too late to look it up, but I’m assuming this is wrong; surely somebody somewhere is trying to unseat a president this year. So, ha, got you on a technicality. I wrote last week about the idea that COVID-19 was a big conspiracy to somehow hurt the president, and how that depended not only on not having any knowledge about the pandemic, but also on not knowing much about doctors, because of whom I’ve been subjected to more doctor’s lounge Fox News broadcasts in the last decade than I ever wanted to watch in my lifetime. That’s about as political as I get on this blog, except to say this; dispelling this meme, and the beliefs behind it, should not be my job. It’s the job of our national leaders, and especially the presidential administration, to challenge these lies that are so incredibly dangerous to Americans, instead of tacitly endorsing and even actively promoting them. Every time they refuse, people die as the result.
Stay alive. Stay alive. I have never seen a patient so hypoxic They start out with a cough but by day 10 they’re looking toxic. Our leaders tweet “the doctors are faking this virus” We shoot back, “stop supporting these lies your job is to inspire us” Social media’s nothing but conspiracies, politics, They won’t listen to truth and reason, so everyday more get sick.
My name is TJ Webb and I endorse this message.
I haven’t thoroughly vetted this one, but I really like it.
Last week I saw about 80 patients who had screened positive for either exposure to COVID-19 or possible respiratory viral symptoms; this week more of my time is devoted to working in outdoor COVID-19 testing clinics, so it will probably be well over 100. Some of those patients had been ‘caught’ by our screening questions but really had no COVID-19 exposure or symptoms; the lady with a chronic cough who was really just coming for her high blood pressure, the gentleman with a fever that was caused by an abscess under his axilla (we call it ‘axilla’ because ‘armpit’ sounds so un-doctory). I treated them too, of course. But for the most part people were seen in our COVID-19 focused clinic specifically for COVID-19 related concerns. I don’t have exact numbers in front of me, but of the 70 or so I tested for the virus, about 20 came back positive (Epidemiology note: this is too small of a sample to calculate anything like a test positivity rate or prevalence from), and there were at least a couple that, due to certain combinations of exposures and symptoms, I’m convinced had the virus despite a negative test (way, way too small of a sample to make any calculations from; please don’t go and quote me as saying that based on my sample of 2 out of 50 negative tests I think there is a false negative rate of 4% or something crazy like that)(although now that I look at prevalence estimates and test sensitivity, 4% is actually about right. Hmm…).
I called each patient who tested positive personally to give them the news and answer their questions. Amid the many questions I was asked (‘Should I go to the hospital’?; not now, but let’s talk again about red flag symptoms and emergency precautions. ‘Should I isolate from my children?’; that’s really complicated, and it depends on the age of your children, your support structure, and their specific developmental, physical, and emotional needs), one question that came up over and over again is one I sincerely wish I had a better answer to; ‘what medicine can I take to make sure this gets better?’
This is a big and important question. Doctors kind of like medicine; kind of a lot. After all, prescribing them is a big part of our job, and even though adding a medication is not always the right answer (more on this later), it is incredibly satisfying to prescribe the right medication or therapy for the right diagnosis and then see your patient get better. It can also be fairly stressful at times, because no medication (except prenatal vitamins) is perfectly safe; giving someone a medicine, especially one that wasn’t actually necessary, and then seeing them suffer because of drug interactions or unexpected side effects is devastating to a physician. We have taken an oath to ‘first do no harm,’ and we take it seriously. This is why I’ll spend 10 minutes carefully explaining to a parent about how viruses and bacteria infect the body differently and how antibiotics work rather than spend 2 minutes prescribing their child an unnecessary antibiotic for a viral illness, which would surely feel more satisfying for both of us. It is also why, as certain as I am that some of the patients I have shared the news of a positive COVID-19 test result with will end up getting sicker, and as nervous as that makes me on their behalf, I have not been prescribing unproven, untested medications out of desperation, but have instead focused on teaching those patients how to keep themselves and others safe and how to recognize the early signs of a severe infection.
It’s also why I check for new or updated studies or professional recommendations, and review information being shared between doctors and other clinicians on COVID-19 social media groups every every single. The moment that there is a proven, safe early therapy to prevent COVID-19 infections from becoming severe, I will be the first to start using it.
Dr. Richard Bartlett discovers silver bullet for COVID-19.
Last night I came across a viral video, which has since been sent to me multiple times, which seemed to promise exactly this. A doctor here in Texas went on a morning news show to discuss the 100% effective, perfectly safe COVID-19 treatment he is using to prevent severe illness in his patients. If you have any degree of medical training or even personal experience with medical issues, you are probably just as skeptical as I am about both the ‘perfectly safe’ and the ‘100% effective’ claims; few medicines are ever either. We will go through Dr. Bartlett’s interview in detail below and try to evaluate the quality of data he is relying to make these claims, and answer two questions; should you call and ask your doctor for this ‘new’ treatment, and should I call back all of my patients and tell them, much to my satisfaction, that we do have a medication I can put them on after all?
One quick note: the video is about 30 minutes long and trails off a lot into conspiracy territory concerning mandating vaccines, instituting lockdowns to destroy the economy in order to hurt President Trump’s reelection chances, and quite a few other areas. We’ve covered a lot of that before, and frankly a lot of it falls outside the realm of medical misinformation. We will try to cover the most important parts of Dr. Bartlett’s interview regarding his new COVID-19 therapy, but I won’t try to write the 10,000 words it would take for a rebuttal to all of these ideas.
Here is the video:
00:16: Midland Texas is located in Midland County, about 6 hours West of Waco (golly, Texas really is huge). With a population of 138,000, it is almost exactly the size of Waco. Just like for us and the rest of Texas, they began to see a significant increase in COVID-19 infections about 3 weeks ago. Before this, they had seen very few cases total, like most pre-surge areas. You can review their data here.
00:33: The article is here; it provides some additional details and we will reference it later.
At 02:04 Dr. Bartlett begins his discussion on COVID-19 treatment in earnest by discussing the context for the pandemic in America, namely a comparison to both nations that have fought the pandemic successfully and those who have struggled more with a higher number of infections and deaths. He begins with Taiwan.
02:07 “In the country of Taiwan there’s over 25 million people, they’re stacked on top of each other, if they did social distancing they’d be out in the ocean floating around.”
He goes on to say that there isn’t enough room to social distance, and yet the country has seen only 7 COVID-19 deaths, “as many people as you could stack in a minivan.”
The problem here, besides Dr. Bartlett’s strange obsession with stacking people, is that Taiwan has done social distancing. Dr. Bartlett goes on in the video to assert that Taiwan has foregone both social distancing measures and widespread face mask use (which he associates with Communist China). Do any reading on Taiwan’s response to COVID-19 and you will find widespread wearing of face masks and aggressive physical/social distancing measures since the earliest days of the pandemic, in addition to other mitigation strategies such as providing social support for quarantined patients to help them maintain a high level of isolation, and using mobile phone technology to perform extremely precise contact tracing. This is all in the context of a strongly collectivist culture willing to engage in such measures for the good of their neighbors regardless of official mandates, with a history of understanding the stakes in such a pandemic because of their experience with SARS in 2003.
So as Dr. Bartlett moves forward talking about Taiwan later in this video, you need to understand that, perhaps entirely unintentionally, almost everything he has said about their success in fighting COVID-19 so far is the opposite of what they have actually done.
02:41 At this point Dr. Bartlett also mentions Iceland, Singapore, and Japan, who all engaged in some combination of extensive masking and social distancing except Iceland, who used aggressive contact tracing and quarantine measures. Dr. Bartlett’s assertion that they have been successful because they have used similar treatment plans to what he uses for his patients seems entirely unfounded.
02:59 “That’s not possible according to what we’re being told in the mainstream media.”
Literally nobody is hiding this data. If you google “Taiwan COVID” you get this:
“You can even look it up in the Johns Hopkins COVID website and you’ll see those numbers. They’re hidden in there, but I’m pointing them out.”
“Hidden” in the sense that geography is hard.
I’m concerned that what Dr. Bartlett is doing here is contributing to a false narrative that the powers that be, especially the CDC, the WHO, and the medical establishment (i.e. he and I), doesn’t want people to have access to good reliable data. Maybe this is where Dr. Bartlett’s search for reliable information to back up his COVID-19 treatment has led him; not trusting the available information because he wasn’t able to find the scientific verification he is sure must be out there for his new therapy. Maybe this is strongly ingrained in his political position (he recently ran for office) and he is interpreting the ready availability of this kind of data through a lens of suspicion, or knows that his audience on this show will affirm the idea that this information is being hidden from them and that it is harmless to reinforce that belief. But I am always a little suspicious of physicians who want to weave these tells of conspiracy theories and hidden truths about the pandemic while promoting their own unverified findings, and part of me wonders if they are certain they will face pushback from their fellow doctors and scientists, and want to head it off at the pass by encouraging the idea that those doctors and scientists don’t want you to know ‘the truth.’ I certainly hope this isn’t the case with Dr. Bartlett, but part of me thinks it must be an easy trap to fall into without realizing it.
It isn’t Hydroxychloroquine
03:32 “(In these other countries) they’re doing what I’m doing, which is not hydroxychloroquine, although that works….
Before he reveals his miracle drug, he gives a brief shout-out to Hydroxychloroquine, stating it does work but not providing further explanation as to how he knows it does or why he doesn’t use it as well. I almost wrote today about a viral post by a doctor in McKinney Texas again promoting outpatient, widespread hydroxychloroquine use in patients regardless of test results and risk factors. We covered this pretty extensively over a month ago following his colleague Dr. Lozano’s speech at the Set Texas Free Rally in Dallas. He also claims that masking, social distancing, and even testing are ineffective. I’ve chosen to write about Dr. Bartlett’s video instead, but in terms of relying on anecdotal evidence and not understanding representative sample sizes, there are a lot of similarities. If things are quiet this week I will try to write about Dr. Procter’s social media post as well and try to tackle hydrochloroquine one last time.
I want to talk hydroxychloroquine. I want to talk about these scripts that you’re writing; Put down the pen, stop prescribing. I want to talk about what I have learned, About the research you have spurned…
The Silver Bullet: Inhaled Budesonide
03:36 “So what they’re doing is an inhaled steroid. So my silver bullet is inhaled budesonide.”
Dr. Bartlett finally reveals his miracle drug, inhaled budesonide; a commonly used inhaled corticosteroid that is commonly used for patients with Asthma or COPD.
This is the first good place to stop and look at this idea in more detail. The first two questions we need to ask when someone proposes a novel use of a medication or therapy are 1. Is there a proposed mechanism by which this would work? 2. Why did nobody else think of this (has this been tried/studied before)?
Dr. Bartlett’s rationale is that since this is an inhaled respiratory anti-inflammatory, it should work for COVID-19 which is a ‘respiratory inflammatory condition.’ Part of the problem here is that this is gross oversimplification of the virus’s pathophysiology, which is still not completely understood (see below). It is supposed to make you go “wow, that’s just common sense! It causes inflammation in the lungs, so an anti-inflammatory breathed into the lungs will cure it!” But if you reflect on whatever extent of experience you have with medicine, you will realize that things are never quite that simple. If you came to me for your severe, debilitating back pain you’ve been struggling with for years and I said, “oh I’ve got it, back pain is caused by inflammation of the muscles and joints, so I’ll give you a medicine to decrease inflammation; here’s some ibuprofen,” you’d probably lose a great deal of respect for me. You’d be right to. NSAID’s (non-steroidal anti-inflammatory drugs, like ibuprofen) may well be part of your treatment plan, but your back pain is complicated and is going to require more thorough evaluation and treatment. In medicine, you are right to beware of easy answers.
Sentences like these are why I went into clinicalmedicine.
Budesonide is a common medication, as he points out repeatedly beginning in a few minutes, and I think this is actually the strongest argument against his proposed use of it in COVID-19. You read that right; I’ll explain. The usual dosing of budesonide is twice a day as a maintenance medication; by decreasing inflammation and swelling in the airways, it can eventually (it may take weeks to months) lead to less frequent asthma and COPD symptoms like cough and chest tightness, and fewer exacerbations. However, Asthma and COPD patients still have acute exacerbations despite using inhaled corticosteroids. We still see patients on budesonide in the clinic and in the hospital for acute worsening of their symptoms due to respiratory infections. Sometimes these are bacterial infections, but more often they are viral; including coronavirus species. Sometimes these patients go into respiratory distress, and sometimes die, even when the virus they have isn’t nearly as deadly as COVID-19. If budesonide was able to completely prevent viral respiratory illnesses from causing inflammatory respiratory symptoms like cough, shortness of breath, wheezing, and chest tightness, we would never see these patients getting sick from respiratory viruses; but we do, because the medication doesn’t really work that way. If Dr. Bartlett consulted his complex understanding and professional history of treating respiratory infections he would realize that his proposed mechanism really doesn’t make sense, especially as the 100% effective silver bullet he is promoting it to be.
Later in the video (around the 06:36 mark) Dr. Bartlett does talk about the “cytokine storm” in COVID-19 and prevention of the body’s own inflammatory response to the virus. Is it possible that the medication he is using, while not preventing all respiratory viral infections, at least treats this one? Without getting into the weeds too much here (the idea of a cytokine storm being the underlying cause of ARDS in COVID-19 is still controversial), we need to understand that you don’t just have this one thing called ‘your immune system’ causing this process called ‘inflammation’, so that if ‘inflammation’ (or in this case, ‘cytokine storm’) is the problem we can just suppress the immune system and call it a day. The immune system is incredibly complex, and any given immunomodulating medication is going to work on parts of the immune system (and not always in the ways we hope or expect) while not significantly affecting others. As an example, the primary cytokine implicated in the COVID-19 cytokine storm seems to be interleukin 6, a pro-inflammatory cytokine that budesonide, in previous studies unrelated to COVID-19, doesn’t seem to affect appreciably. Studies focused on medications that do appreciably decrease IL-6 activity are currently underway.
I’m having bad flashbacks to 2nd year of med school right now.
The second question, if the mechanism did make perfect sense, would be to ask whether anyone has tried this before. Dr. Bartlett indicates that it has been tried elsewhere; he states that this is what they are doing already in Taiwan and Singapore. I was unable to substantiate this; I cannot find any evidence that these nations have used anything like widespread protocols with inhaled steroids to treat COVID-19 early in the disease course. There are some ongoing trials with use of inhaled corticosteroids (not budesonide, at least that I could find), as Dr. Bartlett mentions, but there is not any data available from them yet; if they prove safe and beneficial for COVID-19 patients, we would start using them in all the clinical contexts where they were shown to be effective.
There are two other data sources we could look at. First, the most successful trial we have right now with use of steroids in COVID-19 is the RECOVERY Trial out of Oxford, which I wrote about recently. In this study patients were put on systemic steroids (dexamethasone) once they were already hospitalized. You might argue that this isn’t what Dr. Bartlett is talking about at all, that he wants to use budesonide before they are sick enough to go to the hospital. I understand that; but the study showed a reduction in mortality in both the groups needing oxygen and those requiring mechanical ventilation, but not in those who didn’t require oxygen. You can only extrapolate so much from this, but if Dr. Bartlett’s theory of the earlier the steroids the better panned out, you would expect the non-oxygen group to see at least as much improvement in outcomes as the patients who were already very, very sick; but that wasn’t the case. We need to remember that even though our first successful randomized drug trial for COVID-19 is indeed a steroid, the role it plays is complex and the benefits limited to certain clinical scenarios; the data still shows that immunocompromised patients, including those on medications that modulate the immune system, are at a higher risk for COVID-19 than those who aren’t.
We can also look at the two closest viruses to COVID-19 that we have experienced, SARS in 2003 and MERS in 2012. These are both Coronaviruses that seemed to involve a ‘cytokine storm’ causing acute respiratory distress syndrome. During these outbreaks inhaled corticosteroids were used more widely, but results were mixed; there was no strong evidence of benefit, and some evidence of worsening of the disease, including increased risks of secondary bacterial pneumonia and prolonging the time it took for the body to clear the virus.
Edit: When discussing this issue, a colleague also pointed that this idea of ‘what about decreasing inflammation in the lungs’ is not novel, and studies have tested inhaled corticosteroids on practically every lung infection (infection is a very pro-inflammatory state) over the past 30 years, not just SARS and MERS. Results have been extremely unimpressive, but there has been consistent evidence of increased risk of certain types of lung infections, including tuberculosis, non-tuberculosis mycobacterium infections, and severe drug-resistant bacterial pneumonia.
So I’ll conclude this section where many people with much more expertise in this area than myself have, by saying that the balance of risks and benefits still doesn’t justify use of an inhaled steroid in people without asthma or COPD who are already taking one or would benefit from one anyway. There is no reason to believe that they will appreciably decrease the chances of developing the severe acute respiratory distress syndrome that makes the virus so dangerous for some people, and for the vast majority of people who will do fine with their own innate immune system fighting the virus, steroids would potentially increase both the risk of worsening infection and delayed clearance of the virus, and the risk for associated bacterial infections (in addition to a host of other potential side effects). If we were to begin using this in patients who don’t have COVID-19 as prophylaxis, we could conceivably increase their likelihood of getting the virus. The mechanism of causing these types of harm is at least as strong as the proposed mechanism of preventing worsening of the disease.
03:46 “It’s super cheap, it costs about $200 for the total treatment if you pay cash.”
I understand that he is probably intending this as a comparison to a hospitalization for COVID-19, which is disastrously expensive, as he truly believes the budesonide will prevent hospitalization. Still, all I can say is that Dr. Bartlett and I have different ideas about what constitutes super cheap medication; most of my patients could not afford a $200 medicine.
“But what does all of that matter? He said it is working for his patients.”
There are some more problematic statements in this video, including the idea that our numbers in Texas are only going up because of increased testing (17:05), revisionist statements that totally invert the sequence of events and thus cause and effect of social distancing and masking measures in the most affected countries (21:50), a troubling statement about Japanese people ‘crawling all over each other in Sushi bars’ (22:55), and strangest of all, repeated statements about how waiting to treat someone until they have symptoms is un-American, whereas early treatment is the American way (both preventative and acute care are part of every healthcare system in the world; there is nothing particularly American about throwing medications at people before you know whether or not they need them).
I hope to update this post with some rapid-fire answers to these issues later, but I want to focus here, for now, because I sincerely believe this is the part of Dr. Bartlett’s interview that people find most convincing.
“One hundred percent of my patients are alive. I’ve been treating this since March.”
I’ve written before about the dangers of anecdotal evidence. I think as physicians we are prone to fall into this trap for a couple of reasons. One is because we want so badly to help our patients, and if we hit on a medication that really feels like it is working, it’s hard to let go of that feeling. Another is because we spend so much time thinking about our patients and working for their well-being that their stories loom very large in our minds, and it’s easy for the relative importance, as data, of our personal small numbers of cases to become overinflated. With that in mind, I think it’s worth looking at Dr. Bartlett’s evidence from the outside and asking whether it really has the value he credits to it.
According to the local news article featuring Dr. Bartlett back on May 21st where he first publicly called budesonide his ‘silver bullet’ against COVID-19, at that time he had treated 12 people. Twelve. This is an incredibly small sample size, but we could hardly expect larger; Dr. Bartlett is not the only doctor in Midland, and throughout March, April, and May the entire county only had 1 or 2 new cases of COVID-19 most days; there just weren’t that many COVID-19 patients to go around. Dr. Lozano had previously gotten around this issue by saying that she wasn’t even testing, but was treating empirically based on symptoms or possible exposure, which doesn’t really make sense in a pre-surge area with incredibly low prevalence. Dr. Bartlett has stated that he believes in testing, and although his comments are mixed on whether he is treating only confirmed COVID-19 cases with budesonide, I think we could credit him with such qualms. Twelve cases over 3 months is an extremely small sample size, and it is important that we understand that this is not coming from someone who has been inundated with COVID-19 cases like our peers in New York; at the time that Dr. Bartlett decided that budesonide was a miracle drug he had practically no experience with the virus. It is certain that his numbers have come up by now, with cases rising all across Texas; but with lag time between exposure and the onset of symptoms, and a second lag between the beginning of symptoms and severe respiratory complications, it is not possible to say that all of Dr. Bartlett’s recent COVID-19 patients are out of the woods yet.
So Dr. Bartlett’s first error is over valuing the data from his sample size, but his second error is in thinking this disease is more dangerous than it actually is. I know that seems like a strange thing to type; the disease is plenty dangerous, and I have encouraged the utmost caution on this blog more times than I can count. We have looked over and over at the hundreds of thousands to millions of lives that might be lost if we do not discover effective drug therapies and if the virus continues to spread unabated because of poor adherence to mitigation strategies like face masks and physical distancing. But the virus has never been estimated as having a 20% fatality rate as Dr. Bartlett says in the video. Dr. Bartlett has no doubt been worried about COVID-19 since March, just like me. Just like me, he probably has friends and classmates working in ER’s and hospitals in New York and New Orleans and other areas that have already been hit hard, and has heard the horror stories about what this can do to both individual patients and entire healthcare systems. Like me, as soon as he started thinking about this respiratory virus he probably immediately thought of the names and faces of two dozen patients that he was particularly worried about. Due to this anxiety, surviving the virus has become, in his mind, the exception rather than the rule. We see this in his account of the woman battling cancer; he says “she should die according to what you hear from the CDC and the WHO,” even though we know that COVID-19 is not universally fatal for any group. By increasing the danger of the virus in his mind, or at least increasing the probability that any given patient will go to the hospital or die, it makes it seemingly unlikely for people to get better without some specific intervention, even though we know that is what happens most of the time; thus the interventions he has chosen (budesonide, zinc, antibiotics) receive the credit for his patients’ recovery.
Put these two biases or statistical errors together and it may be easy for a physician to believe, based on the slightest of clinical experience with this virus, that he has discovered a cure. Each patient you treat this way will confirm it for you, as long as they get better, even if they would have gotten better anyway, and particularly if they tell you they feel better right away, which is such a wonderful feeling even if it doesn’t always correlate to their eventual outcome. If you are willing to loosen your treatment criteria to include people who have had no test or negative tests, or who are fully asymptomatic as Dr. Lozano seems to have done with hydroxychloroquine, you can inflate your treatment numbers even higher. And if you top-out at something manageable for a small-town physician, say in the low 100’s, you might never see a fatality from COVID-19. Imagine that we were back in May when Dr. Bartlett had only treated 12 COVID-19 patients. He states boldly that 100% of his patients were alive, yet we think the death rate is around 1.3%. If just one of his 12 patients had died we might still find this convincing because we are so easily swayed by anecdotal evidence, but that would have been a fatality rate of 8.3% in his budesonide patients. We would have fallen into the same trap as Dr. Bartlett, of picturing those 12 patients heading toward certain demise and all but one rescued by his treatment plan, without which they would have died, when in reality there is no evidence to suggest that they would have been any worse off without the treatment. Dr. Bartlett’s experiences with the virus so far are exactly what we would expect without budesonide and antibiotics.
“Look, he says it is helping his patients and you don’t have to use it for yours, so why does it matter to you?”
Great question, hypothetical person who keeps arguing with me on the internet. Any time we begin talking about someone’s personal experiences, the temptation is to treat their narrative as incontestable; I wasn’t there, I didn’t see his patients, so I don’t have the ability to second-guess his clinical judgement. In a way this is actually sort of fair; Dr. Bartlett had just as many years of medical school and residency as I did, and has many years more clinical experience, and to some degree each physician has earned a degree of professional trust to practice in a way we see fit with accountability only to ourselves and our patients, at least in many circumstances. But we know that this professional leeway has been abused in the past, and even in the absence of abuse of that privilege, lone-wolf medicine is a real problem because by it’s very nature it is disconnected from one of the best tools we have to improve our clinical abilities and correct our errors; the honest feedback and accountability of our fellow doctors. If a physician feels that a patient’s clinical situation calls for a unique approach that is not supported by evidence, this can often still be tried as long it is accompanied by an honest and careful explanation to the patient of the reasoning behind this approach, the unproven nature of the treatment, and the risks involved. If we begin to make a habit of such practices, and particularly if we do so ignoring the voices of our peers around the world saying we’ve tried this before and it didn’t show reliable results on a larger scale, or the voice of researchers and scientists saying that doesn’t actually work the way you think it does, then we are doing so at our own, and more importantly at our patients’, peril.
In many ways I think Dr. Bartlett is actually going about this fairly well. He seems to imply that he is using the medication, which does have a theoretical mechanism of action after all, only on those who really do have COVID-19. He does not seem to be doing television interviews or talking with newspapers in order to make a name for himself and attract clientele from all over the state to help his business, as seems to be the case with some other doctors prescribing unproven treatments, but in order to ‘get the word out there’ to other doctors (as one of those other doctors, I deeply appreciate this impulse), although I am not sure why he has not utilized any of the many avenues on social media that many of use are using to get physician specific feedback and share ideas; maybe he is and we just aren’t part of the same COVID-19 doctor groups. Most importantly, he states that he has written and is submitting a paper for publication, which will provide both more details about his patients, their demographics, commodities, and clinical presentations, and allow for peer review and a higher degree of detail and scrutiny than we could possibly get through a TV interview.
But there are at least three ways (besides the tacit endorsement of several conspiracy theories) that I find Dr. Bartlett’s approach truly troubling. First, he is not presenting his treatment plan as an entirely unsubstantiated experimental approach driven by hope and a hunch, which is what it absolutely is, but as a “Silver Bullet” that is perfectly safe and cannot fail, which is certainly is not. One would hope that this is bravado or enthusiasm for the TV audience and not hubris; in other words, we have to hope that whatever confidence in his treatment regimen he shows in this interview, he is still very carefully explaining to his patients the limitations of his evidence and the potential risks they are taking on if they use it, and the red flags to look for in case it doesn’t work.
Second, he is not just promoting his unproven treatment but also discouraging mitigation measures, such as physical (social) distancing and wearing masks, that actually have been proven to save lives. It is unclear whether he believes the misinformation around these strategies not working or is just so confident in his treatment approach that he no longer thinks they are necessary, but the effect will be the same; as Dr. Bartlett’s video goes viral there will be increased pushback against wearing masks and observing distancing measures by those who find him convincing, which will ultimately lead to more cases, more hospitalizations, and more deaths. His evidence is too weak and his scientific rationale too shaky to convince a conscientious doctor to start using his treatment approach; but he speaks with enough confidence and sincerity to convince some people on the fence not to wear masks. The net effect of his interview, like any viral misinformation, is to make the pandemic more dangerous for everyone.
And third, by presenting his treatment plan as something that it isn’t and ascribing to it all of the confidence and reliability of a truly proven treatment, he is spreading misinformation that blocks out the transmission of reliable information for the public and pollutes the relationship between his listeners and their own doctors and healthcare systems. When I explain to patients that I do not have a proven medication I can in good conscience prescribe them to prevent their COVID-19 from progressing, their exposure to voices like Dr. Bartlett’s, Dr. Lozano’s, and Dr. Procter’s have already sewn the seeds of mistrust in the information I am providing, and they are less likely to believe the other recommendations I am carefully trying to give, such as isolating within their home and monitoring for red flag symptoms, and the reassurance I am trying to provide to alleviate their fear and anxiety as we discuss their individual chances of having a severe course of the virus. It may lead anxious patients to seek additional visits elsewhere and shop for a doctor that will prescribe them what Dr. Bartlett says they need, further increasing their chances of exposing others and potentially increasing the costs associated with their medical care, both to them personally and to an already strained system. It may even lead some patients, convinced by these doctors and desperate for medicines they now believe are their only hope of beating the virus, to misrepresent their symptoms in ways they think might push their doctor into prescribing them.
When lone wolf doctors promote unproven therapies and set themselves up as experts with miracle cures, without having actually done the clinical research to validate their claims, it erodes the fragile trust that we work so hard to build with our patients when we are unwilling to engage in that same type of speculative treatment. This unearned mistrust has the potential to breakdown the patient-physician relationship and affect our patients’ health for years to come. Millions of doctors, nurses, and other medical professionals around the world are working as hard as we can to both care for our patients in the midst of this pandemic and stay up to date with the latest diagnostic and treatment options. Viral voices drowning out the excellent work that is being done researching potential treatments, and calling out any doctor not willing to follow their lead, should humbly re-evaluate their limited clinical experiences in the face of this global pandemic and bring forward their innovations, not with less hope or enthusiasm, but with much more care and a realistic appraisal of the strength, or lack thereof, of their evidence.